
988368
Fri, Jul 24, 2026

Volume 17, Issue 3 (September 2019)
Iranian Rehabilitation Journal 2019, 17(3): 197-206 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Fadavi-Ghaffari M, Azad A, Meimandi M, Arani-Kashani Z, Ghorbanpoor H. The Psychometric Properties of Falls Efficacy Scale in the Elderly Iranian Residents of Nursing Homes. Iranian Rehabilitation Journal 2019; 17 (3) :197-206
URL: http://irj.uswr.ac.ir/article-1-973-en.html
URL: http://irj.uswr.ac.ir/article-1-973-en.html
Mahsa Fadavi-Ghaffari1 

 , Akram Azad *1 , Mahsa Meimandi1 , Zohre Arani-Kashani2 , Hamze Ghorbanpoor1
, Akram Azad *1 , Mahsa Meimandi1 , Zohre Arani-Kashani2 , Hamze Ghorbanpoor1
, Akram Azad *1 , Mahsa Meimandi1 , Zohre Arani-Kashani2 , Hamze Ghorbanpoor1
1- Rehabilitation Research Center, Department of Occupational Therapy, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Rehabilitation Research Center, Department of Speech Therapy, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Rehabilitation Research Center, Department of Speech Therapy, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 859 kb]
(2779 Downloads)
| Abstract (HTML) (7385 Views)



Full-Text: (1912 Views)
1. Introduction
s defined by the World Health Organization (WHO), people aged ≥60 years are regarded as older adults. In Iran, in 2015, about (10%) of the population aged ≥60 years, and this rate will reach (33%) in the next 35 years. Approximately (30-50%) of the elders living in nursing homes experience at least one fall per year, and (40%) of them experience more than one fall annually [1, 2]. One of the most frequent problems in older adults is the Fear of Falling (FOF). The prevalence of FOF as an anticipatory fear of falling in older adults is equal to (29-76%) [3].
FOF can lead to the loss of self-esteem, depression, limitations in Activities of Daily Living (ADL), restricted mobility, and balance performances. Falls reoccur without controlling these symptoms, and the level of performance will be compromised; therefore, the diagnosis and prevention of FOF are of particular importance. Numerous studies investigated FOF, and a wide range of tools (single item scales and more complex and precise tools) are available to assess it [4, 5]. Despite their simplicity and validity for evaluating FOF in older adults, the Single Item Question (SIQ) tools fail to discover the extent and variability of FOF [5]. The Activities-specific Balance Confidence (ABC) scale assesses confidence in the balance as self-efficacy for performing indoor and outdoor activities. This scale provides individuals’ capacities to carry out activities based on Bandura’s self-efficacy theory and emphasizes self-confidence [6].
The Falls Efficacy Scale (FES) developed by Tinetti et al. assesses perceived confidence in avoiding falls while performing the Basic Activities of Daily Living (BADL) in older adults. Therapists or individuals can complete this easily administered scale [7]; however, it is inappropriate for older adults who spend time outside the house and have high mobility [5]. Acceptable validity and reliability have been reported for the original version of FES and modified versions in diverse languages and cultures [8-10]. The Swedish version of FES (FES-S) was cross-culturally adapted and validated in community-dwelling elder adults in Iran [11]. Additionally, the original version of FES was translated and validated in community-dwelling elder adults in Iran; however, its comprehensive validity and reliability must be investigated before considering it as a useful scale in the future clinical and research settings [12]. Examining the underlying factor structure of a scale improves its precision and refinements. Therefore, because of an increase of older adults’ population in nursing homes, the current study aimed at translating and determining the reliability and validity of FES in the elderly Iranian residents of nursing homes [1].
2. Methods
The current methodological study was conducted in Tehran City, Iran, in 2017. The study participants were selected based on convenience sampling method. The inclusion criteria were people aged ≥60 years, the cognitive level of ≥21 according to Mini-Mental Status Examination (MMSE), walking ability for ≥10m, a residence history of ≥6 mon in nursing homes, and ability to understand and communicate in the Persian language [13]. The study participants would be excluded if they were unwilling to participate in the study or absent in the second assessment. The minimum sample size was 5 to 10 times higher than the number of items in the scale. Therefore, 100 healthy 60-87 year-old elder adults were selected in about 6 months.
All the study participants were assessed in the morning. The Falls Efficacy Scale-International (FES-I), FES, and SIQ were randomly applied by an experienced occupational therapist. The average time for assessments was 15 min. The study participants were assessed twice with a 4-7 day time interval based on similar articles [7, 14].
