
988368
Fri, Jul 17, 2026

Volume 15, Issue 3 (September 2017)
Iranian Rehabilitation Journal 2017, 15(3): 215-220 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Seraji M, Shojaeizadeh D, Goldoost F. Quality of Life of the Elderly Residing in Zahedan (South East of Iran). Iranian Rehabilitation Journal 2017; 15 (3) :215-220
URL: http://irj.uswr.ac.ir/article-1-665-en.html
URL: http://irj.uswr.ac.ir/article-1-665-en.html


1- Department of Health Education and Health Promotion, School of Public Health, Zahedan University of Medical Sciences, Zahedan, Iran.
2- Department of Health Education and Promotion, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran.
2- Department of Health Education and Promotion, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 482 kb]
(4030 Downloads)
| Abstract (HTML) (8765 Views)

Full-Text: (1807 Views)
1. Introduction
Aging of population or rapid increase in the number of the elderly is a global phenomenon. Decrease in childbearing capacity and increase in life expectancy has caused the elderly population to grow faster than the younger population [1]. Predictions indicate that the number of world’s elderly people will reach 1 billion in the year 2020. On an average 16% of the population in industrialized countries consist of elderly people and it is predicted that this rate will increase to 19% in future decades [2].
According to the reports of Statistical Center of Iran (SCI), in the census taken in 1385, the number of elderly people above 60 years old in Iran was 5.1 million, which makes 7.3% of the country’s population [3]. If this trend continues in Iran, we will, hereafter, have a population which is known as the elderly population [4]. Factors such as the increasing number of elderly people suffering from disability and functional disorder, lack of a supportive family system due to shrinking family size, women’s employment and jobs, and dispersion of family members will increase the need for long-term cares for the elderly in future decades [5].
Even though the main challenge of general health in the 20th century was “enhancing life expectancy”, the most important issue in this regard in the 21st century is “better quality life”. This is completely evident because elderly does not only mean having greater age and being alive, but their type and quality of life are very important issues too. Therefore, enhancing the quality of life of the elderly in the first instance, requires having comprehensive information about their quality of life [6].
Quality of life is the criterion for measuring the best energy or force in an individual. This force and energy are used for successful compatibility of an individual with the existing challenges. Various factors including shortages in elderly period, which cause a decrease in cognitive compatibility and decease in self-reliance can affect elderly people’s quality of life [7]. In general, aging can probably increase the affinity to some diseases and also lead to occurrence of disability during the final years of life [8]. In addition, the negative effects of aging on the ability to protect their independence will increase the need for assistance. The various problems and difficulties which occur physiologically during old age have some effect in decreasing the quality of life in that period.
In our country, Iran, about 28% of the elderly have limitations in performing physical activities independently, and they need help and assistance in order to do their usual daily activities. All these issues lead to decrease in quality of their life [9]. A study conducted on the elderly population of Tehran revealed a high rate of disability in them [10]. Since quality of life in this period of an individual’s life can easily be threatened, considering all the background factors in this regard that have a significance potential to influence [11].
2. Methods
This is a cross-sectional and correlational study which takes into account 117 elderly people above 60 years old residing in Zahedan. The sampling method in this study was population-based cluster random sampling. This means that area 2, 4, and 6 from among various areas in Zahedan (areas 1 to 6) were randomly selected on the map. Then, public places (mosques, parks, gyms, and shopping centers) and houses were recognized separately, so that in each area, one mosque, one park, and one shopping center were randomly selected. After that, the researcher with two other questioners who were trained in interviewing and filling the questionnaires went to these places and finally, 13 people from each public place were selected to take part in the study. Of course, the individuals had the required features for the study, and they were willing to participate. Meanwhile, physically disabled people were omitted from the study.
Data collection instrument was a questionnaire and the response to the question, inscribed questionnaire was written down and recorded by the researchers through interview. The criteria for entering into the study included having six months residency in the center, not having any chronic or acute diseases which are physically or mentally disabling, not having cognitive disorder, being literate or able to give interview. In order to account for the study’s ethical issues, a consent form was signed by each participant before filling in the questionnaire. Then, the questionnaire was given to each of them and they were informed about the study’s purposes and confidentiality of the obtained data.
The data collection instrument was a questionnaire on measuring the quality of life (SF-36) which consists of 36 questions and expressions on micro scales about physical performance, playing physical roles, body pain, general health, energy and joy, social performance, playing emotional role, and mental health. This is a standard questionnaire and has been validated in Iran [12]. The questionnaire was filled by the elderly participants themselves. Those who were illiterate or were not able to fill the form on their own were helped by trained questioners; the trained questioners helped the elderly fill the forms through interview. In order to determine the relationship between variables, we made use of Pearson correlation coefficient, independent t-test, and ANOVA. In addition, the data were analyzed by SPSS software, version 19.
