
988368
Tue, Jul 28, 2026

Volume 23, Issue 2 (June 2025)
Iranian Rehabilitation Journal 2025, 23(2): 131-140 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nazir A, Lidyana L, Sayyidah S. A Review of the Management, Outcomes, and Barriers to Rehabilitation in Patients With Post-intensive Care Syndrome. Iranian Rehabilitation Journal 2025; 23 (2) :131-140
URL: http://irj.uswr.ac.ir/article-1-2016-en.html
URL: http://irj.uswr.ac.ir/article-1-2016-en.html



1- Department of Physical and Rehabilitation Medicine, Faculty of Medicine, Dr. Hasan Sadikin General Hospital, Padjadjaran University, Bandung, Indonesia.
2- Department of Psychiatric, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia.
3- Post Graduate Medical Program, Faculty of Medicine, Padjadjaran University, Bandung, Indonesia.
2- Department of Psychiatric, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia.
3- Post Graduate Medical Program, Faculty of Medicine, Padjadjaran University, Bandung, Indonesia.
Full-Text [PDF 663 kb]
(998 Downloads)
| Abstract (HTML) (4627 Views)
Full-Text: (367 Views)
Introduction
Advances in knowledge and technology of intensive care unit (ICU) management have facilitated an increased survival rate from critical illnesses. However, many of these survivors often have long-term complications [1]. Physical, cognitive, and psychological dysfunctions, known as post-intensive care syndrome (PICS), are types of ICU-related dysfunctions caused by the severity of critical illness and the use of mechanical ventilation. PICS can also extend to affect the family, leading to PICS family (PICS-F) [2, 3].
The most common physical dysfunction found in PICS is ICU-acquired weakness (ICU-AW), a weakness of skeletal muscles that occurs during an ICU admission [3]. ICU-AW incidence increased by 24%-55% among patients with 7-10 days of care [4]. Cognitive dysfunctions associated with PICS include impairment of memory, executive function, language, attention, and visuospatial ability [5]. After three years, 15% of ICU survivors were diagnosed with new-onset dementia [6]. One study found that 74% of 821 ICU patients experienced delirium during hospitalization [7]. Another study reported that nearly 80% of patients experienced cognitive impairment three months after ICU stay [8]. Psychological disorders found in PICS included anxiety (70%), depression (30%), and post-traumatic stress disorder (PTSD) (10-50%) [5]. A study by Vlake et al. found that 59% (95% CI, 44% to 74%) of patients experienced psychological PICS in the form of depression, PTSD, or both. The incidence of PTSD and depression was higher in psychological PICS than in non-psychological PICS [9].
The impact of PICS extends well beyond the ICU, affecting patients' quality of life. A previous study found that ICU-AW symptoms lasted 2-5 years in 85-95% of patients [10]. Cognitive impairment affected 70% of patients one year after ICU care [8]. Depression, anxiety, and sleep disturbances lasted more than a year in 10-50% of patients, while PTSD symptoms persisted for over four years in 33% of family members [10].
One of the preventive measures for PICS is the implementation of rehabilitation programs through early mobilization in the ICU. Physical rehabilitation performed immediately after ICU admission improves functional outcomes [11]. A previous review found that the incidence of muscle weakness was lower in the early rehabilitation group. However, no significant changes were found in cognitive and psychological functions [12].
Currently, no standard guidelines exist for the management of PICS. The increasing number of ICU survivors poses a significant challenge to rehabilitation. This review aimed to explore the rehabilitation management of PICS, focusing on interventions, outcomes, and barriers.
Materials and Methods
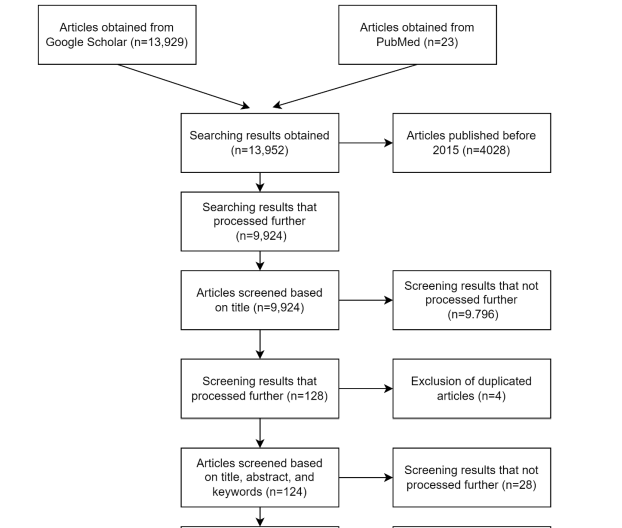
This study systematically reviewed articles on the rehabilitation management of patients with PICS. Articles published within the last five years were searched using the Google Scholar and PubMed databases. The keywords used included "PICS," "post-intensive care syndrome," "rehabilitation," "physical," "cognitive, and psychological disorders," "intensive care unit-acquired weakness," "ICU-AW," "interventions," "outcomes," "barriers," "physical impairment," "cognitive impairment," "dementia," "delirium," "psychological impairment," "anxiety," "depression," "post-traumatic stress disorder," "PTSD," "management," "early mobilization," "early rehabilitation," and "physical therapy." The types of articles analyzed were original and review papers written in English. Meanwhile, those irrelevant to the topic and unavailable or could not be accessed in full text were excluded. The extracted data included interventions, outcomes, and barriers to rehabilitation. The articles were first filtered based on titles and abstracts, then the full text was read, and filtration was performed based on publication periods and inclusion or exclusion criteria.
