
988368
Tue, Jul 28, 2026

Volume 23, Issue 1 (March 2025)
Iranian Rehabilitation Journal 2025, 23(1): 13-20 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Talebi H, Hosseini Dastgerdi Z, Yaghini O, Faghihzadeh S, Narimani M H. The Prevalence of Auditory Processing Disorders in Persian-speaking Children. Iranian Rehabilitation Journal 2025; 23 (1) :13-20
URL: http://irj.uswr.ac.ir/article-1-2232-en.html
URL: http://irj.uswr.ac.ir/article-1-2232-en.html
Hossein Talebi1 

 , Zahra Hosseini Dastgerdi *1 , Omid Yaghini2 , Soghrat Faghihzadeh3 , Mohammad Hossein Narimani1
, Zahra Hosseini Dastgerdi *1 , Omid Yaghini2 , Soghrat Faghihzadeh3 , Mohammad Hossein Narimani1
, Zahra Hosseini Dastgerdi *1 , Omid Yaghini2 , Soghrat Faghihzadeh3 , Mohammad Hossein Narimani1
1- Department of Audiology, School of Rehabilitation Sciences, Isfahan University of Medical Sciences, Isfahan, Iran.
2- Child Growth and Development Research Center, Research Institute for Primordial Prevention of Non-Communicable Disease, Isfahan University of Medical Sciences, Isfahan, Iran.
3- Department of Biostatistics, School of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran.
2- Child Growth and Development Research Center, Research Institute for Primordial Prevention of Non-Communicable Disease, Isfahan University of Medical Sciences, Isfahan, Iran.
3- Department of Biostatistics, School of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran.
Full-Text [PDF 463 kb]
(822 Downloads)
| Abstract (HTML) (3318 Views)
Full-Text: (606 Views)
Introduction
Auditory processing disorder (APD) impacts the brain’s capacity to analyze and make sense of auditory information [1]. «The British Society of Audiology (BSA) described three groups of APD: Developmental type, in which neural developmental delay can occur in infancy and is the most common type; acquired type, which is shown by the events after birth; and secondary type, which is evidenced by hearing loss» [2]. APD can cause difficulties in various processing aspects, affecting communication and learning abilities [3]. Individuals with APD can experience various challenges even though they have normal hearing and intelligence. The most common complaints are difficulty in speech perception in noisy and reverberant situations, inability to follow oral commands, attention deficits, and difficulties with oral and written language [4]. Although no standardized protocol exists for diagnosing APD, various studies have reported different prevalence rates in children. According to Chermak and Musiek, approximately two to three percent of children may exhibit this disorder. Additionally, research suggests that the prevalence of APD in boys can be up to twice as high as in girls [5]. According to a study by Hind, APDs among children and adolescents may range from 0.5% to 1% of the entire population [5]. Additionally, some studies have shown that the prevalence of APD can be as high as 7% [6]. Several researchers believe that the APD rate can increase to 20% when accurate and comprehensive diagnostic tests are used [7]. This rate can increase to as high as 70% in adults aged >70 years [8]. It has been indicated that children with APD can show co-occurring impairments with a prevalence rate of 7-9% [9] and attention problems (9%) [10]. Additionally, 2-5% of children with APD may also have dyslexia or specific language impairment [11].
In real-world and demanding environments, individuals with APD often face significant challenges when listening to complex stimuli, such as speech. This includes noisy situations and locations with multiple speakers [8, 12]. These conditions can be particularly detrimental for school-aged children in the classroom, leading to various problems, including difficulties with reading and language, educational setbacks and emotional and social issues [8, 12, 13].
Therefore, early detection and management of auditory impairments are essential to reduce their adverse effects on the maturation of the CNS [12]. Auditory processing difficulties can negatively impact children’s communication, educational achievement, and social interactions. Given the prevalence of this disorder among young people, screening programs, evaluation, rehabilitation, and management of APD in school-aged children are regarded as a priority in many hearing-related research initiatives [14, 15].
In Iran, studies investigating the prevalence of APD are limited and often use smaller sample sizes than the present study. Additionally, these studies primarily relied on tools, such as questionnaires. For instance, a study conducted by Jarollahi et al. involved 536 students and utilized an APD questionnaire (APDQ) [14]. Ahmadi et al. conducted their study on 360 cases using the APDQ questionnaire [16] and Moloudi et al. surveyed 396 cases using the APDQ questionnaire, speech in noise and dichotic digit test (DDT) [17]. This study was conducted to conduct a comprehensive survey of APD and estimate its prevalence among school-aged children in Isfahan City, Iran.
Materials and Methods
An analytical-descriptive study was conducted on primary school students aged 8-12 in Isfahan City between 2020 and 2022. This study utilized a cross-sectional design with a stratified sampling method based on sex and educational level (age). To ensure a representative sample, each school was randomly chosen as a cluster according to its geographical location on a map of Isfahan City. From each school, a single desired class was selected using a simple random selection method and within each class, students were chosen randomly. A total of 637 boys (325) and girls (348) from schools in areas 5 and 6 (south of Isfahan City), 12 and 14 (north of Isfahan City) and 13 (west of Isfahan City) were examined based on the sample volume formula ni=(Ni/N)xn, considering the restrictions imposed by the coronavirus pandemic.
The inclusion criteria included age 8 to 12 years [18], hearing thresholds in 250 to 8000 Hz frequency range were 20 dB HL or lower in both ears [18], normal otoscopy, right-handedness (using the Edinburgh questionnaire) [19], the standard intelligence quotient (IQ) score is equal to or better than 85 in the revised Persian version of the Wechsler IQ test for children, no background of head injury, epilepsy and convulsions and use of antiepileptic medication, no history of behavioral disorders according to the opinion of relevant experts, not suffering from attention deficit hyperactivity disorder and autism according to the opinion of teachers and parents, monolingualism (Persian speaking with monolingual Persian speaking parents), lack of professional music experience. The exclusion criteria included reluctance to continue cooperation.