Study instruments
Falls Efficacy Scale (FES)
The FES has been developed by Tinetti et al. to evaluate the perceived confidence in avoiding falls while performing indoor BADL. This scale consists of 10 items, and each item is scored from 1 (very confident) to 10 (not confident at all). The total score, obtained by summing up the item scores, ranges from 10 to 100. A total score of greater than 70 indicates FOF in the person [7].
Single Item Question
This simple question assesses FOF by asking: “Were you afraid of falling in the past 6 months?” the “yes” answer is followed by the question: “Did you avoid certain activities due to FOF?” the potential answer is yes/ no [5].
Falls Efficacy Scale-International
This scale provides information about FOF while performing indoor and outdoor basic and instrumental activities. The FES-I consists of 16 items (10 items of the original FES and 6 additional items regarding social activities); each item is scored on a 4-point (1=not concerned at all, 4=very concerned) Likert-type scale. The summation of scores provides a total score of 16 (the absence of FOF) to 64 (the extreme concern of FOF) [15].
Translation protocol
First, permission was obtained from the tool developer (Tinetti). Then, according to the International Quality of Life Assessment (IQOLA) protocol, two professional individuals in English translated the scale into Persian. After making necessary revisions, the preliminary forward translated version was produced. In the next stage, the scale was back-translated into English, and after the reconciliation of problematic items, the final version of FES was produced (Figure 1), Persian version in Appendix 1.
s defined by the World Health Organization (WHO), people aged ≥60 years are regarded as older adults. In Iran, in 2015, about (10%) of the population aged ≥60 years, and this rate will reach (33%) in the next 35 years. Approximately (30-50%) of the elders living in nursing homes experience at least one fall per year, and (40%) of them experience more than one fall annually [1, 2]. One of the most frequent problems in older adults is the Fear of Falling (FOF). The prevalence of FOF as an anticipatory fear of falling in older adults is equal to (29-76%) [3].
FOF can lead to the loss of self-esteem, depression, limitations in Activities of Daily Living (ADL), restricted mobility, and balance performances. Falls reoccur without controlling these symptoms, and the level of performance will be compromised; therefore, the diagnosis and prevention of FOF are of particular importance. Numerous studies investigated FOF, and a wide range of tools (single item scales and more complex and precise tools) are available to assess it [4, 5]. Despite their simplicity and validity for evaluating FOF in older adults, the Single Item Question (SIQ) tools fail to discover the extent and variability of FOF [5]. The Activities-specific Balance Confidence (ABC) scale assesses confidence in the balance as self-efficacy for performing indoor and outdoor activities. This scale provides individuals’ capacities to carry out activities based on Bandura’s self-efficacy theory and emphasizes self-confidence [6].
The Falls Efficacy Scale (FES) developed by Tinetti et al. assesses perceived confidence in avoiding falls while performing the Basic Activities of Daily Living (BADL) in older adults. Therapists or individuals can complete this easily administered scale [7]; however, it is inappropriate for older adults who spend time outside the house and have high mobility [5]. Acceptable validity and reliability have been reported for the original version of FES and modified versions in diverse languages and cultures [8-10]. The Swedish version of FES (FES-S) was cross-culturally adapted and validated in community-dwelling elder adults in Iran [11]. Additionally, the original version of FES was translated and validated in community-dwelling elder adults in Iran; however, its comprehensive validity and reliability must be investigated before considering it as a useful scale in the future clinical and research settings [12]. Examining the underlying factor structure of a scale improves its precision and refinements. Therefore, because of an increase of older adults’ population in nursing homes, the current study aimed at translating and determining the reliability and validity of FES in the elderly Iranian residents of nursing homes [1].
2. Methods
The current methodological study was conducted in Tehran City, Iran, in 2017. The study participants were selected based on convenience sampling method. The inclusion criteria were people aged ≥60 years, the cognitive level of ≥21 according to Mini-Mental Status Examination (MMSE), walking ability for ≥10m, a residence history of ≥6 mon in nursing homes, and ability to understand and communicate in the Persian language [13]. The study participants would be excluded if they were unwilling to participate in the study or absent in the second assessment. The minimum sample size was 5 to 10 times higher than the number of items in the scale. Therefore, 100 healthy 60-87 year-old elder adults were selected in about 6 months.