Results
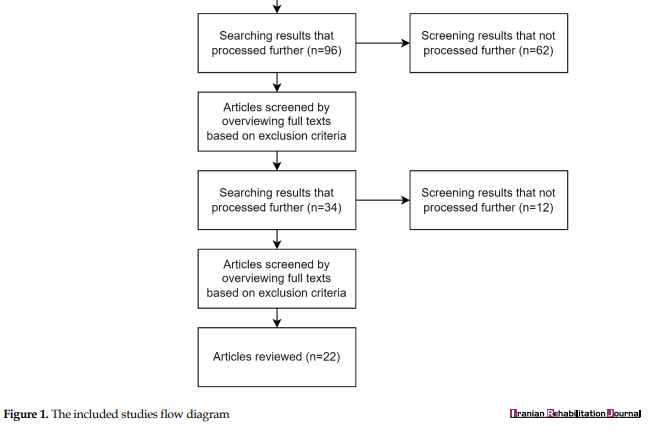
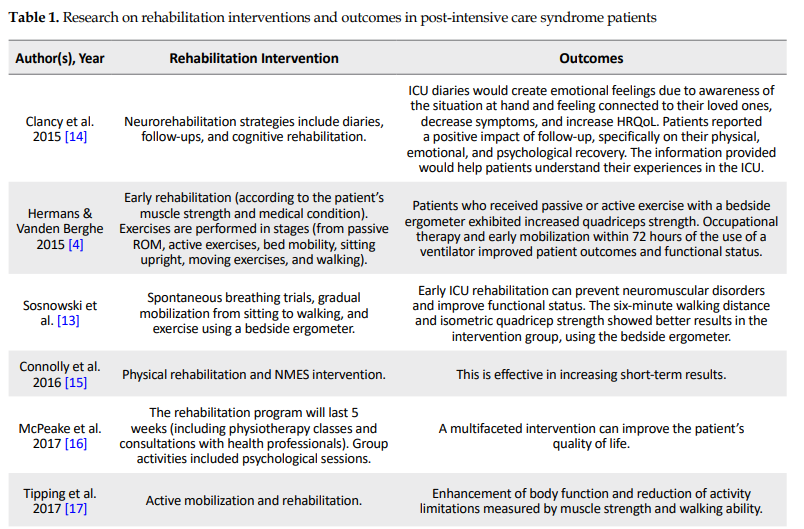
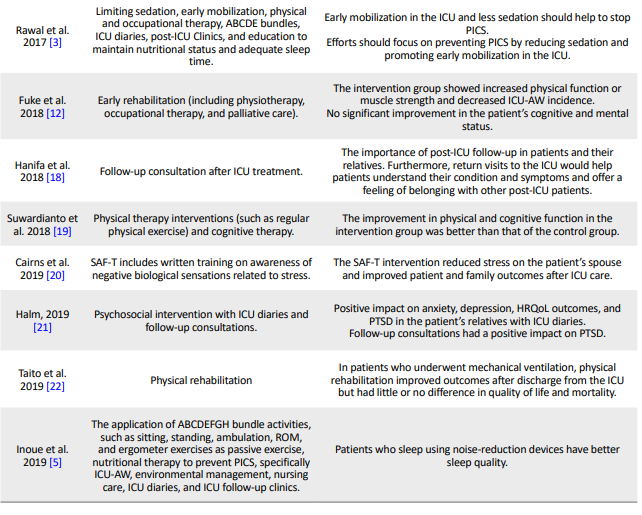
Based on the titles and abstracts, 22 articles relevant to the topic were selected from 128 (Figure 1). Eighteen articles discussed rehabilitation interventions for patients with PICS (Table 1), 16 discussed rehabilitation outcomes (Table 1), and seven discussed barriers (Table 2). Table 3 presents a summary of this review.