3. Results
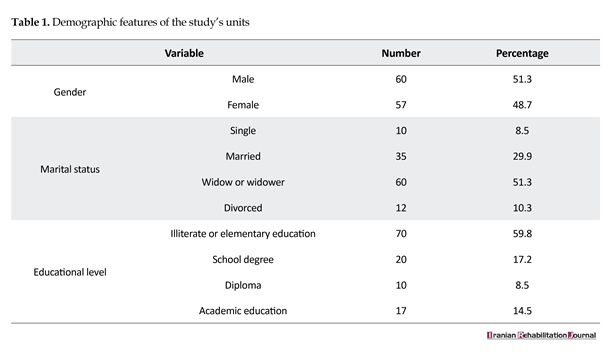
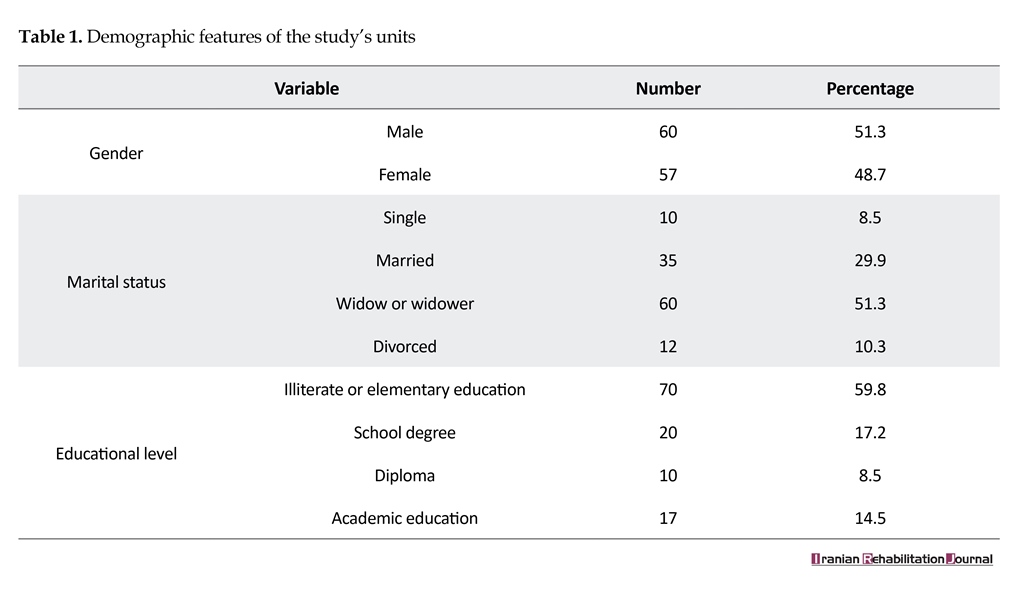
In this study, 117 elderly people with the average age of 71.68±9.24 years were taken into consideration. As shown in Table 1, the number of men and women participating in this study were equal. Regarding the marital status, the majority of the individuals were widowed, and most of the participants were illiterate or with elementary education. (Demographic features of the samples taking part in the study are shown in Table 1.
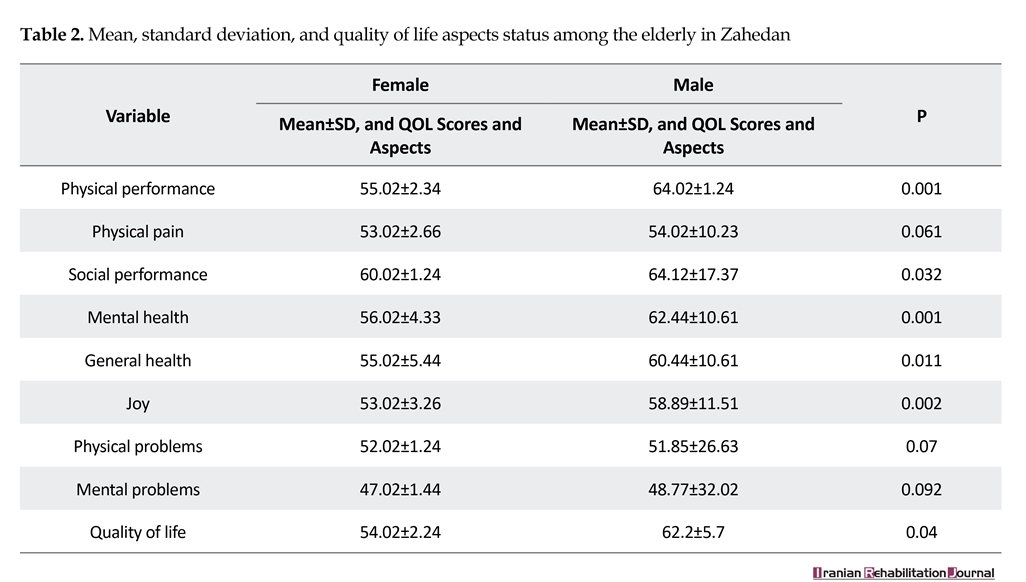
Results of the current study indicated that the mean score of quality of life of the elderly in this study was 57.2±6.7. The mean score of life quality in men and women was 62.52±6.7 and 51.2±6.7, respectively. Statistical independent t-test showed that quality of life in women was significantly lower than that in men (P=0.04). Quality of life score is related to marital status; that is widowed individuals had lower scores than married or single individuals (P=0.048). However, the quality of life score had no relationship with other demographic variables such as age and educational level (P˃0.05) (Table 2).
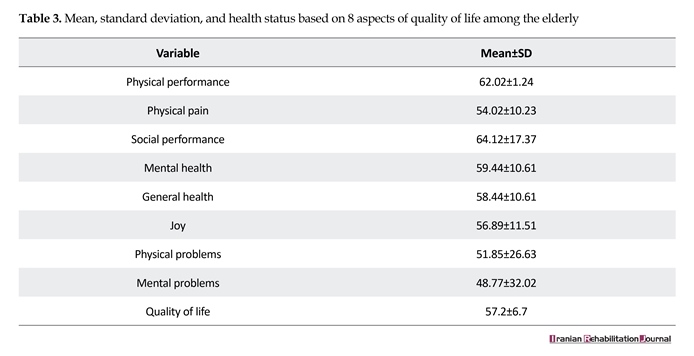
Furthermore, results of the current study revealed that the quality of life of the elderly is average. Generally, this means that quality of life is average in all aspects of their life except in their social performance. That is, in comparison with other aspects, the quality of life in social performance was in a better condition (Table 3).
