
988368
Thu, Jul 30, 2026

Volume 16, Issue 1 (March 2018)
Iranian Rehabilitation Journal 2018, 16(1): 55-60 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Massah O, Bakhshi E, Shishehgar S, Moradi A. Gender Differences Among Patients With Hepatitis C Virus Undergoing Rehabilitation Through Methadone Maintenance Treatment. Iranian Rehabilitation Journal 2018; 16 (1) :55-60
URL: http://irj.uswr.ac.ir/article-1-760-en.html
URL: http://irj.uswr.ac.ir/article-1-760-en.html



1- Substance Abuse and Dependence Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Biostatistics, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Public Health, Faculty of Health, University of Technology Sydney, Sydney, Australia.
4- Department of Educational Psychology, Faculty of Educational Sciences and Psychology, Alzahra University, Tehran, Iran.
2- Department of Biostatistics, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Public Health, Faculty of Health, University of Technology Sydney, Sydney, Australia.
4- Department of Educational Psychology, Faculty of Educational Sciences and Psychology, Alzahra University, Tehran, Iran.
Full-Text [PDF 579 kb]
(2203 Downloads)
| Abstract (HTML) (8126 Views)
Full-Text: (1527 Views)
1. Introduction
Hepatitis C Virus (HCV) is a serious cause of chronic liver diseases, as well as the most common chronic blood borne infection in the world [1]. Overall, 170 million men and women are infected with HCV [2, 3]. About 70-80% of infected patients develop chronic infections, which lead to serious health problems [2-4]. Hepatitis C is very common in intravenous drug users in Iran [5, 6] and HCV is a serious health concern among methadone patients in Iran [7]. A study of 539 injection opiate users in methadone treatment indicated that all of them were HCV-infected. There was a significant relationship between the rate of HCV prevalence and sharing needles [8]. A study was conducted on 259 methadone patients. The HCV prevalence was 50%. The study indicated that the rate of unsafe drug injection and high risk sexual behaviors were lower among the participants after receiving the treatment. Furthermore, methadone treatment was an effective intervention to reduce HCV transmission [7].
Multiple reasons can increase HCV in methadone treatment. Some methadone patients are already infected with HCV at the time that they enter drug treatment. For others, the high prevalence of HCV ensures that even occasional risky drug use can lead to HCV. Other factors contributing to the HCV prevalence include an inadequate methadone dose [9]. Psychological problems have been frequently reported among methadone patients with HCV problem. A study of methadone patients indicated that depression, anxiety, fatigue and irritability were associated with the HCV prevalence. Patients with drug dependence had a high chance to discontinue HCV-treatment early in the first three treatment months [10]. A study of 3755 methadone patients with HCV problem indicated that 14% had received HCV treatment during the study period. Annual HCV treatment rates during methadone treatment ranged between 1.3% in 2005 and 2.6% in 2008 with no significant changes over time. HCV treatment uptake was associated with heavy benzodiazepine use for poor mental health [11]. This indicates an increased awareness for HCV and associated psychological problems among methadone patients [12].
To date, there are few studies about HCV problem among men and women in methadone treatment. The current study aimed to examine gender differences among a group of methadone patients with HCV problem. This was conducted in four domains: baseline characteristics, perceived stress, social support, coping strategies and mental health.
2. Methods
Study design and settings
A cross-sectional and multicenter study was designed. Nine methadone clinics in Tehran, Iran were the study sites. Overall, seven study sites were in middle socio-economic areas. Two of the study sites were women-only centers in low-socio-economic areas. The study was part of a larger study which was approved by University of Social Welfare and Rehabilitation Sciences.
Participants
Overall, 150 participants were randomly recruited. Overall, 15 or 16 male and female participants were recruited from each center. Following criteria were needed for recruitment: (1) reporting at least 18 years old; (2) being able to complete the study questionnaires; and (3) providing serological specimens for HCV. Furthermore, eligible candidates were needed to be in methadone treatment for at least one month. Participants were excluded if they reported severe drug withdrawal and/or intoxication symptoms at the time of interviewing. Fortunately, no participant was excluded from this study.
Questionnaires
Baseline Checklist (BC)
A checklist was designed to collect baseline characteristics and drug use details as well as current mental health status. The assessed reliability of the checklist in two weeks was (a=92) in this study.
Perceived Stress Scale (PSS)
The Persian version of the PSS was administered to collect data on stress. The PSS is a 10-item measure of perceived stress. The questionnaire has high reliability and validity [13]. The assessed reliability of the PSS in two weeks was (a=90) in this study.
Brief Cope Scale (BCS)
The Persian version of the BCS was administered to collect data on coping strategies. The BCS is a 28-item self-report measure of adaptive and maladaptive coping skills [14]. The assessed reliability of the BCS in two weeks was (a=91) in this study.
Social Support Survey (SSS)
The Persian version of the SSS was administered to collect data on social support. The questionnaire is a 13-item self-report measure of social support. The measure has four subscales-emotional/informational, tangible, affectionate, and positive social interaction-as well as an overall social support index [15]. The assessed reliability of the questionnaire in two weeks was (a=88) in this study.
Data analyses
Individual and demographic variables were examined by gender. Independent t-tests and Chi-square (χ²) tests were performed to analyze the data. All analyses were conducted using SPSS version 22 and statistical significance was set at P<0.05.