.PNG)
Discussion
Interventions and outcomes of rehabilitation in patients with PICS
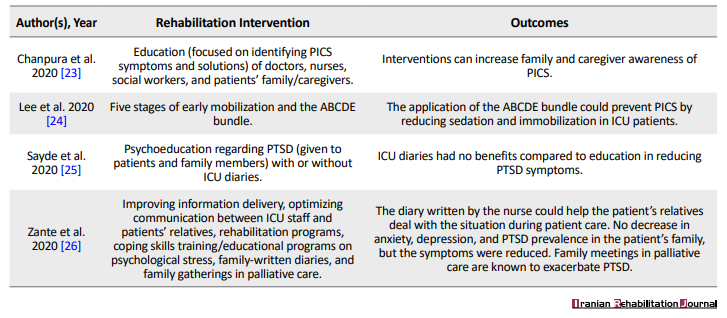
The management of PICS was implemented to prevent disability and worsening of patients’ or their families’ functional disorders [3]. ICU rehabilitation aims to restore patients’ physical, psychological, and cognitive functions [13]. Preventive measures to reduce the risk of PICS include the A, airway management, assessment, prevention, and management of pain; B, breathing trials; C, choice of analgesia and sedation, coordination of care and communication; D, delirium assessment, prevention, and management; and E, early mobility and exercise (ABCDE) bundle, early mobilization and physical therapy, cognitive and psychological rehabilitation, education, as well as follow-up management. The forms of intervention and outcomes/effects of rehabilitation were discussed in 18 articles (Table 1).
The ABCDE bundle was applied to prevent PICS by reducing sedation and immobilization among patients admitted to the ICU [3, 5, 24]. The components consist of ABCDE [5].
Physical rehabilitation's goals include decreasing the duration of immobilization, maintaining or restoring the patient's ability to perform daily activities, and improving the quality of life [4, 5]. This was achieved through early mobilization, active and passive exercise programs, ambulation, and occupational therapy.
Early rehabilitation initiated within seven days of ICU admission has increased physical function (measured by the medical research council) and decreased ICU-AW incidence. However, cognitive function and mental status did not improve significantly [12]. One of the crucial components of rehabilitation intervention is to conduct spontaneous breathing trials to determine the readiness of patients to breathe without support, thereby preventing prolonged use of ventilator [13].
Physical exercise in ICU patients includes passive and active mobilization. Passive exercises, such as passive range of motion (ROM), were performed for unconscious patients [4]. In addition, an ergometer is another suitable intervention. One study found that the 6-minute walking distance and isometric quadriceps strength were increased in the intervention group who received the bedside ergometer intervention [13]. Early administration of neuromuscular electrical stimulation (NMES) intervention in the ICU proved beneficial and effective in improving short-term outcomes [15].
Active mobilization is performed with ROM exercises, early mobilization, and ambulation. Early mobilization consists of sitting upright and on the edge of the bed, shifting and transferring, standing, moving from the bed, sitting on a chair, and walking [4, 24] Ambulation was performed when patients can stand with balance, march in place, and perform balance exercises with weight shifting [13].
Mobilization and rehabilitation improve physical function and reduce activity limitations in ICU patients. These two aspects were evaluated by muscle strength and walking ability assessment [17]. The early rehabilitation program enhanced physical function after discharge from the ICU. However, little or no difference was observed in the mortality and quality of life [22].
A previous study provided physical therapy accompanied by cognitive therapy for patients in the ICU. Physical function was assessed using the physical function measurement tool, and cognitive function using the mini-mental state examination. The intervention group showed a significant effect, with a higher improvement in physical function than the control group. It was concluded that regular physical exercise increases neuromuscular activity and prevents apoptosis in the muscle. In addition, cognitive function improved significantly in the intervention group [19].
Psychological rehabilitation helps patients cope with their psychological trauma and vulnerability and restore independence after a critical illness [14]. The use of the ICU diary is known to positively impact patients and families. This diary is a note written by family, doctors, or medical personnel to record a patient's condition during ICU care. It could demonstrate the orientation, assist relatives in coping with treatment, and prevent PICS by relieving anxiety, depression, and PTSD symptoms [5, 26]. The ICU diaries positively impacted health-related quality of life (HRQoL) [21]. Although the use of an ICU diary may not reduce the prevalence of anxiety, depression, and PTSD in the patient's family, it can mitigate PTSD symptoms [26].
Consistent follow-up and consultations after ICU discharge will help patients and relatives understand the critical illness's condition and symptoms. This can aid patients in returning to work and achieving their previous level of functionality [18, 21]. In several countries across Europe and America, healthcare providers have developed post-ICU follow-up clinics to provide support to survivors. This clinic offers counselling, rehabilitation support, cognitive function assessment, mental health care, and assistance for patients and their families [3, 5].
The intensive care syndrome: Promoting independence and return to employment program was developed over five weeks and consisted of physiotherapy classes and meetings with healthcare workers, pharmacists, and physiotherapists. Patients and caregivers also attended group discussions, which included psychological sessions. The results showed that this program improved patients' quality of life and functional abilities. However, further investigation was needed to evaluate its full impact [16].