Procedure
Students were randomly selected at each age level by gender after preparing a geography map of schools and selecting schools and classes. Written consent from the parents and informed consent from the students were obtained before inclusion in the study. A history-taking form was completed for all students through interviews with parents and teachers and examination of the child’s medical records at school. The Edinburgh questionnaire was used to assess right-handedness. The Wechsler IQ test results were recorded in a school file for all students. In cases in which this information was incomplete, the student was referred to a psychologist.
Auditory threshold and auditory processing evaluations were conducted in a room with lower than 30 dBA background noise in schools between 8 AM and 12 AM. Otoscopic examination (with a Heine mini 3000 otoscope, Germany) and pure tone audiometric test at frequencies of 250 to 8000 Hz (with audiometer SA78B, Pejvak Ava, Iran) were performed to check the hearing thresholds of the students. The primary assessment stage included children whose preliminary assessment results were consistent. In this study, to identify students suspected of APD, the multiple auditory processing assessment (MAPA) test battery consisting of DDT, pitch pattern sequence test (PPST) and selective auditory attention test (mSAAT) was used. MAPA test battery reveals a sensitivity of 90% and a specificity of 100% in diagnosing APD. The criteria for selecting APD students involve obtaining a score lower than 2SD from the standard value in at least two tests [20]. The normative data was obtained from the Rezapour [21] and Lotfi study [22]. The stimuli were introduced via a laptop and Sennheiser HD202 headphones.
DDT
The DDT involves presenting two number pairs (numbers 1 to 10 ) simultaneously to each ear of the participants, who are then instructed to repeat freely recall all four digits or in any sequence. A total of 40 patterns are presented. Rezapour et al., in a study, presented the normal range of data for the DDT among Iranian children [21].
PPST
Each item in the PPST includes three tonal stimuli with two different pitches: one low-frequency tone (880 Hz) and one high-frequency tone (1122 Hz). Thirty patterns are delivered to each ear. The stimuli were presented at a 55 dB sensation level (relative to the 1000 hertz threshold). The Lotfi study [22, 23] provides normative data for the PPS test in Iranian students.
