
988368
Sat, Jul 5, 2025

Volume 17, Issue 3 (September 2019)
Iranian Rehabilitation Journal 2019, 17(3): 215-224 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Chaudhary P, Hamdani N, Sharma P. The Effects of Visuomotor Training Using Pablo System on Hand Grip Strength and Wrist Movements in Adults and Elderly. Iranian Rehabilitation Journal 2019; 17 (3) :215-224
URL: http://irj.uswr.ac.ir/article-1-811-en.html
URL: http://irj.uswr.ac.ir/article-1-811-en.html



1- Department of Rehabilitation Sciences, School of Nursing Sciences and Allied Health, Jamia Hamdard University, New Delhi, India.
2- Delhi Commonwealth Women's Association Medical Center, Indian Head Injury Foundation, Zamrudpur, New Delhi, India.
2- Delhi Commonwealth Women's Association Medical Center, Indian Head Injury Foundation, Zamrudpur, New Delhi, India.
Keywords: Visuomotor training, Grip strength, Pablo system, Michigan hand outcome questionnaire, Computer-based rehabilitation, Elderly
Full-Text [PDF 3041 kb]
(2123 Downloads)
| Abstract (HTML) (5714 Views)

Full-Text: (1667 Views)
1. Introduction
isuomotor training can be defined as any kind of training or practice that integrates visual perception with the motor performance [1]. It can be provided in several ways, like computer-based techniques; with the advancement of technology, the use of such techniques has constantly increased in rehabilitation. These techniques can provide passive, active, or interactive therapy, depending on the capabilities of the patient. Such therapies offer active, challenging and real-time training along with virtual feedback, provided that the patient has cognitive skills [2]. Studies on stroke, cerebral palsy, traumatic brain injury, Parkinson disease, post hand surgery, and degenerative diseases like rheumatoid arthritis and osteoarthritis have already reported the usefulness of such interactive and active technology [2-9].
A study recognized visuomotor skills as efficient in rehabilitation. According to that study, skills can be acquired with motor training and the repetitive practice of tasks that will facilitate normal movements and posture.Voluntary movement requires normal sensorimotor control [10]. It consists of 3 processes; sensory feedback, central processing, and motor output. Sensory information from peripheral receptors travel as afferent input into central areas which process it [11]. This leads to neuromuscular responses for movement, stability, and motor control during activity. Trauma, underlying pathologies, as well as physiological and anatomical changes, can disrupt these sensorimotor processes [12, 13].
One example of such alteration is observed in the elderly population due to aging. This issue may delay the sensorimotor processing in this population; in turn, it can affect their performance in the functional Activities of Daily Living (ADLs) [14]. These factors consist of intrinsic ones, such as hormonal changes, metabolic and degenerative diseases, as well as extrinsic factors, like physical activity, nutrition, traumatic injury, etc. responsible for the delay [15]. The literature suggests that games positively affect biopsychological wellbeing of the elderly, and improve their participation in daily living activities [16].
The games also help in providing motor-cognitive and balance training for them that, along with exercises, motivates older adults to increase social interaction and participation in daily living activities [17]. It also provides an opportunity for sedentary older adults to remain active and engaged in activities [16]. Visuomotor training in old age population (≥60 years) will not stop the natural aging process of central and peripheral nervous systems; however, it could improve their performance, compared to those who do not engage in such activities [18].
Studies on the elderly population have extensively worked on grip strength, making it an important outcome measure and a predictor. In the present study, for the first time, we worked on the training of grip strength using game-based equipment, Pablo system [19-22]. Along with grip strength, wrist Range of Movement (ROM), and the scores of Michigan Hand Outcomes Questionnaire (MHQ) were also collected. The MHQ is a subjective measurement of 6 parameters of hand and wrist, as follows: function, ADLs, work, pain, aesthetics, and satisfaction.
2. Methods
Jamia Hamdard Institutional Ethics Committee approved the research. A total of 51 subjects participated in this study; of whom, 26 were assigned in group 1 (adults) aged 25-44 years and the rest in group 2 (elderly) aged 65-79 years. Right-handed subjects were recruited from the Indian Head Injury Foundation based in Delhi Commonwealth Women’s Association Medical Center, Zamrudpur, and Senior Citizen Welfare Association, Lajpat Nagar-II. The subjects were selected based on the age criteria, having Manual Muscle Testing (MMT), and Mini-Mental State Examination (MMSE) scores of ≥24, with normal, corrected to normal vision. MMT, as described by Daniels, assesses muscle strength [2, 23, 24].
The grading system is recorded from 0-5, where grades ≥3 indicate active movement against gravity. MMSE is a simple and brief examination of cognition based on 11 questions. This test was devised by Folstein and McHugh in 1975 [24]. People suffering from any medical conditions such as epilepsy, seizures, dementia, depression, diabetes, visual/ perceptual deficits, post-fracture/ surgery of upper limb, a previous history of neuromuscular/ orthopaedic dysfunction affecting hand strength/ upper limb movements, e.g. OA of hand/ wrist, etc [25-28]. suffering from severe osteoporosis especially in elderly, contractures/ spasticity were excluded from the study [25].