4. Discussion
Since in our society, the basic index and normative criterion of the elderly people’s quality of life were not determined, therefore we assume this criterion to be from 0 to 100 regarding the present questionnaires. We can determine the average of 50 and standard deviation of 10 at the society’s normal index and an acceptable index for the elderly people’s quality of life status [13]. Therefore, in this study, the quality of life among the elderly is moderate which is confirmed by the results of other studies conducted, as well. Nejati and Ashayeri concluded that scores of all aspects of the elderly life quality are greater than 50 and it is something appropriate [14]. Moreover, Habibi Sola et al. found out that 60% of elderly people have good quality of life and the mean of their life quality is moderate [15]. However, some other studies indicate that the elderly quality of life in our country is not suitable and favorable.
Ahmadi et al. stated that quality of life among the elderly is lower than moderate and about 42% of them have disorder in their body systems, and 46% of them suffer from sleeping disorder (insomnia). All of these conditions have a negative effect on their quality of life [13]. Furthermore, in his study Nejati found out that about 86% of the elderly suffer from physical problems [16]. The score of women’s quality of life in this study is significantly lower than that of men. This finding matches the results of some other studies [6, 14, 15, 17]. However, in some other studies, it was reported that the men’s quality of life was at a higher level [18-22].
Moreover, in this study, the results of life quality had no significant relationship with educational level, but Habibi Sola et al. [15] and Aghanouri et al. showed that educational status has some relationship with quality of life of the elderly. That is, in most of the variables, people having an educational level above diploma degree had a higher quality of life than others [23]. This observed relationship between quality of life and educational level matches the
Aging of population or rapid increase in the number of the elderly is a global phenomenon. Decrease in childbearing capacity and increase in life expectancy has caused the elderly population to grow faster than the younger population [1]. Predictions indicate that the number of world’s elderly people will reach 1 billion in the year 2020. On an average 16% of the population in industrialized countries consist of elderly people and it is predicted that this rate will increase to 19% in future decades [2].
According to the reports of Statistical Center of Iran (SCI), in the census taken in 1385, the number of elderly people above 60 years old in Iran was 5.1 million, which makes 7.3% of the country’s population [3]. If this trend continues in Iran, we will, hereafter, have a population which is known as the elderly population [4]. Factors such as the increasing number of elderly people suffering from disability and functional disorder, lack of a supportive family system due to shrinking family size, women’s employment and jobs, and dispersion of family members will increase the need for long-term cares for the elderly in future decades [5].
Even though the main challenge of general health in the 20th century was “enhancing life expectancy”, the most important issue in this regard in the 21st century is “better quality life”. This is completely evident because elderly does not only mean having greater age and being alive, but their type and quality of life are very important issues too. Therefore, enhancing the quality of life of the elderly in the first instance, requires having comprehensive information about their quality of life [6].
Quality of life is the criterion for measuring the best energy or force in an individual. This force and energy are used for successful compatibility of an individual with the existing challenges. Various factors including shortages in elderly period, which cause a decrease in cognitive compatibility and decease in self-reliance can affect elderly people’s quality of life [7]. In general, aging can probably increase the affinity to some diseases and also lead to occurrence of disability during the final years of life [8]. In addition, the negative effects of aging on the ability to protect their independence will increase the need for assistance. The various problems and difficulties which occur physiologically during old age have some effect in decreasing the quality of life in that period.
In our country, Iran, about 28% of the elderly have limitations in performing physical activities independently, and they need help and assistance in order to do their usual daily activities. All these issues lead to decrease in quality of their life [9]. A study conducted on the elderly population of Tehran revealed a high rate of disability in them [10]. Since quality of life in this period of an individual’s life can easily be threatened, considering all the background factors in this regard that have a significance potential to influence [11].
2. Methods
This is a cross-sectional and correlational study which takes into account 117 elderly people above 60 years old residing in Zahedan. The sampling method in this study was population-based cluster random sampling. This means that area 2, 4, and 6 from among various areas in Zahedan (areas 1 to 6) were randomly selected on the map. Then, public places (mosques, parks, gyms, and shopping centers) and houses were recognized separately, so that in each area, one mosque, one park, and one shopping center were randomly selected. After that, the researcher with two other questioners who were trained in interviewing and filling the questionnaires went to these places and finally, 13 people from each public place were selected to take part in the study. Of course, the individuals had the required features for the study, and they were willing to participate. Meanwhile, physically disabled people were omitted from the study.
Data collection instrument was a questionnaire and the response to the question, inscribed questionnaire was written down and recorded by the researchers through interview. The criteria for entering into the study included having six months residency in the center, not having any chronic or acute diseases which are physically or mentally disabling, not having cognitive disorder, being literate or able to give interview. In order to account for the study’s ethical issues, a consent form was signed by each participant before filling in the questionnaire. Then, the questionnaire was given to each of them and they were informed about the study’s purposes and confidentiality of the obtained data.