All the study participants were assessed in the morning. The Falls Efficacy Scale-International (FES-I), FES, and SIQ were randomly applied by an experienced occupational therapist. The average time for assessments was 15 min. The study participants were assessed twice with a 4-7 day time interval based on similar articles [7, 14].
Study instruments
Falls Efficacy Scale (FES)
The FES has been developed by Tinetti et al. to evaluate the perceived confidence in avoiding falls while performing indoor BADL. This scale consists of 10 items, and each item is scored from 1 (very confident) to 10 (not confident at all). The total score, obtained by summing up the item scores, ranges from 10 to 100. A total score of greater than 70 indicates FOF in the person [7].
Single Item Question
This simple question assesses FOF by asking: “Were you afraid of falling in the past 6 months?” the “yes” answer is followed by the question: “Did you avoid certain activities due to FOF?” the potential answer is yes/ no [5].
Falls Efficacy Scale-International
This scale provides information about FOF while performing indoor and outdoor basic and instrumental activities. The FES-I consists of 16 items (10 items of the original FES and 6 additional items regarding social activities); each item is scored on a 4-point (1=not concerned at all, 4=very concerned) Likert-type scale. The summation of scores provides a total score of 16 (the absence of FOF) to 64 (the extreme concern of FOF) [15].
Translation protocol
First, permission was obtained from the tool developer (Tinetti). Then, according to the International Quality of Life Assessment (IQOLA) protocol, two professional individuals in English translated the scale into Persian. After making necessary revisions, the preliminary forward translated version was produced. In the next stage, the scale was back-translated into English, and after the reconciliation of problematic items, the final version of FES was produced (Figure 1), Persian version in Appendix 1.
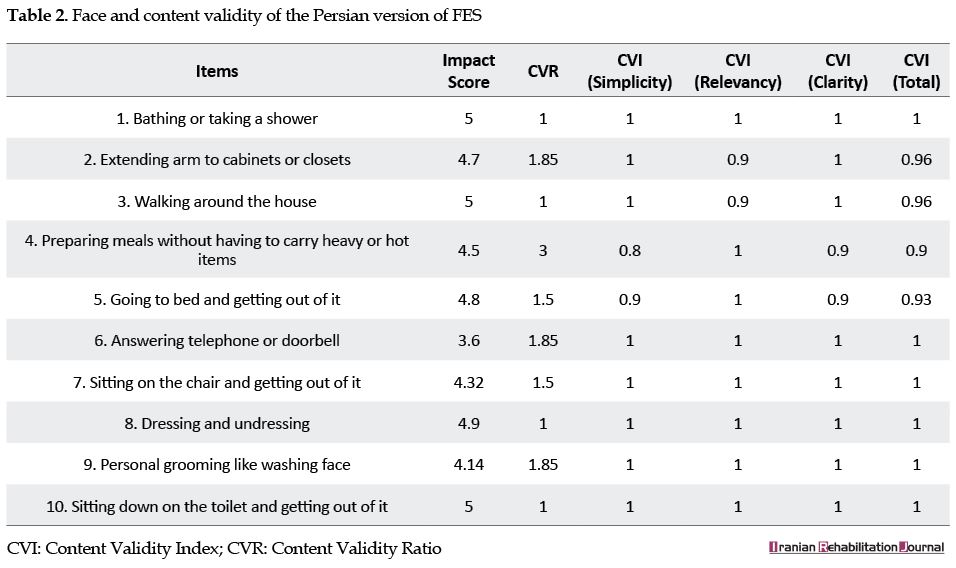
The obtained data were analyzed in SPSS. Kolmogorov-Smirnov Test was applied to assess the data distribution (P<0.05). To investigate the content validity of the translated scale, 10 occupational therapists with at least 5 years of professional experience in elders’ rehabilitation were requested to qualitatively express their opinions. In the quantitative method, according to the Lawshe table for determining the minimum Content Validity Ratio (CVR), items with CVR>0.75 were included. Moreover, Content Validity Index (CVI) values of >0.79, <0.79, and (0.79-0.70), were considered as acceptable, unacceptable, and questionable, respectively. Face validity was examined by the opinions of 10 elder adults in qualitative method, and impact score was calculated in the quantitative method. Impact scores of ≥1.5 were considered acceptable [16].