Educational sessions in the management of PICS are given to patients and their families, focusing on psychoeducation regarding psychological stress, PTSD, and training in coping skills [25, 26]. One study provided education to patients' families/caregivers. The participants in the educational sessions included doctors, nurses, and social workers. Each session was conducted once a week for 45 minutes. The education was focused on identifying symptoms of PICS and its solutions and providing education for the family/caregiver that could increase their awareness of this syndrome [23]. However, another found that providing educational interventions alongside an ICU diary did not yield significantly different benefits compared to education alone for reducing PTSD symptoms associated with intensive care [25].
Barriers to rehabilitation in PICS patients
The identified barriers to the management of patients with PICS were included patient, structural, and culture-related (Table 2).
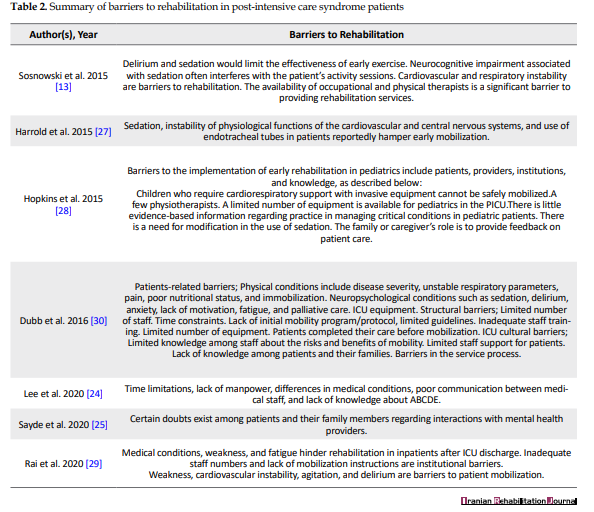
Patients admitted to the ICU require intensive therapy to support their body functions, such as mechanical ventilation or other supporting devices. The disease severity and other medical conditions, including immobilization, instability of cardiovascular and respiratory functions, and weakness may interfere with rehabilitation programs [24, 27, 29, 30]. based on the early ABCDE bundle (admitted to the ICU from June – August 2013 In addition, neuropsychological and cognitive conditions associated with sedation, anxiety, and delirium also interfere with rehabilitation programs [13, 29, 30]. A previous study found that the endotracheal tube insertion hindered early mobilization [27]. there is little data on baseline mobilisation practises and the barriers to them for patients of all admission diagnoses. Methods: The objectives of the study were to (1 Children reliant on invasive support for cardiorespiratory functions might not be mobilized safely [28].
Limited numbers of staff and therapists are structural barriers associated with the rehabilitation of PICS [13, 24, 28]. Other barriers include a lack of training and direction for the mobilization program and the unavailability of equipment. Some pediatric ICUs lack specialized equipment for pediatric patients, thereby limiting the implementation of rehabilitation programs [28-30].
Rehabilitation practice remains limited due to the lack of guidelines/protocols regarding early mobilization.30 Limited evidence also exists regarding managing patients with critical conditions, specifically in children. In pediatric rehabilitation, the family is crucial in providing information about treatment and patient comfort. The family or caregiver could also facilitate communication with the patient and participate in physical therapy and mobilization programs [28].
The lack of knowledge among patients, families, and medical staff about PICS and its risks or benefits constitutes a cultural barrier [24, 30]. One study found that implementing the ABCDE bundle faced barriers of limited time, lack of human resources, variable patient conditions, poor communication between medical personnel, and lack of knowledge about the program [24].
Conclusion
In conclusion, rehabilitation for patients with PICS is essential to prevent the progression of disorders, disability, and restore functional status. Rehabilitation management should begin with a preventive approach using the ABCDE bundle, early physical mobilization, and cognitive or psychological therapy. The use of ICU diary, education, consultations, and post-ICU follow-up contributed to rehabilitation success. Rehabilitation programs improved patients’ conditions and reduced symptoms of PICS. However, various barriers to its implementation have been identified, including patient, structural, and cultural barriers. These barriers included a lack of equipment, limited human resources, and a lack of awareness among patients, their families, and health care professionals.
Ethical Considerations
Compliance with ethical guidelines
This article is a review of literature with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology, data collection, funding acquisition and resources: Arnengsih Nazir and Shofiyyah Sayyidah; Supervision: Arnengsih Nazir and Lynna Lidyana; Investigation, data analysis and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge the Faculty of Medicine, Padjadjaran University, for the opportunity to conduct this review.
References
Advances in knowledge and technology of intensive care unit (ICU) management have facilitated an increased survival rate from critical illnesses. However, many of these survivors often have long-term complications [1]. Physical, cognitive, and psychological dysfunctions, known as post-intensive care syndrome (PICS), are types of ICU-related dysfunctions caused by the severity of critical illness and the use of mechanical ventilation. PICS can also extend to affect the family, leading to PICS family (PICS-F) [2, 3].