The data collection instrument was a questionnaire on measuring the quality of life (SF-36) which consists of 36 questions and expressions on micro scales about physical performance, playing physical roles, body pain, general health, energy and joy, social performance, playing emotional role, and mental health. This is a standard questionnaire and has been validated in Iran [12]. The questionnaire was filled by the elderly participants themselves. Those who were illiterate or were not able to fill the form on their own were helped by trained questioners; the trained questioners helped the elderly fill the forms through interview. In order to determine the relationship between variables, we made use of Pearson correlation coefficient, independent t-test, and ANOVA. In addition, the data were analyzed by SPSS software, version 19.
3. Results
In this study, 117 elderly people with the average age of 71.68±9.24 years were taken into consideration. As shown in Table 1, the number of men and women participating in this study were equal. Regarding the marital status, the majority of the individuals were widowed, and most of the participants were illiterate or with elementary education. (Demographic features of the samples taking part in the study are shown in Table 1.
Results of the current study indicated that the mean score of quality of life of the elderly in this study was 57.2±6.7. The mean score of life quality in men and women was 62.52±6.7 and 51.2±6.7, respectively. Statistical independent t-test showed that quality of life in women was significantly lower than that in men (P=0.04). Quality of life score is related to marital status; that is widowed individuals had lower scores than married or single individuals (P=0.048). However, the quality of life score had no relationship with other demographic variables such as age and educational level (P˃0.05) (Table 2).
Furthermore, results of the current study revealed that the quality of life of the elderly is average. Generally, this means that quality of life is average in all aspects of their life except in their social performance. That is, in comparison with other aspects, the quality of life in social performance was in a better condition (Table 3).
4. Discussion
Since in our society, the basic index and normative criterion of the elderly people’s quality of life were not determined, therefore we assume this criterion to be from 0 to 100 regarding the present questionnaires. We can determine the average of 50 and standard deviation of 10 at the society’s normal index and an acceptable index for the elderly people’s quality of life status [13]. Therefore, in this study, the quality of life among the elderly is moderate which is confirmed by the results of other studies conducted, as well. Nejati and Ashayeri concluded that scores of all aspects of the elderly life quality are greater than 50 and it is something appropriate [14]. Moreover, Habibi Sola et al. found out that 60% of elderly people have good quality of life and the mean of their life quality is moderate [15]. However, some other studies indicate that the elderly quality of life in our country is not suitable and favorable.
Ahmadi et al. stated that quality of life among the elderly is lower than moderate and about 42% of them have disorder in their body systems, and 46% of them suffer from sleeping disorder (insomnia). All of these conditions have a negative effect on their quality of life [13]. Furthermore, in his study Nejati found out that about 86% of the elderly suffer from physical problems [16]. The score of women’s quality of life in this study is significantly lower than that of men. This finding matches the results of some other studies [6, 14, 15, 17]. However, in some other studies, it was reported that the men’s quality of life was at a higher level [18-22].
Moreover, in this study, the results of life quality had no significant relationship with educational level, but Habibi Sola et al. [15] and Aghanouri et al. showed that educational status has some relationship with quality of life of the elderly. That is, in most of the variables, people having an educational level above diploma degree had a higher quality of life than others [23]. This observed relationship between quality of life and educational level matches the
results of some other studies as well [24, 25]. Friedman et al. mentioned that illiterate individuals are not familiar enough with problem solving methods; moreover, in the majority of the cases, economical status of the illiterate individuals is not good enough and this issue can expose them to stressful conditions and therefore result in low quality of life [26]. Furthermore, aging phenomenon can lead to a decrease in quality of life in most aspects of life [13], but the current study did not confirm such a result.
Quality of life scores were associated with marital status; so the widowed individuals obtained less score than married or unmarried individuals (P=0.048). But in Hassani’s study [19], it was reported that unmarried men had a better quality of life and in Borhaninejad’s study, it was shown that married individuals had a better quality of life than widowed or unmarried individuals [20].
In addition, in a study conducted by Hagedoorn et al. on 1649 elderly people above 65 years of age, aiming at considering the effects of marital status on protection of the elderly against life pressures, it was concluded that married individuals tolerate less pressure than widows [27]. Other researchers have confirmed this finding as
Quality of life scores were associated with marital status; so the widowed individuals obtained less score than married or unmarried individuals (P=0.048). But in Hassani’s study [19], it was reported that unmarried men had a better quality of life and in Borhaninejad’s study, it was shown that married individuals had a better quality of life than widowed or unmarried individuals [20].
In addition, in a study conducted by Hagedoorn et al. on 1649 elderly people above 65 years of age, aiming at considering the effects of marital status on protection of the elderly against life pressures, it was concluded that married individuals tolerate less pressure than widows [27]. Other researchers have confirmed this finding as

well [8, 28]. Moreover, results of this study showed that the elderly people’s quality of life is average almost in all aspects of their life, but their social performance had a better condition.
In a study carried out on the elderly in Markazi province, Iran, Aghanouri et al. concluded that high scores of the elderly people’s quality of life belong to their social performance aspect (67.85±27) [11]. Similarly, in Farhady’s study, the highest score with regard to the elderly quality of life belonged to social performance aspect [29]. However, studying the life quality of elderly women, Sajadi and Beiglari came to this conclusion that from physical aspects, elderly women are in a good condition but from mental health perspective, they are at a moderate level [6].
5. Conclusion
Results of this study showed that the quality of life of the elderly people was average and their social performance was better than their physical health status. It was also seen that the quality of life was lower especially in elderly women; therefore, it is essential that more attention be paid to this group of the society.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors would like to thank all the participants for their cooperation during the collection of data.
Conflict of Interest
The authors declare that there is no conflicts of interest.