Construct validity was examined by conducting Exploratory Factor Analysis (EFA) using principal component analysis method by varimax rotation. The appropriateness of the samples and factor analysis was assessed by the Kaiser-Meyer-Olkin (KMO) test and Bartlett’s test of sphericity. Factors were determined according to eigenvalues >1 and the absolute loading values of ≥0.4. Convergent validity was evaluated by the Spearman’s rank correlation coefficient between the FES, and FES-I and SIQ. The strength of correlation based on Munro’s guideline was determined as ≥0.9, (0.89-0.68), (0.67-0.36), and ≤0.35, indicating very high, high, moderate, and low values, respectively [17, 18].
The Cronbach's α coefficient and Intra-Class Correlation (ICC) were used to investigate the internal consistency and test-retest reliability of the scale, respectively. The Cronbach's α coefficient was set as acceptable at ≥0.70, and ICC values above (0.75) and (0.6-0.74) indicated excellent and good reliability, respectively. The scales precision was explored by measuring the Standard Error of Measurement (SEM), by this formula as . Furthermore, the Minimal Detectable Change (MDC) as the change that is beyond the measurement error was calculated at a (95%) confidence interval, as follows: The SEM values of <10% of the maximum score of the scale indicate acceptable absolute reliability. Ceiling and floor effects were determined considering the acceptable level of <15% [19, 20].
3. Results
The Kolmogorov-Smirnov test results suggested that the total score of FES was not normally distributed. The study population (n=100) consisted of 63 males with the Mean±SD age of 72.30±6.06 years. Sixty percent of the participants reported falling experience, and (64%) reported FOF. Table 1 illustrates the detailed demographic characteristics of the study participants. For the total score of FES, ceiling and floor effects were (1%) and (0%), respectively.
Construct validity was examined by conducting Exploratory Factor Analysis (EFA) using principal component analysis method by varimax rotation. The appropriateness of the samples and factor analysis was assessed by the Kaiser-Meyer-Olkin (KMO) test and Bartlett’s test of sphericity. Factors were determined according to eigenvalues >1 and the absolute loading values of ≥0.4. Convergent validity was evaluated by the Spearman’s rank correlation coefficient between the FES, and FES-I and SIQ. The strength of correlation based on Munro’s guideline was determined as ≥0.9, (0.89-0.68), (0.67-0.36), and ≤0.35, indicating very high, high, moderate, and low values, respectively [17, 18].
The Cronbach's α coefficient and Intra-Class Correlation (ICC) were used to investigate the internal consistency and test-retest reliability of the scale, respectively. The Cronbach's α coefficient was set as acceptable at ≥0.70, and ICC values above (0.75) and (0.6-0.74) indicated excellent and good reliability, respectively. The scales precision was explored by measuring the Standard Error of Measurement (SEM), by this formula as . Furthermore, the Minimal Detectable Change (MDC) as the change that is beyond the measurement error was calculated at a (95%) confidence interval, as follows: The SEM values of <10% of the maximum score of the scale indicate acceptable absolute reliability. Ceiling and floor effects were determined considering the acceptable level of <15% [19, 20].
3. Results
The Kolmogorov-Smirnov test results suggested that the total score of FES was not normally distributed. The study population (n=100) consisted of 63 males with the Mean±SD age of 72.30±6.06 years. Sixty percent of the participants reported falling experience, and (64%) reported FOF. Table 1 illustrates the detailed demographic characteristics of the study participants. For the total score of FES, ceiling and floor effects were (1%) and (0%), respectively.
Concerning the validity, the scale’s qualitative content validity was reported as appropriate based on the experts’ opinions. The CVR scores of all items were above (0.75), indicating they should be in the scale. Moreover, all items had a CVI score of ˃0.79; considered as suitable. By the qualitative face validity, all items were recognized as understandable and clear by the elderly. The impact score was obtained as ≥1.5 (Table 2).