Study procedure
A total of 150 participants met the inclusion criteria and signed informed consent to enrol in the study. The study was conducted in a private interview room at each study site between July 2013 and June 2014. Participation was voluntary and confidential. Consent form was obtained from each participant. All participants had one hour interviews with two trained clinical psychologists to complete the questionnaires.
3. Results
Demographics
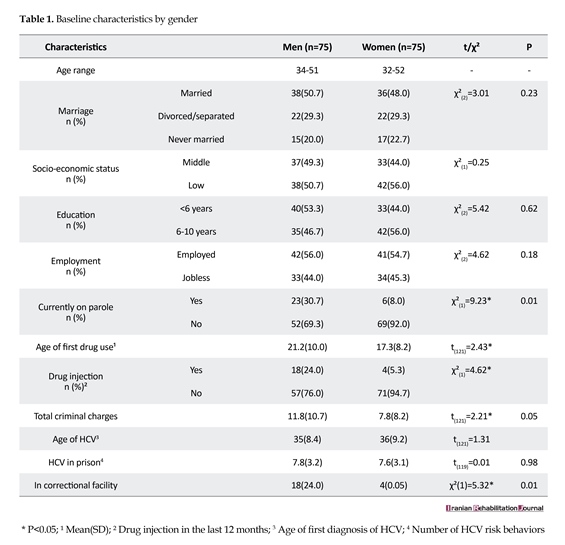
Participants were in the age range of 32-52 years. Demographic characteristics for men and women are presented in Table 1. Men were more likely to report being currently on parole than women (χ²(1)=9.23). Age of first illicit drug use was significantly lower among women than men (t(121)=2.43). Men were more likely to report drug injection in the last 12 months compared with women (χ²(1)=4.62). Men were more likely to report criminal charges (t(121)=2.21) and being in correctional facilities (χ²(1)=5.32) compared with women.
Psychological problems
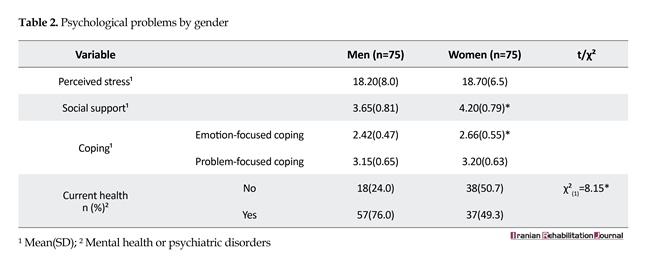
There were no gender differences in perceived stress. Despite women reporting more social support [4.20(0.79)], they also reported higher levels of emotion-focused coping [2.66(0.55)] than men. There was no effect of gender in problem-focused coping. Women were more likely to have a current mental health disorder (χ²(1)=8.15) (Table 2).
4. Discussion
Little research has examined gender differences among HCV-infected patients in methadone treatment. The present findings suggest that there were some differences among the baseline characteristics of the participants. Higher rates of current parole, drug injection, criminal charges and being in correctional facilities among men were considerable compared with women. In contrast, women reported lower ages of initial illicit drug use than men. Such characteristics were likely to contribute to engagement in high risk behaviors and the emergence of HCV prevalence among the participants. Furthermore, such characteristics may reduce positive treatment outcomes among the participants. This is consistent with previous studies which indicate that drug-dependent men with HCV problem have higher rates of criminality, drug injection, high risk behaviors and imprisonment [16-19]. Further studies are suggested.
The study findings indicated that there were no gender differences in perceived stress. Despite women reporting more social support, they also reported higher levels of emotion-focused coping than men. Furthermore, women were more likely to have a current mental health disorder. The reported psychological problems among these women may increase HCV problem. When considering treatment for HCV, particular attention must be paid to mental health conditions.
These study findings are consistent with some studies in other countries. A study of 111 patients showed high lifetime (82%) and current (57%) diagnosis rates of substance use disorders. Lifetime prevalence of any mood disorder was 67% while current prevalence of any mood disorder was 35%. Lifetime prevalence of any anxiety disorder was 63% while current prevalence of any mood disorder was 22%. A total of 66% of the patients received psychiatric medications prior to HCV treatment; more than half were receiving antidepressant medications. Overall, 15% of the patients were ineligible for HCV treatment due to psychiatric severity [20]. A study of Thai methadone clients indicated that depression was prevalent among HCV-infected patients. Positive HCV status and greater perceived stress were independently associated with depression [21]. A study of 576 methadone participants; 514 were HCV positive indicated high levels of anxiety (21.0%), depression (27.2%), attempted suicide (32.7%), and taking psychiatric medications (16.1%) [22]. The prevalence of psychological
Hepatitis C Virus (HCV) is a serious cause of chronic liver diseases, as well as the most common chronic blood borne infection in the world [1]. Overall, 170 million men and women are infected with HCV [2, 3]. About 70-80% of infected patients develop chronic infections, which lead to serious health problems [2-4]. Hepatitis C is very common in intravenous drug users in Iran [5, 6] and HCV is a serious health concern among methadone patients in Iran [7]. A study of 539 injection opiate users in methadone treatment indicated that all of them were HCV-infected. There was a significant relationship between the rate of HCV prevalence and sharing needles [8]. A study was conducted on 259 methadone patients. The HCV prevalence was 50%. The study indicated that the rate of unsafe drug injection and high risk sexual behaviors were lower among the participants after receiving the treatment. Furthermore, methadone treatment was an effective intervention to reduce HCV transmission [7].