References
[1]Jadidi A, Farahaninia M, Janmohammadi S, Haghani H. [The relationship between spiritual well-being and quality of life among elderly people residing in Kahrizak senior house (Persian)]. Iran Journal of Nursing. 2011; 24(72):48-56.
[2]Tajvar M, Arab M, Montazeri A. Determinants of health-related quality of life in elderly in Tehran, Iran. BMC Public Health. 2008; 8(1):323. doi: 10.1186/1471-2458-8-323
[3]Khoshbin S. [World Health Organization Regional Office for Eastern Mediterranean. Active and healthy ageing and aged care strategy in the Eastern Mediterranean region (Persian)]. Tehran: Mezrab; 2010.
[4]Nejati V, Shirinbayan P, Akbari Kamrani A, Foroughan M, Taheri P, Sheikhvatan M. Quality of life in elderly people in Kashan, Iran. Middle East Journal of Age and Ageing. 2008; 5(2):21-5.
[5]Sadeghi M, Kazemi H. [Prevalence of dementia and depression in the elderly living in nursing homes in Tehran province (Persian)]. Iranian Journal of Psychiatry & Clinical Psychology. 2004; 9(4):49-55.
[6]Sajjadi H, Biglryian A. [Quality of life among elderly women in kahrizak charity foundation, Tehran, Iran (Persian)]. Payesh. 2007; 6(2):105-8.
[7]Tajvar M, Farziyanpour F. Elderly health and a review on different aspects of their life. Tehran: Nasle Farda; 2004.
[8]Alipoor F, Sajadi M, Foruzan A, Biglarian A, Jalilian A. [Elderly quality of life in Tehran's district two (Persian)]. Iranian Journal of Ageing. 2008; 3(3-4):75-83.
[9]Bize R, Johnson JA, Plotnikoff RC. Physical activity level and health-related quality of life in the general adult population: A systematic review. Preventive Medicine. 2007; 45(6):401-15. doi: 10.1016/j.ypmed.2007.07.017
[10]Shahbazi M, Mirkhani M, Hatamizadeh N, Rahgozar M. [Evaluation of disability in Tehran elderly (Persian)]. Iranian Journal of Ageing. 2009; 3(9):81-9.
[11]Vahdaninia M, Goshtasbi A, Montazeri A, Maftoun F. [Health-related quality of life in an elderly population in Iran: A population-based study (Persian)]. Payesh. 2005; 4(2):113-20.
[12]Karimlou M, Salehi M, Zayeri F, Massah O, Hatami A, Moosavy-Khattat M. [Developing the Persian version of the world health organization quality of life-100 questionnaire (Persian)]. Archives of Rehabilitation. 2011; 11(4):73-82.
[13]Ahmadi F, Salar A, Faghihzadeh S. [Quality of life in Zahedan elderly population (Persian)]. Journal of Hayat. 2004; 10(3):61-7.
[14]Nejati V, Ashayeri H. [Health related quality of life in the elderly in Kashan (Persian)]. Iranian Journal of Psychiatry and Clinical Psychology. 2008; 14(1):56-61.
[15]Habibi S, Nikpour S, Sohbatzadeh R, Haghani H. [Quality of life in elderly people of west of Tehran (Persian)]. Iranian Journal of Nursing Research. 2008; 2 (6-7):29-35
[16]Nejati V. [Assessing the health status of elderly people in the province of Qom (2007) (Persian)]. Journal of Qazvin University of Medical Sciences. 2009; 13(1):67-73.
[17]Litin CD, Trastek VF, Barthley HB. Mayo clinic. Mayo clinic family health book [M. Nasr Esfahani, A Bastani, A. Aziz Ahari, M. Rezaiean, Persian trans]. Tehran: Teimoorzadeh; 2000.
[18]Abdollahi F, Mohammadpour RA. [Health related quality of life among the elderly living in nursing home and homes (Persian)]. Journal of Mazandaran University of Medical Sciences. 2013; 23(104):20-5.
[19]Hasani F, Kamali M, Akbarfahimi M, Davatgaran K. [Factors affecting quality of life of the elderly in the residential homes of Tehran (2009) (Persian)]. Journal of Birjand University of Medical Sciences. 2011; 18(4):320-8.
[20]Borhaninejad V, Kazazi L, Haghi M, Chehrehnegar N. [Quality of life and its related factors among elderly with diabetes (Persian)]. Iranian Journal of Ageing. 2016; 11(1):162-73.
[21]Lima MG, Barros MBdA, César CLG, Goldbaum M, Carandina L, Ciconelli RM. Health related quality of life among the elderly: A population-based study using SF-36 survey. Cadernos de Saúde Pública. 2009; 25(10):2159-67. doi: 10.1590/s0102-311x2009001000007
[22]Hyttinen L, Kekäläinen P, Vuorio AF, Sintonen H, Strandberg TE. Health-related quality of life in elderly patients with familial hypercholesterolemia. International Journal of Technology Assessment in Health Care. 2008; 24(2):228-34. doi: 10.1017/s0266462308080318
[23]Agha nouri A, Mahmoudi M, Salehi H, Jafarian K. [Quality of life in the elderly people covered by health centers in the urban areas of Markazi Province, Iran (Persian)]. Iranian Journal of Ageing. 2012; 6(4):20-9.
[24]Bazrafshan MR, Hosseini M, Rahgozar M, Sadat Madah B. [Quality of elderly’s life in Shiraz, Jahandidegan club (Persian)]. Iranian Journal of Ageing. 2008; 3(1):33-41.
