
988368
Mon, Jul 15, 2024

Volume 17, Issue 2 (June 2019)
Iranian Rehabilitation Journal 2019, 17(2): 113-120 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohammadi S, Zabolypour S, Ghaffari F, Arazi T. The Effect of Family-Oriented Discharge Program on the Level of Preparedness for Care-Giving and Stress Experienced by the Family of Stroke Survivors . Iranian Rehabilitation Journal 2019; 17 (2) :113-120
URL: http://irj.uswr.ac.ir/article-1-895-en.html
URL: http://irj.uswr.ac.ir/article-1-895-en.html



1- Department of Medical Surgical Nursing, Ramsar School of Nursing and Midwifery, Babol University of Medical Sciences, Babol, Iran.
2- Department of Nursing, School of Nursing and Midwifery, Yasuj University of Medical Sciences, Yasuj, Iran.
3- Department of Nursing, School of Nursing and Midwifery, Neyshabur University of Medical Sciences, Neyshabur, Iran.
2- Department of Nursing, School of Nursing and Midwifery, Yasuj University of Medical Sciences, Yasuj, Iran.
3- Department of Nursing, School of Nursing and Midwifery, Neyshabur University of Medical Sciences, Neyshabur, Iran.
Full-Text [PDF 577 kb]
(2318 Downloads)
| Abstract (HTML) (4637 Views)

Full-Text: (1069 Views)
Highlights
● Stroke patients suffer from varying degrees of disability that require inpatient treatment and extended care at home.
● Attention should be paid to the discharge transition of stroke survivors.
● The family members should be provided with information about the illness and its caregiving, as well as post-discharge follow up.
● Discharge planning program with an emphasis on individualized education can enhance family preparedness for caregiving and decrease their stress.
Plain Language Summary
When family caregivers of stroke patients do not feel well prepared to manage their caregiving responsibilities, they are at risk for caregiver role burden and stress. It is defined as a perceived problem in representing the caring role. Stress and burden negatively impact the caring and rehabilitation of stroke patients. The program introduced in this study is vital for helping caregivers to adjust to their role and could be implemented in Iranian hospitals at a minimal cost.
1. Introduction
Stroke is among main chronic conditions, a major cause of long-term disability and the third common cause of death in the world. The global burden of stroke is dramatically increasing [1]. Usually, following a stroke, patients experience various bacteriological complications [2] and considerable disabilities, after hospital discharge. Patients with moderate and severe strokes should access ongoing rehabilitation care [1]. They are usually incapable of self-care and performing daily living activities [3]. Therefore, family members are their major support source [4].
Following a stroke, the new role of being a stroke caregiver is unexpectedly imposed to the family members; their families’ lifestyle often changes considerably [5]. The long-term caregiving, the responsibility to provide care for stroke patient, and the lack of time to devote to their daily activities are the causes of psychological disorders in caregivers [6]. Furthermore, they suffer from anxiety, burden and depressive symptoms [7].
Camak (2015) [8] indicated that anxiety and depression are prevalent complications among the family caregivers of stroke patients before and after hospital discharge; moreover, these psychological complications are caused by the lack of caring preparedness and supportive organizations.
Expensive private care centers; financial limitations for visiting a private physical or psychological therapist at home; and the lack of governmental rehabilitation centers for stroke survivors are important issues in Iran. Thus, family members are the primary caregivers of stroke patients [9].
A study revealed that due to the lack of information about caregiving and rehabilitation, and the lack of supportive centers in the society, family caregivers experience numerous problems in providing appropriate care for stroke survivors [10]. Many families in Iran fail to adapt to their new condition. Thus, they experience high levels of distress that may need some form of support; it may also persist over time [11].
Hospital nurses should recognize families as part of the caregiving procedure. Evaluating family members’ distress and burden is an advanced role of nurses during the hospitalization of stroke patients. Usually, nurses focus on the stroke patients’ needs without assessing their family members’ needs [8].
Providing suitable and adequate information along with a supporting program are the main steps to prepare family caregivers for their caring role [12]. Therefore, the present study aimed to evaluate the effect of family caregiver-oriented discharge planning program on the level of preparedness for caregiving and stress experienced by the Iranian caregivers of stroke patients.
2. Methods
A post-test only randomized controlled trial design was used. The reason to select a post-test only method was that stroke occurs suddenly; thus, it is illogical to assess the level of preparedness for caregiving and stress experienced by the family of stroke survivors in the first 48 hours of stroke (time before the intervention). Usually, preparedness for caregiving is developed over weeks and it was impossible to assess it at the beginning of the study.
The study participants were the family caregivers of stroke survivors. They were selected from two hospitals affiliated to Tehran University of Medical Sciences. Inclusion criteria were the ability to speak, write, and read in Persian; providing care for at least 4 days a week, and non-participation in any other similar study. The exclusion criteria were any serious illness or notable disability, absence from educational classes or unwillingness to answer researchers’ call, death during the course of study, and being transferred to a private care unit.
For subjects’ allocation and to avoid direct contact between participants and the contamination of educational program in the groups, cluster randomization method was applied. Thus, we allocated the participants of the hospital A in the control group, and the participants of the hospital B in the experimental group. After the discharge of all study participants from the two hospitals, inverted allocation strategy was used.
To estimate the sample size, we conducted a pilot study on 20 family caregivers in two groups, by a power of 80% and Confidence Interval (CI) of 95%; 30 samples were calculated for the control and experimental groups. In total, 79 family caregivers and their patients joined the present study. Ten stroke survivors in the control group and 8 stroke survivors in the experimental group passed away during the study; they were excluded from the study. One study participant failed to answer researcher’s calls and was excluded from the control group. Finally, the data were collected from 60 family caregivers in the two groups.
