
988368
Sun, Feb 22, 2026

Volume 22, Issue 4 (December 2024)
Iranian Rehabilitation Journal 2024, 22(4): 663-672 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Barathi M, Chew W H, Subramaniam S N R, Loo Y L. Impact of Hallux Valgus on Dynamic Balance in Community-Dwelling Older Adults. Iranian Rehabilitation Journal 2024; 22 (4) :663-672
URL: http://irj.uswr.ac.ir/article-1-1976-en.html
URL: http://irj.uswr.ac.ir/article-1-1976-en.html



1- Department of Physiotherapy, M. Kandiah Faculty of Medicine and Health Sciences, Universiti Tunku Abdul Rahman, Selangor, Malaysia.
2- Department of Physiotherapy, Faculty of Health Sciences, MAHSA University, Jenjarom, Malaysia.
2- Department of Physiotherapy, Faculty of Health Sciences, MAHSA University, Jenjarom, Malaysia.
Full-Text [PDF 583 kb]
(941 Downloads)
| Abstract (HTML) (4912 Views)
Full-Text: (443 Views)
Introduction
Falls pose a significant concern for older adults globally, prompting extensive studies to prevent them by understanding associated risk factors [1]. Some studies have underscored hallux valgus (HV) as a potential risk factor for falls in older adults [2, 3]. This progressive foot condition develops over several years and is characterized by the abduction of the first toe and the medial displacement of the first metatarsal bone [4]. As HV is common among older adults, with prevalence rates as high as 35.7% [5], there is an increasing need to examine the subtle effects of HV severity on different aspects of functional performance in older adults.
Ensuring stability in older adults is crucial for fall prevention, with balance being a key component. To maintain stability during activities of daily living, balance will need to be maintained during walking, turning, getting up from a chair, stepping over objects, taking a step in any direction, and even coordinating various stepping movements to avoid objects [6, 7]. It is, therefore, imperative to assess whether potential risk factors for falls, such as HV, can affect these aspects and consequently influence the risk of falls.
The impact of HV severity on balance has been previously investigated, but the findings have shown inconsistency [8-12]. Menz and Lord were among the first investigators looking at the effects of HV on balance [8]. They investigated the impact of HV on gait and acceleration patterns of the head and pelvis. The results indicated significant moderate to severe HV effects on velocity and step length, while mild HV showed no significant impact. Recently, Yoshida et al. observed a reduction in walking speed among the elderly group with HV compared to those without it [10]. It is worth noting that the sample size was relatively small, consisting of only 10 participants in each group.
Barbee et al., on the other hand, specifically compared older adults with and without HV, revealing no significant changes in walking speed or alterations in the center of mass between the two groups [9]. As seen, there seem to be conflicting results found with the speed of walking, and further studies are required to confirm these findings. While these three studies have used force plates to assess the center of mass, center of pressure, and other gait parameters during walking, the test only consists of walking in a straight line. Maintaining balance in the real world is more than walking in a straight line. The assessment of stability or balance is nuanced, as different tasks, such as turning or stepping over objects, may influence it differently [13, 14]. Thus, it would be interesting to see the effects of HV severity on other aspects of mobility, like turning and getting up from a chair.
There have been studies examining functional outcomes but with inconsistent findings. For example, Shima et al. found an impaired balance using the timed-up and go (TUG) test and Berg’s balance test in the HV group [15]. On the contrary, Kavlak, in a study involving older men and utilizing a goniometer to assess HV, reported no discernible impact on the TUG, thus demonstrating further conflicting findings [12]. It is noteworthy, however, that the reliability of clinical goniometer measurements for HV has been scrutinized in previous research [16].
Concerning the assessment of HV severity, the evaluation methods also vary. These may include radiological evaluation [17], clinical goniometry [16], plantar pressure [16], and the Manchester scale [18]. Notably, the Manchester scale has been established as reliable and valid for assessing HV severity [18, 19]. Its efficiency, cost-effectiveness, and practicality in a busy clinical setting set it apart, making it quickly adopted by clinicians. In contrast to other studies that utilized equipment-intensive methods such as motion sensors [20], foot printers [10], radiological assessments [15], less reliable techniques like goniometry [3, 12] or non-standardized methods [11], in the current study, the authors have opted for a technique that seamlessly translates to real-world clinical practice. Thus, this study was carried out to compare the impact of different HV severity on dynamic balance in community-dwelling older adults utilizing clinically-based tools.
Given the conflicting findings, varied outcome measures, and diverse assessment techniques for measuring HV severity, it is imperative to delve deeper and confirm the effects of HV severity on balance in older adults. To enhance clinical and patient relevance, investigating the impact of HV during tasks such as turning, coordination, and stepping over an objects, activities prevalent in daily life and linked to an increased risk of falls would be beneficial [21]. This study thus aims to compare the effects of varied severity of HV on dynamic balance tests that are relevant to the patient. This study utilizes the TUG test and the 4 square step test (FSST), which examines various components of balance that have not been thoroughly investigated in previous HV trials. This study also uses the Manchester scale to assess the severity of HV. These methods are quick, reliable, and valid. The outcomes are correlated to the risk of falls, and, most importantly, they can be used in most clinical settings, giving the clinician a method to assess the severity of HV’ effects.
There are various ways to use the findings of a study. Clinicians can compare their patient findings and add to the data pool. Methods such as these can lead to increased data that can be easily used to evaluate outcomes of treatment regimens and develop fall prevention programs. In addition, considering the distinctive foot morphology [22, 23] and cultural practices prevalent among older adults in Asian populations, it is crucial to add to the pool of data available. Currently, there is data from countries such as the USA [9], Europe [3], Japan [10], but a lack of data from areas such as Indonesia, Malaysia, and Thailand. It would be interesting to compare clinically significant findings across various morphologies as the world becomes more cosmopolitan. This study will enhance comprehension and provide practical findings for managing balance issues in older adults with HV across diverse ethnicities.
Materials and Methods
This study is a cross-sectional comparative study, examining mean differences between the groups with mild HV and moderate to severe HV. The sample size was determined through G*Power software version 3.1. Based on an alpha error probability of 0.05, a power of 80%, and an effect size of 0.96, drawn from the study by Ji et al. [24], the calculated sample size was set at 30. The participants were community-dwelling older adults above 60 with HV deformity on at least one foot. Recruitment was carried out through a convenience sampling method in Klang Valley, Malaysia, in 2020. The inclusion criteria included a score of 6 on the Katz index of independence in activities of daily living scale and the ability to walk unassisted. The exclusion criteria comprised cognitive, vision, or auditory impairments, prior foot surgeries, systemic diseases, diabetes, severe cardiovascular diseases, and neurological disorders. These criteria were based on those in a previous study [9].
The subject’s HV severity was measured using the Manchester scale. The photographs from the scale were compared with the subjects’ feet, and the HV severity was graded based on the closest resembling photo. Those subjects with mild HV deformity were put in one group, whereas those with moderate and severe HV deformity were put in another group for comparison. For those who presented with bilateral HV deformities with differing severities, the worst severity was considered for the grouping. The Manchester scale’s validity and reliability has been established in previous studies [18, 19], justifying its application in this study.