The most common physical dysfunction found in PICS is ICU-acquired weakness (ICU-AW), a weakness of skeletal muscles that occurs during an ICU admission [3]. ICU-AW incidence increased by 24%-55% among patients with 7-10 days of care [4]. Cognitive dysfunctions associated with PICS include impairment of memory, executive function, language, attention, and visuospatial ability [5]. After three years, 15% of ICU survivors were diagnosed with new-onset dementia [6]. One study found that 74% of 821 ICU patients experienced delirium during hospitalization [7]. Another study reported that nearly 80% of patients experienced cognitive impairment three months after ICU stay [8]. Psychological disorders found in PICS included anxiety (70%), depression (30%), and post-traumatic stress disorder (PTSD) (10-50%) [5]. A study by Vlake et al. found that 59% (95% CI, 44% to 74%) of patients experienced psychological PICS in the form of depression, PTSD, or both. The incidence of PTSD and depression was higher in psychological PICS than in non-psychological PICS [9].
The impact of PICS extends well beyond the ICU, affecting patients' quality of life. A previous study found that ICU-AW symptoms lasted 2-5 years in 85-95% of patients [10]. Cognitive impairment affected 70% of patients one year after ICU care [8]. Depression, anxiety, and sleep disturbances lasted more than a year in 10-50% of patients, while PTSD symptoms persisted for over four years in 33% of family members [10].
One of the preventive measures for PICS is the implementation of rehabilitation programs through early mobilization in the ICU. Physical rehabilitation performed immediately after ICU admission improves functional outcomes [11]. A previous review found that the incidence of muscle weakness was lower in the early rehabilitation group. However, no significant changes were found in cognitive and psychological functions [12].
Currently, no standard guidelines exist for the management of PICS. The increasing number of ICU survivors poses a significant challenge to rehabilitation. This review aimed to explore the rehabilitation management of PICS, focusing on interventions, outcomes, and barriers.
Materials and Methods
This study systematically reviewed articles on the rehabilitation management of patients with PICS. Articles published within the last five years were searched using the Google Scholar and PubMed databases. The keywords used included "PICS," "post-intensive care syndrome," "rehabilitation," "physical," "cognitive, and psychological disorders," "intensive care unit-acquired weakness," "ICU-AW," "interventions," "outcomes," "barriers," "physical impairment," "cognitive impairment," "dementia," "delirium," "psychological impairment," "anxiety," "depression," "post-traumatic stress disorder," "PTSD," "management," "early mobilization," "early rehabilitation," and "physical therapy." The types of articles analyzed were original and review papers written in English. Meanwhile, those irrelevant to the topic and unavailable or could not be accessed in full text were excluded. The extracted data included interventions, outcomes, and barriers to rehabilitation. The articles were first filtered based on titles and abstracts, then the full text was read, and filtration was performed based on publication periods and inclusion or exclusion criteria.
Results
Based on the titles and abstracts, 22 articles relevant to the topic were selected from 128 (Figure 1). Eighteen articles discussed rehabilitation interventions for patients with PICS (Table 1), 16 discussed rehabilitation outcomes (Table 1), and seven discussed barriers (Table 2). Table 3 presents a summary of this review.
Discussion
Interventions and outcomes of rehabilitation in patients with PICS
The management of PICS was implemented to prevent disability and worsening of patients’ or their families’ functional disorders [3]. ICU rehabilitation aims to restore patients’ physical, psychological, and cognitive functions [13]. Preventive measures to reduce the risk of PICS include the A, airway management, assessment, prevention, and management of pain; B, breathing trials; C, choice of analgesia and sedation, coordination of care and communication; D, delirium assessment, prevention, and management; and E, early mobility and exercise (ABCDE) bundle, early mobilization and physical therapy, cognitive and psychological rehabilitation, education, as well as follow-up management. The forms of intervention and outcomes/effects of rehabilitation were discussed in 18 articles (Table 1).
The ABCDE bundle was applied to prevent PICS by reducing sedation and immobilization among patients admitted to the ICU [3, 5, 24]. The components consist of ABCDE [5].
Physical rehabilitation's goals include decreasing the duration of immobilization, maintaining or restoring the patient's ability to perform daily activities, and improving the quality of life [4, 5]. This was achieved through early mobilization, active and passive exercise programs, ambulation, and occupational therapy.
Early rehabilitation initiated within seven days of ICU admission has increased physical function (measured by the medical research council) and decreased ICU-AW incidence. However, cognitive function and mental status did not improve significantly [12]. One of the crucial components of rehabilitation intervention is to conduct spontaneous breathing trials to determine the readiness of patients to breathe without support, thereby preventing prolonged use of ventilator [13].
Physical exercise in ICU patients includes passive and active mobilization. Passive exercises, such as passive range of motion (ROM), were performed for unconscious patients [4]. In addition, an ergometer is another suitable intervention. One study found that the 6-minute walking distance and isometric quadriceps strength were increased in the intervention group who received the bedside ergometer intervention [13]. Early administration of neuromuscular electrical stimulation (NMES) intervention in the ICU proved beneficial and effective in improving short-term outcomes [15].