The dependent variables included the level of stress experienced by family caregivers and their preparedness for caregiving. They were measured by the Kingston Caregiver Stress Scale (KCSS) and the Preparedness for Caregiving Scale (PCS). The KCSS is a standard tool that measures stress in a caregiver. This scale can assess stress level changes over time, as the caregiver’s condition changes. The KCSS is developed for community living lay caregivers like families and not institutional care staff. It can be administered on a person who provides care on a daily basis at home; usually spouse or other relatives [13].
The PCS is an 8-item self-rated standard scale for caregivers [14]. Preparedness in this scale is defined as perceived preparation for the various aspects of caregiving; e.g. providing physical care, psychological support, coping with the stress and pressure of home-based caregiving. Each item has a 5-point Likert-type scale, ranging from 0 to 4 (0=not at all prepared to 4=very well prepared). Finally, each answer is scored from 0 to 4 [14].
The back-translation technique was applied by bilingual experts for the validation of scales. For assuring the face validity and readability of the two scales, 15 family caregivers of stroke survivors were requested to read the scales. Therefore, the scale items were revised and modified based on the caregivers’ understanding. The reliability of the scales was estimated by the internal consistency method. In total, 30 family caregivers of stroke patients were requested to complete the scales, two months after stroke. Finally, the Cronbach’s alpha coefficient was calculated equal to 0.86 for the PCS and 0.89 for the KCSS.
Stroke patients and their family caregivers in the control group received the hospital routine care. The experimental group received a family caregiver-oriented discharge planning program, including 3 phases; evaluating the families’ educational needs, educating the families, and follow-up calls after discharge.
The study subjects were selected among those with patients hospitalized for 48 hours. In the first step, we used a checklist for evaluating the families’ educational needs in terms of bio-psychological rehabilitation. Then, they were educated based on the Adult Learning Theory [15] and their needs, in a friendly, flexible, and understandable atmosphere. We conducted 3 educational sessions with an individualized approach; each session lasted 60 to 120 minutes.
The sessions’ topics were as follows: the reasons and risk factors of stroke, the role of family members in post-stroke care, stroke complications, caring role in cognitive, affective and sensory complications (the impairment of attention and consciousness, depression, visual problems, disorientation to place and time, etc.), caring role in motor disorders (pledgee, paresis, paralysis, etc.), caring role in bowel and bladder dysfunction, caring role in sleep problems and preventing role in common complications such as bed sore, Urinary Tract Infection (UTI), and pneumonia.
The researcher also provided information about appropriate diets and feeding methods , feeding with a NasoGastric (NG) tube, caring role in swallowing problems and dysphagia, emphasis on medication’ effects and adverse effects. After each educational session, the educator used observation techniques and the question and answer method to evaluate the study participants’ ability in the thought topics. If the study participants encountered any difficulty or problems with the procedures, the educator re-educated them. At the end of each educational session, a pamphlet consisting of educational goals were provided to the family caregivers.
After the stroke patients were discharged, the researchers made weekly (or based on families’ needs), phone calls to the family caregivers. Phone calls were made with different purposes such as assessing the study participants’ concerns about caring, and re-educating the essential points of supportive care. The study participants were allowed to call to discuss their problems.
To ensure that the control group received the routine care of hospital, we called them 1 month after their entrance to the study. The hospitals’ routine care were the same (based on the protocols provided by the Ministry of Health and Medical Education in Iran) and included simple and brief educations without educational booklets or follow-ups after discharge.
We provided the questionnaires to the families in both groups for completion after two months via post. Finally, their answers were obtained via phone. At the end of the study, all information taught to the intervention group were provided to the controls in the form of a booklet.
Data were analyzed using SPSS. The samples’ demographic data were analyzed using Mean±SD or percentages and frequencies for nominal variables. Baseline group comparability was analyzed using Chi-squared test and the Independent Samples t-test. A 0.05 significance level was used for all inferential tests. The research proposal was approved by the Ethics Committee of Tehran University of Medical Sciences. After providing family caregivers with information on the purpose of the study and before allocating them into groups, an informed consent was obtained from the caregivers. All caregivers were assured of their anonymity and confidentiality.