Persian monaural selective auditory attention test (mSAAT)
Persian mSAAT consists of 25 monosyllabic words integrated into a narrative context. The same speaker presents the score and competing stimuli, and the signal-to-noise ratio is set at zero decibel. Normative data for Iranian children can be found in studies by Aarabi et al. and Ebadi et al. [24-26].
Descriptive statistics (frequency, Mean±SD, an independent t-test (to assess the impact of demographic factors, such as gender, on the test scores), and analysis of variance (ANOVA) (to evaluate the difference between age groups) were utilized for statistical data analysis.
Results
A total of 673 students participated in the study and information from 605 participants was provided according to the inclusion criteria. Fifteen schools in 5 regions were investigated. The number of female students was 323(53.4%), and the number of boys was 282(46.6%); 94 students (15.53%) in the second grade, 120(19.83%) in the third grade, 138(22.8%) in the fourth grade, 142(23.47%) in the fifth and 11(18.34%) in the sixth grade. The age range was 10.18±1.37 years for girls and 10±1.29 for boys. A total of 69.42% of the samples were from the west (area 13) and north (areas 12 and 14) of Isfahan City. Tables 1 and 2 present the mean scores of tests and the number/percentage of students suspected of APD by gender, school grade and age.
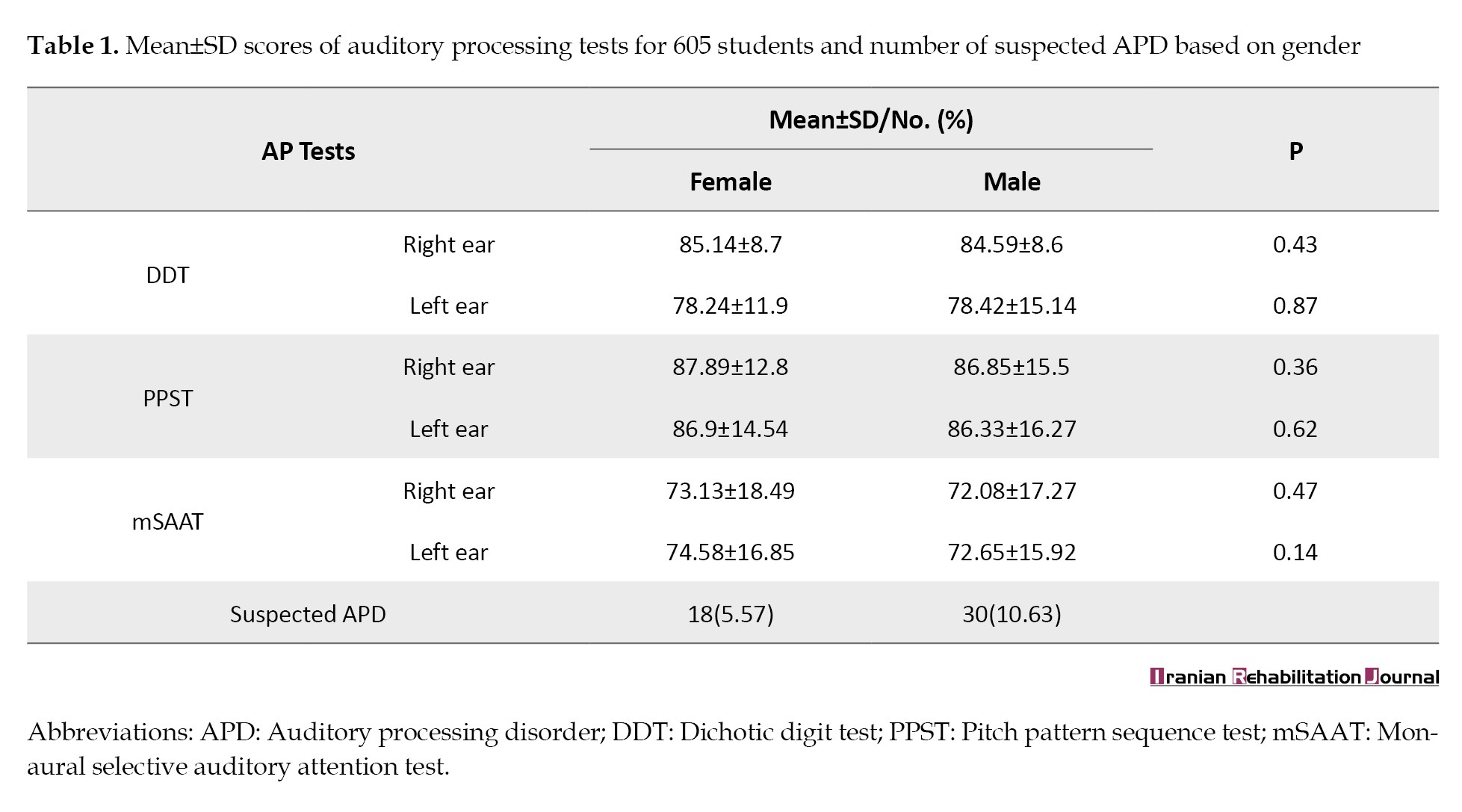
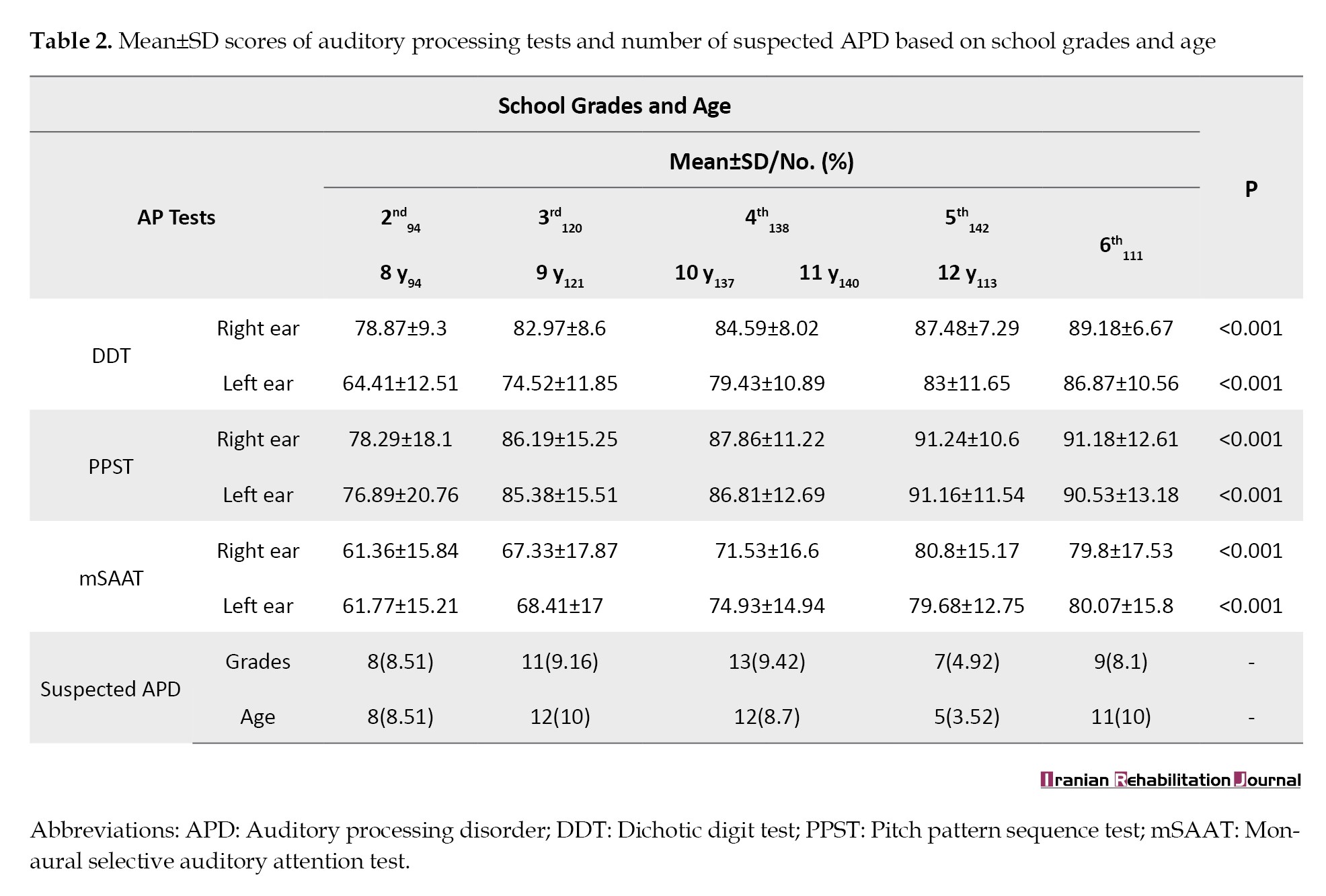
Based on the analysis, the two groups of boys and girls were not different in their auditory processing test scores (P>0.05) (Table 1). It was found that the difference in the performance of students in different educational levels is statistically significant. In other words, with increasing age and educational level, the scores of the tests revealed an improvement (P<0.05) (Table 2). A total of 48 students, accounting for 7.93%, experienced difficulties in at least two of the DDT, PPST and mSAAT tests. Most students (35 of 48) exhibited abnormal results in the DDT and PPST tests. A total of 13 out of 48 students had difficulty in all three tests. The ratio of male to female students suspected to have APD was 1.9.