[25]Ahangari M, Kamali M, Arjmand Hesabi M. [The study of quality of life in the elderly with hypertension who are member of Tehran Senile Culture House Clubs (Persian)]. Iranian Journal of Ageing. 2008; 3(1):26-32.
[26]Friedman EM, Love GD, Rosenkranz MA, Urry HL, Davidson RJ, Singer BH, et al. Socioeconomic status predicts objective and subjective sleep quality in aging women. Psychosomatic Medicine. 2007; 69(7):682-91. doi: 10.1097/psy.0b013e31814ceada
[27]Hagedoorn M, Van Yperen NW, Coyne JC, Van Jaarsveld CH, Ranchor AV, van Sonderen E, et al. Does marriage protect older people from distress? The role of equity and recency of bereavement. Psychology and Aging. 2006; 21(3):611-20. doi: 10.1037/0882-7974.21.3.611
[28]Sato S, Demura S, Kobayashi H, Nagasawa Y. The relationship and its change with aging between ADL and daily life satisfaction characteristics in independent Japanese elderly living at home. Journal of Physiological Anthropology and Applied Human Science. 2002; 21(4):195-204. doi: 10.2114/jpa.21.195
[29]Farhadi A, Foroughan M, Mohammadi F. [The quality of life among rural elderlies a cross-sectional study (Persian)]. Iranian Journal of Ageing. 2011; 6(2):22-26.
In a study carried out on the elderly in Markazi province, Iran, Aghanouri et al. concluded that high scores of the elderly people’s quality of life belong to their social performance aspect (67.85±27) [11]. Similarly, in Farhady’s study, the highest score with regard to the elderly quality of life belonged to social performance aspect [29]. However, studying the life quality of elderly women, Sajadi and Beiglari came to this conclusion that from physical aspects, elderly women are in a good condition but from mental health perspective, they are at a moderate level [6].
5. Conclusion
Results of this study showed that the quality of life of the elderly people was average and their social performance was better than their physical health status. It was also seen that the quality of life was lower especially in elderly women; therefore, it is essential that more attention be paid to this group of the society.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors would like to thank all the participants for their cooperation during the collection of data.
Conflict of Interest
The authors declare that there is no conflicts of interest.
References
[1]Jadidi A, Farahaninia M, Janmohammadi S, Haghani H. [The relationship between spiritual well-being and quality of life among elderly people residing in Kahrizak senior house (Persian)]. Iran Journal of Nursing. 2011; 24(72):48-56.
[2]Tajvar M, Arab M, Montazeri A. Determinants of health-related quality of life in elderly in Tehran, Iran. BMC Public Health. 2008; 8(1):323. doi: 10.1186/1471-2458-8-323
[3]Khoshbin S. [World Health Organization Regional Office for Eastern Mediterranean. Active and healthy ageing and aged care strategy in the Eastern Mediterranean region (Persian)]. Tehran: Mezrab; 2010.
[4]Nejati V, Shirinbayan P, Akbari Kamrani A, Foroughan M, Taheri P, Sheikhvatan M. Quality of life in elderly people in Kashan, Iran. Middle East Journal of Age and Ageing. 2008; 5(2):21-5.
[5]Sadeghi M, Kazemi H. [Prevalence of dementia and depression in the elderly living in nursing homes in Tehran province (Persian)]. Iranian Journal of Psychiatry & Clinical Psychology. 2004; 9(4):49-55.
[6]Sajjadi H, Biglryian A. [Quality of life among elderly women in kahrizak charity foundation, Tehran, Iran (Persian)]. Payesh. 2007; 6(2):105-8.
[7]Tajvar M, Farziyanpour F. Elderly health and a review on different aspects of their life. Tehran: Nasle Farda; 2004.
[8]Alipoor F, Sajadi M, Foruzan A, Biglarian A, Jalilian A. [Elderly quality of life in Tehran's district two (Persian)]. Iranian Journal of Ageing. 2008; 3(3-4):75-83.
[9]Bize R, Johnson JA, Plotnikoff RC. Physical activity level and health-related quality of life in the general adult population: A systematic review. Preventive Medicine. 2007; 45(6):401-15. doi: 10.1016/j.ypmed.2007.07.017
[10]Shahbazi M, Mirkhani M, Hatamizadeh N, Rahgozar M. [Evaluation of disability in Tehran elderly (Persian)]. Iranian Journal of Ageing. 2009; 3(9):81-9.
[11]Vahdaninia M, Goshtasbi A, Montazeri A, Maftoun F. [Health-related quality of life in an elderly population in Iran: A population-based study (Persian)]. Payesh. 2005; 4(2):113-20.
[12]Karimlou M, Salehi M, Zayeri F, Massah O, Hatami A, Moosavy-Khattat M. [Developing the Persian version of the world health organization quality of life-100 questionnaire (Persian)]. Archives of Rehabilitation. 2011; 11(4):73-82.
[13]Ahmadi F, Salar A, Faghihzadeh S. [Quality of life in Zahedan elderly population (Persian)]. Journal of Hayat. 2004; 10(3):61-7.
[14]Nejati V, Ashayeri H. [Health related quality of life in the elderly in Kashan (Persian)]. Iranian Journal of Psychiatry and Clinical Psychology. 2008; 14(1):56-61.
[15]Habibi S, Nikpour S, Sohbatzadeh R, Haghani H. [Quality of life in elderly people of west of Tehran (Persian)]. Iranian Journal of Nursing Research. 2008; 2 (6-7):29-35
[16]Nejati V. [Assessing the health status of elderly people in the province of Qom (2007) (Persian)]. Journal of Qazvin University of Medical Sciences. 2009; 13(1):67-73.