Pablo system [26] was used to provide visuomotor training. It is a game-based rehabilitation in one-dimensional as well as two-dimensional modules. The training through this equipment is based on the principles of motor learning [29]. The Pablo system has a handheld device, multi-ball, and multi-board systems with sensors to control the games. The handheld device was used for assessing as well as training in this study (Figure 1).
isuomotor training can be defined as any kind of training or practice that integrates visual perception with the motor performance [1]. It can be provided in several ways, like computer-based techniques; with the advancement of technology, the use of such techniques has constantly increased in rehabilitation. These techniques can provide passive, active, or interactive therapy, depending on the capabilities of the patient. Such therapies offer active, challenging and real-time training along with virtual feedback, provided that the patient has cognitive skills [2]. Studies on stroke, cerebral palsy, traumatic brain injury, Parkinson disease, post hand surgery, and degenerative diseases like rheumatoid arthritis and osteoarthritis have already reported the usefulness of such interactive and active technology [2-9].
A study recognized visuomotor skills as efficient in rehabilitation. According to that study, skills can be acquired with motor training and the repetitive practice of tasks that will facilitate normal movements and posture.Voluntary movement requires normal sensorimotor control [10]. It consists of 3 processes; sensory feedback, central processing, and motor output. Sensory information from peripheral receptors travel as afferent input into central areas which process it [11]. This leads to neuromuscular responses for movement, stability, and motor control during activity. Trauma, underlying pathologies, as well as physiological and anatomical changes, can disrupt these sensorimotor processes [12, 13].
One example of such alteration is observed in the elderly population due to aging. This issue may delay the sensorimotor processing in this population; in turn, it can affect their performance in the functional Activities of Daily Living (ADLs) [14]. These factors consist of intrinsic ones, such as hormonal changes, metabolic and degenerative diseases, as well as extrinsic factors, like physical activity, nutrition, traumatic injury, etc. responsible for the delay [15]. The literature suggests that games positively affect biopsychological wellbeing of the elderly, and improve their participation in daily living activities [16].
The games also help in providing motor-cognitive and balance training for them that, along with exercises, motivates older adults to increase social interaction and participation in daily living activities [17]. It also provides an opportunity for sedentary older adults to remain active and engaged in activities [16]. Visuomotor training in old age population (≥60 years) will not stop the natural aging process of central and peripheral nervous systems; however, it could improve their performance, compared to those who do not engage in such activities [18].
Studies on the elderly population have extensively worked on grip strength, making it an important outcome measure and a predictor. In the present study, for the first time, we worked on the training of grip strength using game-based equipment, Pablo system [19-22]. Along with grip strength, wrist Range of Movement (ROM), and the scores of Michigan Hand Outcomes Questionnaire (MHQ) were also collected. The MHQ is a subjective measurement of 6 parameters of hand and wrist, as follows: function, ADLs, work, pain, aesthetics, and satisfaction.
2. Methods
Jamia Hamdard Institutional Ethics Committee approved the research. A total of 51 subjects participated in this study; of whom, 26 were assigned in group 1 (adults) aged 25-44 years and the rest in group 2 (elderly) aged 65-79 years. Right-handed subjects were recruited from the Indian Head Injury Foundation based in Delhi Commonwealth Women’s Association Medical Center, Zamrudpur, and Senior Citizen Welfare Association, Lajpat Nagar-II. The subjects were selected based on the age criteria, having Manual Muscle Testing (MMT), and Mini-Mental State Examination (MMSE) scores of ≥24, with normal, corrected to normal vision. MMT, as described by Daniels, assesses muscle strength [2, 23, 24].
The grading system is recorded from 0-5, where grades ≥3 indicate active movement against gravity. MMSE is a simple and brief examination of cognition based on 11 questions. This test was devised by Folstein and McHugh in 1975 [24]. People suffering from any medical conditions such as epilepsy, seizures, dementia, depression, diabetes, visual/ perceptual deficits, post-fracture/ surgery of upper limb, a previous history of neuromuscular/ orthopaedic dysfunction affecting hand strength/ upper limb movements, e.g. OA of hand/ wrist, etc [25-28]. suffering from severe osteoporosis especially in elderly, contractures/ spasticity were excluded from the study [25].
Pablo system [26] was used to provide visuomotor training. It is a game-based rehabilitation in one-dimensional as well as two-dimensional modules. The training through this equipment is based on the principles of motor learning [29]. The Pablo system has a handheld device, multi-ball, and multi-board systems with sensors to control the games. The handheld device was used for assessing as well as training in this study (Figure 1).
An informed consent form was obtained from all study participants. Grip strength and wrist ROM were recorded using the equipment in sitting position with the shoulder in adduction and elbow flexed to 90˚ and forearm in a neutral position. A score of MHQ was taken based on the subjects’ responses to all 6 parameters in the context of hand and wrist. These 6 parameters were function, ADLs, work, pain, aesthetics, and satisfaction. MHQ probes both hands; however, it can be performed with one hand, depending on the objectives of the examiner. Items are scored on a 5-point Likert-type scale from 1 (very good/ not at all difficult/ always/ very mild/ very satisfied) to 5 (very poor/ very difficult/ never/ severe/ very dissatisfied) [30]. For all the parameters, the higher the score, the better the performance. After recording the responses, the raw score was converted to a scale from 0 to100 according to a scoring algorithm for each parameter [30].