Discussion
This study was conducted to examine APD among 8-12-year-old students in Isfahan City. This age range was chosen for screening due to the lack of a comprehensive assessment tool to evaluate auditory processing and the potential cognitive limitations and variability in responses among children younger than 7. In addition, access to school-aged children is more feasible.
The study found a prevalence rate of 7.93% of APD among students in this age group. Of the 605 students screened, 48 scored below (2 standard deviations) the expected value in at least two tests.
It is also important to note that a slight sex difference was observed (male/female=1.9). The results indicated that the proportion of boys suspected of having APD was nearly twice that of girls, consistent with previous global reports [7]. The exact global prevalence of APD is not well established, but estimates vary widely, from 2% to 20% [14]. In the United States and the United Kingdom, it is estimated to be 2-7% [27]. These numbers indicate that APD is a reasonably common issue, highlighting the importance of early detection and intervention to provide appropriate support for those affected. Based on some research projects, the rate of this disorder in school-aged children is around 7% [17]. In 1990, Musiek estimated that 3%-7% of elementary school students experienced learning difficulty, and a significant portion of this group also had APD [28]. Geffner’s research using behavioral tests found a prevalence of 12% for APD, while Tillery reported an even higher prevalence of 20% using the behavioral manifested questionnaire [29]. Brewer et al. suggested that the APD prevalence may increase to 10% when comorbidities are considered [30]. Ebadi et al. showed a rate of 5% for APD in Arak City, Iran, utilizing a Persian version of the MAPA [26]. Moloudi et al. conducted a study in Oshnavieh City, Iran, involving 396 elementary students. The prevalence of suspected APD was 9.8%, according to data obtained from the APDQ, DDT, and speech-in-noise tests [17]. Jarollahi et al. used the APDQ to investigate the prevalence of APD among elementary school students in Tehran City, Iran. Their results revealed a prevalence rate of 4.6%, along with a boy-to-girl proportion 2.6 [14] .
Undoubtedly, the lack of standardized diagnostic criteria for APD and the use of various diagnostic tests can result in differing prevalence rates across studies. Additionally, some experts have raised concerns about the validity and reliability of specific tests used to diagnose APD, which can further complicate the interpretation of prevalence rates. Therefore, it is crucial to consider the specific diagnostic criteria and methods employed in each study when comparing prevalence rates.
Moreover, it is crucial to consider the possible effect of cultural and environmental factors on the prevalence of APD in different populations. According to some studies, using behavioral tests instead of questionnaires can provide more accurate information and reduce errors in identifying APD [14]. However, the accuracy of diagnostic tests can vary based on factors, such as the specific test used, characteristics of the population being tested and expertise of the examiner administering the test. In contrast, more accurate diagnostic tests may lead to an increased prevalence of APD [7]. It is essential to ensure the validity and reliability of diagnostic criteria to prevent overdiagnosis or misdiagnosis. Therefore, appropriate diagnostic tests should be used carefully to accurately assess APD’s prevalence alongside clinical observations and medical history.
The current study employed three behavioral tests from MAPA test batteries: DDT, PPST and mSAAT. These tests demonstrated a strong ability to identify APD in children with 90% sensitivity and 100% specificity. These tests are efficient in accurately detecting APD in children [24, 27]. Screening studies for APD are essential to provide audiologists with the information needed to establish criteria for central auditory processing tests. Additionally, these studies offer valuable insights for policymakers, enabling them to implement effective and timely measures in the healthcare system. In audiology, diagnosing and treating APD has become a priority research area for children. Consequently, identifying individuals at risk of APD through screening is extremely valuable. This approach ensures that children receive early intervention and appropriate treatment, which can significantly enhance their communication skills, language development, and academic performance. Specifically, the current study found that performance in three auditory skills, dichotic processing, temporal processing, and speech understanding in noise, improved with age among children aged 8-12 years. No difference was observed in auditory processing scores between girls and boys, suggesting that the way sounds are processed may not be influenced by sex. It is also crucial to consider the influence of age when examining auditory processing because it can impact the results.
In 2017, Mattsson’s study of children from Norway aged 7-12 years revealed no substantial discrepancies in results between boys and girls. However, it observed an age-related effect in most assessments, except for the gaps in noise and binaural masking level differences tests. Specifically, performance in tests assessing dichotic digits, pitch patterns, and speech in noise improved with age. As a result, the study found that performance improved and the variability of scores decreased with age, indicating the growth and development of central auditory processing pathway. Additionally, this project showed that the maturation period for specific processes, such as frequency pattern recognition, may extend beyond 12 [31].
Conclusion
This study estimated the APD prevalence among 8-12-year-old students in Isfahan City at 7.93%. Given the negative impact of APD on children’s learning, education and communication skills, which ultimately affects their quality of life and can lead to broader issues for families and communities alike, it is necessary to implement APD screening programs in education and healthcare systems. This will facilitate more accurate diagnosis of APD and related disorders, as well as provide treatment solutions to those affected.