[17]Litin CD, Trastek VF, Barthley HB. Mayo clinic. Mayo clinic family health book [M. Nasr Esfahani, A Bastani, A. Aziz Ahari, M. Rezaiean, Persian trans]. Tehran: Teimoorzadeh; 2000.
[18]Abdollahi F, Mohammadpour RA. [Health related quality of life among the elderly living in nursing home and homes (Persian)]. Journal of Mazandaran University of Medical Sciences. 2013; 23(104):20-5.
[19]Hasani F, Kamali M, Akbarfahimi M, Davatgaran K. [Factors affecting quality of life of the elderly in the residential homes of Tehran (2009) (Persian)]. Journal of Birjand University of Medical Sciences. 2011; 18(4):320-8.
[20]Borhaninejad V, Kazazi L, Haghi M, Chehrehnegar N. [Quality of life and its related factors among elderly with diabetes (Persian)]. Iranian Journal of Ageing. 2016; 11(1):162-73.
[21]Lima MG, Barros MBdA, César CLG, Goldbaum M, Carandina L, Ciconelli RM. Health related quality of life among the elderly: A population-based study using SF-36 survey. Cadernos de Saúde Pública. 2009; 25(10):2159-67. doi: 10.1590/s0102-311x2009001000007
[22]Hyttinen L, Kekäläinen P, Vuorio AF, Sintonen H, Strandberg TE. Health-related quality of life in elderly patients with familial hypercholesterolemia. International Journal of Technology Assessment in Health Care. 2008; 24(2):228-34. doi: 10.1017/s0266462308080318
[23]Agha nouri A, Mahmoudi M, Salehi H, Jafarian K. [Quality of life in the elderly people covered by health centers in the urban areas of Markazi Province, Iran (Persian)]. Iranian Journal of Ageing. 2012; 6(4):20-9.
[24]Bazrafshan MR, Hosseini M, Rahgozar M, Sadat Madah B. [Quality of elderly’s life in Shiraz, Jahandidegan club (Persian)]. Iranian Journal of Ageing. 2008; 3(1):33-41.
[25]Ahangari M, Kamali M, Arjmand Hesabi M. [The study of quality of life in the elderly with hypertension who are member of Tehran Senile Culture House Clubs (Persian)]. Iranian Journal of Ageing. 2008; 3(1):26-32.
[26]Friedman EM, Love GD, Rosenkranz MA, Urry HL, Davidson RJ, Singer BH, et al. Socioeconomic status predicts objective and subjective sleep quality in aging women. Psychosomatic Medicine. 2007; 69(7):682-91. doi: 10.1097/psy.0b013e31814ceada
[27]Hagedoorn M, Van Yperen NW, Coyne JC, Van Jaarsveld CH, Ranchor AV, van Sonderen E, et al. Does marriage protect older people from distress? The role of equity and recency of bereavement. Psychology and Aging. 2006; 21(3):611-20. doi: 10.1037/0882-7974.21.3.611
[28]Sato S, Demura S, Kobayashi H, Nagasawa Y. The relationship and its change with aging between ADL and daily life satisfaction characteristics in independent Japanese elderly living at home. Journal of Physiological Anthropology and Applied Human Science. 2002; 21(4):195-204. doi: 10.2114/jpa.21.195
[29]Farhadi A, Foroughan M, Mohammadi F. [The quality of life among rural elderlies a cross-sectional study (Persian)]. Iranian Journal of Ageing. 2011; 6(2):22-26.
Article type: Original Research Articles |
Subject:
Aging Studies
Received: 2016/11/1 | Accepted: 2017/07/30 | Published: 2017/10/2
Received: 2016/11/1 | Accepted: 2017/07/30 | Published: 2017/10/2
References
1. Jadidi A, Farahaninia M, Janmohammadi S, Haghani H. [The relationship between spiritual well-being and quality of life among elderly people residing in Kahrizak senior house (Persian)]. Iran Journal of Nursing. 2011; 24(72):48-56.
2. Tajvar M, Arab M, Montazeri A. Determinants of health-related quality of life in elderly in Tehran, Iran. BMC Public Health. 2008; 8(1):323. doi: 10.1186/1471-2458-8-323 [DOI:10.1186/1471-2458-8-323]
3. Khoshbin S. [World Health Organization Regional Office for Eastern Mediterranean. Active and healthy ageing and aged care strategy in the Eastern Mediterranean region (Persian)]. Tehran: Mezrab; 2010.
4. Nejati V, Shirinbayan P, Akbari Kamrani A, Foroughan M, Taheri P, Sheikhvatan M. Quality of life in elderly people in Kashan, Iran. Middle East Journal of Age and Ageing. 2008; 5(2):21-5.
5. Sadeghi M, Kazemi H. [Prevalence of dementia and depression in the elderly living in nursing homes in Tehran province (Persian)]. Iranian Journal of Psychiatry & Clinical Psychology. 2004; 9(4):49-55.
6. Sajjadi H, Biglryian A. [Quality of life among elderly women in kahrizak charity foundation, Tehran, Iran (Persian)]. Payesh. 2007; 6(2):105-8.
7. Tajvar M, Farziyanpour F. Elderly health and a review on different aspects of their life. Tehran: Nasle Farda; 2004.
8. Alipoor F, Sajadi M, Foruzan A, Biglarian A, Jalilian A. [Elderly quality of life in Tehran's district two (Persian)]. Iranian Journal of Ageing. 2008; 3(3-4):75-83.