The categorization of older adults into mild and moderate/severe HV groups aligns with established research methodologies. An initial study comparing a group with mild severity with a group with moderate to severe HV found no significant impact of mild HV on function [8]. Subsequently, recent investigations have predominantly focused on moderate to severe HV [9, 15, 24], comparing this group with participants with mild or no HV. Barbee et al. delved into the effects of moderate to severe HV on balance [9]. Park et al. examined gait patterns in moderate-severity HV [25], and Shima et al. explored postural stability in participants with moderate to severe HV [15].
This classification facilitates a comparative analysis of functional outcomes between the two groups, providing insights to guide decisions on diverse management strategies if necessary. This categorization also streamlines implementation in clinical settings, enabling effective assessment using the Manchester scale. Additionally, it facilitates direct comparisons with normative values for selected outcome measures, enhancing the study’s clinical relevance.
In addition, there have been changes in gait patterns with the prevalence of HV [10, 26]. To measure the dynamic balance, the subjects underwent FSST followed by TUG with their usual footwear. FSST measures an individual’s ability to take a step in different directions. Numerous studies have supported FSST psychometric properties [27-29]. TUG is a performance-based measure of dynamic balance and risk of falls in older adults. It is a highly reliable and valid test [30, 31]. The independent t-test was used to compare the dynamic balance between the two groups. The data were analyzed using SPSS software, version 27, at a significant level of P<0.05.
Data and statistical analyses
Data were analyzed using SPSS software, version 23 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were performed on demographic data, including age (Mean±SD) and gender (frequency). All variables were tested for normality of distribution. The Mean±SD of the mean times for each group for the TUG test and FSST were also calculated. The independent sample t-test was used to determine significant differences between the mild HV group and the moderate to severity HV group when performing the TUG and the FSST. The level of significant differences was set at P<0.05.
Results
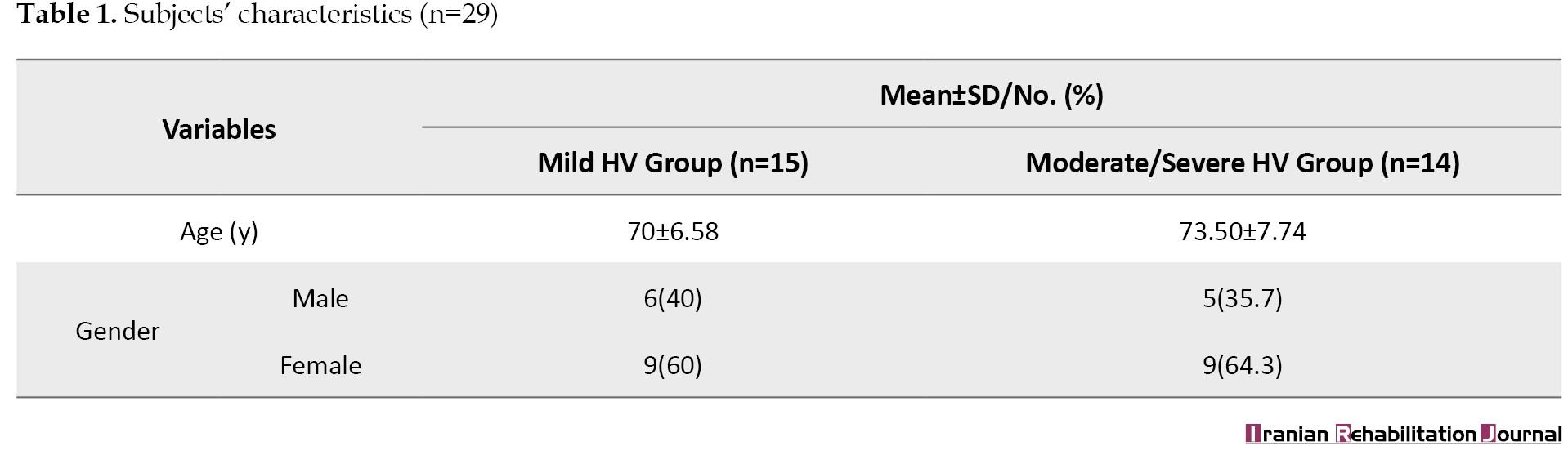
A total of 29 subjects were recruited with a mean age of 71.69±7.26 years. The subjects’ characteristics are provided in Table 1.
Of all subjects, 52% presented with mild HV and 48% with moderate and severe HV. The functional performances of the two groups were assessed using the FSST and the TUG test.
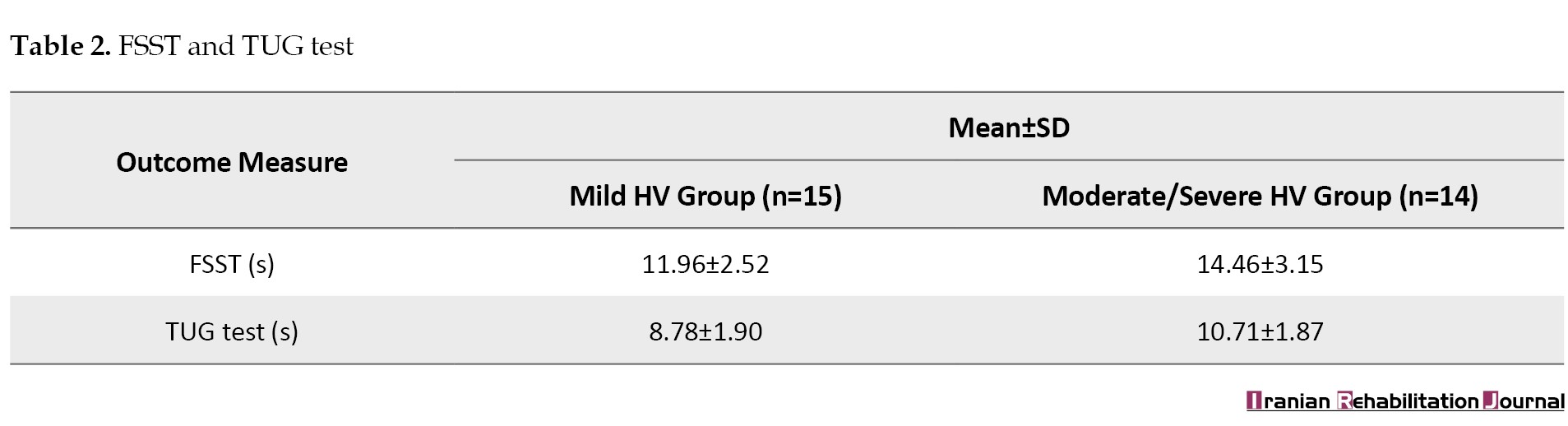
For the mild HV group, the mean scores for FSST and TUG test were 11.96±2.52 and 8.78±1.90 seconds, respectively. Whereas for moderate and severe HV group, the mean scores for FSST and TUG test were 14.46±3.15 and 10.71±1.87 seconds, respectively (Table 2).