3. Results
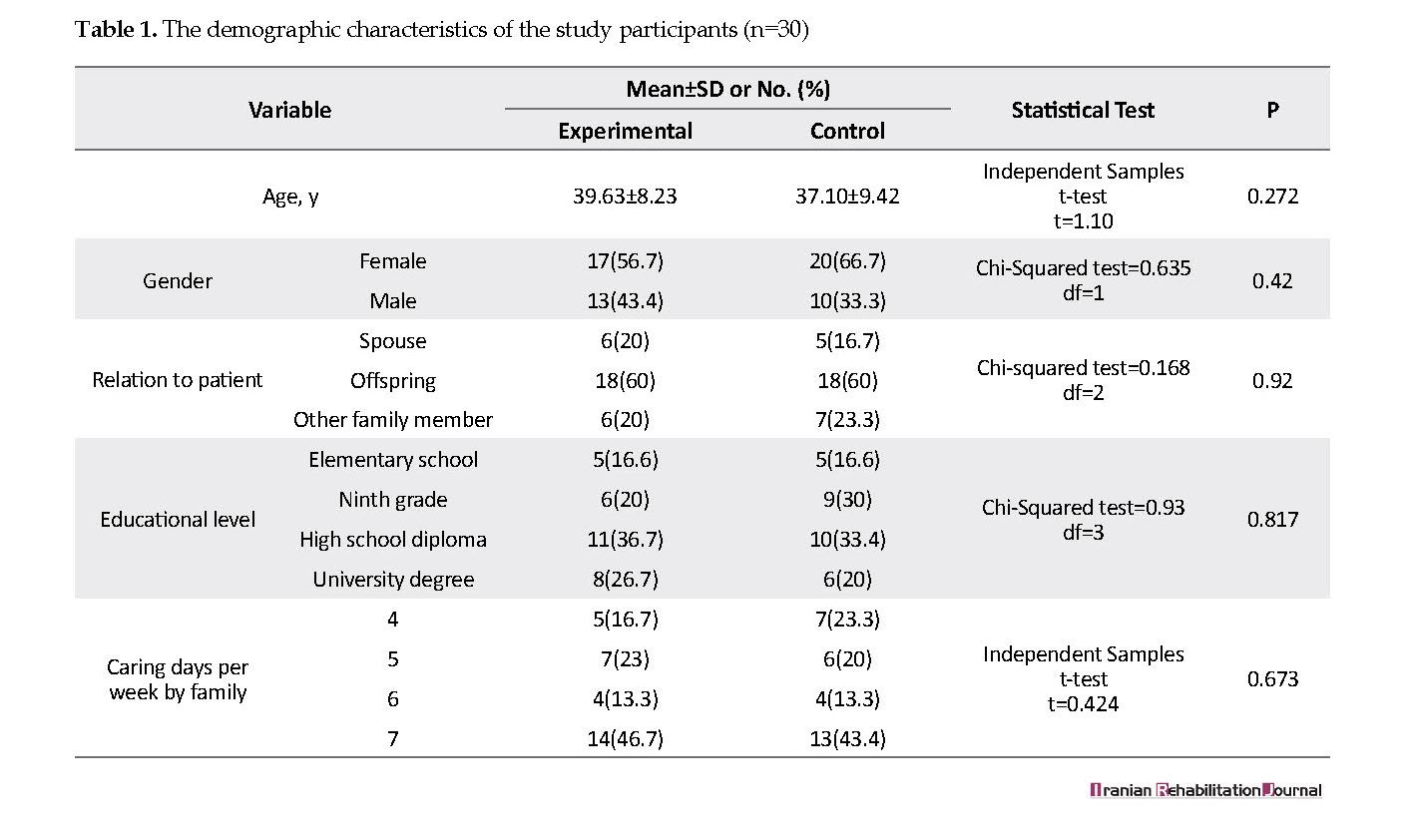
Most of the study participants were females (61.7%), with no academic educations (76.6%) and aged 30-49 years (36.7%). Most of them were the offspring of patients (mostly their daughter), and they reported no prior experience of an acute stroke patient care. There was no significant difference in the demographic characteristics of the study groups (P<0.05) (Table 1). According to the obtained results, the levels of preparedness for caregiving were significantly higher in the experimental group. Moreover, the experimental group reported lower levels of stress, compared to the controls (P<0.001) (Table 2).
● Stroke patients suffer from varying degrees of disability that require inpatient treatment and extended care at home.
● Attention should be paid to the discharge transition of stroke survivors.
● The family members should be provided with information about the illness and its caregiving, as well as post-discharge follow up.
● Discharge planning program with an emphasis on individualized education can enhance family preparedness for caregiving and decrease their stress.
Plain Language Summary
When family caregivers of stroke patients do not feel well prepared to manage their caregiving responsibilities, they are at risk for caregiver role burden and stress. It is defined as a perceived problem in representing the caring role. Stress and burden negatively impact the caring and rehabilitation of stroke patients. The program introduced in this study is vital for helping caregivers to adjust to their role and could be implemented in Iranian hospitals at a minimal cost.
1. Introduction
Stroke is among main chronic conditions, a major cause of long-term disability and the third common cause of death in the world. The global burden of stroke is dramatically increasing [1]. Usually, following a stroke, patients experience various bacteriological complications [2] and considerable disabilities, after hospital discharge. Patients with moderate and severe strokes should access ongoing rehabilitation care [1]. They are usually incapable of self-care and performing daily living activities [3]. Therefore, family members are their major support source [4].
Following a stroke, the new role of being a stroke caregiver is unexpectedly imposed to the family members; their families’ lifestyle often changes considerably [5]. The long-term caregiving, the responsibility to provide care for stroke patient, and the lack of time to devote to their daily activities are the causes of psychological disorders in caregivers [6]. Furthermore, they suffer from anxiety, burden and depressive symptoms [7].
Camak (2015) [8] indicated that anxiety and depression are prevalent complications among the family caregivers of stroke patients before and after hospital discharge; moreover, these psychological complications are caused by the lack of caring preparedness and supportive organizations.
Expensive private care centers; financial limitations for visiting a private physical or psychological therapist at home; and the lack of governmental rehabilitation centers for stroke survivors are important issues in Iran. Thus, family members are the primary caregivers of stroke patients [9].
A study revealed that due to the lack of information about caregiving and rehabilitation, and the lack of supportive centers in the society, family caregivers experience numerous problems in providing appropriate care for stroke survivors [10]. Many families in Iran fail to adapt to their new condition. Thus, they experience high levels of distress that may need some form of support; it may also persist over time [11].
Hospital nurses should recognize families as part of the caregiving procedure. Evaluating family members’ distress and burden is an advanced role of nurses during the hospitalization of stroke patients. Usually, nurses focus on the stroke patients’ needs without assessing their family members’ needs [8].