Active mobilization is performed with ROM exercises, early mobilization, and ambulation. Early mobilization consists of sitting upright and on the edge of the bed, shifting and transferring, standing, moving from the bed, sitting on a chair, and walking [4, 24] Ambulation was performed when patients can stand with balance, march in place, and perform balance exercises with weight shifting [13].
Mobilization and rehabilitation improve physical function and reduce activity limitations in ICU patients. These two aspects were evaluated by muscle strength and walking ability assessment [17]. The early rehabilitation program enhanced physical function after discharge from the ICU. However, little or no difference was observed in the mortality and quality of life [22].
A previous study provided physical therapy accompanied by cognitive therapy for patients in the ICU. Physical function was assessed using the physical function measurement tool, and cognitive function using the mini-mental state examination. The intervention group showed a significant effect, with a higher improvement in physical function than the control group. It was concluded that regular physical exercise increases neuromuscular activity and prevents apoptosis in the muscle. In addition, cognitive function improved significantly in the intervention group [19].
Psychological rehabilitation helps patients cope with their psychological trauma and vulnerability and restore independence after a critical illness [14]. The use of the ICU diary is known to positively impact patients and families. This diary is a note written by family, doctors, or medical personnel to record a patient's condition during ICU care. It could demonstrate the orientation, assist relatives in coping with treatment, and prevent PICS by relieving anxiety, depression, and PTSD symptoms [5, 26]. The ICU diaries positively impacted health-related quality of life (HRQoL) [21]. Although the use of an ICU diary may not reduce the prevalence of anxiety, depression, and PTSD in the patient's family, it can mitigate PTSD symptoms [26].
Consistent follow-up and consultations after ICU discharge will help patients and relatives understand the critical illness's condition and symptoms. This can aid patients in returning to work and achieving their previous level of functionality [18, 21]. In several countries across Europe and America, healthcare providers have developed post-ICU follow-up clinics to provide support to survivors. This clinic offers counselling, rehabilitation support, cognitive function assessment, mental health care, and assistance for patients and their families [3, 5].
The intensive care syndrome: Promoting independence and return to employment program was developed over five weeks and consisted of physiotherapy classes and meetings with healthcare workers, pharmacists, and physiotherapists. Patients and caregivers also attended group discussions, which included psychological sessions. The results showed that this program improved patients' quality of life and functional abilities. However, further investigation was needed to evaluate its full impact [16].
Educational sessions in the management of PICS are given to patients and their families, focusing on psychoeducation regarding psychological stress, PTSD, and training in coping skills [25, 26]. One study provided education to patients' families/caregivers. The participants in the educational sessions included doctors, nurses, and social workers. Each session was conducted once a week for 45 minutes. The education was focused on identifying symptoms of PICS and its solutions and providing education for the family/caregiver that could increase their awareness of this syndrome [23]. However, another found that providing educational interventions alongside an ICU diary did not yield significantly different benefits compared to education alone for reducing PTSD symptoms associated with intensive care [25].
Barriers to rehabilitation in PICS patients
The identified barriers to the management of patients with PICS were included patient, structural, and culture-related (Table 2).
Patients admitted to the ICU require intensive therapy to support their body functions, such as mechanical ventilation or other supporting devices. The disease severity and other medical conditions, including immobilization, instability of cardiovascular and respiratory functions, and weakness may interfere with rehabilitation programs [24, 27, 29, 30]. based on the early ABCDE bundle (admitted to the ICU from June – August 2013 In addition, neuropsychological and cognitive conditions associated with sedation, anxiety, and delirium also interfere with rehabilitation programs [13, 29, 30]. A previous study found that the endotracheal tube insertion hindered early mobilization [27]. there is little data on baseline mobilisation practises and the barriers to them for patients of all admission diagnoses. Methods: The objectives of the study were to (1 Children reliant on invasive support for cardiorespiratory functions might not be mobilized safely [28].
Limited numbers of staff and therapists are structural barriers associated with the rehabilitation of PICS [13, 24, 28]. Other barriers include a lack of training and direction for the mobilization program and the unavailability of equipment. Some pediatric ICUs lack specialized equipment for pediatric patients, thereby limiting the implementation of rehabilitation programs [28-30].
Rehabilitation practice remains limited due to the lack of guidelines/protocols regarding early mobilization.30 Limited evidence also exists regarding managing patients with critical conditions, specifically in children. In pediatric rehabilitation, the family is crucial in providing information about treatment and patient comfort. The family or caregiver could also facilitate communication with the patient and participate in physical therapy and mobilization programs [28].
The lack of knowledge among patients, families, and medical staff about PICS and its risks or benefits constitutes a cultural barrier [24, 30]. One study found that implementing the ABCDE bundle faced barriers of limited time, lack of human resources, variable patient conditions, poor communication between medical personnel, and lack of knowledge about the program [24].