9. Bize R, Johnson JA, Plotnikoff RC. Physical activity level and health-related quality of life in the general adult population: A systematic review. Preventive Medicine. 2007; 45(6):401-15. doi: 10.1016/j.ypmed.2007.07.017 [DOI:10.1016/j.ypmed.2007.07.017]
10. Shahbazi M, Mirkhani M, Hatamizadeh N, Rahgozar M. [Evaluation of disability in Tehran elderly (Persian)]. Iranian Journal of Ageing. 2009; 3(9):81-9.
11. Vahdaninia M, Goshtasbi A, Montazeri A, Maftoun F. [Health-related quality of life in an elderly population in Iran: A population-based study (Persian)]. Payesh. 2005; 4(2):113-20.
12. Karimlou M, Salehi M, Zayeri F, Massah O, Hatami A, Moosavy-Khattat M. [Developing the Persian version of the world health organization quality of life-100 questionnaire (Persian)]. Archives of Rehabilitation. 2011; 11(4):73-82.
13. Ahmadi F, Salar A, Faghihzadeh S. [Quality of life in Zahedan elderly population (Persian)]. Journal of Hayat. 2004; 10(3):61-7.
14. Nejati V, Ashayeri H. [Health related quality of life in the elderly in Kashan (Persian)]. Iranian Journal of Psychiatry and Clinical Psychology. 2008; 14(1):56-61.
15. Habibi S, Nikpour S, Sohbatzadeh R, Haghani H. [Quality of life in elderly people of west of Tehran (Persian)]. Iranian Journal of Nursing Research. 2008; 2 (6-7):29-35
16. Nejati V. [Assessing the health status of elderly people in the province of Qom (2007) (Persian)]. Journal of Qazvin University of Medical Sciences. 2009; 13(1):67-73.
17. Litin CD, Trastek VF, Barthley HB. Mayo clinic. Mayo clinic family health book [M. Nasr Esfahani, A Bastani, A. Aziz Ahari, M. Rezaiean, Persian trans]. Tehran: Teimoorzadeh; 2000. [PMID]
18. Abdollahi F, Mohammadpour RA. [Health related quality of life among the elderly living in nursing home and homes (Persian)]. Journal of Mazandaran University of Medical Sciences. 2013; 23(104):20-5.
19. Hasani F, Kamali M, Akbarfahimi M, Davatgaran K. [Factors affecting quality of life of the elderly in the residential homes of Tehran (2009) (Persian)]. Journal of Birjand University of Medical Sciences. 2011; 18(4):320-8.
20. Borhaninejad V, Kazazi L, Haghi M, Chehrehnegar N. [Quality of life and its related factors among elderly with diabetes (Persian)]. Iranian Journal of Ageing. 2016; 11(1):162-73.
21. Lima MG, Barros MBdA, César CLG, Goldbaum M, Carandina L, Ciconelli RM. Health related quality of life among the elderly: A population-based study using SF-36 survey. Cadernos de Saúde Pública. 2009; 25(10):2159-67. doi: 10.1590/s0102-311x2009001000007 [DOI:10.1590/S0102-311X2009001000007]
22. Hyttinen L, Kekäläinen P, Vuorio AF, Sintonen H, Strandberg TE. Health-related quality of life in elderly patients with familial hypercholesterolemia. International Journal of Technology Assessment in Health Care. 2008; 24(2):228-34. doi: 10.1017/s0266462308080318 [DOI:10.1017/S0266462308080318]
23. Agha nouri A, Mahmoudi M, Salehi H, Jafarian K. [Quality of life in the elderly people covered by health centers in the urban areas of Markazi Province, Iran (Persian)]. Iranian Journal of Ageing. 2012; 6(4):20-9.
24. Bazrafshan MR, Hosseini M, Rahgozar M, Sadat Madah B. [Quality of elderly's life in Shiraz, Jahandidegan club (Persian)]. Iranian Journal of Ageing. 2008; 3(1):33-41.
25. Ahangari M, Kamali M, Arjmand Hesabi M. [The study of quality of life in the elderly with hypertension who are member of Tehran Senile Culture House Clubs (Persian)]. Iranian Journal of Ageing. 2008; 3(1):26-32.
26. Friedman EM, Love GD, Rosenkranz MA, Urry HL, Davidson RJ, Singer BH, et al. Socioeconomic status predicts objective and subjective sleep quality in aging women. Psychosomatic Medicine. 2007; 69(7):682-91. doi: 10.1097/psy.0b013e31814ceada [DOI:10.1097/PSY.0b013e31814ceada]
27. Hagedoorn M, Van Yperen NW, Coyne JC, Van Jaarsveld CH, Ranchor AV, van Sonderen E, et al. Does marriage protect older people from distress? The role of equity and recency of bereavement. Psychology and Aging. 2006; 21(3):611-20. doi: 10.1037/0882-7974.21.3.611 [DOI:10.1037/0882-7974.21.3.611]
28. Sato S, Demura S, Kobayashi H, Nagasawa Y. The relationship and its change with aging between ADL and daily life satisfaction characteristics in independent Japanese elderly living at home. Journal of Physiological Anthropology and Applied Human Science. 2002; 21(4):195-204. doi: 10.2114/jpa.21.195 [DOI:10.2114/jpa.21.195]
29. Farhadi A, Foroughan M, Mohammadi F. [The quality of life among rural elderlies a cross-sectional study (Persian)]. Iranian Journal of Ageing. 2011; 6(2):22-26.
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