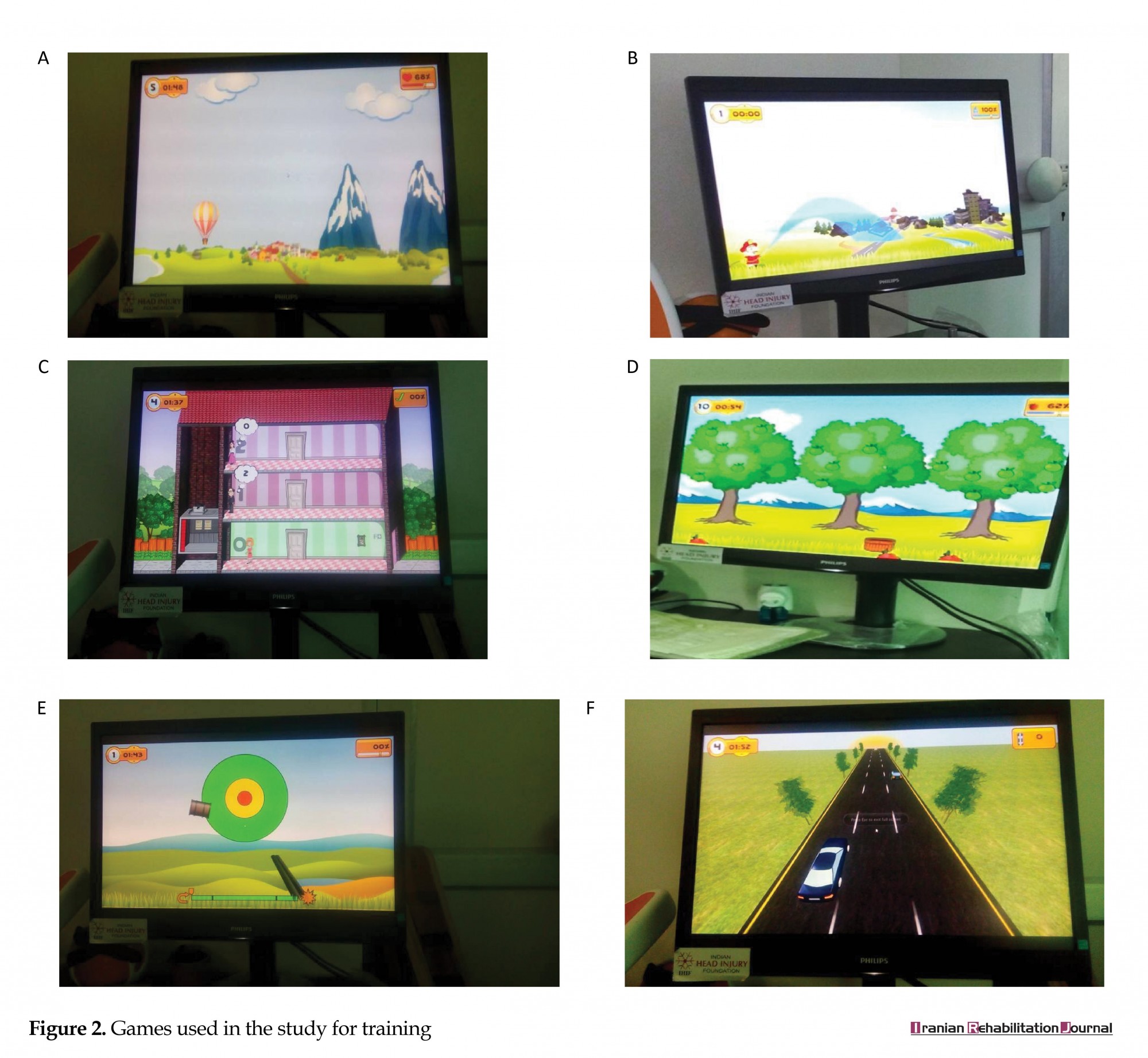
Once pre-training values of all the dependent variables were recorded, then the practice session was started. All 6 games used in training were practiced by the subjects for 3 min. From the next day, the intervention was started for 24 min (each game was randomly played for 3 min), 3 days a week. After 4 weeks, the values of grip strength, wrist ROM, and MHQ were recorded again. The 6 games used during the training were as follows (Figure 2): A. Hot air balloon: The balloon moves forward on its own. The main target is to move it up/ down trying not to collide it with mountains, birds, and helicopter appearing on the screen; B. Fire-fighter: The screen shows a fireman who has to extinguish the fire wherever it appears throughout the game; C. Elevator: The screen shows a lift on different floors. As soon as the game starts, people appear on different floors one by one; the main goal is to take the person to the floor he or she is indicating; D. Apple farmer: In this game, apple trees appear on the screen with a basket on the ground. The main aim is to collect all the apples in the basket by moving them to right-left directions; E. Shooting can: In the shooting game, the bullet must shoot the dart in the middle. Before shooting, the gun needs to be reloaded; F. Highway: It is a car game, where the main goal is to not collide the car with others coming in the way by moving it to the right-left direction [29].