Conclusion
In conclusion, rehabilitation for patients with PICS is essential to prevent the progression of disorders, disability, and restore functional status. Rehabilitation management should begin with a preventive approach using the ABCDE bundle, early physical mobilization, and cognitive or psychological therapy. The use of ICU diary, education, consultations, and post-ICU follow-up contributed to rehabilitation success. Rehabilitation programs improved patients’ conditions and reduced symptoms of PICS. However, various barriers to its implementation have been identified, including patient, structural, and cultural barriers. These barriers included a lack of equipment, limited human resources, and a lack of awareness among patients, their families, and health care professionals.
Ethical Considerations
Compliance with ethical guidelines
This article is a review of literature with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology, data collection, funding acquisition and resources: Arnengsih Nazir and Shofiyyah Sayyidah; Supervision: Arnengsih Nazir and Lynna Lidyana; Investigation, data analysis and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge the Faculty of Medicine, Padjadjaran University, for the opportunity to conduct this review.
References
- Desai SV, Law TJ, Needham DM. Long-term complications of critical care. Critical Care Medicine. 2011; 39(2):371-9. [DOI:10.1097/CCM.0b013e3181fd66e5] [PMID]
- Colbenson GA, Johnson A, Wilson ME. Post-intensive care syndrome: impact, prevention, and management. Breathe (Sheffield, England). 2019; 15(2):98-101. [DOI:10.1183/20734735.0013-2019] [PMID]
- Rawal G, Yadav S, Kumar R. Post-intensive Care Syndrome: An Overview. Journal of Translational Internal Medicine. 2017; 5(2):90-2. [DOI:10.1515/jtim-2016-0016] [PMID]
- Hermans G, Van den Berghe G. Clinical review: Intensive care unit acquired weakness. Crit Care. 2015; 19(1):274. [DOI:10.1186/s13054-015-0993-7] [PMID]
- Inoue S, Hatakeyama J, Kondo Y, Hifumi T, Sakuramoto H, Kawasaki T, et al. Post-intensive care syndrome: Its pathophysiology, prevention, and future directions. Acute Medicine & Surgery. 2019; 6(3):233-46. [DOI:10.1002/ams2.415] [PMID]
- Guerra C, Hua M, Wunsch H. Risk of a diagnosis of dementia for elderly medicare beneficiaries after intensive care. Anesthesiology. 2015; 123(5):1105-12. [DOI:10.1097/ALN.0000000000000821] [PMID]
- Pandharipande PP, Girard TD, Jackson JC, Morandi A, Thompson JL, Pun BT, et al. Long-term cognitive impairment after critical illness. The New England Journal of Medicine. 2013; 369(14):1306-16. [DOI:10.1056/NEJMoa1301372] [PMID]
- Girard TD, Jackson JC, Pandharipande PP, Pun BT, Thompson JL, Shintani AK, et al. Delirium as a predictor of long-term cognitive impairment in survivors of critical illness. Critical Care Medicine. 2010; 38(7):1513-20. [DOI:10.1097/CCM.0b013e3181e47be1] [PMID]
- Vlake JH, Van Genderen ME, Schut A, Verkade M, Wils EJ, Gommers D, et al. Patients suffering from psychological impairments following critical illness are in need of information. Journal of Intensive Care. 2020; 8:6. [DOI:10.1186/s40560-019-0422-0] [PMID]
- Harvey MA. The truth about consequences--Post-intensive care syndrome in intensive care unit survivors and their families. Critical Care Medicine. 2012; 40(8):2506-7. [DOI:10.1097/CCM.0b013e318258e943] [PMID]
- Griffith DM, Walsh TS. Physical rehabilitation and critical illness. Anaesthesia & Intensive Care Medicine. 2019; 20(1):25-8. [DOI:10.1016/j.mpaic.2018.11.006]
- Fuke R, Hifumi T, Kondo Y, Hatakeyama J, Takei T, Yamakawa K, et al. Early rehabilitation to prevent postintensive care syndrome in patients with critical illness: A systematic review and meta-analysis. BMJ Open. 2018; 8(5):e019998.[DOI:10.1136/bmjopen-2017-019998] [PMID]
- Sosnowski K, Lin F, Mitchell ML, White H. Early rehabilitation in the intensive care unit: An integrative literature review. Australian Critical Care. 2015; 28(4):216-25. [DOI:10.1016/j.aucc.2015.05.002] [PMID]
- Clancy O, Edginton T, Casarin A, Vizcaychipi MP. The psychological and neurocognitive consequences of critical illness. A pragmatic review of current evidence. Journal of The Intensive Care Society. 2015; 16(3):226-33. [DOI:10.1177/1751143715569637] [PMID]