Providing suitable and adequate information along with a supporting program are the main steps to prepare family caregivers for their caring role [12]. Therefore, the present study aimed to evaluate the effect of family caregiver-oriented discharge planning program on the level of preparedness for caregiving and stress experienced by the Iranian caregivers of stroke patients.
2. Methods
A post-test only randomized controlled trial design was used. The reason to select a post-test only method was that stroke occurs suddenly; thus, it is illogical to assess the level of preparedness for caregiving and stress experienced by the family of stroke survivors in the first 48 hours of stroke (time before the intervention). Usually, preparedness for caregiving is developed over weeks and it was impossible to assess it at the beginning of the study.
The study participants were the family caregivers of stroke survivors. They were selected from two hospitals affiliated to Tehran University of Medical Sciences. Inclusion criteria were the ability to speak, write, and read in Persian; providing care for at least 4 days a week, and non-participation in any other similar study. The exclusion criteria were any serious illness or notable disability, absence from educational classes or unwillingness to answer researchers’ call, death during the course of study, and being transferred to a private care unit.
For subjects’ allocation and to avoid direct contact between participants and the contamination of educational program in the groups, cluster randomization method was applied. Thus, we allocated the participants of the hospital A in the control group, and the participants of the hospital B in the experimental group. After the discharge of all study participants from the two hospitals, inverted allocation strategy was used.
To estimate the sample size, we conducted a pilot study on 20 family caregivers in two groups, by a power of 80% and Confidence Interval (CI) of 95%; 30 samples were calculated for the control and experimental groups. In total, 79 family caregivers and their patients joined the present study. Ten stroke survivors in the control group and 8 stroke survivors in the experimental group passed away during the study; they were excluded from the study. One study participant failed to answer researcher’s calls and was excluded from the control group. Finally, the data were collected from 60 family caregivers in the two groups.
The dependent variables included the level of stress experienced by family caregivers and their preparedness for caregiving. They were measured by the Kingston Caregiver Stress Scale (KCSS) and the Preparedness for Caregiving Scale (PCS). The KCSS is a standard tool that measures stress in a caregiver. This scale can assess stress level changes over time, as the caregiver’s condition changes. The KCSS is developed for community living lay caregivers like families and not institutional care staff. It can be administered on a person who provides care on a daily basis at home; usually spouse or other relatives [13].
The PCS is an 8-item self-rated standard scale for caregivers [14]. Preparedness in this scale is defined as perceived preparation for the various aspects of caregiving; e.g. providing physical care, psychological support, coping with the stress and pressure of home-based caregiving. Each item has a 5-point Likert-type scale, ranging from 0 to 4 (0=not at all prepared to 4=very well prepared). Finally, each answer is scored from 0 to 4 [14].
The back-translation technique was applied by bilingual experts for the validation of scales. For assuring the face validity and readability of the two scales, 15 family caregivers of stroke survivors were requested to read the scales. Therefore, the scale items were revised and modified based on the caregivers’ understanding. The reliability of the scales was estimated by the internal consistency method. In total, 30 family caregivers of stroke patients were requested to complete the scales, two months after stroke. Finally, the Cronbach’s alpha coefficient was calculated equal to 0.86 for the PCS and 0.89 for the KCSS.
Stroke patients and their family caregivers in the control group received the hospital routine care. The experimental group received a family caregiver-oriented discharge planning program, including 3 phases; evaluating the families’ educational needs, educating the families, and follow-up calls after discharge.
The study subjects were selected among those with patients hospitalized for 48 hours. In the first step, we used a checklist for evaluating the families’ educational needs in terms of bio-psychological rehabilitation. Then, they were educated based on the Adult Learning Theory [15] and their needs, in a friendly, flexible, and understandable atmosphere. We conducted 3 educational sessions with an individualized approach; each session lasted 60 to 120 minutes.
The sessions’ topics were as follows: the reasons and risk factors of stroke, the role of family members in post-stroke care, stroke complications, caring role in cognitive, affective and sensory complications (the impairment of attention and consciousness, depression, visual problems, disorientation to place and time, etc.), caring role in motor disorders (pledgee, paresis, paralysis, etc.), caring role in bowel and bladder dysfunction, caring role in sleep problems and preventing role in common complications such as bed sore, Urinary Tract Infection (UTI), and pneumonia.
The researcher also provided information about appropriate diets and feeding methods , feeding with a NasoGastric (NG) tube, caring role in swallowing problems and dysphagia, emphasis on medication’ effects and adverse effects. After each educational session, the educator used observation techniques and the question and answer method to evaluate the study participants’ ability in the thought topics. If the study participants encountered any difficulty or problems with the procedures, the educator re-educated them. At the end of each educational session, a pamphlet consisting of educational goals were provided to the family caregivers.
After the stroke patients were discharged, the researchers made weekly (or based on families’ needs), phone calls to the family caregivers. Phone calls were made with different purposes such as assessing the study participants’ concerns about caring, and re-educating the essential points of supportive care. The study participants were allowed to call to discuss their problems.
To ensure that the control group received the routine care of hospital, we called them 1 month after their entrance to the study. The hospitals’ routine care were the same (based on the protocols provided by the Ministry of Health and Medical Education in Iran) and included simple and brief educations without educational booklets or follow-ups after discharge.
We provided the questionnaires to the families in both groups for completion after two months via post. Finally, their answers were obtained via phone. At the end of the study, all information taught to the intervention group were provided to the controls in the form of a booklet.