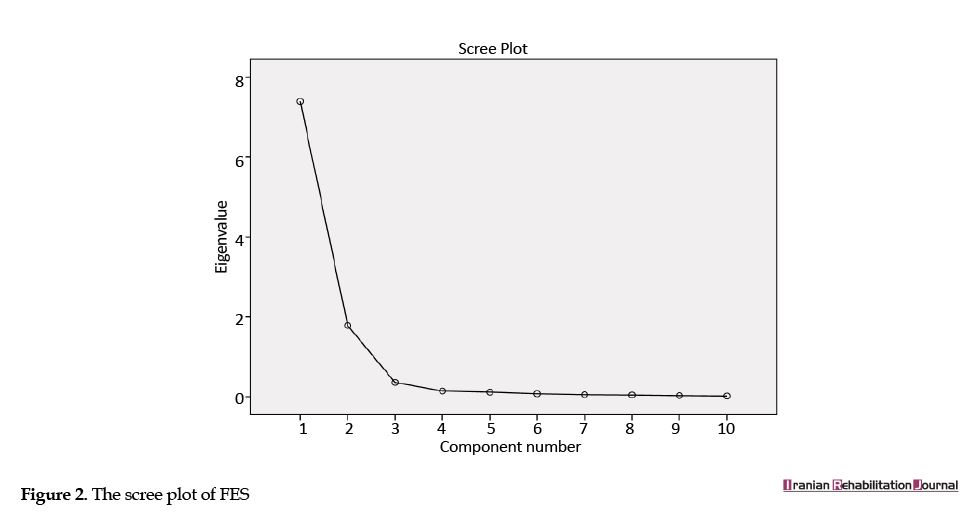
The KMO was equal to (0.92), revealing that the obtained data and sample size were sufficient for factor analysis. In addition, the approximate Chi-squared (X2) value of Bartlett’s Test of sphericity (X2=1788.933, df=45, P<0.0001) indicated the appropriateness of the factor model. The data suitability for factor analysis was confirmed by these two tests. As per (Table 3) and based on the scree plot of (Figure 2), two factors were extracted, which had the eigenvalues of ˃1 and accounted for (91.70%) of the variance. The first factor included items 1 and 10; the second factor included items 2, 3, 4, 5, 6, 7, 8, and 9.
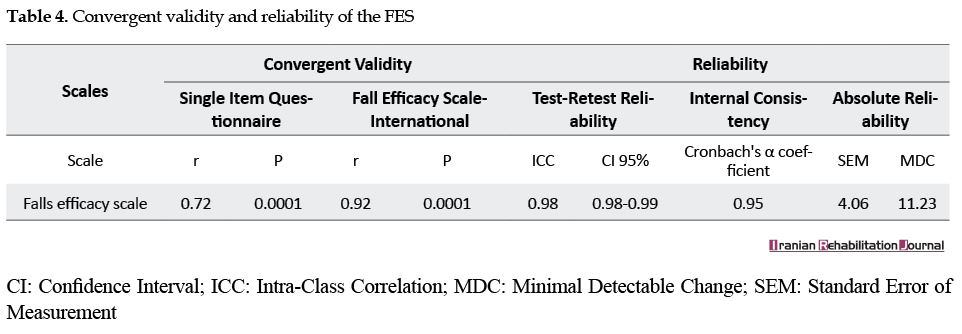
Convergent validity indicated a strong relationship (rho=0.92, P<0.001) between the FES and FES-I and high relationship (rho=0.72, P<0.001) between the FES and SIQ (Table 4).
In terms of the scale’s reliability, its internal consistency was acceptable (α= 0.95), and the test-retest reliability of it was excellent (ICC=0.98, CI: 0.98-0.99). The SEM (2.16) and MDC (11.23) values of the FES indicated an acceptable level of reliability (Table 4).
4. Discussion
The current study was designed to translate FES and investigate its validity and reliability of in the elderly Iranian residents of nursing homes. The obtained results suggested that this scale has a favorable translation, and all the items have acceptable content and face validities. The EFA revealed that the FES has two dimensions among the elderly residents of nursing homes. The convergent validity analysis demonstrated very high to the high correlation between the FES and FES-I, and the FES and SIQ, respectively. An acceptable internal consistency and excellent test-retest reliability were also reported for this scale.
In the present study, no ceiling and floor effects were found. Therefore, the FES is capable of detecting outcome changes and is appropriate for monitoring over-time changes in clinical settings. Previous studies have disregarded its ceiling and floor effects.
In respect of the scale’s validity, all items (10 items) of this scale had appropriate translation and acceptable content validity. These findings are in accordance with the Portuguese version [21]. The achieved EFA results indicated that the FES is a two-dimensional scale. The first factor consisted of item 1 (bathing or taking a shower) and 10 (sitting down on the toilet and getting out of it) and the second factor consisted of other BADLs. Only Bula et al. in the adapted version of FES extracted two factors for this scale [10]. The present results may be explained through the frequent use of bathroom and toilet and experiencing more falls in these places according to the WHO report [2]. The convergent validity analysis results suggested a strong correlation between the FES and FES-I. The obtained results are in accordance with Hauer et al. study [22]. Such a strong correlation indicates the overlapping contents of these scales due to the similarity of items in both scales.