Once pre-training values of all the dependent variables were recorded, then the practice session was started. All 6 games used in training were practiced by the subjects for 3 min. From the next day, the intervention was started for 24 min (each game was randomly played for 3 min), 3 days a week. After 4 weeks, the values of grip strength, wrist ROM, and MHQ were recorded again. The 6 games used during the training were as follows (Figure 2): A. Hot air balloon: The balloon moves forward on its own. The main target is to move it up/ down trying not to collide it with mountains, birds, and helicopter appearing on the screen; B. Fire-fighter: The screen shows a fireman who has to extinguish the fire wherever it appears throughout the game; C. Elevator: The screen shows a lift on different floors. As soon as the game starts, people appear on different floors one by one; the main goal is to take the person to the floor he or she is indicating; D. Apple farmer: In this game, apple trees appear on the screen with a basket on the ground. The main aim is to collect all the apples in the basket by moving them to right-left directions; E. Shooting can: In the shooting game, the bullet must shoot the dart in the middle. Before shooting, the gun needs to be reloaded; F. Highway: It is a car game, where the main goal is to not collide the car with others coming in the way by moving it to the right-left direction [29].
The first 3 games, i.e. “Hot air balloon”, “Fire-fighter”, and “Elevator” were controlled and played using the grip strength, while in the next three “Apple farmer, Shooting can, Highway”, wrist movements were used, i.e. flexion and extension.
The obtained data were analysed in GraphPad InStat. The One-Way Analysis of Variance (ANOVA) followed by Tukey-Kramer multiple comparison test was used to compare the pre-test and post-test scores, both within and between the groups. The data are expressed as Mean±SD, and q value is given along with it. (P˂0.05) was considered as statistically significant.
3. Results
Group 1 consisted of 16 females and 10 males with the Mean±SD age of 35.8±9 years. Group 2 consisted of 10 females and 15 males with the Mean±SD age of 68.5±7.2 years.
The obtained data were analysed in GraphPad InStat. The One-Way Analysis of Variance (ANOVA) followed by Tukey-Kramer multiple comparison test was used to compare the pre-test and post-test scores, both within and between the groups. The data are expressed as Mean±SD, and q value is given along with it. (P˂0.05) was considered as statistically significant.
3. Results
Group 1 consisted of 16 females and 10 males with the Mean±SD age of 35.8±9 years. Group 2 consisted of 10 females and 15 males with the Mean±SD age of 68.5±7.2 years.
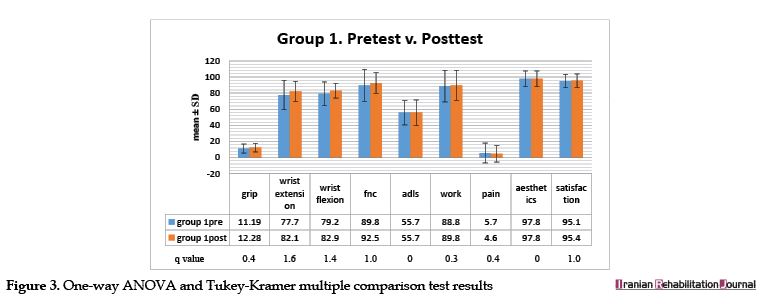
The pre-test-post-test within-group analysis of group 1 (adults) is shown in (Figure 3). There was an overall score improvement from pre-test to post-test in all the variables, except for ADLs and aesthetics. However, the change was not statistically significant in any parameter. ADLs and aesthetics showed no changes.
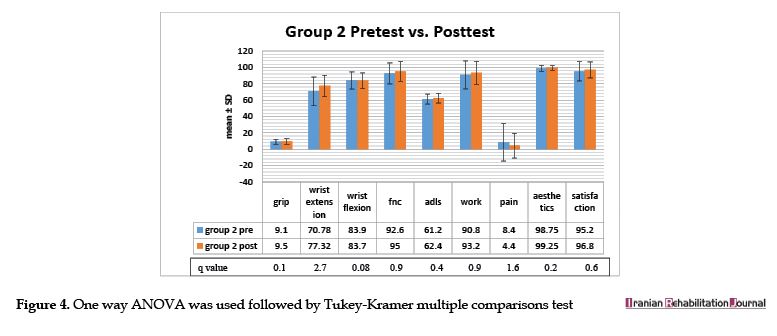
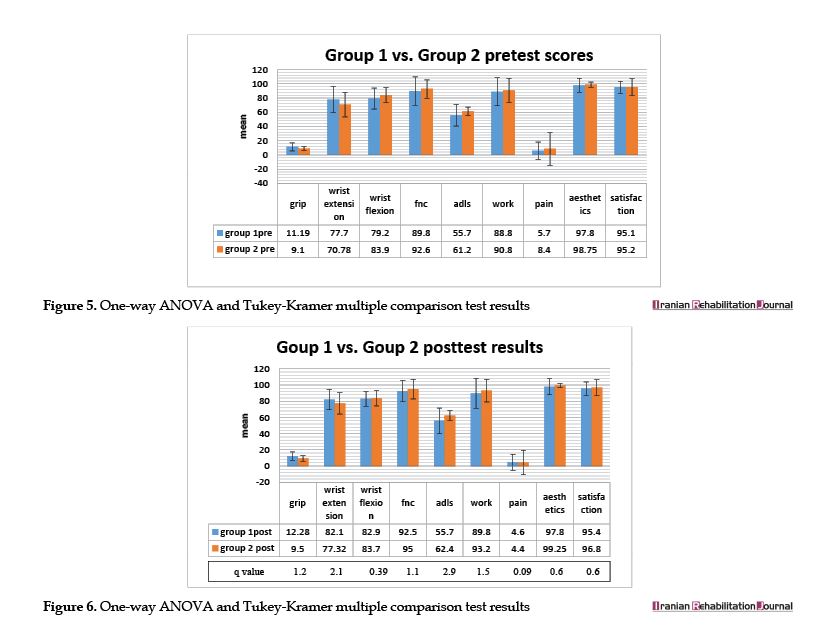
The within-group analysis in group 2 revealed an improvement in all the scores, except for wrist flexion, which decreased (Figure 4). The between-group analysis of pre-test scores of group 1 (adults) and group 2 (elderly) are presented in (Figure 5). The grip strength, wrist extension, and pain were better in adults, compared to the elderly, while wrist flexion, function, ADLs, work, and aesthetics were better in the elderly before the training.