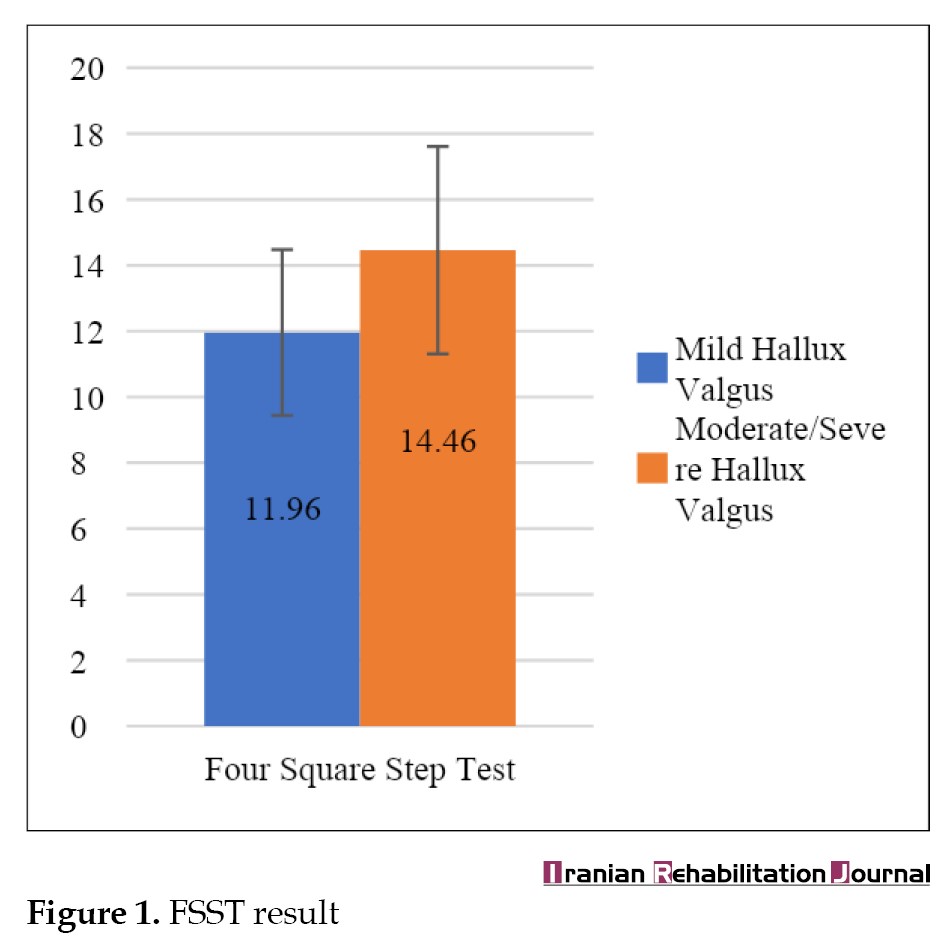
Figures 1 and 2 illustrate the FSST and TUG test results of the mild HV and moderate/severe HV groups.
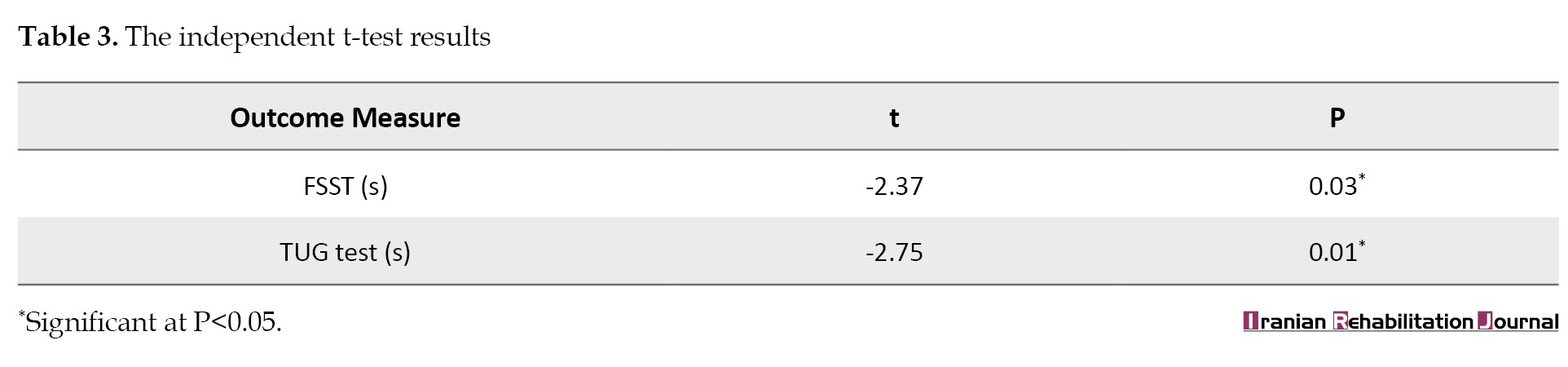
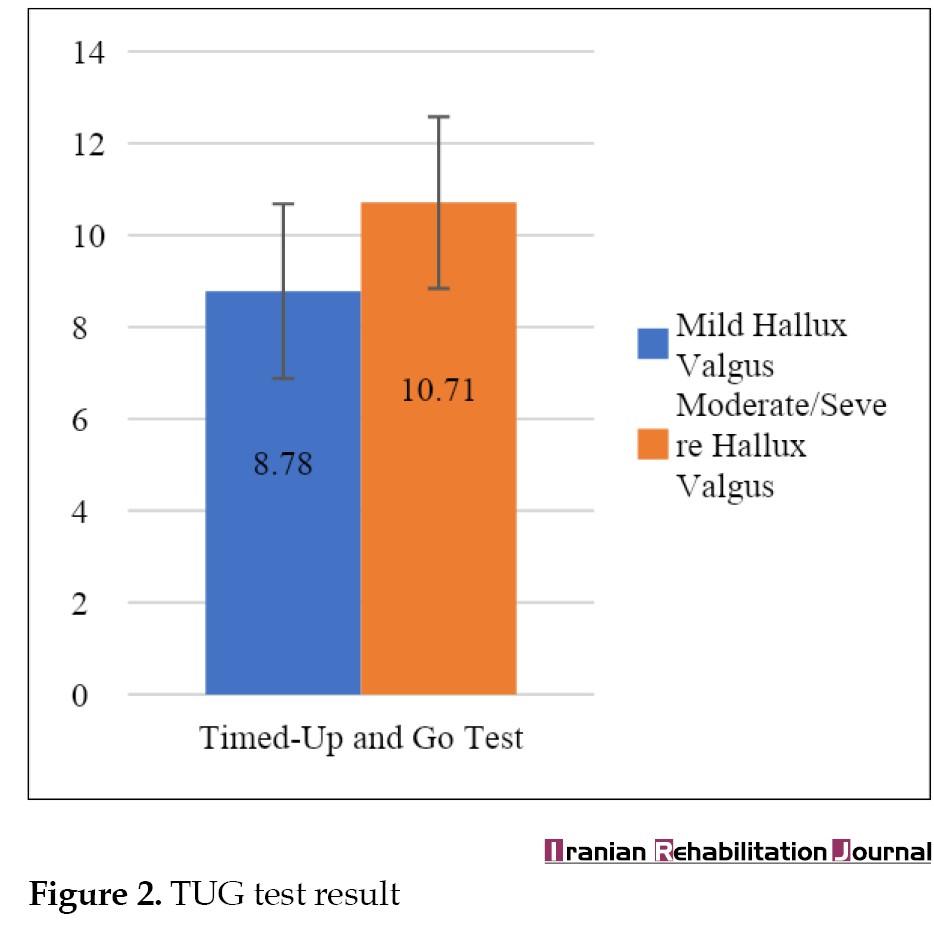 The mild HV group demonstrated significantly less time in completing the FSST (t=-2.37, P=0.025) and TUG (t=-2.75, P=0.011) test compared to the moderate and severe HV group (Table 3).