Moreover, the convergent validity between the FES and SIQ indicated a high correlation in this regard. This high correlation may be due to the structure of SIQ, which a general question is asked about FOF; however, in the FES, separate and detailed questions assess FOF during BADL. Previous studies failed to explore the correlation between the FES and SIQ. This is while studies conducted in Iran, England, the Netherlands, and Greece have documented a high correlation between FES-I and SIQ [15].
Concerning the scale’s reliability, the present study suggested an acceptable internal consistency of the FES, which is in line with previous studies (α= 0.75-0.98) in elder adults [7, 10-12, 22-26]. Therefore, this scale’s items cover all aspects of FOF. The excellent obtained test-retest reliability is similar to the results of Bula (2008), Hauer (2010), Mosallanezhad (2011), and Melo (2011) studies (ICC= 0.82-0.99). The probable cause of this similarity can be attributed to the same time interval (4-7 days) and the target population [10, 11, 21, 22]. Tinetti (1990) and Parry (2001) reported moderate to good (ICC=0.58-0.71) test-retest reliability for it. This difference may be due to different applied assessment (self-report) methods [7, 23]. The MDC value of the FES (11.23) indicates that changes greater than 11.23 in the total score of FES with (95%) CI are not the result of measurement error. This finding suggests that the FES has adequate precision.
This study had some limitations. Only older adults who were literate with a cognitive level of ≥21 were assessed. These limitations should be considered for the generalizability of our findings and addressed in future studies.
5. Conclusion
The FES is a reliable and valid scale for evaluating FOF in elderly residents of nursing homes. Therefore, the Persian version of FES can be used for the assessment of FOF in clinical settings and research studies.
Ethical Considerations
Compliance with ethical guidelines
The Ethics Committee of Iran University of Medical Sciences approved this study (Code: IR.IUMS.REC. 27855). All of the study participants signed informed consent to participate in the study. A code number was placed on each participant’s names to provide information confidentiality.
Funding
This research was supported by Iran University of Medical Sciences (Grant No. 95-02-32-27855).
Authors' contributions
Conceptualization: Akram Azad, Mahsa Fadavi-Ghaffari; Methodology: Akram Azad, Mahsa Meimandi; Investigation: Hamze Ghorbanpoor; Writing-original draft: Akram Azad, Mahsa Fadavi-Ghaffari; Writing-review, and editing: Mahsa Meimandi, Zohre Arani Kashani; Funding acquisition: Akram Azad; Supervision: Akram Azad.
Conflict of interest
The authors declare no conflicts of interests.
Appendix (JPEG)
References
4. Discussion
The current study was designed to translate FES and investigate its validity and reliability of in the elderly Iranian residents of nursing homes. The obtained results suggested that this scale has a favorable translation, and all the items have acceptable content and face validities. The EFA revealed that the FES has two dimensions among the elderly residents of nursing homes. The convergent validity analysis demonstrated very high to the high correlation between the FES and FES-I, and the FES and SIQ, respectively. An acceptable internal consistency and excellent test-retest reliability were also reported for this scale.
In the present study, no ceiling and floor effects were found. Therefore, the FES is capable of detecting outcome changes and is appropriate for monitoring over-time changes in clinical settings. Previous studies have disregarded its ceiling and floor effects.
In respect of the scale’s validity, all items (10 items) of this scale had appropriate translation and acceptable content validity. These findings are in accordance with the Portuguese version [21]. The achieved EFA results indicated that the FES is a two-dimensional scale. The first factor consisted of item 1 (bathing or taking a shower) and 10 (sitting down on the toilet and getting out of it) and the second factor consisted of other BADLs. Only Bula et al. in the adapted version of FES extracted two factors for this scale [10]. The present results may be explained through the frequent use of bathroom and toilet and experiencing more falls in these places according to the WHO report [2]. The convergent validity analysis results suggested a strong correlation between the FES and FES-I. The obtained results are in accordance with Hauer et al. study [22]. Such a strong correlation indicates the overlapping contents of these scales due to the similarity of items in both scales.
Moreover, the convergent validity between the FES and SIQ indicated a high correlation in this regard. This high correlation may be due to the structure of SIQ, which a general question is asked about FOF; however, in the FES, separate and detailed questions assess FOF during BADL. Previous studies failed to explore the correlation between the FES and SIQ. This is while studies conducted in Iran, England, the Netherlands, and Greece have documented a high correlation between FES-I and SIQ [15].