Multiple reasons can increase HCV in methadone treatment. Some methadone patients are already infected with HCV at the time that they enter drug treatment. For others, the high prevalence of HCV ensures that even occasional risky drug use can lead to HCV. Other factors contributing to the HCV prevalence include an inadequate methadone dose [9]. Psychological problems have been frequently reported among methadone patients with HCV problem. A study of methadone patients indicated that depression, anxiety, fatigue and irritability were associated with the HCV prevalence. Patients with drug dependence had a high chance to discontinue HCV-treatment early in the first three treatment months [10]. A study of 3755 methadone patients with HCV problem indicated that 14% had received HCV treatment during the study period. Annual HCV treatment rates during methadone treatment ranged between 1.3% in 2005 and 2.6% in 2008 with no significant changes over time. HCV treatment uptake was associated with heavy benzodiazepine use for poor mental health [11]. This indicates an increased awareness for HCV and associated psychological problems among methadone patients [12].
To date, there are few studies about HCV problem among men and women in methadone treatment. The current study aimed to examine gender differences among a group of methadone patients with HCV problem. This was conducted in four domains: baseline characteristics, perceived stress, social support, coping strategies and mental health.
2. Methods
Study design and settings
A cross-sectional and multicenter study was designed. Nine methadone clinics in Tehran, Iran were the study sites. Overall, seven study sites were in middle socio-economic areas. Two of the study sites were women-only centers in low-socio-economic areas. The study was part of a larger study which was approved by University of Social Welfare and Rehabilitation Sciences.
Participants
Overall, 150 participants were randomly recruited. Overall, 15 or 16 male and female participants were recruited from each center. Following criteria were needed for recruitment: (1) reporting at least 18 years old; (2) being able to complete the study questionnaires; and (3) providing serological specimens for HCV. Furthermore, eligible candidates were needed to be in methadone treatment for at least one month. Participants were excluded if they reported severe drug withdrawal and/or intoxication symptoms at the time of interviewing. Fortunately, no participant was excluded from this study.
Questionnaires
Baseline Checklist (BC)
A checklist was designed to collect baseline characteristics and drug use details as well as current mental health status. The assessed reliability of the checklist in two weeks was (a=92) in this study.
Perceived Stress Scale (PSS)
The Persian version of the PSS was administered to collect data on stress. The PSS is a 10-item measure of perceived stress. The questionnaire has high reliability and validity [13]. The assessed reliability of the PSS in two weeks was (a=90) in this study.
Brief Cope Scale (BCS)
The Persian version of the BCS was administered to collect data on coping strategies. The BCS is a 28-item self-report measure of adaptive and maladaptive coping skills [14]. The assessed reliability of the BCS in two weeks was (a=91) in this study.
Social Support Survey (SSS)
The Persian version of the SSS was administered to collect data on social support. The questionnaire is a 13-item self-report measure of social support. The measure has four subscales-emotional/informational, tangible, affectionate, and positive social interaction-as well as an overall social support index [15]. The assessed reliability of the questionnaire in two weeks was (a=88) in this study.
Data analyses
Individual and demographic variables were examined by gender. Independent t-tests and Chi-square (χ²) tests were performed to analyze the data. All analyses were conducted using SPSS version 22 and statistical significance was set at P<0.05.
Study procedure
A total of 150 participants met the inclusion criteria and signed informed consent to enrol in the study. The study was conducted in a private interview room at each study site between July 2013 and June 2014. Participation was voluntary and confidential. Consent form was obtained from each participant. All participants had one hour interviews with two trained clinical psychologists to complete the questionnaires.
3. Results
Demographics
Participants were in the age range of 32-52 years. Demographic characteristics for men and women are presented in Table 1. Men were more likely to report being currently on parole than women (χ²(1)=9.23). Age of first illicit drug use was significantly lower among women than men (t(121)=2.43). Men were more likely to report drug injection in the last 12 months compared with women (χ²(1)=4.62). Men were more likely to report criminal charges (t(121)=2.21) and being in correctional facilities (χ²(1)=5.32) compared with women.
Psychological problems
There were no gender differences in perceived stress. Despite women reporting more social support [4.20(0.79)], they also reported higher levels of emotion-focused coping [2.66(0.55)] than men. There was no effect of gender in problem-focused coping. Women were more likely to have a current mental health disorder (χ²(1)=8.15) (Table 2).
4. Discussion
Little research has examined gender differences among HCV-infected patients in methadone treatment. The present findings suggest that there were some differences among the baseline characteristics of the participants. Higher rates of current parole, drug injection, criminal charges and being in correctional facilities among men were considerable compared with women. In contrast, women reported lower ages of initial illicit drug use than men. Such characteristics were likely to contribute to engagement in high risk behaviors and the emergence of HCV prevalence among the participants. Furthermore, such characteristics may reduce positive treatment outcomes among the participants. This is consistent with previous studies which indicate that drug-dependent men with HCV problem have higher rates of criminality, drug injection, high risk behaviors and imprisonment [16-19]. Further studies are suggested.
The study findings indicated that there were no gender differences in perceived stress. Despite women reporting more social support, they also reported higher levels of emotion-focused coping than men. Furthermore, women were more likely to have a current mental health disorder. The reported psychological problems among these women may increase HCV problem. When considering treatment for HCV, particular attention must be paid to mental health conditions.