The mild HV group demonstrated significantly less time in completing the FSST (t=-2.37, P=0.025) and TUG (t=-2.75, P=0.011) test compared to the moderate and severe HV group (Table 3).
Discussion
This study examined the effect of HV severity on dynamic balance in community-dwelling older adults. The study comprised 29 participants, with 15 individuals in the mild HV group (52%) and 14 in the moderate to severe HV group (48%). Both groups exhibited comparable mean ages, with an equivalent distribution of men and women in each group.
In addition, this study aimed to determine the effects of severity of HV, verified by a clinically relevant, valid, and reliable tool, on outcomes that are relevant to patients. The current pressure on the need for evidence-based practice has resulted in bumper crops of trials utilizing technologically advanced and equipment-heavy instruments to assess outcomes [32]. Does this make the gap between the researcher and the clinician even wider? Coster has emphasized that when choosing an outcome measure or a measurement tool, aspects such as relevance to the patient and clinician should be considered [32]. This issue includes evaluating whether the outcome measure can capture change and, if performance-based, determining its suitability for the patient population to perform.
HV has undergone a fair amount of investigation, as evidenced by numerous studies [2, 3, 8, 9, 10, 15, 20]. Despite this, the practical applicability of certain outcomes in a clinical setting has been limited. Specifically, measures such as force platform assessments [9, 20] have been confined to laboratory environments, lacking direct relevance to a patient’s daily functional performance. In this study, we opted for the Manchester scale, a tool acknowledged for validity and reliability. Utilizing the scale’s requirement for capturing foot images is both straightforward and accurate, particularly with the ubiquity of smartphones equipped with capable cameras in most clinical settings. This approach ensures easily comprehensible outcomes for patients, potentially holding greater relevance than more intricate radiological measurements.
In this study, we categorized the patients into mild HV severity and moderate to severe HV severity. People with mild severity seemed to have relatively normal postural sway [33], and those with moderate to severe HV had significantly decreased step length and velocity compared to the no or mild HV group [8]. Subsequently, we found that investigators had omitted the mild severity group from their studies [9, 15]. In this study, we wanted to compare any differences between the two groups, as this may determine any modifications to physiotherapy and other management. In this study, the mild HV group demonstrated a significantly shorter time in completing the FSST and TUG test than the moderate and severe HV group. Shima et al. found similar results, where TUG, falls efficacy scale, Berg’s balance test, and velocity were significantly lower in the HV group (moderate to severe) as compared to the control group with no HV [15]. These researchers, however, had included participants with bilateral HV. The current study’s findings are complementary to those of Shima et al. as it looks at HV found in one foot [15]. This is also important as the prevalence of unilateral HV is at 29.8% of the study population [34].
Biomechanically, the hallux and the first metatarsophalangeal joint play a vital role in gait and stability. The hallux impacts the propulsive phase in walking. Behaving as a pivot, the first metatarsophalangeal joint facilitates the forward transference of the body [2, 35]. There is also reduced capacity to generate force by the great toe, which may decrease peak swing speed in older adults with HV [2, 10, 36]. Moreover, it has been suggested that efficient toe-off is affected by the continued subluxation of the first metatarsophalangeal joint in HV [10]. This condition leads to decreased cadence and speed of walking [10, 36], which may lead to an increased risk of falls [37].
In addition, factors that contributed to decreased walking speed, long foot-flat, and short push-off duration [36]may also alter propulsion during the terminal stance and early swing phase. The longer contact duration at the hind foot may also explain the compensation due to the weak propulsion during weight transfer. Several studies have reported that HV could modify the loading patterns of the foot [36, 38, 39], which may have a detrimental influence on the stability and function of the foot. It has also been reported that older adults with moderate to severe HV also had greater peak pressures and increased pressure-time integral [39]. Previous studies have reported that with HV, there is an increased pressure at the first and second metatarsal heads [38] and at the third to fifth toes [36]. These increased pressures can lead to longer total duration at the hindfoot, decreased metatarsophalangeal motion at the terminal stance, reduced toe-off pitch angle, reduced peak vertical force, and slow peak swing speed, leading to decreased walking speed [36]. The effects will lead to some of the changes found in our study and that of Shima et al. [15].
Barbee et al. found no significant differences in the center of mass-center of pressure inclination angles between people with moderate to severe HV and people without hallux valgus [9]. There could be several reasons for these differing results. The absence of these effects in the study conducted by Barbee et al. might be attributed to the nature of the presented task [9]. It is conceivable that the task was of short duration, conducted in a straight line, and potentially prone to greater practice effects than a task such as the TUG, which inherently involves completing the task as quickly as possible.
The TUG test is one of the assessments used to identify increased fall risk in older adults [1]. Based on a recent study that investigated 169 older adults, it was found that the TUG test time of more than 10.2 s discriminates between the subjects with high and low fall risk [40]. In the present study, the mild hallux valgus group exhibited a TUG test time of 8.78 s, while the moderate/severe HV group recorded a TUG time of 10.71 s. Notably, the latter places the moderate/severe group in a category associated with a high risk of falls, as indicated by Choo et al.’s study in 2021 [40]. This finding holds practical significance for clinicians, considering the widespread use of the TUG test in managing older adults. The inclusion of an assessment for the severity of HV may now be deemed essential, potentially necessitating specific management interventions.
The FSST is a valuable tool for assessing dynamic balance related to stepping tasks in various directions, including forward, backward, and side movements. In a near-fall circumstance, it is essential to be proficient in protective stepping in varied directions. It has been found that when people fall, almost equal numbers of people fall in the forward, backward, and lateral directions [41]. Therefore, the FSST may also be a relevant and necessary measure when assessing the risk of falls in older adults. This study found that the mild HV group demonstrated significantly less time in completing the FSST tests than the moderate and severe HV group. Currently, there are no studies investigating the effects of HV severity on FSST. A previous study has reported that an FSST time of more than 10.14 s discriminates between fallers and non-fallers [42]. In the current study, the FSST time is 11.96 s in the mild HV group and 14.46 s in the moderate/severe HV group, categorizing both groups as fallers. For the FSST test, as it is performance-based and related to function, lower performance should alert the clinician to look at factors such as HV in patients and manage them accordingly.
The present study has successfully filled existing gaps and reinforced the evidence from previous research regarding the adverse impact of HV deformities on the balance performance of older adults. These findings underscore the need for diverse treatment strategies in addressing falls and balance concerns among older adults with HV deformities. The study also emphasizes the potential translatability of methods and the results in the clinical setting.
Conclusion
The study’s findings illuminate the significant impact of HV severity on dynamic balance in older adults. By employing the Manchester scale, a clinically relevant tool, the study unveils distinctions between mild and moderate/severe HV groups in functional tests, emphasizing the practical relevance of these outcomes. This research contributes to addressing gaps in existing literature, providing insights crucial for clinicians in managing older adults with HV. It underscores the potential applicability of its methods and findings in real-world clinical settings.
Study limitations and future recommendations
This study has limitations. The cross-sectional design restricts causal inference and observing changes over time. The sample size may impact generalizability, requiring consideration of larger cohorts. Demographic homogeneity and a specific geographic focus limit broader applicability. While chosen outcome measures are relevant, broader assessments could provide a more comprehensive understanding. The convenience sampling method introduces potential selection bias, affecting external validity. Future studies should address these limitations for a more robust understanding of HV and its impact on dynamic balance.