The within-group analysis in group 2 revealed an improvement in all the scores, except for wrist flexion, which decreased (Figure 4). The between-group analysis of pre-test scores of group 1 (adults) and group 2 (elderly) are presented in (Figure 5). The grip strength, wrist extension, and pain were better in adults, compared to the elderly, while wrist flexion, function, ADLs, work, and aesthetics were better in the elderly before the training.
Satisfaction parameter difference was not high between the two groups. After the training (Figure 6), grip strength and wrist extension were better in the adults; however, pre-test values and scores of wrist flexion, function, ADLs, work, pain, aesthetics, and satisfaction were better in the elderly. No significant change was found in this area.
4. Discussion
The main aim of the present study was to compare the effect of visuomotor training in adults and the elderly. Visuomotor training can be defined as any training or practice that integrates visual perception with the motor performance [1]. Studies on the visuomotor training using game-based rehabilitation, non-immersive virtual reality, or robotic therapy have reported that it would provide neuroplasticity, cortical reorganization [28, 31], and would enhance brain reward system [31, 32]. This outcome is because it is based on motor learning approaches.
Thus, these are essential in rehabilitation, specially neurorehabilitation [8, 10, 28, 32-34]. The outcome variables were hand grip strength and wrist movements. These objective measures are assessed on Pablo system, while MHQ scores are subjective measures where subjects are asked about right hand and wrist regarding 6 parameters, i.e. function, ADLs, work, pain, aesthetics, and satisfaction.
A previous study indicated that the Pablo system could be efficiently used for evaluation and treatment. Therefore, we used the Pablo system to measure the grip strength and wrist range of motions (flexion and extension) [34]. It was concurrently used as treatment equipment for providing visuomotor training. The visuomotor training by Pablo Plus System provided visual and audio feedback. This multimode feedback reflects task progress and task completion, following rewarding model. According to Brailescu et al. and Nica et al. besides improvement in functional and quantitative scores, game-based training also enhances motivation and attention, in turn, it can improve the patient’s overall performance [8, 33].
We anticipated that training would positively affect both groups but in adults more due to age-related changes in elderly, leading to decreased performance levels [15, 35, 36]. The literature review shows extensive studies on the primary and secondary age-related changes. However, satisfactory prevention or intervention strategies have been overlooked [37, 38]. The present study mainly focused on two aspects; training through the Pablo system and the potential difference of this effect between the two different age groups (adults and elderly).
The results of the within-group 1 pre-test-post-test analysis suggested positive changes in the mean scores of grip strength, wrist ROM (flexion and extension), and MHQ. The lowest difference belonged to satisfaction, which is most probably due to initial high scores and besides satisfaction being a qualitative measure depending on everyone’s perception [39].
The within-group analysis in group 2 indicated the lowest difference in aesthetics parameter and highest in pain. The higher score of pain in the elderly group in pre-reading is quite possible due to degenerative changes like osteoarthritis. Performing light exercises help older adults regain their strength, which may not be too significant, but profoundly affects other parameters.
The between-group analysis indicated lower scores of grip strength, wrist extension, and function in the elderly. These results agree with the results of Puh et al., Lawrence et al., and Carmeli et al. [15, 19, 21]. However, the values of wrist flexion, ADLs, and work were higher compared to those in the adults, which needs to be clarified in future studies. Similarly, the aesthetics and satisfaction components higher scores in the elderly are most probably due to the contentedness and sense of wellbeing among them [40].
The small sample size, no control groups, and short training duration were some limitations of the study, as opposed to that by Brailescu et al. and Nica et al., respectively [13, 33]. Future studies are recommended with larger sample sizes, control groups, and incorporating other factors such as endurance, fatigue, error numbers, and reaction time.
5. Conclusion
The obtained data could be beneficial in overcoming the limitations of conventional protocols such as being time-consuming, requiring hard labor, lacking resource, needing intensive therapy, depending on patients’ cooperation and treatment adherence [31, 32]. It could also provide new insight into the rehabilitation, incorporating precise assessment and training methods with fun and challenging aspects. In addition, it will also help in providing cognitive training and can be used as an adjunct to conventional therapies.