These study findings are consistent with some studies in other countries. A study of 111 patients showed high lifetime (82%) and current (57%) diagnosis rates of substance use disorders. Lifetime prevalence of any mood disorder was 67% while current prevalence of any mood disorder was 35%. Lifetime prevalence of any anxiety disorder was 63% while current prevalence of any mood disorder was 22%. A total of 66% of the patients received psychiatric medications prior to HCV treatment; more than half were receiving antidepressant medications. Overall, 15% of the patients were ineligible for HCV treatment due to psychiatric severity [20]. A study of Thai methadone clients indicated that depression was prevalent among HCV-infected patients. Positive HCV status and greater perceived stress were independently associated with depression [21]. A study of 576 methadone participants; 514 were HCV positive indicated high levels of anxiety (21.0%), depression (27.2%), attempted suicide (32.7%), and taking psychiatric medications (16.1%) [22]. The prevalence of psychological


problems among this group demands a timely treatment [23]. There are many barriers to the treatment of HCV in addict patients in Iran [24] and their gender differences should be considered for therapeutic planning.
The current study had several limitations. First, the study was cross-sectional. Second, the study was limited to Tehran. Therefore, the study results may not be generalizable all HCV-infected methadone patients or other parts of Iran. Further studies with more male and female participants in other parts of Iran are suggested.
5. Conclusion
The study results indicated some gender differences in baseline characteristics and psychological problems among HCV-infected men and women. Such differences may have crucial impacts on methadone treatment outcomes. In summary, HCV is one of many challenges which must be met in the process of providing methadone treatment for opioid-dependent patients. Further research in gender differences, epidemiology and HCV treatment is essential if better methadone outcomes are to be achieved.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors would like to thank the study participants.
Conflict of Interest
The authors declared no conflicts of interest.
References
[1]Nelson PK, Mathers BM, Cowie B, Hagan H, Des Jarlais D, Horyniak D, et al. Global epidemiology of hepatitis B and hepatitis C in people who inject drugs: Results of systematic reviews. Lancet. 2011; 378(9791):571-83. Available from: http://dx.doi.org/10.1016/s0140-6736(11)61097-0
[2]Thein HH, Yi Q, Dore GJ, Krahn MD. Estimation of stage‐specific fibrosis progression rates in chronic hepatitis C virus infection: A meta‐analysis and meta‐regression. Hepatology. 2008; 48(2):418-31. Available from: http://dx.doi.org/10.1002/hep.22375
[3]Samimi-Rad K, Toosi MN, Masoudi-nejad A, Najafi A, Rahimnia R, Asgari F, et al. Molecular epidemiology of hepatitis C virus among injection drug users in Iran: a slight change in prevalence of HCV genotypes over time. Archives of Virology. 2012; 157(10):1959-65. Available from: http://dx.doi.org/10.1007/s00705-012-1369-9
[4]Kheirandish P, SeyedAlinaghi S, Jahani M, Shirzad H, Ahmadian MS, Majidi A, et al. Prevalence and correlates of hepatitis C infection among male injection drug users in detention, Tehran, Iran. Journal of Urban Health. 2009; 86(6):902-8. Available from: http://dx.doi.org/10.1007/s11524-009-9393-0
[5]Rezaie F, Noroozi A, Armoon B, Farhoudian A, Massah O, Sharifi H, et al. Social determinants and hepatitis C among people who inject drugs in Kermanshah, Iran: Socioeconomic status, homelessness, and sufficient syringe coverage. Journal of Substance Use. 2017; 22(5):474-78. Available from: http://dx.doi.org/10.1080/14659891.2016.1245793
[6]Alam-Mehrjerdi Z, Moradi A, Xu F, Zarghami M, Salehi-Fadardi J, Dolan K. Willingness to receive treatment for hepatitis c among injecting drug users on methadone program: implications for education and treatment. Addiction & Health. 2016; 8(2):90-7. PMID: 27882206
[7]Alavian SM, Mirahmadizadeh A, Javanbakht M, Keshtkaran A, Heidari A, Mashayekhi A, et al. Effectiveness of methadone maintenance treatment in prevention of hepatitis C virus transmission among injecting drug users. Hepatitis monthly. 2013; 13(8):e12411. Available from: http://dx.doi.org/doi: 10.5812/hepatmon.12411.