Future research should prioritize refining user-friendly clinical tools for assessing HV severity in diverse clinical settings. Longitudinal studies are warranted to investigate the progression of HV deformities and their evolving impact on dynamic balance in older adults. Intervention studies targeting this population can evaluate the effectiveness of various interventions in improving balance and reducing fall risk. Incorporating patient-centered outcomes is essential for understanding the holistic implications of HV on daily activities and quality of life. Comparative studies between different measurement tools should be conducted to guide clinicians in their selection. Additionally, initiatives to implement findings in routine clinical practice, educational programs for healthcare professionals and older adults, and collaborative efforts between researchers and clinicians can bridge the gap between research and practical applications. Developing cost-effective assessment tools accessible in various clinical settings will enhance widespread adoption and address the disparity between advanced research instruments and clinical needs.
Ethical Considerations
Compliance with ethical guidelines
The procedures used in this study adhere to the principles of the Declaration of Helsinki. All participants provided their informed consent, and the current study was approved by the Faculty of Health Sciences Research Review Committee of MAHSA University, Malaysia, (Code: FOHS/PT/20/UG76).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Yee Lin Loo, and Mahadevi Barathi; Experiments: Loo Yee Lin; Data interpretation, analysis and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the subjects for their involvement in the study.
References
Falls pose a significant concern for older adults globally, prompting extensive studies to prevent them by understanding associated risk factors [1]. Some studies have underscored hallux valgus (HV) as a potential risk factor for falls in older adults [2, 3]. This progressive foot condition develops over several years and is characterized by the abduction of the first toe and the medial displacement of the first metatarsal bone [4]. As HV is common among older adults, with prevalence rates as high as 35.7% [5], there is an increasing need to examine the subtle effects of HV severity on different aspects of functional performance in older adults.
Ensuring stability in older adults is crucial for fall prevention, with balance being a key component. To maintain stability during activities of daily living, balance will need to be maintained during walking, turning, getting up from a chair, stepping over objects, taking a step in any direction, and even coordinating various stepping movements to avoid objects [6, 7]. It is, therefore, imperative to assess whether potential risk factors for falls, such as HV, can affect these aspects and consequently influence the risk of falls.
The impact of HV severity on balance has been previously investigated, but the findings have shown inconsistency [8-12]. Menz and Lord were among the first investigators looking at the effects of HV on balance [8]. They investigated the impact of HV on gait and acceleration patterns of the head and pelvis. The results indicated significant moderate to severe HV effects on velocity and step length, while mild HV showed no significant impact. Recently, Yoshida et al. observed a reduction in walking speed among the elderly group with HV compared to those without it [10]. It is worth noting that the sample size was relatively small, consisting of only 10 participants in each group.
Barbee et al., on the other hand, specifically compared older adults with and without HV, revealing no significant changes in walking speed or alterations in the center of mass between the two groups [9]. As seen, there seem to be conflicting results found with the speed of walking, and further studies are required to confirm these findings. While these three studies have used force plates to assess the center of mass, center of pressure, and other gait parameters during walking, the test only consists of walking in a straight line. Maintaining balance in the real world is more than walking in a straight line. The assessment of stability or balance is nuanced, as different tasks, such as turning or stepping over objects, may influence it differently [13, 14]. Thus, it would be interesting to see the effects of HV severity on other aspects of mobility, like turning and getting up from a chair.
There have been studies examining functional outcomes but with inconsistent findings. For example, Shima et al. found an impaired balance using the timed-up and go (TUG) test and Berg’s balance test in the HV group [15]. On the contrary, Kavlak, in a study involving older men and utilizing a goniometer to assess HV, reported no discernible impact on the TUG, thus demonstrating further conflicting findings [12]. It is noteworthy, however, that the reliability of clinical goniometer measurements for HV has been scrutinized in previous research [16].
Concerning the assessment of HV severity, the evaluation methods also vary. These may include radiological evaluation [17], clinical goniometry [16], plantar pressure [16], and the Manchester scale [18]. Notably, the Manchester scale has been established as reliable and valid for assessing HV severity [18, 19]. Its efficiency, cost-effectiveness, and practicality in a busy clinical setting set it apart, making it quickly adopted by clinicians. In contrast to other studies that utilized equipment-intensive methods such as motion sensors [20], foot printers [10], radiological assessments [15], less reliable techniques like goniometry [3, 12] or non-standardized methods [11], in the current study, the authors have opted for a technique that seamlessly translates to real-world clinical practice. Thus, this study was carried out to compare the impact of different HV severity on dynamic balance in community-dwelling older adults utilizing clinically-based tools.
Given the conflicting findings, varied outcome measures, and diverse assessment techniques for measuring HV severity, it is imperative to delve deeper and confirm the effects of HV severity on balance in older adults. To enhance clinical and patient relevance, investigating the impact of HV during tasks such as turning, coordination, and stepping over an objects, activities prevalent in daily life and linked to an increased risk of falls would be beneficial [21]. This study thus aims to compare the effects of varied severity of HV on dynamic balance tests that are relevant to the patient. This study utilizes the TUG test and the 4 square step test (FSST), which examines various components of balance that have not been thoroughly investigated in previous HV trials. This study also uses the Manchester scale to assess the severity of HV. These methods are quick, reliable, and valid. The outcomes are correlated to the risk of falls, and, most importantly, they can be used in most clinical settings, giving the clinician a method to assess the severity of HV’ effects.
There are various ways to use the findings of a study. Clinicians can compare their patient findings and add to the data pool. Methods such as these can lead to increased data that can be easily used to evaluate outcomes of treatment regimens and develop fall prevention programs. In addition, considering the distinctive foot morphology [22, 23] and cultural practices prevalent among older adults in Asian populations, it is crucial to add to the pool of data available. Currently, there is data from countries such as the USA [9], Europe [3], Japan [10], but a lack of data from areas such as Indonesia, Malaysia, and Thailand. It would be interesting to compare clinically significant findings across various morphologies as the world becomes more cosmopolitan. This study will enhance comprehension and provide practical findings for managing balance issues in older adults with HV across diverse ethnicities.
Materials and Methods
This study is a cross-sectional comparative study, examining mean differences between the groups with mild HV and moderate to severe HV. The sample size was determined through G*Power software version 3.1. Based on an alpha error probability of 0.05, a power of 80%, and an effect size of 0.96, drawn from the study by Ji et al. [24], the calculated sample size was set at 30. The participants were community-dwelling older adults above 60 with HV deformity on at least one foot. Recruitment was carried out through a convenience sampling method in Klang Valley, Malaysia, in 2020. The inclusion criteria included a score of 6 on the Katz index of independence in activities of daily living scale and the ability to walk unassisted. The exclusion criteria comprised cognitive, vision, or auditory impairments, prior foot surgeries, systemic diseases, diabetes, severe cardiovascular diseases, and neurological disorders. These criteria were based on those in a previous study [9].
The subject’s HV severity was measured using the Manchester scale. The photographs from the scale were compared with the subjects’ feet, and the HV severity was graded based on the closest resembling photo. Those subjects with mild HV deformity were put in one group, whereas those with moderate and severe HV deformity were put in another group for comparison. For those who presented with bilateral HV deformities with differing severities, the worst severity was considered for the grouping. The Manchester scale’s validity and reliability has been established in previous studies [18, 19], justifying its application in this study.