- Connolly B, O'Neill B, Salisbury L, Blackwood B; Enhanced Recovery After Critical Illness Programme Group. Physical rehabilitation interventions for adult patients during critical illness: An overview of systematic reviews. Thorax. 2016; 71(10):881-90. [DOI:10.1136/thoraxjnl-2015-208273] [PMID]
- McPeake J, Shaw M, Iwashyna TJ, Daniel M, Devine H, Jarvie L, et al. Intensive Care Syndrome: Promoting independence and Return to Employment (InS:PIRE). Early evaluation of a complex intervention. PLoS One. 2017; 12(11):e0188028.[DOI:10.1371/journal.pone.0188028] [PMID]
- Tipping CJ, Harrold M, Holland A, Romero L, Nisbet T, Hodgson CL. The effects of active mobilisation and rehabilitation in ICU on mortality and function: A systematic review. Intensive Care Medicine. 2017; 43(2):171-83. [DOI:10.1007/s00134-016-4612-0] [PMID]
- Hanifa ALB, Glæemose AO, Laursen BS. Picking up the pieces: Qualitative evaluation of follow-up consultations post intensive care admission. Intensive & Critical Care Nursing. 2018; 48:85-91. [DOI:10.1016/j.iccn.2018.06.004] [PMID]
- Suwardianto H, Prasetyo A, Utami RS. Effects of physical-cognitive therapy (PCT) on criticaly ill patients in intensive care unit. Hiroshima Journal of Medical Sciences. 2018; 67(1):63-9. [Link]
- Cairns PL, Buck HG, Kip KE, Rodriguez CS, Liang Z, Munro CL. Stress management intervention to prevent post-intensive care syndrome-family in patients' spouses. American Journal of Critical Care. 2019; 28(6):471-6. [DOI:10.4037/ajcc2019668] [PMID]
- Halm MA. Intensive Care Unit Diaries, Part 2: Impact of diaries and follow-up consultation on post-intensive care syndrome. American Journal of Critical Care. 2019; 28(6):488-92. [DOI:10.4037/ajcc2019839] [PMID]
- Taito S, Yamauchi K, Tsujimoto Y, Banno M, Tsujimoto H, Kataoka Y. Does enhanced physical rehabilitation following intensive care unit discharge improve outcomes in patients who received mechanical ventilation? A systematic review and meta-analysis. BMJ Open. 2019; 9(6):e026075. [DOI:10.1136/bmjopen-2018-026075] [PMID]
- Chanpura T, Aparanji K, Shetty R, Gandam S, Sapra A, Siddarth S, et al. Impact of post icu care syndrome (PICS) education session on the knowledge and awareness of family/caregiver of critically ill patient - intervention study. EC Emergency Medicine And Critical Care. 2020; 6(2020):92-7. [Link]
- Lee YM, Kim K, Lim C, Kim JS. Effects of the ABCDE bundle on the prevention of post-intensive care syndrome: A retrospective study. Journal of Advanced Nursing. 2020; 76(2):588-99. [DOI:10.1111/jan.14267] [PMID]
- Sayde GE, Stefanescu A, Conrad E, Nielsen N, Hammer R. Implementing an intensive care unit (ICU) diary program at a large academic medical center: Results from a randomized control trial evaluating psychological morbidity associated with critical illness. General Hospital Psychiatry. 2020; 66:96-102. [DOI:10.1016/j.genhosppsych.2020.06.017] [PMID]
- Zante B, Camenisch SA, Schefold JC. Interventions in post-intensive care syndrome-family: A systematic literature review. Critical Care Medicine. 2020; 48(9):e835-40. [DOI:10.1097/CCM.0000000000004450] [PMID]
- Harrold ME, Salisbury LG, Webb SA, Allison GT; Australia and Scotland ICU Physiotherapy Collaboration. Early mobilisation in intensive care units in Australia and Scotland: A prospective, observational cohort study examining mobilisation practises and barriers. Critical Care. 2015; 19(1):336. [DOI:10.1186/s13054-015-1033-3] [PMID]
- Hopkins RO, Choong K, Zebuhr CA, Kudchadkar SR. Transforming PICU culture to facilitate early rehabilitation. Journal of Pediatric Intensive Care. 2015; 04(04):204-11. [DOI:10.1055/s-0035-1563547] [PMID]
- Rai S, Anthony L, Needham DM, Georgousopoulou EN, Sudheer B, Brown R, et al. Barriers to rehabilitation after critical illness: A survey of multidisciplinary healthcare professionals caring for ICU survivors in an acute care hospital. Australian Critical Care. 2020; 33(3):264-71. [DOI:10.1016/j.aucc.2019.05.006] [PMID]
- Dubb R, Nydahl P, Hermes C, Schwabbauer N, Toonstra A, Parker AM, et al. Barriers and strategies for early mobilization of patients in intensive care units. Annals of The American Thoracic Society. 2016; 13(5).724-30. [DOI:10.1513/AnnalsATS.201509-586CME] [PMID]
Article type: Reviews |
Subject:
Rehabilitation Management
Received: 2023/07/6 | Accepted: 2024/01/20 | Published: 2025/06/1
Received: 2023/07/6 | Accepted: 2024/01/20 | Published: 2025/06/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