[8]Javadi A, Ataei B, Kassaian N, Nokhodian Z, Yaran M. Co-infection of human immunodeficiency virus, hepatitis C and hepatitis B virus among injection drug users in Drop in centers. International Journal of Research in Medical Sciences. 2014; 19(Suppl 1):17-21. PMCID: PMC4078381
[9]Strain EC, Bigelow GE, Liebson IA, Stitzer ML. Moderate-vs high-dose methadone in the treatment of opioid dependence: a randomized trial. JAMA. 1999; 281(11):1000-5. Available from: http://dx.doi.org/10.1001/jama.281.11.1000
[10]Schaefer M, Mauss S. Hepatitis C treatment in patients with drug addiction: Clinical management of interferon-alpha-associated psychiatric side effects. Current Drug Abuse Reviewse. 2008; 1(2):177-87. Available from: http://dx.doi.org/10.2174/1874473710801020177
[11]Pu L, Su Y, Wang G, Bai J. [Prevalence of HIV and HCV infections in patients receiving methadone maintenance treatment in Kaiyuan, Yunnan (Chinese)]. Zhonghua Liuxingbingxue Zazhi. 2015; 36(8):829-31. PMID: 26714537
[12]Midgard H, Bramness JG, Skurtveit S, Haukeland JW, Dalgard O. Hepatitis C treatment uptake among patients who have received opioid substitution treatment: A population-based study. PLOS ONE. 2016; 11(11):e0166451. Available from: http://dx.doi.org/10.1371/journal.pone.0166451
[13]Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of Health and Social Behavior. 1983; 24(4):385-96. Available from: http://dx.doi.org/10.2307/2136404
[14]Carver CS. You want to measure coping but your protocol’too long: Consider the brief cope. International journal of behavioral medicine. 1997; 4(1):92-100. Available from: http://dx.doi.org/10.1207/s15327558ijbm0401_6
[15]Sherbourne CD, Stewart AL. The MOS social support survey. Social Science & Medicine. 1991; 32(6):705-14. Available from: http://dx.doi.org/10.1016/0277-9536(91)90150-b
[16]Shi J, Zhao LY, Epstein DH, Zhao C, Shuai Y, Yan B, et al. The effect of methadone maintenance on illicit opioid use, human immunodeficiency virus and hepatitis C virus infection, health status, employment, and criminal activity among heroin abusers during 6 months of treatment in china. Journal of Addiction Medicine. 2007; 1(4):186-90. Available from: http://dx.doi.org/10.1097/adm.0b013e318156cc19
[17]Overbeck K, Dufour JF, Muellhaupt B, Helbling B, Borovicka J, Malinverni R, et al. Impact of international consensus guidelines on antiviral therapy of chronic hepatitis C patients in Switzerland. Swiss Medical Weekly. 2010; 140(9-10):146-52. Available from: http://dx.doi.org/smw-12928.
[18]Norouzian H, Gholami M, Shakib P, Goudarzi G, Diali HG, Rezvani A. Prevalence of HCV infections and co-infection with HBV and HIV and associated risk factors among addicts in drug treatment centers, Lorestan Province, Iran. International Journal of High Risk Behaviors and Addiction. 2016; 5(1): e25028. Available from: http://dx.doi.org/10.5812/ijhrba.25028
[19]Noroozi M, Mirzazadeh A, Noroozi A, Sharifi H, Higgs P, Jorjoran-Shushtari Z, et al. Injecting and sexual networks and sociodemographic factors and dual HIV risk among people who inject drugs: A cross-sectional study in Kermanshah Province, Iran. Addiction & Health. 2016; 8(3):186-94. PMID: 28496957
[20]Batki SL, Canfield KM, Ploutz‐Snyder R. Psychiatric and substance use disorders among methadone maintenance patients with chronic hepatitis C infection: effects on eligibility for hepatitis C treatment. The American Journal on Addictions. 2011; 20(4):312-8. Available from: http://dx.doi.org/10.1111/j.1521-0391.2011.00139.x
[21]Wang Z, Du J, Zhao M, Page K, Xiao Z, Mandel JS. Hepatitis C virus infection is independently associated with depression among methadone maintenance treatment heroin users in China. Asia‐Pacific Psychiatry. 2013; 5(3):191-6. Available from: http://dx.doi.org/10.1111/j.1758-5872.2012.00209.x
[22]Lee TSH, Shen HC, Wu WH, Huang CW, Yen MY, Wang BE, et al. Clinical characteristics and risk behavior as a function of HIV status among heroin users enrolled in methadone treatment in northern Taiwan. Substance Abuse Treatment, Prevention, and Policy. 2011; 6(1):6. Available from: http://dx.doi.org/10.1186/1747-597x-6-6
[23]Sakoman S. [Prevention and treatment of hepatitis C in illicit drug users (Croatian)]. Acta medica Croatica. 2009; 63(5):437-42. PMID: 20198904
[24]Massah O, Effatpanah M, Moradi A, Salehi M, Farhoudian A. Barriers to Hepatitis Treatment among Women in Methadone Treatment: A Study from Iran, the Most Populous Persian Gulf Country. Addiction and Health. In press.
The current study had several limitations. First, the study was cross-sectional. Second, the study was limited to Tehran. Therefore, the study results may not be generalizable all HCV-infected methadone patients or other parts of Iran. Further studies with more male and female participants in other parts of Iran are suggested.
5. Conclusion
The study results indicated some gender differences in baseline characteristics and psychological problems among HCV-infected men and women. Such differences may have crucial impacts on methadone treatment outcomes. In summary, HCV is one of many challenges which must be met in the process of providing methadone treatment for opioid-dependent patients. Further research in gender differences, epidemiology and HCV treatment is essential if better methadone outcomes are to be achieved.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors would like to thank the study participants.
Conflict of Interest
The authors declared no conflicts of interest.