Limitations
One of the primary limitations of this research project was the insufficient cooperation of students. This resulted in a group of participants not cooperating until the end of the tests, resulting in their exclusion from the study. Furthermore, we faced difficulties and restrictions when entering school and obtaining permission to implement the project, which prolonged its implementation. Due to these limitations, we cannot consider the sample size of boys to be twice that of girls. In future studies, the sample size of boys should be double that of girls according to the reported prevalence.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences, Isfahan, Iran (Code: IR.MUI.MED.REC.1400.462).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Zahra Hosseini Dastgerdi; Methodology: Hossein Talebi, Soghrat Faghihzadeh and Zahra Hosseini Dastgerdi; Funding acquisition: Hossein Talebi; Supervision and writing the original draft: Hossein Talebi and Zahra Hosseini Dastgerdi; Investigation, resources, review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all participants, parents and school officials for their contributions.
References
Auditory processing disorder (APD) impacts the brain’s capacity to analyze and make sense of auditory information [1]. «The British Society of Audiology (BSA) described three groups of APD: Developmental type, in which neural developmental delay can occur in infancy and is the most common type; acquired type, which is shown by the events after birth; and secondary type, which is evidenced by hearing loss» [2]. APD can cause difficulties in various processing aspects, affecting communication and learning abilities [3]. Individuals with APD can experience various challenges even though they have normal hearing and intelligence. The most common complaints are difficulty in speech perception in noisy and reverberant situations, inability to follow oral commands, attention deficits, and difficulties with oral and written language [4]. Although no standardized protocol exists for diagnosing APD, various studies have reported different prevalence rates in children. According to Chermak and Musiek, approximately two to three percent of children may exhibit this disorder. Additionally, research suggests that the prevalence of APD in boys can be up to twice as high as in girls [5]. According to a study by Hind, APDs among children and adolescents may range from 0.5% to 1% of the entire population [5]. Additionally, some studies have shown that the prevalence of APD can be as high as 7% [6]. Several researchers believe that the APD rate can increase to 20% when accurate and comprehensive diagnostic tests are used [7]. This rate can increase to as high as 70% in adults aged >70 years [8]. It has been indicated that children with APD can show co-occurring impairments with a prevalence rate of 7-9% [9] and attention problems (9%) [10]. Additionally, 2-5% of children with APD may also have dyslexia or specific language impairment [11].
In real-world and demanding environments, individuals with APD often face significant challenges when listening to complex stimuli, such as speech. This includes noisy situations and locations with multiple speakers [8, 12]. These conditions can be particularly detrimental for school-aged children in the classroom, leading to various problems, including difficulties with reading and language, educational setbacks and emotional and social issues [8, 12, 13].
Therefore, early detection and management of auditory impairments are essential to reduce their adverse effects on the maturation of the CNS [12]. Auditory processing difficulties can negatively impact children’s communication, educational achievement, and social interactions. Given the prevalence of this disorder among young people, screening programs, evaluation, rehabilitation, and management of APD in school-aged children are regarded as a priority in many hearing-related research initiatives [14, 15].
In Iran, studies investigating the prevalence of APD are limited and often use smaller sample sizes than the present study. Additionally, these studies primarily relied on tools, such as questionnaires. For instance, a study conducted by Jarollahi et al. involved 536 students and utilized an APD questionnaire (APDQ) [14]. Ahmadi et al. conducted their study on 360 cases using the APDQ questionnaire [16] and Moloudi et al. surveyed 396 cases using the APDQ questionnaire, speech in noise and dichotic digit test (DDT) [17]. This study was conducted to conduct a comprehensive survey of APD and estimate its prevalence among school-aged children in Isfahan City, Iran.
Materials and Methods
An analytical-descriptive study was conducted on primary school students aged 8-12 in Isfahan City between 2020 and 2022. This study utilized a cross-sectional design with a stratified sampling method based on sex and educational level (age). To ensure a representative sample, each school was randomly chosen as a cluster according to its geographical location on a map of Isfahan City. From each school, a single desired class was selected using a simple random selection method and within each class, students were chosen randomly. A total of 637 boys (325) and girls (348) from schools in areas 5 and 6 (south of Isfahan City), 12 and 14 (north of Isfahan City) and 13 (west of Isfahan City) were examined based on the sample volume formula ni=(Ni/N)xn, considering the restrictions imposed by the coronavirus pandemic.
The inclusion criteria included age 8 to 12 years [18], hearing thresholds in 250 to 8000 Hz frequency range were 20 dB HL or lower in both ears [18], normal otoscopy, right-handedness (using the Edinburgh questionnaire) [19], the standard intelligence quotient (IQ) score is equal to or better than 85 in the revised Persian version of the Wechsler IQ test for children, no background of head injury, epilepsy and convulsions and use of antiepileptic medication, no history of behavioral disorders according to the opinion of relevant experts, not suffering from attention deficit hyperactivity disorder and autism according to the opinion of teachers and parents, monolingualism (Persian speaking with monolingual Persian speaking parents), lack of professional music experience. The exclusion criteria included reluctance to continue cooperation.
Procedure
Students were randomly selected at each age level by gender after preparing a geography map of schools and selecting schools and classes. Written consent from the parents and informed consent from the students were obtained before inclusion in the study. A history-taking form was completed for all students through interviews with parents and teachers and examination of the child’s medical records at school. The Edinburgh questionnaire was used to assess right-handedness. The Wechsler IQ test results were recorded in a school file for all students. In cases in which this information was incomplete, the student was referred to a psychologist.