Concerning the scale’s reliability, the present study suggested an acceptable internal consistency of the FES, which is in line with previous studies (α= 0.75-0.98) in elder adults [7, 10-12, 22-26]. Therefore, this scale’s items cover all aspects of FOF. The excellent obtained test-retest reliability is similar to the results of Bula (2008), Hauer (2010), Mosallanezhad (2011), and Melo (2011) studies (ICC= 0.82-0.99). The probable cause of this similarity can be attributed to the same time interval (4-7 days) and the target population [10, 11, 21, 22]. Tinetti (1990) and Parry (2001) reported moderate to good (ICC=0.58-0.71) test-retest reliability for it. This difference may be due to different applied assessment (self-report) methods [7, 23]. The MDC value of the FES (11.23) indicates that changes greater than 11.23 in the total score of FES with (95%) CI are not the result of measurement error. This finding suggests that the FES has adequate precision.
This study had some limitations. Only older adults who were literate with a cognitive level of ≥21 were assessed. These limitations should be considered for the generalizability of our findings and addressed in future studies.
5. Conclusion
The FES is a reliable and valid scale for evaluating FOF in elderly residents of nursing homes. Therefore, the Persian version of FES can be used for the assessment of FOF in clinical settings and research studies.
Ethical Considerations
Compliance with ethical guidelines
The Ethics Committee of Iran University of Medical Sciences approved this study (Code: IR.IUMS.REC. 27855). All of the study participants signed informed consent to participate in the study. A code number was placed on each participant’s names to provide information confidentiality.
Funding
This research was supported by Iran University of Medical Sciences (Grant No. 95-02-32-27855).
Authors' contributions
Conceptualization: Akram Azad, Mahsa Fadavi-Ghaffari; Methodology: Akram Azad, Mahsa Meimandi; Investigation: Hamze Ghorbanpoor; Writing-original draft: Akram Azad, Mahsa Fadavi-Ghaffari; Writing-review, and editing: Mahsa Meimandi, Zohre Arani Kashani; Funding acquisition: Akram Azad; Supervision: Akram Azad.
Conflict of interest
The authors declare no conflicts of interests.
Appendix (JPEG)
References
- World Health Organization. World report on ageing and health 2015. Geneva: World Health Organization; 2015.
- World Health Organization. WHO global report on falls prevention in older age. Ageing life course, family and community health. Geneva: World Health Organization; 2007.
- Liu TW, Ng GY, Chung RC, Ng SS. Cognitive behavioral therapy for fear of falling and balance among older people: A systematic review and meta-analysis. Age and Ageing. 2018; 47(4):520-7. [DOI:10.1093/ageing/afy010]
- Scheffer AC, Schuurmans MJ, Van Dijk N, Van Der Hooft T, De Rooij SE. Fear of falling: Measurement strategy, prevalence, risk factors and consequences among older persons. Age and Ageing. 2008; 37(1):19-24. [DOI:10.1093/ageing/afm169]
- Mehdizadeh H, Taghizadeh G, Ghomashchi H, Parnianpour M, Khalaf K, Salehi R, et al. The effects of a short-term memory task on postural control of stroke patients. Topics in Stroke Rehabilitation. 2015; 22(5):335-41.[DOI: 10.1179/1074935714Z.0000000039] [PMID]
- Myers AM, Powell LE, Maki BE, Holliday PJ, Brawley LR, Sherk W. Psychological indicators of balance confidence: Relationship to actual and perceived abilities. The Journals of Gerontology. 1996; 51(1):M37-43. [DOI:10.1093/gerona/51A.1.M37]
- Tinetti ME, Richman D, Powell L. Falls efficacy as a measure of fear of falling. Journal of Gerontology. 1990; 45(6):239-43. [DOI:10.1093/geronj/45.6.P239]
- Kempen GI, Yardley L, Van Haastregt JC, Zijlstra GR, Beyer N, Hauer K, et al. The Short FES-I: A shortened version of the falls efficacy scale-international to assess fear of falling. Age and Ageing. 2007; 37(1):45-50. [DOI:10.1093/ageing/afm157]