Data were analyzed using SPSS. The samples’ demographic data were analyzed using Mean±SD or percentages and frequencies for nominal variables. Baseline group comparability was analyzed using Chi-squared test and the Independent Samples t-test. A 0.05 significance level was used for all inferential tests. The research proposal was approved by the Ethics Committee of Tehran University of Medical Sciences. After providing family caregivers with information on the purpose of the study and before allocating them into groups, an informed consent was obtained from the caregivers. All caregivers were assured of their anonymity and confidentiality.
3. Results
Most of the study participants were females (61.7%), with no academic educations (76.6%) and aged 30-49 years (36.7%). Most of them were the offspring of patients (mostly their daughter), and they reported no prior experience of an acute stroke patient care. There was no significant difference in the demographic characteristics of the study groups (P<0.05) (Table 1). According to the obtained results, the levels of preparedness for caregiving were significantly higher in the experimental group. Moreover, the experimental group reported lower levels of stress, compared to the controls (P<0.001) (Table 2).
4. Discussion
According to the obtained results, there were no significant differences among the groups in terms of demographic characteristics. Most of the study participants were female with no academic educations. This finding is similar to another study conducted in Iran on the demographic characteristics of caregivers of stroke patients [16]. Most of the study participants were patients’ daughters. The obtained data are consistent with a study in Thailand [12]. That study indicated that in Thai culture, patients’ offspring, especially daughters appreciate their parents by taking care of them [12]; this is similar to the Iranian culture.
The present study revealed providing a supportive program to the family members of stroke patients, including educational sessions based on the Adult Learning Theory can enhance preparedness for caregiving. The effectiveness of the program in the experimental group resulted from the families’ attention to all educational sessions and their active learning. Despite recent global efforts to creating a supportive program for stroke survivors, Iranian stroke patients and their families do not consistently receive the supportive care [17].
Iranian nurses occasionally provide family caregiver support programs and the families are referred to private care centers. However, private care centers for stroke survivors are expensive in Iran, and most of the family caregivers cannot afford those [18]. As a result, family caregivers prefer to care for their stroke survivor at home. Usually, family members rely on their personal and non-scientific information about stroke patients caring; some chronic complications in patients are caused by such nonscientific care. Therefore, the study participants who had received family caregiver-oriented discharge planning program were more prepared for caring, compared to the other participants.
Prior research also indicated that stroke survivors and their caregivers benefited from a family caregiver-oriented discharge program that improved the families’ preparation for caring and satisfied their needs during discharge transition [19]. Furthermore, consecutive follow-ups after administering educational sessions have been reported as the important predictor of caregivers’ ability and preparedness for the rehabilitation of stroke survivors [18].
When family caregivers do not feel well prepared to manage their caregiving responsibilities, they are at risk for caregiver role burden and role strain, defined as a perceived problem in representing the caring role. Family caregivers’ perceptions about the severity of problems and burden in stroke survivors caring may be caused by the lack of families preparedness; it could be related to their psychological problems such as depression and stress [20].
Stress and burden negatively impact the caring and rehabilitation of stroke patients. The results of this study suggested that educational support for the caregivers of stroke survivors can reduce their stress. Furthermore, providing informational support for caregivers was associated with decreased stress in caregivers. Family caregivers must learn new caring skills in a short time while usually simultaneously face economic problems and try to cope with the symptoms exhibited by the stroke patient [21].
It is not surprising that family caregivers experience some level of stress. In the lack of socio-educational support, families feel insecure about their ability to take the caregiving role; this can cause even more burden and stress [22]. Preparation for caring was the most powerful predictor of stress in stroke caregivers [23].
Family support in stroke rehabilitation may reduce stress and depression in stroke survivors and their family caregivers [24]. Additionally, the lack of educational support was associated with stress in stroke survivors and their caregivers [6]. Our findings support the use of supportive educative programs to decrease caregivers’ stress.
5. Conclusion
Developing a professional nursing and discharge planning program for the Iranian stroke survivors was the important purpose of this study. Attention should be paid to the discharge transition of stroke survivors and their family members, with providing information about illness and caregiving, as well as post-discharge follow-up. This program is vital for helping caregivers to adjust with their role and could be implemented in Iranian hospitals at a minimal cost.
Conducting both hospital- and home-based interventions was the strength of this supporting program. An important point of the supportive program was its structured approach to individual family caregiver learning, including 3 hospital-based visits with one-on-one education. It was provided in accordance with the caregivers’ needs, Adult Learning Theory, written instructions, and skills demonstration.
Family caregivers of stroke survivors experience the deterioration of general health at different dimensions. Therefore, it is recommended that planning for general health and social support for caregivers should be demonstrated through polymerizing in health and treatment. The lack of an observational follow-up for assessing the implementation of family caregiver-oriented discharge planning program at home was an important limitation of the current study.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by ethics committee of Tehran University of Medical Sciences.
Funding
This research was supported by Tehran University of Medical Sciences.
Authors' contributions
Conceptualization: Sepideh Mohammadi; Methodology: Fatemeh Ghafari, Tajmohamad Arazi; Investigation: All authors; Writing original draft: All authors; Writing, review and editing: Sepideh Mohammadi, Soheila Zabolipour; Funding acquisition: Sepideh Mohammadi, Soheila Zabolipour; and Resources: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the nurses for their participation in this study.
References
Dehghan Nayeri N, Mohammadi S, Pedram Razi S, Kazemnejad A. Investigating the effects of a family-centered care program on stroke patients’ adherence to their therapeutic regimens. Contemporary Nurse. 2014; 47(1-2):88-96. [DOI:10.1080/10376178.2014.11081910]
Kumar R, Kaur S, Reddemma K. Needs, burden, coping and quality of life in stroke caregivers: A pilot survey. Nursing and Midwifery Research Journal. 2015; 11(2):57-67.