Auditory threshold and auditory processing evaluations were conducted in a room with lower than 30 dBA background noise in schools between 8 AM and 12 AM. Otoscopic examination (with a Heine mini 3000 otoscope, Germany) and pure tone audiometric test at frequencies of 250 to 8000 Hz (with audiometer SA78B, Pejvak Ava, Iran) were performed to check the hearing thresholds of the students. The primary assessment stage included children whose preliminary assessment results were consistent. In this study, to identify students suspected of APD, the multiple auditory processing assessment (MAPA) test battery consisting of DDT, pitch pattern sequence test (PPST) and selective auditory attention test (mSAAT) was used. MAPA test battery reveals a sensitivity of 90% and a specificity of 100% in diagnosing APD. The criteria for selecting APD students involve obtaining a score lower than 2SD from the standard value in at least two tests [20]. The normative data was obtained from the Rezapour [21] and Lotfi study [22]. The stimuli were introduced via a laptop and Sennheiser HD202 headphones.
DDT
The DDT involves presenting two number pairs (numbers 1 to 10 ) simultaneously to each ear of the participants, who are then instructed to repeat freely recall all four digits or in any sequence. A total of 40 patterns are presented. Rezapour et al., in a study, presented the normal range of data for the DDT among Iranian children [21].
PPST
Each item in the PPST includes three tonal stimuli with two different pitches: one low-frequency tone (880 Hz) and one high-frequency tone (1122 Hz). Thirty patterns are delivered to each ear. The stimuli were presented at a 55 dB sensation level (relative to the 1000 hertz threshold). The Lotfi study [22, 23] provides normative data for the PPS test in Iranian students.
Persian monaural selective auditory attention test (mSAAT)
Persian mSAAT consists of 25 monosyllabic words integrated into a narrative context. The same speaker presents the score and competing stimuli, and the signal-to-noise ratio is set at zero decibel. Normative data for Iranian children can be found in studies by Aarabi et al. and Ebadi et al. [24-26].
Descriptive statistics (frequency, Mean±SD, an independent t-test (to assess the impact of demographic factors, such as gender, on the test scores), and analysis of variance (ANOVA) (to evaluate the difference between age groups) were utilized for statistical data analysis.
Results
A total of 673 students participated in the study and information from 605 participants was provided according to the inclusion criteria. Fifteen schools in 5 regions were investigated. The number of female students was 323(53.4%), and the number of boys was 282(46.6%); 94 students (15.53%) in the second grade, 120(19.83%) in the third grade, 138(22.8%) in the fourth grade, 142(23.47%) in the fifth and 11(18.34%) in the sixth grade. The age range was 10.18±1.37 years for girls and 10±1.29 for boys. A total of 69.42% of the samples were from the west (area 13) and north (areas 12 and 14) of Isfahan City. Tables 1 and 2 present the mean scores of tests and the number/percentage of students suspected of APD by gender, school grade and age.
Based on the analysis, the two groups of boys and girls were not different in their auditory processing test scores (P>0.05) (Table 1). It was found that the difference in the performance of students in different educational levels is statistically significant. In other words, with increasing age and educational level, the scores of the tests revealed an improvement (P<0.05) (Table 2). A total of 48 students, accounting for 7.93%, experienced difficulties in at least two of the DDT, PPST and mSAAT tests. Most students (35 of 48) exhibited abnormal results in the DDT and PPST tests. A total of 13 out of 48 students had difficulty in all three tests. The ratio of male to female students suspected to have APD was 1.9.
Discussion
This study was conducted to examine APD among 8-12-year-old students in Isfahan City. This age range was chosen for screening due to the lack of a comprehensive assessment tool to evaluate auditory processing and the potential cognitive limitations and variability in responses among children younger than 7. In addition, access to school-aged children is more feasible.
The study found a prevalence rate of 7.93% of APD among students in this age group. Of the 605 students screened, 48 scored below (2 standard deviations) the expected value in at least two tests.
It is also important to note that a slight sex difference was observed (male/female=1.9). The results indicated that the proportion of boys suspected of having APD was nearly twice that of girls, consistent with previous global reports [7]. The exact global prevalence of APD is not well established, but estimates vary widely, from 2% to 20% [14]. In the United States and the United Kingdom, it is estimated to be 2-7% [27]. These numbers indicate that APD is a reasonably common issue, highlighting the importance of early detection and intervention to provide appropriate support for those affected. Based on some research projects, the rate of this disorder in school-aged children is around 7% [17]. In 1990, Musiek estimated that 3%-7% of elementary school students experienced learning difficulty, and a significant portion of this group also had APD [28]. Geffner’s research using behavioral tests found a prevalence of 12% for APD, while Tillery reported an even higher prevalence of 20% using the behavioral manifested questionnaire [29]. Brewer et al. suggested that the APD prevalence may increase to 10% when comorbidities are considered [30]. Ebadi et al. showed a rate of 5% for APD in Arak City, Iran, utilizing a Persian version of the MAPA [26]. Moloudi et al. conducted a study in Oshnavieh City, Iran, involving 396 elementary students. The prevalence of suspected APD was 9.8%, according to data obtained from the APDQ, DDT, and speech-in-noise tests [17]. Jarollahi et al. used the APDQ to investigate the prevalence of APD among elementary school students in Tehran City, Iran. Their results revealed a prevalence rate of 4.6%, along with a boy-to-girl proportion 2.6 [14] .
Undoubtedly, the lack of standardized diagnostic criteria for APD and the use of various diagnostic tests can result in differing prevalence rates across studies. Additionally, some experts have raised concerns about the validity and reliability of specific tests used to diagnose APD, which can further complicate the interpretation of prevalence rates. Therefore, it is crucial to consider the specific diagnostic criteria and methods employed in each study when comparing prevalence rates.