The categorization of older adults into mild and moderate/severe HV groups aligns with established research methodologies. An initial study comparing a group with mild severity with a group with moderate to severe HV found no significant impact of mild HV on function [8]. Subsequently, recent investigations have predominantly focused on moderate to severe HV [9, 15, 24], comparing this group with participants with mild or no HV. Barbee et al. delved into the effects of moderate to severe HV on balance [9]. Park et al. examined gait patterns in moderate-severity HV [25], and Shima et al. explored postural stability in participants with moderate to severe HV [15].
This classification facilitates a comparative analysis of functional outcomes between the two groups, providing insights to guide decisions on diverse management strategies if necessary. This categorization also streamlines implementation in clinical settings, enabling effective assessment using the Manchester scale. Additionally, it facilitates direct comparisons with normative values for selected outcome measures, enhancing the study’s clinical relevance.
In addition, there have been changes in gait patterns with the prevalence of HV [10, 26]. To measure the dynamic balance, the subjects underwent FSST followed by TUG with their usual footwear. FSST measures an individual’s ability to take a step in different directions. Numerous studies have supported FSST psychometric properties [27-29]. TUG is a performance-based measure of dynamic balance and risk of falls in older adults. It is a highly reliable and valid test [30, 31]. The independent t-test was used to compare the dynamic balance between the two groups. The data were analyzed using SPSS software, version 27, at a significant level of P<0.05.
Data and statistical analyses
Data were analyzed using SPSS software, version 23 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were performed on demographic data, including age (Mean±SD) and gender (frequency). All variables were tested for normality of distribution. The Mean±SD of the mean times for each group for the TUG test and FSST were also calculated. The independent sample t-test was used to determine significant differences between the mild HV group and the moderate to severity HV group when performing the TUG and the FSST. The level of significant differences was set at P<0.05.
Results
A total of 29 subjects were recruited with a mean age of 71.69±7.26 years. The subjects’ characteristics are provided in Table 1.
Of all subjects, 52% presented with mild HV and 48% with moderate and severe HV. The functional performances of the two groups were assessed using the FSST and the TUG test.
For the mild HV group, the mean scores for FSST and TUG test were 11.96±2.52 and 8.78±1.90 seconds, respectively. Whereas for moderate and severe HV group, the mean scores for FSST and TUG test were 14.46±3.15 and 10.71±1.87 seconds, respectively (Table 2).
Figures 1 and 2 illustrate the FSST and TUG test results of the mild HV and moderate/severe HV groups.
Discussion
This study examined the effect of HV severity on dynamic balance in community-dwelling older adults. The study comprised 29 participants, with 15 individuals in the mild HV group (52%) and 14 in the moderate to severe HV group (48%). Both groups exhibited comparable mean ages, with an equivalent distribution of men and women in each group.
In addition, this study aimed to determine the effects of severity of HV, verified by a clinically relevant, valid, and reliable tool, on outcomes that are relevant to patients. The current pressure on the need for evidence-based practice has resulted in bumper crops of trials utilizing technologically advanced and equipment-heavy instruments to assess outcomes [32]. Does this make the gap between the researcher and the clinician even wider? Coster has emphasized that when choosing an outcome measure or a measurement tool, aspects such as relevance to the patient and clinician should be considered [32]. This issue includes evaluating whether the outcome measure can capture change and, if performance-based, determining its suitability for the patient population to perform.
HV has undergone a fair amount of investigation, as evidenced by numerous studies [2, 3, 8, 9, 10, 15, 20]. Despite this, the practical applicability of certain outcomes in a clinical setting has been limited. Specifically, measures such as force platform assessments [9, 20] have been confined to laboratory environments, lacking direct relevance to a patient’s daily functional performance. In this study, we opted for the Manchester scale, a tool acknowledged for validity and reliability. Utilizing the scale’s requirement for capturing foot images is both straightforward and accurate, particularly with the ubiquity of smartphones equipped with capable cameras in most clinical settings. This approach ensures easily comprehensible outcomes for patients, potentially holding greater relevance than more intricate radiological measurements.
In this study, we categorized the patients into mild HV severity and moderate to severe HV severity. People with mild severity seemed to have relatively normal postural sway [33], and those with moderate to severe HV had significantly decreased step length and velocity compared to the no or mild HV group [8]. Subsequently, we found that investigators had omitted the mild severity group from their studies [9, 15]. In this study, we wanted to compare any differences between the two groups, as this may determine any modifications to physiotherapy and other management. In this study, the mild HV group demonstrated a significantly shorter time in completing the FSST and TUG test than the moderate and severe HV group. Shima et al. found similar results, where TUG, falls efficacy scale, Berg’s balance test, and velocity were significantly lower in the HV group (moderate to severe) as compared to the control group with no HV [15]. These researchers, however, had included participants with bilateral HV. The current study’s findings are complementary to those of Shima et al. as it looks at HV found in one foot [15]. This is also important as the prevalence of unilateral HV is at 29.8% of the study population [34].
Biomechanically, the hallux and the first metatarsophalangeal joint play a vital role in gait and stability. The hallux impacts the propulsive phase in walking. Behaving as a pivot, the first metatarsophalangeal joint facilitates the forward transference of the body [2, 35]. There is also reduced capacity to generate force by the great toe, which may decrease peak swing speed in older adults with HV [2, 10, 36]. Moreover, it has been suggested that efficient toe-off is affected by the continued subluxation of the first metatarsophalangeal joint in HV [10]. This condition leads to decreased cadence and speed of walking [10, 36], which may lead to an increased risk of falls [37].
In addition, factors that contributed to decreased walking speed, long foot-flat, and short push-off duration [36]may also alter propulsion during the terminal stance and early swing phase. The longer contact duration at the hind foot may also explain the compensation due to the weak propulsion during weight transfer. Several studies have reported that HV could modify the loading patterns of the foot [36, 38, 39], which may have a detrimental influence on the stability and function of the foot. It has also been reported that older adults with moderate to severe HV also had greater peak pressures and increased pressure-time integral [39]. Previous studies have reported that with HV, there is an increased pressure at the first and second metatarsal heads [38] and at the third to fifth toes [36]. These increased pressures can lead to longer total duration at the hindfoot, decreased metatarsophalangeal motion at the terminal stance, reduced toe-off pitch angle, reduced peak vertical force, and slow peak swing speed, leading to decreased walking speed [36]. The effects will lead to some of the changes found in our study and that of Shima et al. [15].
Barbee et al. found no significant differences in the center of mass-center of pressure inclination angles between people with moderate to severe HV and people without hallux valgus [9]. There could be several reasons for these differing results. The absence of these effects in the study conducted by Barbee et al. might be attributed to the nature of the presented task [9]. It is conceivable that the task was of short duration, conducted in a straight line, and potentially prone to greater practice effects than a task such as the TUG, which inherently involves completing the task as quickly as possible.