- Hellström K, Lindmark B. Fear of falling in patients with stroke: A reliability study. Clinical Rehabilitation. 1999; 13(6):509-17. [DOI:10.1191/026921599677784567]
- Büla CHJ, Martin E, Rochat S, Piot-Ziegler CH. Validation of an adapted falls efficacy scale in older rehabilitation patients. Archives of Physical Medicine and Rehabilitation. 2008; 89(2):291-6. [DOI:10.1016/j.apmr.2007.08.152]
- Mosallanezhad Z, Salavati M, Hellström K, Reza Sotoudeh G, Nilsson Wikmar L, Frändin K. Cross-cultural adaptation, reliability and validity of the Persian version of the modified falls efficacy scale. Disability and Rehabilitation. 2011; 33(25-26):2446-53. [DOI:10.3109/09638288.2011.574774]
- Dadgari A, Hamid TA, Mousavi SA, Hakim N, Hin LP, Dadvar L. Internal consistency of Persian version of falls efficacy scale and activity-specific balance scale. International Journal of Health Studies. 2015;1(3):29-32. [DOI:10.22100/ijhs.v1i3.73]
- Azad A, Taghizadeh G, Ghorbanpoor H, Lajevardi L, Farhadian M. Relationship between laterality and handedness with the higher order sensory functions and manual dexterity of the elderly. Iranian Rehabilitation Journal. 2017; 15(4):367-76. [DOI: 10.29252/nrip.irj.15.4.367]
- Delbaere K, Smith S, Lord S. Development and initial validation of the iconographical falls efficacy scale.The Journals of Gerontology. 2011; 66(6):674-80. [DOI:10.1093/gerona/glr019]
- Khajavi D. Validation and reliability of Persian version of Fall Efficacy Scale-International (FES-I) in community-dwelling older adults. Iranian Journal of Aging. 2013; 8(2):39-47.
- Yaghmaei F. Content validity and its estimation. Journal of Medical Education. 2003; 3(1):25-7.
- Taghizadeh G, Azad A, Kashefi S, Fallah S, Daneshjoo F. The effect of sensory-motor training on hand and upper extremity sensory and motor function in patients with idiopathic Parkinson disease. Journal of Hand Therapy. 2018; 31(4):486-93. [DOI:10.1016/j.jht.2017.08.001]
- Plichta SB, Kelvin EA, Munro BH. Munro’s statistical methods for health care research. 5th edition. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2013.
- Perron BE, Gillespie DF. Key concepts in measurement. Oxford: Oxford University Press; 2015.
- McDowell I. Measuring health: A guide to rating scales and questionnaires. 3rd edition. Oxford: Oxford University Press; 2006.
- De Melo CA. [Adaptação cultural e validação da escala “Falls Efficacy Scale” de Tinetti (Portuguese)]. Ifisionline. 2011; 1(2):33-43.
- Hauer K, Yardley L, Beyer N, Kempen G, Dias N, Campbell M, et al. Validation of the Falls Efficacy Scale and Falls Efficacy Scale International in geriatric patients with and without cognitive impairment: Results of self-report and interview-based questionnaires. Journal of Gerontology. 2010; 56(2):190-9. [DOI:10.1159/000236027] [PMID]
- Parry SW, Steen N, Galloway SR, Kenny RA, Bond J. Falls and confidence related quality of life outcome measures in an older British cohort. Postgraduate Medical Journal. 2001; 77(904):103-8. [DOI:10.1136/pmj.77.904.103]
- Jazaeri SZ, Azad A, Mehdizadeh H, Habibi SA, Mandehgary Najafabadi M, Saberi ZS, et al. The effects of anxiety and external attentional focus on postural control in patients with Parkinson’s disease. PloS One. 2018; 13(2):e0192168. [DOI:10.1371/journal.pone.0192168] [PMID] [PMID]
- Huang T, Wang W. Comparison of three established measures of fear of falling in community-dwelling older adults: Psychometric testing. International Journal of Nursing Studies. 2009; 46(10):1313-9. [DOI:10.1016/j.ijnurstu.2009.03.010]
- Song H, Park S, Kim J. The effects of proprioceptive neuromuscular facilitation integration pattern exercise program on the fall efficacy and gait ability of the elders with experienced fall. Journal Exercise Rehabilitation. 2014; 10(4):236-40. [DOI:10.12965/jer.140141
Article type: Original Research Articles |
Subject:
Occupational therapy
Received: 2018/12/23 | Accepted: 2019/04/29 | Published: 2019/09/1
Received: 2018/12/23 | Accepted: 2019/04/29 | Published: 2019/09/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