Moreover, it is crucial to consider the possible effect of cultural and environmental factors on the prevalence of APD in different populations. According to some studies, using behavioral tests instead of questionnaires can provide more accurate information and reduce errors in identifying APD [14]. However, the accuracy of diagnostic tests can vary based on factors, such as the specific test used, characteristics of the population being tested and expertise of the examiner administering the test. In contrast, more accurate diagnostic tests may lead to an increased prevalence of APD [7]. It is essential to ensure the validity and reliability of diagnostic criteria to prevent overdiagnosis or misdiagnosis. Therefore, appropriate diagnostic tests should be used carefully to accurately assess APD’s prevalence alongside clinical observations and medical history.
The current study employed three behavioral tests from MAPA test batteries: DDT, PPST and mSAAT. These tests demonstrated a strong ability to identify APD in children with 90% sensitivity and 100% specificity. These tests are efficient in accurately detecting APD in children [24, 27]. Screening studies for APD are essential to provide audiologists with the information needed to establish criteria for central auditory processing tests. Additionally, these studies offer valuable insights for policymakers, enabling them to implement effective and timely measures in the healthcare system. In audiology, diagnosing and treating APD has become a priority research area for children. Consequently, identifying individuals at risk of APD through screening is extremely valuable. This approach ensures that children receive early intervention and appropriate treatment, which can significantly enhance their communication skills, language development, and academic performance. Specifically, the current study found that performance in three auditory skills, dichotic processing, temporal processing, and speech understanding in noise, improved with age among children aged 8-12 years. No difference was observed in auditory processing scores between girls and boys, suggesting that the way sounds are processed may not be influenced by sex. It is also crucial to consider the influence of age when examining auditory processing because it can impact the results.
In 2017, Mattsson’s study of children from Norway aged 7-12 years revealed no substantial discrepancies in results between boys and girls. However, it observed an age-related effect in most assessments, except for the gaps in noise and binaural masking level differences tests. Specifically, performance in tests assessing dichotic digits, pitch patterns, and speech in noise improved with age. As a result, the study found that performance improved and the variability of scores decreased with age, indicating the growth and development of central auditory processing pathway. Additionally, this project showed that the maturation period for specific processes, such as frequency pattern recognition, may extend beyond 12 [31].
Conclusion
This study estimated the APD prevalence among 8-12-year-old students in Isfahan City at 7.93%. Given the negative impact of APD on children’s learning, education and communication skills, which ultimately affects their quality of life and can lead to broader issues for families and communities alike, it is necessary to implement APD screening programs in education and healthcare systems. This will facilitate more accurate diagnosis of APD and related disorders, as well as provide treatment solutions to those affected.
Limitations
One of the primary limitations of this research project was the insufficient cooperation of students. This resulted in a group of participants not cooperating until the end of the tests, resulting in their exclusion from the study. Furthermore, we faced difficulties and restrictions when entering school and obtaining permission to implement the project, which prolonged its implementation. Due to these limitations, we cannot consider the sample size of boys to be twice that of girls. In future studies, the sample size of boys should be double that of girls according to the reported prevalence.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences, Isfahan, Iran (Code: IR.MUI.MED.REC.1400.462).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Zahra Hosseini Dastgerdi; Methodology: Hossein Talebi, Soghrat Faghihzadeh and Zahra Hosseini Dastgerdi; Funding acquisition: Hossein Talebi; Supervision and writing the original draft: Hossein Talebi and Zahra Hosseini Dastgerdi; Investigation, resources, review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all participants, parents and school officials for their contributions.
References
- Iliadou V, Bamiou DE. Psychometric evaluation of children with auditory processing disorder (APD): Comparison with normal-hearing and clinical non-APD groups. Journal of Speech, language, and hearing research. 2012; 55(3):791-9. [DOI:10.1044/1092-4388(2011/11-0035)] [PMID]
- Br Soc Audiol. Practice guidance: An overview of current management of auditory processing disorder (APD). Seafield: British Society of Audiology; 2011. [Link]
- Am Speech-Language-Hearing Assoc. (Central) auditory processing disorders—the role of the audiologist. Maryland: American Speech-Language-Hearing Association; 2005. [Link]
- Moore DR. Auditory processing disorders: Acquisition and treatment. Journal of Communication Disorders. 2007; 40(4):295-304. [DOI:10.1016/j.jcomdis.2007.03.005] [PMID]
- Hind SE, Haines-Bazrafshan R, Benton CL, Brassington W, Towle B, Moore DR. Prevalence of clinical referrals having hearing thresholds within normal limits. International journal of audiology. 2011; 50(10):708-16. [DOI:10.3109/14992027.2011.582049] [PMID]