Ostwald SK, Davis S, Hersch G, Kelley C, Godwin KM. Evidence-based educational guidelines for stroke survivors after discharge home. Journal of Neuroscience Nursing. 2008; 40(3):173-91. [DOI:10.1097/01376517-200806000-00008] [PMID] [PMID]
Chafjiri RT, Navabi N, Shamsalinia A, Ghaffari F. The relationship between the spiritual attitude of the family caregivers of older patients with stroke and their burden. Clinical Interventions in Aging. 2017; 12:453. [DOI:10.2147/CIA.S121285] [PMID] [PMCID]
Li X, Xia X, Wang P, Zhang S, Liu M, Wang L. Needs and rights awareness of stroke survivors and caregivers: A cross-sectional, single-centre questionnaire survey. BMJ Open. 2017; 7(10):e013210. [DOI:10.1136/bmjopen-2016-013210] [PMID] [PMCID]
Pierce LL, Thompson TL, Govoni AL, Steiner V. Caregivers’ incongruence: Emotional strain in caring for persons with stroke. Rehabilitation Nursing. 2012; 37(5):258-66. [DOI:10.1002/rnj.35] [PMID] [PMCID]
Roth DL, Sheehan OC, Huang J, Rhodes JD, Judd SE, Haley WE. Abstract TMP49: Depressive symptoms after stroke are linked longitudinally between stroke survivors and their family caregivers. Stroke. 2017; 48(suppl_1):ATMP49.
Camak DJ. Addressing the burden of stroke caregivers: A literature review. Journal of Clinical Nursing. 2015; 24(17-18):2376-82. [DOI:10.1111/jocn.12884] [PMID]
Dehghan Nayeri N, Mohammadi S, Pedram Razi S, Kazemnejad A. [Adherence of family caregivers of patients with stroke to rehabilitation regimen (Persian)]. Journal of Hayat. 2012; 18(1):30-41.
Dalvandi A, Heikkilä K, Maddah SS, Khankeh HR, Ekman SL. Life experiences after stroke among Iranian stroke survivors. International Nursing Review. 2010; 57(2):247-53. [DOI:10.1111/j.1466-7657.2009.00786.x] [PMID]
Nayeri ND, Mohammadi S, Arazi T. Examining the level of adherence of therapeutic regime by the family caregivers of stroke patients. Canadian Journal on Medicine. 2011; 2(3):87-98.
Oupra R, Griffiths R, Pryor J, Mott S. Effectiveness of supportive educative learning programme on the level of strain experienced by caregivers of stroke patients in Thailand. Health & Social Care in the Community. 2010; 18(1):10-20. [DOI:10.1111/j.1365-2524.2009.00865.x] [PMID]
Sadak T, Korpak A, Wright JD, Lee MK, Noel M, Buckwalter K, Borson S. Psychometric evaluation of Kingston Caregiver Stress Scale. Clinical Gerontology. 2017; 40(4):268-280.
Zwicker D. Preparedness for caregiving scale. Movement Disorders. 2010; 28:1-2.
Smith MK. Malcolm knowles, informal adult education, self-direction and andragogy. London: Encyclopedia of Informal Education; 2002.
Tajvidi M, Dalvandi A, Sahaf R, Rahgozar M. Relationship between general health and demographic characteristics of family caregivers of stroke survivors. Iranian Journal of Ageing. 2018; 12(4):494-505. [DOI:10.21859/sija.12.4.494]
Bakas T, Farran CJ, Austin JK, Given BA, Johnson EA, Williams LS. Stroke caregiver outcomes from the Telephone Assessment and Skill-Building kit (TASK). Topics in Stroke Rehabilitation. 2009; 16(2):105-21. [DOI:10.1310/tsr1602-105] [PMID] [PMCID]
Kazemnejad A. [Effectiveness of family empowerment program on level of adherence to treatment regimens in stroke patients; A randomized controlled trial (Persian)]. Evidence Based Care. 2015; 5(1):57-66. [DOI:10.22038/EBCJ.2015.4072]
Shyu YI, Chen MC, Chen ST, Wang HP, Shao JH. A family caregiver‐oriented discharge planning program for older stroke patients and their family caregivers. Journal of Clinical Nursing. 2008; 17(18):2497-508. [DOI:10.1111/j.1365-2702.2008.02450.x] [PMID]
Tosun ZK, Temel M. Burden of caregiving for stroke patients and the role of social support among family members: an assessment through home visits. International Journal of Caring Sciences. 2017; 10(3):1696.