References
[1]Nelson PK, Mathers BM, Cowie B, Hagan H, Des Jarlais D, Horyniak D, et al. Global epidemiology of hepatitis B and hepatitis C in people who inject drugs: Results of systematic reviews. Lancet. 2011; 378(9791):571-83. Available from: http://dx.doi.org/10.1016/s0140-6736(11)61097-0
[2]Thein HH, Yi Q, Dore GJ, Krahn MD. Estimation of stage‐specific fibrosis progression rates in chronic hepatitis C virus infection: A meta‐analysis and meta‐regression. Hepatology. 2008; 48(2):418-31. Available from: http://dx.doi.org/10.1002/hep.22375
[3]Samimi-Rad K, Toosi MN, Masoudi-nejad A, Najafi A, Rahimnia R, Asgari F, et al. Molecular epidemiology of hepatitis C virus among injection drug users in Iran: a slight change in prevalence of HCV genotypes over time. Archives of Virology. 2012; 157(10):1959-65. Available from: http://dx.doi.org/10.1007/s00705-012-1369-9
[4]Kheirandish P, SeyedAlinaghi S, Jahani M, Shirzad H, Ahmadian MS, Majidi A, et al. Prevalence and correlates of hepatitis C infection among male injection drug users in detention, Tehran, Iran. Journal of Urban Health. 2009; 86(6):902-8. Available from: http://dx.doi.org/10.1007/s11524-009-9393-0
[5]Rezaie F, Noroozi A, Armoon B, Farhoudian A, Massah O, Sharifi H, et al. Social determinants and hepatitis C among people who inject drugs in Kermanshah, Iran: Socioeconomic status, homelessness, and sufficient syringe coverage. Journal of Substance Use. 2017; 22(5):474-78. Available from: http://dx.doi.org/10.1080/14659891.2016.1245793
[6]Alam-Mehrjerdi Z, Moradi A, Xu F, Zarghami M, Salehi-Fadardi J, Dolan K. Willingness to receive treatment for hepatitis c among injecting drug users on methadone program: implications for education and treatment. Addiction & Health. 2016; 8(2):90-7. PMID: 27882206
[7]Alavian SM, Mirahmadizadeh A, Javanbakht M, Keshtkaran A, Heidari A, Mashayekhi A, et al. Effectiveness of methadone maintenance treatment in prevention of hepatitis C virus transmission among injecting drug users. Hepatitis monthly. 2013; 13(8):e12411. Available from: http://dx.doi.org/doi: 10.5812/hepatmon.12411.
[8]Javadi A, Ataei B, Kassaian N, Nokhodian Z, Yaran M. Co-infection of human immunodeficiency virus, hepatitis C and hepatitis B virus among injection drug users in Drop in centers. International Journal of Research in Medical Sciences. 2014; 19(Suppl 1):17-21. PMCID: PMC4078381
[9]Strain EC, Bigelow GE, Liebson IA, Stitzer ML. Moderate-vs high-dose methadone in the treatment of opioid dependence: a randomized trial. JAMA. 1999; 281(11):1000-5. Available from: http://dx.doi.org/10.1001/jama.281.11.1000
[10]Schaefer M, Mauss S. Hepatitis C treatment in patients with drug addiction: Clinical management of interferon-alpha-associated psychiatric side effects. Current Drug Abuse Reviewse. 2008; 1(2):177-87. Available from: http://dx.doi.org/10.2174/1874473710801020177
[11]Pu L, Su Y, Wang G, Bai J. [Prevalence of HIV and HCV infections in patients receiving methadone maintenance treatment in Kaiyuan, Yunnan (Chinese)]. Zhonghua Liuxingbingxue Zazhi. 2015; 36(8):829-31. PMID: 26714537
[12]Midgard H, Bramness JG, Skurtveit S, Haukeland JW, Dalgard O. Hepatitis C treatment uptake among patients who have received opioid substitution treatment: A population-based study. PLOS ONE. 2016; 11(11):e0166451. Available from: http://dx.doi.org/10.1371/journal.pone.0166451
[13]Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of Health and Social Behavior. 1983; 24(4):385-96. Available from: http://dx.doi.org/10.2307/2136404
[14]Carver CS. You want to measure coping but your protocol’too long: Consider the brief cope. International journal of behavioral medicine. 1997; 4(1):92-100. Available from: http://dx.doi.org/10.1207/s15327558ijbm0401_6
[15]Sherbourne CD, Stewart AL. The MOS social support survey. Social Science & Medicine. 1991; 32(6):705-14. Available from: http://dx.doi.org/10.1016/0277-9536(91)90150-b
[16]Shi J, Zhao LY, Epstein DH, Zhao C, Shuai Y, Yan B, et al. The effect of methadone maintenance on illicit opioid use, human immunodeficiency virus and hepatitis C virus infection, health status, employment, and criminal activity among heroin abusers during 6 months of treatment in china. Journal of Addiction Medicine. 2007; 1(4):186-90. Available from: http://dx.doi.org/10.1097/adm.0b013e318156cc19
[17]Overbeck K, Dufour JF, Muellhaupt B, Helbling B, Borovicka J, Malinverni R, et al. Impact of international consensus guidelines on antiviral therapy of chronic hepatitis C patients in Switzerland. Swiss Medical Weekly. 2010; 140(9-10):146-52. Available from: http://dx.doi.org/smw-12928.