The TUG test is one of the assessments used to identify increased fall risk in older adults [1]. Based on a recent study that investigated 169 older adults, it was found that the TUG test time of more than 10.2 s discriminates between the subjects with high and low fall risk [40]. In the present study, the mild hallux valgus group exhibited a TUG test time of 8.78 s, while the moderate/severe HV group recorded a TUG time of 10.71 s. Notably, the latter places the moderate/severe group in a category associated with a high risk of falls, as indicated by Choo et al.’s study in 2021 [40]. This finding holds practical significance for clinicians, considering the widespread use of the TUG test in managing older adults. The inclusion of an assessment for the severity of HV may now be deemed essential, potentially necessitating specific management interventions.
The FSST is a valuable tool for assessing dynamic balance related to stepping tasks in various directions, including forward, backward, and side movements. In a near-fall circumstance, it is essential to be proficient in protective stepping in varied directions. It has been found that when people fall, almost equal numbers of people fall in the forward, backward, and lateral directions [41]. Therefore, the FSST may also be a relevant and necessary measure when assessing the risk of falls in older adults. This study found that the mild HV group demonstrated significantly less time in completing the FSST tests than the moderate and severe HV group. Currently, there are no studies investigating the effects of HV severity on FSST. A previous study has reported that an FSST time of more than 10.14 s discriminates between fallers and non-fallers [42]. In the current study, the FSST time is 11.96 s in the mild HV group and 14.46 s in the moderate/severe HV group, categorizing both groups as fallers. For the FSST test, as it is performance-based and related to function, lower performance should alert the clinician to look at factors such as HV in patients and manage them accordingly.
The present study has successfully filled existing gaps and reinforced the evidence from previous research regarding the adverse impact of HV deformities on the balance performance of older adults. These findings underscore the need for diverse treatment strategies in addressing falls and balance concerns among older adults with HV deformities. The study also emphasizes the potential translatability of methods and the results in the clinical setting.
Conclusion
The study’s findings illuminate the significant impact of HV severity on dynamic balance in older adults. By employing the Manchester scale, a clinically relevant tool, the study unveils distinctions between mild and moderate/severe HV groups in functional tests, emphasizing the practical relevance of these outcomes. This research contributes to addressing gaps in existing literature, providing insights crucial for clinicians in managing older adults with HV. It underscores the potential applicability of its methods and findings in real-world clinical settings.
Study limitations and future recommendations
This study has limitations. The cross-sectional design restricts causal inference and observing changes over time. The sample size may impact generalizability, requiring consideration of larger cohorts. Demographic homogeneity and a specific geographic focus limit broader applicability. While chosen outcome measures are relevant, broader assessments could provide a more comprehensive understanding. The convenience sampling method introduces potential selection bias, affecting external validity. Future studies should address these limitations for a more robust understanding of HV and its impact on dynamic balance.
Future research should prioritize refining user-friendly clinical tools for assessing HV severity in diverse clinical settings. Longitudinal studies are warranted to investigate the progression of HV deformities and their evolving impact on dynamic balance in older adults. Intervention studies targeting this population can evaluate the effectiveness of various interventions in improving balance and reducing fall risk. Incorporating patient-centered outcomes is essential for understanding the holistic implications of HV on daily activities and quality of life. Comparative studies between different measurement tools should be conducted to guide clinicians in their selection. Additionally, initiatives to implement findings in routine clinical practice, educational programs for healthcare professionals and older adults, and collaborative efforts between researchers and clinicians can bridge the gap between research and practical applications. Developing cost-effective assessment tools accessible in various clinical settings will enhance widespread adoption and address the disparity between advanced research instruments and clinical needs.
Ethical Considerations
Compliance with ethical guidelines
The procedures used in this study adhere to the principles of the Declaration of Helsinki. All participants provided their informed consent, and the current study was approved by the Faculty of Health Sciences Research Review Committee of MAHSA University, Malaysia, (Code: FOHS/PT/20/UG76).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Yee Lin Loo, and Mahadevi Barathi; Experiments: Loo Yee Lin; Data interpretation, analysis and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the subjects for their involvement in the study.
References
- Montero-Odasso M, van der Velde N, Martin FC, Petrovic M, Tan MP, Ryg J, et al. World guidelines for falls prevention and management for older adults: A global initiative. Age and Ageing. 2022; 51(9):afac205. [DOI:10.1093/ageing/afac205]
- Menz HB, Morris ME, Lord SR. Foot and ankle risk factors for falls in older people: A prospective study. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2006; 61(8):866-70. [DOI:10.1093/gerona/61.8.866]
- Sánchez-Sanjuan A, Romero-Morales C, Alfaro-Santafé J, Almenar-Arasanz AJ, Gómez-Bernal A, Pareja-Galeano H. Foot anatomical structural variations increase the risk of falls in older adults. Applied Sciences (Switzerland). 2022; 12(19):9825. [DOI:10.3390/app12199825]
- Kuhn J, Alvi F. Hallux Valgus. Treasure Island: StatPearls [Internet]. 2022. [Link]
- Nix S, Smith M, Vicenzino B. Prevalence of hallux valgus in the general population: A systematic review and meta-analysis. Journal of Foot and Ankle Research. 2010; 3(1):21. [DOI:10.1186/1757-1146-3-21]
- Leach JM, Mellone S, Palumbo P, Bandinelli S, Chiari L. Natural turn measures predict recurrent falls in community-dwelling older adults: A longitudinal cohort study. Scientific Reports. 2018; 8:4316. [DOI:10.1038/s41598-018-22492-6]
- Halvarsson A, Dohrn IM, Ståhle A. Taking balance training for older adults one step further: The rationale for and a description of a proven balance training programme. Clinical Rehabilitation. 2015; 29(5):417-25. [DOI:10.1177/0269215514546770]
- Menz HB, Lord SR. Gait instability in older people with hallux valgus. Foot & Ankle International. 2005; 26(6):483-9. [DOI:10.1177/107110070502600610]
- Barbee CE, Buddhadev HH, Chalmers GR, Suprak DN. The effects of hallux valgus and walking speed on dynamic balance in older adults. Gait & Posture. 2020; 80:137-42. [DOI:10.1016/j.gaitpost.2020.05.039]