Grant JS, Glandon GL, Elliott TR, Giger JN, Weaver M. Caregiving problems and feelings experienced by family caregivers of stroke survivors the first month after discharge. International Journal of Rehabilitation Research. 2004; 27(2):105-11. [DOI:10.1097/01.mrr.0000127639.47494.e3] [PMID]
Jönsson AC, Lindgren I, Hallström B, Norrving B, Lindgren A. Determinants of quality of life in stroke survivors and their informal caregivers. Stroke. 2005; 36(4):803-8. [DOI:10.1161/01.STR.0000160873.32791.20] [PMID]
Ostwald SK, Bernal MP, Cron SG, Godwin KM. Stress experienced by stroke survivors and spousal caregivers during the first year after discharge from inpatient rehabilitation. Topics in Stroke Rehabilitation. 2009; 16(2):93-104. [DOI:10.1310/tsr1602-93] [PMID] [PMCID]
Vallury KD, Jones M, Gray R. Do family-oriented interventions reduce poststroke depression? A systematic review and recommendations for practice. Topics in Stroke Rehabilitation. 2015; 22(6):453-9. [DOI:10.1179/1074935715Z.00000000061] [PMID]
According to the obtained results, there were no significant differences among the groups in terms of demographic characteristics. Most of the study participants were female with no academic educations. This finding is similar to another study conducted in Iran on the demographic characteristics of caregivers of stroke patients [16]. Most of the study participants were patients’ daughters. The obtained data are consistent with a study in Thailand [12]. That study indicated that in Thai culture, patients’ offspring, especially daughters appreciate their parents by taking care of them [12]; this is similar to the Iranian culture.
The present study revealed providing a supportive program to the family members of stroke patients, including educational sessions based on the Adult Learning Theory can enhance preparedness for caregiving. The effectiveness of the program in the experimental group resulted from the families’ attention to all educational sessions and their active learning. Despite recent global efforts to creating a supportive program for stroke survivors, Iranian stroke patients and their families do not consistently receive the supportive care [17].
Iranian nurses occasionally provide family caregiver support programs and the families are referred to private care centers. However, private care centers for stroke survivors are expensive in Iran, and most of the family caregivers cannot afford those [18]. As a result, family caregivers prefer to care for their stroke survivor at home. Usually, family members rely on their personal and non-scientific information about stroke patients caring; some chronic complications in patients are caused by such nonscientific care. Therefore, the study participants who had received family caregiver-oriented discharge planning program were more prepared for caring, compared to the other participants.
Prior research also indicated that stroke survivors and their caregivers benefited from a family caregiver-oriented discharge program that improved the families’ preparation for caring and satisfied their needs during discharge transition [19]. Furthermore, consecutive follow-ups after administering educational sessions have been reported as the important predictor of caregivers’ ability and preparedness for the rehabilitation of stroke survivors [18].
When family caregivers do not feel well prepared to manage their caregiving responsibilities, they are at risk for caregiver role burden and role strain, defined as a perceived problem in representing the caring role. Family caregivers’ perceptions about the severity of problems and burden in stroke survivors caring may be caused by the lack of families preparedness; it could be related to their psychological problems such as depression and stress [20].
Stress and burden negatively impact the caring and rehabilitation of stroke patients. The results of this study suggested that educational support for the caregivers of stroke survivors can reduce their stress. Furthermore, providing informational support for caregivers was associated with decreased stress in caregivers. Family caregivers must learn new caring skills in a short time while usually simultaneously face economic problems and try to cope with the symptoms exhibited by the stroke patient [21].
It is not surprising that family caregivers experience some level of stress. In the lack of socio-educational support, families feel insecure about their ability to take the caregiving role; this can cause even more burden and stress [22]. Preparation for caring was the most powerful predictor of stress in stroke caregivers [23].
Family support in stroke rehabilitation may reduce stress and depression in stroke survivors and their family caregivers [24]. Additionally, the lack of educational support was associated with stress in stroke survivors and their caregivers [6]. Our findings support the use of supportive educative programs to decrease caregivers’ stress.
5. Conclusion
Developing a professional nursing and discharge planning program for the Iranian stroke survivors was the important purpose of this study. Attention should be paid to the discharge transition of stroke survivors and their family members, with providing information about illness and caregiving, as well as post-discharge follow-up. This program is vital for helping caregivers to adjust with their role and could be implemented in Iranian hospitals at a minimal cost.
Conducting both hospital- and home-based interventions was the strength of this supporting program. An important point of the supportive program was its structured approach to individual family caregiver learning, including 3 hospital-based visits with one-on-one education. It was provided in accordance with the caregivers’ needs, Adult Learning Theory, written instructions, and skills demonstration.
Family caregivers of stroke survivors experience the deterioration of general health at different dimensions. Therefore, it is recommended that planning for general health and social support for caregivers should be demonstrated through polymerizing in health and treatment. The lack of an observational follow-up for assessing the implementation of family caregiver-oriented discharge planning program at home was an important limitation of the current study.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by ethics committee of Tehran University of Medical Sciences.
Funding
This research was supported by Tehran University of Medical Sciences.
Authors' contributions
Conceptualization: Sepideh Mohammadi; Methodology: Fatemeh Ghafari, Tajmohamad Arazi; Investigation: All authors; Writing original draft: All authors; Writing, review and editing: Sepideh Mohammadi, Soheila Zabolipour; Funding acquisition: Sepideh Mohammadi, Soheila Zabolipour; and Resources: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the nurses for their participation in this study.
References
Dehghan Nayeri N, Mohammadi S, Pedram Razi S, Kazemnejad A. Investigating the effects of a family-centered care program on stroke patients’ adherence to their therapeutic regimens. Contemporary Nurse. 2014; 47(1-2):88-96. [DOI:10.1080/10376178.2014.11081910]
Kumar R, Kaur S, Reddemma K. Needs, burden, coping and quality of life in stroke caregivers: A pilot survey. Nursing and Midwifery Research Journal. 2015; 11(2):57-67.