Ethical Considerations
Compliance with ethical guidelines
This study was cleared by the Ethical Committee of Jamia Hamdard University and there were no ethical issues as such; A subject information sheet and a duly signed Informed consent was taken before each data collection
Funding
The paper was extracted from the dissertation of the first author, Department of Rehabilitation Sciences, School of Nursing Sciences and Allied Health, Jamia Hamdard University.
Authors' contributions
Conceptualization: Nusrat Hamdani; Methodology: Nusrat Hamdani, Preeti Chaudhary; Software validation, formal analysis, professional consultation, investigation, data collection: Preeti Chaudhary, Nusrat Hamdani; Original draft writing: Nusrat Hamdani, Preeti Chaudhary; Review and editing: Nusrat Hamdani; Supervision: Nusrat Hamdani, Prateek Sharma.
Conflict of interest
Authors declare no conflicts of interests.
Acknowledgments
Authors are thankful to the University, Faculty Members, students, and other staff in the Department of Rehabilitation Sciences, for supporting the research. We also appreciate IHIF (Indian Head Injury Foundation) based DCWA (Delhi Commonwealth Women’s Association) center at Zamrudpur where the data collection was performed.
References
The main aim of the present study was to compare the effect of visuomotor training in adults and the elderly. Visuomotor training can be defined as any training or practice that integrates visual perception with the motor performance [1]. Studies on the visuomotor training using game-based rehabilitation, non-immersive virtual reality, or robotic therapy have reported that it would provide neuroplasticity, cortical reorganization [28, 31], and would enhance brain reward system [31, 32]. This outcome is because it is based on motor learning approaches.
Thus, these are essential in rehabilitation, specially neurorehabilitation [8, 10, 28, 32-34]. The outcome variables were hand grip strength and wrist movements. These objective measures are assessed on Pablo system, while MHQ scores are subjective measures where subjects are asked about right hand and wrist regarding 6 parameters, i.e. function, ADLs, work, pain, aesthetics, and satisfaction.
A previous study indicated that the Pablo system could be efficiently used for evaluation and treatment. Therefore, we used the Pablo system to measure the grip strength and wrist range of motions (flexion and extension) [34]. It was concurrently used as treatment equipment for providing visuomotor training. The visuomotor training by Pablo Plus System provided visual and audio feedback. This multimode feedback reflects task progress and task completion, following rewarding model. According to Brailescu et al. and Nica et al. besides improvement in functional and quantitative scores, game-based training also enhances motivation and attention, in turn, it can improve the patient’s overall performance [8, 33].
We anticipated that training would positively affect both groups but in adults more due to age-related changes in elderly, leading to decreased performance levels [15, 35, 36]. The literature review shows extensive studies on the primary and secondary age-related changes. However, satisfactory prevention or intervention strategies have been overlooked [37, 38]. The present study mainly focused on two aspects; training through the Pablo system and the potential difference of this effect between the two different age groups (adults and elderly).
The results of the within-group 1 pre-test-post-test analysis suggested positive changes in the mean scores of grip strength, wrist ROM (flexion and extension), and MHQ. The lowest difference belonged to satisfaction, which is most probably due to initial high scores and besides satisfaction being a qualitative measure depending on everyone’s perception [39].
The within-group analysis in group 2 indicated the lowest difference in aesthetics parameter and highest in pain. The higher score of pain in the elderly group in pre-reading is quite possible due to degenerative changes like osteoarthritis. Performing light exercises help older adults regain their strength, which may not be too significant, but profoundly affects other parameters.
The between-group analysis indicated lower scores of grip strength, wrist extension, and function in the elderly. These results agree with the results of Puh et al., Lawrence et al., and Carmeli et al. [15, 19, 21]. However, the values of wrist flexion, ADLs, and work were higher compared to those in the adults, which needs to be clarified in future studies. Similarly, the aesthetics and satisfaction components higher scores in the elderly are most probably due to the contentedness and sense of wellbeing among them [40].
The small sample size, no control groups, and short training duration were some limitations of the study, as opposed to that by Brailescu et al. and Nica et al., respectively [13, 33]. Future studies are recommended with larger sample sizes, control groups, and incorporating other factors such as endurance, fatigue, error numbers, and reaction time.
5. Conclusion
The obtained data could be beneficial in overcoming the limitations of conventional protocols such as being time-consuming, requiring hard labor, lacking resource, needing intensive therapy, depending on patients’ cooperation and treatment adherence [31, 32]. It could also provide new insight into the rehabilitation, incorporating precise assessment and training methods with fun and challenging aspects. In addition, it will also help in providing cognitive training and can be used as an adjunct to conventional therapies.
Ethical Considerations
Compliance with ethical guidelines
This study was cleared by the Ethical Committee of Jamia Hamdard University and there were no ethical issues as such; A subject information sheet and a duly signed Informed consent was taken before each data collection
Funding
The paper was extracted from the dissertation of the first author, Department of Rehabilitation Sciences, School of Nursing Sciences and Allied Health, Jamia Hamdard University.