[18]Norouzian H, Gholami M, Shakib P, Goudarzi G, Diali HG, Rezvani A. Prevalence of HCV infections and co-infection with HBV and HIV and associated risk factors among addicts in drug treatment centers, Lorestan Province, Iran. International Journal of High Risk Behaviors and Addiction. 2016; 5(1): e25028. Available from: http://dx.doi.org/10.5812/ijhrba.25028
[19]Noroozi M, Mirzazadeh A, Noroozi A, Sharifi H, Higgs P, Jorjoran-Shushtari Z, et al. Injecting and sexual networks and sociodemographic factors and dual HIV risk among people who inject drugs: A cross-sectional study in Kermanshah Province, Iran. Addiction & Health. 2016; 8(3):186-94. PMID: 28496957
[20]Batki SL, Canfield KM, Ploutz‐Snyder R. Psychiatric and substance use disorders among methadone maintenance patients with chronic hepatitis C infection: effects on eligibility for hepatitis C treatment. The American Journal on Addictions. 2011; 20(4):312-8. Available from: http://dx.doi.org/10.1111/j.1521-0391.2011.00139.x
[21]Wang Z, Du J, Zhao M, Page K, Xiao Z, Mandel JS. Hepatitis C virus infection is independently associated with depression among methadone maintenance treatment heroin users in China. Asia‐Pacific Psychiatry. 2013; 5(3):191-6. Available from: http://dx.doi.org/10.1111/j.1758-5872.2012.00209.x
[22]Lee TSH, Shen HC, Wu WH, Huang CW, Yen MY, Wang BE, et al. Clinical characteristics and risk behavior as a function of HIV status among heroin users enrolled in methadone treatment in northern Taiwan. Substance Abuse Treatment, Prevention, and Policy. 2011; 6(1):6. Available from: http://dx.doi.org/10.1186/1747-597x-6-6
[23]Sakoman S. [Prevention and treatment of hepatitis C in illicit drug users (Croatian)]. Acta medica Croatica. 2009; 63(5):437-42. PMID: 20198904
[24]Massah O, Effatpanah M, Moradi A, Salehi M, Farhoudian A. Barriers to Hepatitis Treatment among Women in Methadone Treatment: A Study from Iran, the Most Populous Persian Gulf Country. Addiction and Health. In press.
Article type: Original Research Articles |
Subject:
Addiction
Received: 2017/09/4 | Accepted: 2018/01/3 | Published: 2018/03/1
Received: 2017/09/4 | Accepted: 2018/01/3 | Published: 2018/03/1
References
1. Nelson PK, Mathers BM, Cowie B, Hagan H, Des Jarlais D, Horyniak D, et al. Global epidemiology of hepatitis B and hepatitis C in people who inject drugs: Results of systematic reviews. Lancet. 2011; 378(9791):571-83. Available from: http://dx.doi.org/10.1016/s0140-6736(11)61097-0 [DOI:10.1016/S0140-6736(11)61097-0]
2. Thein HH, Yi Q, Dore GJ, Krahn MD. Estimation of stage‐specific fibrosis progression rates in chronic hepatitis C virus infection: A meta‐analysis and meta‐regression. Hepatology. 2008; 48(2):418-31. Available from: http://dx.doi.org/10.1002/hep.22375 [DOI:10.1002/hep.22375]
3. Samimi-Rad K, Toosi MN, Masoudi-nejad A, Najafi A, Rahimnia R, Asgari F, et al. Molecular epidemiology of hepatitis C virus among injection drug users in Iran: a slight change in prevalence of HCV genotypes over time. Archives of Virology. 2012; 157(10):1959-65. Available from: http://dx.doi.org/10.1007/s00705-012-1369-9 [DOI:10.1007/s00705-012-1369-9]
4. Kheirandish P, SeyedAlinaghi S, Jahani M, Shirzad H, Ahmadian MS, Majidi A, et al. Prevalence and correlates of hepatitis C infection among male injection drug users in detention, Tehran, Iran. Journal of Urban Health. 2009; 86(6):902-8. Available from: http://dx.doi.org/10.1007/s11524-009-9393-0 [DOI:10.1007/s11524-009-9393-0]
5. Rezaie F, Noroozi A, Armoon B, Farhoudian A, Massah O, Sharifi H, et al. Social determinants and hepatitis C among people who inject drugs in Kermanshah, Iran: Socioeconomic status, homelessness, and sufficient syringe coverage. Journal of Substance Use. 2017; 22(5):474-78. Available from: http://dx.doi.org/10.1080/14659891.2016.1245793 [DOI:10.1080/14659891.2016.1245793]
6. Alam-Mehrjerdi Z, Moradi A, Xu F, Zarghami M, Salehi-Fadardi J, Dolan K. Willingness to receive treatment for hepatitis c among injecting drug users on methadone program: implications for education and treatment. Addiction & Health. 2016; 8(2):90-7. PMID: 27882206 [PMID] [PMCID]
7. Alavian SM, Mirahmadizadeh A, Javanbakht M, Keshtkaran A, Heidari A, Mashayekhi A, et al. Effectiveness of methadone maintenance treatment in prevention of hepatitis C virus transmission among injecting drug users. Hepatitis monthly. 2013; 13(8):e12411. Available from: http://dx.doi.org/doi: 10.5812/hepatmon.12411. [DOI:10.5812/hepatmon.12411]
8. Javadi A, Ataei B, Kassaian N, Nokhodian Z, Yaran M. Co-infection of human immunodeficiency virus, hepatitis C and hepatitis B virus among injection drug users in Drop in centers. International Journal of Research in Medical Sciences. 2014; 19(Suppl 1):17-21. PMCID: PMC4078381