Ostwald SK, Davis S, Hersch G, Kelley C, Godwin KM. Evidence-based educational guidelines for stroke survivors after discharge home. Journal of Neuroscience Nursing. 2008; 40(3):173-91. [DOI:10.1097/01376517-200806000-00008] [PMID] [PMID]
Chafjiri RT, Navabi N, Shamsalinia A, Ghaffari F. The relationship between the spiritual attitude of the family caregivers of older patients with stroke and their burden. Clinical Interventions in Aging. 2017; 12:453. [DOI:10.2147/CIA.S121285] [PMID] [PMCID]
Li X, Xia X, Wang P, Zhang S, Liu M, Wang L. Needs and rights awareness of stroke survivors and caregivers: A cross-sectional, single-centre questionnaire survey. BMJ Open. 2017; 7(10):e013210. [DOI:10.1136/bmjopen-2016-013210] [PMID] [PMCID]
Pierce LL, Thompson TL, Govoni AL, Steiner V. Caregivers’ incongruence: Emotional strain in caring for persons with stroke. Rehabilitation Nursing. 2012; 37(5):258-66. [DOI:10.1002/rnj.35] [PMID] [PMCID]
Roth DL, Sheehan OC, Huang J, Rhodes JD, Judd SE, Haley WE. Abstract TMP49: Depressive symptoms after stroke are linked longitudinally between stroke survivors and their family caregivers. Stroke. 2017; 48(suppl_1):ATMP49.
Camak DJ. Addressing the burden of stroke caregivers: A literature review. Journal of Clinical Nursing. 2015; 24(17-18):2376-82. [DOI:10.1111/jocn.12884] [PMID]
Dehghan Nayeri N, Mohammadi S, Pedram Razi S, Kazemnejad A. [Adherence of family caregivers of patients with stroke to rehabilitation regimen (Persian)]. Journal of Hayat. 2012; 18(1):30-41.
Dalvandi A, Heikkilä K, Maddah SS, Khankeh HR, Ekman SL. Life experiences after stroke among Iranian stroke survivors. International Nursing Review. 2010; 57(2):247-53. [DOI:10.1111/j.1466-7657.2009.00786.x] [PMID]
Nayeri ND, Mohammadi S, Arazi T. Examining the level of adherence of therapeutic regime by the family caregivers of stroke patients. Canadian Journal on Medicine. 2011; 2(3):87-98.
Oupra R, Griffiths R, Pryor J, Mott S. Effectiveness of supportive educative learning programme on the level of strain experienced by caregivers of stroke patients in Thailand. Health & Social Care in the Community. 2010; 18(1):10-20. [DOI:10.1111/j.1365-2524.2009.00865.x] [PMID]
Sadak T, Korpak A, Wright JD, Lee MK, Noel M, Buckwalter K, Borson S. Psychometric evaluation of Kingston Caregiver Stress Scale. Clinical Gerontology. 2017; 40(4):268-280.
Zwicker D. Preparedness for caregiving scale. Movement Disorders. 2010; 28:1-2.
Smith MK. Malcolm knowles, informal adult education, self-direction and andragogy. London: Encyclopedia of Informal Education; 2002.
Tajvidi M, Dalvandi A, Sahaf R, Rahgozar M. Relationship between general health and demographic characteristics of family caregivers of stroke survivors. Iranian Journal of Ageing. 2018; 12(4):494-505. [DOI:10.21859/sija.12.4.494]
Bakas T, Farran CJ, Austin JK, Given BA, Johnson EA, Williams LS. Stroke caregiver outcomes from the Telephone Assessment and Skill-Building kit (TASK). Topics in Stroke Rehabilitation. 2009; 16(2):105-21. [DOI:10.1310/tsr1602-105] [PMID] [PMCID]
Kazemnejad A. [Effectiveness of family empowerment program on level of adherence to treatment regimens in stroke patients; A randomized controlled trial (Persian)]. Evidence Based Care. 2015; 5(1):57-66. [DOI:10.22038/EBCJ.2015.4072]
Shyu YI, Chen MC, Chen ST, Wang HP, Shao JH. A family caregiver‐oriented discharge planning program for older stroke patients and their family caregivers. Journal of Clinical Nursing. 2008; 17(18):2497-508. [DOI:10.1111/j.1365-2702.2008.02450.x] [PMID]
Tosun ZK, Temel M. Burden of caregiving for stroke patients and the role of social support among family members: an assessment through home visits. International Journal of Caring Sciences. 2017; 10(3):1696.
Grant JS, Glandon GL, Elliott TR, Giger JN, Weaver M. Caregiving problems and feelings experienced by family caregivers of stroke survivors the first month after discharge. International Journal of Rehabilitation Research. 2004; 27(2):105-11. [DOI:10.1097/01.mrr.0000127639.47494.e3] [PMID]
Jönsson AC, Lindgren I, Hallström B, Norrving B, Lindgren A. Determinants of quality of life in stroke survivors and their informal caregivers. Stroke. 2005; 36(4):803-8. [DOI:10.1161/01.STR.0000160873.32791.20] [PMID]
Ostwald SK, Bernal MP, Cron SG, Godwin KM. Stress experienced by stroke survivors and spousal caregivers during the first year after discharge from inpatient rehabilitation. Topics in Stroke Rehabilitation. 2009; 16(2):93-104. [DOI:10.1310/tsr1602-93] [PMID] [PMCID]
Vallury KD, Jones M, Gray R. Do family-oriented interventions reduce poststroke depression? A systematic review and recommendations for practice. Topics in Stroke Rehabilitation. 2015; 22(6):453-9. [DOI:10.1179/1074935715Z.00000000061] [PMID]
Article type: Original Research Articles |
Subject:
Nursing
Received: 2018/09/25 | Accepted: 2019/02/3 | Published: 2019/06/1
Received: 2018/09/25 | Accepted: 2019/02/3 | Published: 2019/06/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