Authors' contributions
Conceptualization: Nusrat Hamdani; Methodology: Nusrat Hamdani, Preeti Chaudhary; Software validation, formal analysis, professional consultation, investigation, data collection: Preeti Chaudhary, Nusrat Hamdani; Original draft writing: Nusrat Hamdani, Preeti Chaudhary; Review and editing: Nusrat Hamdani; Supervision: Nusrat Hamdani, Prateek Sharma.
Conflict of interest
Authors declare no conflicts of interests.
Acknowledgments
Authors are thankful to the University, Faculty Members, students, and other staff in the Department of Rehabilitation Sciences, for supporting the research. We also appreciate IHIF (Indian Head Injury Foundation) based DCWA (Delhi Commonwealth Women’s Association) center at Zamrudpur where the data collection was performed.
References
- Stevens A, Bernier R. Visual-motor function. In: Volkmar FR, editor. Encyclopaedia of Autism Spectrum Disorders. New York: Springer; 2012. [DOI: 10.1007/978-1-4419-1698-3]
- Moser B, Kollreider A, Ram D. Advanced hand function training and evaluation. Graz: Tyromotion; 2010.
- Boian R, Sharma A, Han C, Merians A, Burdea G, Adamovich S, et al. Virtual reality-based post stroke hand rehabilitation. Studies in Health Technology and Informatics. 2000; 85: 64-70. [PMID]
- Holden MK, Dyar TA, Schwamm L, Bizzi E. Virtual environment- based telerehabilitation in patients with stroke. Presence. 2005; 14:214-33. [DOI:10.1162/1054746053967058]
- Howcroft J, Klejman S, Fehlings D, Wright V, Zabjek K, Andrysek J, et al. Active video game play in children with cerebral palsy: Potential for physical activity promotion and rehabilitation therapies. Archives of Physical Medicine and Rehabilitation. 2012; 93(8):1448-56. [DOI:10.1016/j.apmr.2012.02.033] [PMID]
- Gil-Gomez JA, Llorens R, Alcaniz M, Colomer C. Effectiveness of a Wii balance board-based system (eBaViR) for balance rehabilitation: A pilot randomized clinical trial in patients with acquired brain injury. Journal of NeuroEngineering and Rehabilitation. 2011; 8:30. [DOI:10.1186/1743-0003-8-30] [PMID] [PMCID]
- Esculier JF, Vaudrin J, Beriault P, Gagnon K, Tremblay LE. Home-based balance training programme using Wii Fit with balance board for Parkinsons’s disease: A pilot study. Journal of Rehabilitation Medicine. 2012; 44:144-150. [DOI:10.2340/16501977-0922] [PMID]
- Brăilescu C, Scarlet R, Nica A, Lascăr I. A study regarding the results of a rehabilitation program in patients with traumatic lesions of the hand after surgery. Civilization and Sport. 2013; 14(4):263-70.
- Srikesavan CS, Shay B, Robinson DB, Szturm T. Task-oriented training with computer gaming in people with rheumatoid arthritis or osteoarthritis of the hand: Study protocol of a randomized controlled pilot trial. Trials. 2013; 14:69. [DOI:10.1186/1745-6215-14-69] [PMID] [PMCID]
- Seitz RJ, Kammerzell A, Samartzi M, Jander S, Wojtecki L, Verschure PFMJ, et al. Monitoring of visuomotor coordination in healthy subjects and patients with stroke and Parkinson’s disease: An application study using the PABLOR-Device. International Journal of Neurorehabilitation. 2014; 1:113. [DOI:10.4172/2376-0281.1000113]
- Proske U, Gandevia SC. The kinaesthetic senses. The Journal of Physiology. 2009; 587:4139-46. [DOI:10.1113/jphysiol.2009.175372] [PMID] [PMCID]
- Riemann BL, Lephart SM. The sensorimotor system part 1: The physiologic basis of functional joint stability. Journal of Athletic Training. 2002; 37(1):71-9. [PMID] [PMCID]
- Karagiannopoulos C, Michlovitz S. Rehabilitation strategies for wrist sensorimotor control impairement: From theory to practice. Journal of Hand Therapy. 2016; 29(2):154-65. [DOI:10.1016/j.jht.2015.12.003] [PMID]
- McNay EC, Willingham DB. Deficit in learning of a motor skill requiring strategy, but not of perceptuomotor recalibration, with aging. Learning & Memory. 1998; 4(5):411-20. [DOI:10.1101/lm.4.5.411] [PMID]
- Carmeli E, Patish H & Coleman R. The aging hand. The Journals of Gerontology. 2003; 58(2):146-52. [DOI:10.1093/gerona/58.2.M146] [PMID]
- Gerling KM, Livingston IJ, Nacke LE, Mandryk RL. Full-body motion-based game interaction for older adults. Journal of the ACM. 2012; 1873-82. [DOI:10.1145/2207676.2208324]
- Krakauer JW. Motor learning and consolidation: The case of visuomotor rotation. Advances in Experimental Medicine and Biology. 2009; 629:405-21. [DOI:10.1007/978-0-387-77064-2_21] [PMID] [PMCID]
- Rowe JW, Kahn RL. Successful aging. Gerontologist. 1997; 37:433-40. [DOI:10.1093/geront/37.4.433] [PMID]
- Puh U. Age-related and sex-related differences in hand and pinch grip strength in adults. International Journal of Rehabilitation Research. 2010; 33(1):4-11. [DOI:10.1097/MRR.0b013e328325a8ba] [PMID]
- Taekema DG, Gussekloo J, Maier AB, Westendrop RG, de Craen AJ. Handgrip strength as a predictor of functional, psychological and social health: A prospective population-based study among the oldest old. Age and Ageing. 2010; 39(3):331-7. [DOI:10.1093/ageing/afq022] [PMID]
- Lawrence EL, Dayanidhi S, Fassola I, Requejo P, Leclercq C, Winstein CJ, et al. Outcome measures for hand function naturally reveal three latent domains in older adults: Strength, coordinated upper extremity function, and sensorimotor processing. Frontiers in Aging Neuroscience. 2015; 7:108. [DOI:10.3389/fnagi.2015.00108] [PMID] [PMCID]
- Bohannon RW. Hand grip dynamometry predicts future outcomes in aging adults. Journal of Geriatric Physical Therapy. 2008; 31(1):3-10. [DOI:10.1519/00139143-200831010-00002] [PMID]
- Hislop HJ, Montgomery JM. Daniels and worthingham’s muscle testing. Amsterdam: Elsevier; 2007.