- Yoshida T, Tanino Y, Nakao T, Yamazaki W, Suzuki T. Examination of gait characteristics and related factors in elderly subjects with and without hallux valgus. Progress in Rehabilitation Medicine. 2021; 6(0):n/a. [DOI:10.2490/prm.20210028]
- Omae H, Ohsawa T, Hio N, Tsunoda K, Omodaka T, Hashimoto S, et al. Hallux valgus deformity and postural sway: A cross-sectional study. BMC Musculoskeletal Disorders. 2021; 22:503. [DOI:10.1186/s12891-021-04385-4]
- Kavlak Y. The relation of hallux valgus severity with foot function and balance in older men. Fizyoterapi Rehabilitasyon. 2015; 26(2):93-9. [Link]
- Dingwell JB, Render AC, Desmet DM, Cusumano JP. Generalizing stepping concepts to non-straight walking. Journal of Biomechanics. 2023; 161:111840. [DOI:10.1016/j.jbiomech.2023.111840] [PMID]
- Conradsson D, Paquette C, Franzén E. Medio-lateral stability during walking turns in older adults. PLoS One. 2018; 13(6):e0198455. [DOI:10.1371/journal.pone.0198455] [PMID]
- Shima H, Yasuda T, Hida T, Tsujinaka S, Togei K, Nakamura G, et al. Postural stability impairment in patients with bilateral hallux valgus: A case-control study using a stabilometer. Foot and Ankle Surgery. 2021; 27(4):395-9. [DOI:10.1016/j.fas.2020.05.005] [PMID]
- Janssen DM, Sanders AP, Guldemond NA, Hermus J, Walenkamp GH, van Rhijn LW. A comparison of hallux valgus angles assessed with computerised plantar pressure measurements, clinical examination and radiography in patients with diabetes. Journal of Foot and Ankle Research. 2014; 7:33. [DOI:10.1186/1757-1146-7-33] [PMID]
- Heineman N, Liu G, Pacicco T, Dessouky R, Wukich DK, Chhabra A. Clinical and imaging assessment and treatment of hallux valgus. Acta Radiologica (Stockholm, Sweden: 1987). 2020; 61(1):56-66. [DOI:10.1177/0284185119847675] [PMID]
- Menz HB, Munteanu SE. Radiographic validation of the Manchester scale for the classification of hallux valgus deformity. Rheumatology. 2005; 44(8):1061-6. [DOI:10.1093/rheumatology/keh687] [PMID]
- Menz HB, Fotoohabadi MR, Wee E, Spink MJ. Validity of self-assessment of hallux valgus using the Manchester scale BMC Musculoskeletal Disorders. 2010; 11:215. [DOI:10.1186/1471-2474-11-215] [PMID]
- Puszczalowska-Lizis E, Bujas P, Omorczyk J, Jandzis S, Zak M. Feet deformities are correlated with impaired balance and postural stability in seniors over 75. Plos One. 2017; 12(9):e0183227. [DOI:10.1371/journal.pone.0183227] [PMID]
- Cocks AJ, Young WR, Ellmers TJ, Jackson RC, Williams AM. Concern about falling is associated with segmental control when turning in older adults. Gait & Posture. 2021; 88:105-8. [DOI:10.1016/j.gaitpost.2021.05.011] [PMID]
- Jurca A, Žabkar J, Džeroski S. Analysis of 1.2 million foot scans from North America, Europe and Asia. Scientific Reports. 2019; 9(1):19155. [DOI:10.1038/s41598-019-55432-z] [PMID]
- Shariff SM, Merican AF, Shariff AA. Foot morphological between ethnic groups. In: Zakaria N, Gupta D, editors. Anthropometry, Apparel Sizing and Design. Sawston: Woodhead Publishing; 2019. [DOI:10.1016/B978-0-08-102604-5.00012-3]
- Ji M, Park H, Lee H, Yoo M, Ko E, Woo Y. Effects of hallux valgus angle on one-legged stance and gait parameters in young adults: A preliminary study. Physical Therapy Rehabilitation Science. 2020; 9:10-7. [DOI:10.14474/ptrs.2020.9.1.10]
- Park C, Kang N, Jeon K, Park K. Quantifying the dynamic stability of gait patterns in people with hallux valgus. Applied Bionics and Biomechanics. 2021; 2021. [DOI:10.1155/2021/5543704]
- Kim YW. Relationship between hallux valgus severity and 3d ground reaction force in individuals with hallux valgus deformity during gait. Korean Society of Physical Medicine. 2021; 16(3):21-7. [Link]
- Moore M, Barker K. The validity and reliability of the four square step test in different adult populations: A systematic review. Systematic Reviews. 2017; 6(1):187. [DOI:10.1186/s13643-017-0577-5]
- Cleary K, Skornyakov E. Predicting falls in older adults using the four square step test. Physiotherapy Theory and Practice. 2017; 33(10):766-71. [DOI:10.1080/09593985.2017.1354951]
- Dite W, Temple VA. A clinical test of stepping and change of direction to identify multiple falling older adults. Archives of Physical Medicine and Rehabilitation. 2002; 83(11):1566-71. [DOI:10.1053/apmr.2002.35469] [PMID]
- Steffen T, Hacker T, Mollinger L. Age-and gender-related test performance in community-dwelling elderly people: six-minute walk test, berg balance scale, timed up & go test, and gait speeds. Physical Therapy. 2002; 82(2):128–37. [DOI:10.1093/ptj/82.2.128]
- Shumway-Cook A, Brawer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the timed up & go test. Physical Therapy. 2000; 80(9):896-903. [DOI:10.1093/ptj/80.9.896]
- Coster WJ. Making the best match: Selecting outcome measures for clinical trials and outcome studies. The American Journal of Occupational Therapy. 2013; 67(2):162–70. [DOI:10.5014/ajot.2013.006015]
- Hurn SE, Vicenzino B, Smith MD. Functional impairments characterizing mild, moderate, and severe hallux valgus. 67(2), 162–170. 2015; 67(1):80-8. [DOI:10.1002/acr.22380]
- Nishimura A, Kato K, Fukuda A, Nakazora S, Yamada T, Uchida A, et al. Prevalence of hallux valgus and risk factors among Japanese community dwellers. Journal of Orthopaedic Science. 2014; 19(2):257-62. [DOI:10.1007/s00776-013-0513-z]
- Al-Munajjed AA, Bischoff JE, Dharia MA, Telfer S, Woodburn J, Carbes S. Metatarsal loading during gait - A Musculoskeletal Analysis. Journal of Biomechanical Engineering. 2016; 138(3):034503. [DOI:10.1115/1.4032413]
- Chopra S, Moerenhout K, Crevoisier X. Characterization of gait in female patients with moderate to severe hallux valgus deformity. Clinical Biomechanics. 2015; 30(6):629-35. [DOI:10.1016/j.clinbiomech.2015.03.021]
- Kyrdalen IL, Thingstad P, Sandvik L, Ormstad H. Associations between gait speed and well-known fall risk factors among community-dwelling older adults. Physiotherapy Research International. 2019; 24(1):e1743. [DOI:10.1002/pri.1743]
- Mickle KJ, Munro BJ, Lord SR, Menz HB, Steele JR. ISB Clinical Biomechanics Award 2009. Toe weakness and deformity increase the risk of falls in older people. Clinical Biomechanics. 2009; 24(10):787-91. [DOI:10.1016/j.clinbiomech.2009.08.011]
- Zhang B, Lu Q. A current review of foot disorder and plantar pressure alternation in the elderly. Physical Activity and Health. 2020; 4(1):95-107. [DOI:10.5334/paah.57]
- Choo PL, Tou NX, Jun Pang BW, Lau LK, Jabbar KA, Seah WT, et al. Timed Up and Go (TUG) reference values and predictive cut-offs for fall risk and disability in Singaporean community-dwelling adults: Yishun cross-sectional study and singapore longitudinal aging study. Journal of the American Medical Directors Association. 2021; 22(8):1640-5. [DOI:10.1016/j.jamda.2021.03.002]
- Crenshaw JR, Bernhardt KA, Achenbach SJ, Atkinson EJ, Khosla S, Kaufman KR, et al. The circumstances, orientations, and impact locations of falls in community-dwelling older women. Archives of Gerontology and Geriatrics. 2017; 73:240-7. [DOI:10.1016/j.archger.2017.07.011] [PMID]
- Mathurapongsakul P, Siriphorn A. Four square step test with foam is more accurate than those without foam for discriminating between older adults with and without fall history. Journal of Aging and Physical Activity. 2018; 26(4):624-8. [DOI:10.1123/japa.2017-0363] [PMID]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2023/05/23 | Accepted: 2024/02/17 | Published: 2024/12/20
Received: 2023/05/23 | Accepted: 2024/02/17 | Published: 2024/12/20
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