9. Strain EC, Bigelow GE, Liebson IA, Stitzer ML. Moderate-vs high-dose methadone in the treatment of opioid dependence: a randomized trial. JAMA. 1999; 281(11):1000-5. Available from: http://dx.doi.org/10.1001/jama.281.11.1000 [DOI:10.1001/jama.281.11.1000]
10. Schaefer M, Mauss S. Hepatitis C treatment in patients with drug addiction: Clinical management of interferon-alpha-associated psychiatric side effects. Current Drug Abuse Reviewse. 2008; 1(2):177-87. Available from: http://dx.doi.org/10.2174/1874473710801020177 [DOI:10.2174/1874473710801020177]
11. Pu L, Su Y, Wang G, Bai J. [Prevalence of HIV and HCV infections in patients receiving methadone maintenance treatment in Kaiyuan, Yunnan (Chinese)]. Zhonghua Liuxingbingxue Zazhi. 2015; 36(8):829-31. PMID: 26714537 [PMID]
12. Midgard H, Bramness JG, Skurtveit S, Haukeland JW, Dalgard O. Hepatitis C treatment uptake among patients who have received opioid substitution treatment: A population-based study. PLOS ONE. 2016; 11(11):e0166451. Available from: http://dx.doi.org/10.1371/journal.pone.0166451 [DOI:10.1371/journal.pone.0166451]
13. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of Health and Social Behavior. 1983; 24(4):385-96. Available from: http://dx.doi.org/10.2307/2136404 [DOI:10.2307/2136404]
14. Carver CS. You want to measure coping but your protocol'too long: Consider the brief cope. International journal of behavioral medicine. 1997; 4(1):92-100. Available from: http://dx.doi.org/10.1207/s15327558ijbm0401_6 [DOI:10.1207/s15327558ijbm0401_6]
15. Sherbourne CD, Stewart AL. The MOS social support survey. Social Science & Medicine. 1991; 32(6):705-14. Available from: http://dx.doi.org/10.1016/0277-9536(91)90150-b [DOI:10.1016/0277-9536(91)90150-B]
16. Shi J, Zhao LY, Epstein DH, Zhao C, Shuai Y, Yan B, et al. The effect of methadone maintenance on illicit opioid use, human immunodeficiency virus and hepatitis C virus infection, health status, employment, and criminal activity among heroin abusers during 6 months of treatment in china. Journal of Addiction Medicine. 2007; 1(4):186-90. Available from: http://dx.doi.org/10.1097/adm.0b013e318156cc19 [DOI:10.1097/ADM.0b013e318156cc19]
17. Overbeck K, Dufour JF, Muellhaupt B, Helbling B, Borovicka J, Malinverni R, et al. Impact of international consensus guidelines on antiviral therapy of chronic hepatitis C patients in Switzerland. Swiss Medical Weekly. 2010; 140(9-10):146-52. Available from: http://dx.doi.org/smw-12928. [PMID]
18. Norouzian H, Gholami M, Shakib P, Goudarzi G, Diali HG, Rezvani A. Prevalence of HCV infections and co-infection with HBV and HIV and associated risk factors among addicts in drug treatment centers, Lorestan Province, Iran. International Journal of High Risk Behaviors and Addiction. 2016; 5(1): e25028. Available from: http://dx.doi.org/10.5812/ijhrba.25028 [DOI:10.5812/ijhrba.25028]
19. Noroozi M, Mirzazadeh A, Noroozi A, Sharifi H, Higgs P, Jorjoran-Shushtari Z, et al. Injecting and sexual networks and sociodemographic factors and dual HIV risk among people who inject drugs: A cross-sectional study in Kermanshah Province, Iran. Addiction & Health. 2016; 8(3):186-94. PMID: 28496957 [PMID] [PMCID]
20. Batki SL, Canfield KM, Ploutz‐Snyder R. Psychiatric and substance use disorders among methadone maintenance patients with chronic hepatitis C infection: effects on eligibility for hepatitis C treatment. The American Journal on Addictions. 2011; 20(4):312-8. Available from: http://dx.doi.org/10.1111/j.1521-0391.2011.00139.x [DOI:10.1111/j.1521-0391.2011.00139.x]
21. Wang Z, Du J, Zhao M, Page K, Xiao Z, Mandel JS. Hepatitis C virus infection is independently associated with depression among methadone maintenance treatment heroin users in China. Asia‐Pacific Psychiatry. 2013; 5(3):191-6. Available from: http://dx.doi.org/10.1111/j.1758-5872.2012.00209.x [DOI:10.1111/j.1758-5872.2012.00209.x]
22. Lee TSH, Shen HC, Wu WH, Huang CW, Yen MY, Wang BE, et al. Clinical characteristics and risk behavior as a function of HIV status among heroin users enrolled in methadone treatment in northern Taiwan. Substance Abuse Treatment, Prevention, and Policy. 2011; 6(1):6. Available from: http://dx.doi.org/10.1186/1747-597x-6-6 [DOI:10.1186/1747-597X-6-6]
23. Sakoman S. [Prevention and treatment of hepatitis C in illicit drug users (Croatian)]. Acta medica Croatica. 2009; 63(5):437-42. PMID: 20198904 [PMID]
24. Massah O, Effatpanah M, Moradi A, Salehi M, Farhoudian A. Barriers to Hepatitis Treatment among Women in Methadone Treatment: A Study from Iran, the Most Populous Persian Gulf Country. Addiction and Health. In press.
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