- Folstein MF, Folstein SE, McHugh PR. Mini-mental state: A practical method for grading the state of patients for the clinician. Journal of Psychiatric Research. 1975; 12(3):189-98. [DOI:10.1016/0022-3956(75)900266]
- Proffitt R, Lange B. Feasibility of a customized, in-home, game-based stroke exercise program using the Microsoft Kinect® sensor. International Journal of Telerehabilitation. 2015; 7(2):23-34. [DOI:10.5195/IJT.2015.6177] [PMID] [PMCID]
- Felicia P . Handbook of research on improving learning and motivation through educational games: Multidisciplinary approaches: Multidisciplinary approaches. Pennsylvania: iGi Global; 2011.
- Siddiqui HA, Hamdani N, Khan AA. Difference in measure between two point discrimination and grip strength between diabetic and non-diabetic. International Journal of Science and Research. 2015; (SUB155177):380-3.
- Lee H, Voss MW, Prakash RS, Boot WR, Vo LT, Basak C, et al. Videogame training strategy-induced change in brain function during a complex visuomotor task. Behavioural Brain Research. 2012; 232(2):348-57. [DOI:10.1016/j.bbr.2012.03.043] [PMID]
- Hartwig M. Fun and evidence-computer based arm rehabilitation with the Pablo Plus System. Product Profile. 2011; 1-5.
- Poole JL. Measures of hand function. Arthritis Care & Research (Hoboken). 2011; 63(Suppl. 11):S189-99. [DOI:10.1002/acr.20631] [PMID]
- Ovbiagele B, Turan TN. Ischemic stroke therapeutics: A comprehensive guide. Geneva: Springer International Publishing. 2016. [DOI:10.1007/978-3-319-17750-2]
- Saposnik G, Levin M. Virtual reality in stroke rehabilitation: A meta-analysis and implications for clinicians. Stroke. 2011; 42(5):1380-6. [DOI:10.1161/STROKEAHA.110.605451] [PMID]
- Nica AS, Brailescu CM, Scarlet RG. Virtual reality as a method for evaluation and therapy after traumatic hand surgery. Studies in Health Technology and Informatics. 2013; 191:48-52. [PMID]
- Rose FD, Brooks BM and Rizzo AA. Virtual reality in brain damage rehabilitation: Review. CyberPsychology & Behavior. 2005; 8(3):241-62. [DOI:10.1089/cpb.2005.8.241] [PMID]
- Kamarul T, Ahmad TS, Loh WY. Hand grip strength in the adult Malaysian population. Journal of Orthopaedic Surgery. 2006; 14(2):172-7. [DOI:10.1177/230949900601400213] [PMID]
- Sears A, Jacko JA. The human-computer interaction handbook. In: Czaja SJ, Lee CC, editors. Information Technology and Older Adults. Lawrence New Jersey: Lawrence Earlbaum Associates; 2006.
- Prochaska JJ, Prochaska JO. A review of multiple health behavior change interventions for primary prevention. American Journal of Lifestyle Medicine. 2011; 5(3):1-21. [DOI:10.1177/1559827610391883] [PMID] [PMCID]
- Brandt Jr EN, Pope AM. Functional limitations research in rehabilitation science and engineering. Washington, D. C.: The National Academies Press; 1997.
- Stauss B, Neuhaus P. The qualitative satisfaction model. International Journal of Service Industry Management. 1997; 8(3):236-49. [DOI:10.1108/09564239710185424]
- Griffin J, McKenna K. Influences on leisure and life satisfaction of elderly people. Physical & Occupational Therapy in Geriatrics. 1999; 15(4):1-16. [DOI:10.1080/J148V15n04_01]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2018/12/5 | Accepted: 2019/04/17 | Published: 2019/09/1
Received: 2018/12/5 | Accepted: 2019/04/17 | Published: 2019/09/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