- Skarzynski PH, Wlodarczyk AW, Kochanek K, Pilka A, Jedrzejczak WW, Olszewski L, et al. Central auditory processing disorder (CAPD) tests in a school-age hearing screening programme - analysis of 76, 429 children. Annals of Agricultural and Environmental Medicine. 2015; 22(1):90-5. [DOI:10.5604/12321966.1141375] [PMID]
- Chermak GD, Musiek FE. Central auditory processing disorders: new perspective. Norwich: Singular Publishing Group; 1997. [Link]
- Geffner D, Ross-Swain D. Central auditory processing disorders: Assessment, management, and treatment. San Diego: plural publishing incorporated; 2019. [Link]
- Jones CR, Happé F, Baird G, Simonoff E, Marsden AJ, Tregay J, et al. Auditory discrimination and auditory sensory behaviours in autism spectrum disorders. Neuropsychologia. 2009; 47(13):2850-8. [DOI:10.1016/j.neuropsychologia.2009.06.015] [PMID]
- Sharma M, Purdy SC, Kelly AS. Comorbidity of auditory processing, language, and reading disorders. Journal of speech, Language, and Hearing Research. 2009; 52(3):706-22. [DOI:10.1044/1092-4388(2008/07-0226)] [PMID]
- Ferguson MA, Hall RL, Riley A, Moore DR. Communication, listening, cognitive and speech perception skills in children with auditory processing disorder (APD) or Specific Language Impairment (SLI). Journal of speech, language, and hearing research. 2011; 54(1):211-27.[DOI:10.1044/1092-4388(2010/09-0167)] [PMID]
- Gohari N, Dastgerdi ZH, Rouhbakhsh N, Afshar S, Mobini R. Training programs for improving speech perception in noise: A review. Journal of audiology & otology. 2023; 27(1):1-9. [DOI:10.7874/jao.2022.00283] [PMID]
- Zarei M, Hosseini Dastgerdi Z, Momeni A, Nouri NS. Assessment of auditory processing in children with non-syndromic cleft lip and/or palate. Hearing, Balance and Communication. 2021; 20(1):32-8. [DOI:10.1080/21695717.2021.1933317]
- Jarollahi F, Pourbakht A, Jalaie S OM. Screening of auditory processing disorders in school-aged children in Tehran, Iran using the Auditory Processing Domain Questionnaire. Auditory and Vestibular Research. 2022; 31(1):17-22. [DOI:10.18502/avr.v31i1.8130]
- Cacace AT, McFarland DJ. Central auditory processing disorder in school-aged children: a critical review. Journal of Speech, language, and hearing research. 1998; 41(2):355-73. [DOI:10.1044/jslhr.4102.355] [PMID]
- Ahmadi Z, Jarollahi F, Ahadi M, Hosseini AF. Normaliza-tion and validation of auditory processing domain question-naire in normal 8-12 year-old children. Auditory and Vestibular Research Journal. 2017; 26(2):98-103. [Link]
- Moloudi A, Rouzbahani M, Rahbar N, Saneie H. Estimation of the referral rate of suspected cases of central auditory processing disorders in children aged 8-12 years old in Oshnavieh, Western Iran, based on auditory processing domain questionnaire and speech in noise and dichotic digit tests. Auditory and Vestibular Research. 2018; 27(3):164-70. [DOI:10.18502/avr.v27i3.59]
- Musiek FE, Shinn J, Chermak GD, Bamiou DE. Perspectives on the Pure-Tone Audiogram. Journal of the American Academy of Audiology. 2017; 28(7):655-71. [DOI:10.3766/jaaa.16061] [PMID]
- Oldfield RC. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia. 1971; 9(1):97-113. [DOI:10.1016/0028-3932(71)90067-4] [PMID]
- American Academy of Audiology. Clinical practice guidelines: Diagnosis, treatment and management of children and adults with central auditory processing disorder. San Diego: American Academy of Audiology; 2010. [Link]
- Rezapour M, Zamiri Abdollahi F, Delphi M, Lotfi Y, Bakhshi E. Normalization and reliability evaluation of persian version of two-pair dichotic digits in 8 to 12-year-old children. Iranian Rehabilitation Journal. 2016; 14(2):115-20. [DOI:10.18869/nrip.irj.14.2.115]
- Lotfi Y, Moosavi A, Abdollahi FZ, Bakhshi E, Sadjedi H. Effects of an auditory lateralization training in children suspected to central auditory processing disorder. Journal of Audiology & Otology. 2016; 20(2):102-8. [DOI:10.7874/jao.2016.20.2.102] [PMID]
- Lotfi Y, Dastgerdi ZH, Farazi M, Moossavi A, Bakhshi E. Auditory temporal processing assessment in children with developmental stuttering. International Journal of Pediatric Otorhinolaryngology. 2020; 132:109935. [DOI:10.1016/j.ijporl.2020.109935] [PMID]
- Domitz DM, Schow RL. A new CAPD battery--multiple auditory processing assessment: factor analysis and comparisons with SCAN. American Journal of Audiology. 2000; 9(2):101-11. [DOI:10.1044/1059-0889(2000/012)] [PMID]
- Aarabi S, Jarollahi F, Jalaie S. Development and determination of the validity of Persian version of monaural selective auditory attention test in learning disabled children. Auditory and Vestibular Research. 2016; 25(1):49-54. [Link]
- Ebadi E, Jarollahi F, Tahaei AA, Ahadi M, Hosseini AF. Development and evaluation of the Persian version of the multiple auditory processing assessment. Auditory and Vestibular Research. 2016; 25(2):75-81. [Link]
- Musiek FE, Chermak GD. Handbook of central auditoryprocessing disorder, auditory neuroscience and diagnosis. San Diego: Plural Publishing; 2014. [Link]
- Musiek FE, Gollegly KM, Lamb LE, Lamb P. Selected issues in screening for central auditory processing dysfunction. Seminars in Hearing. 1990; 11(4):372-83. [DOI:10.1055/s-0028-1085516]
- Tillery KL. Central auditory processing evaluation: A test battery approach. In: Katz J, Chasin M, English K, Hood LJ, Tillery KL editors. Handbook of Clinical Audiology. Philadelphia: Lippincott Williams & Wilkins; 2015.
- Brewer CC, Zalewski CK, King KA, Zobay O, Riley A, Ferguson MA, et al. Heritability of non-speech auditory processing skills. European Journal of Human Genetics. 2016; 24(8):1137-44. [DOI:10.1038/ejhg.2015.277] [PMID]
- Mattsson TS, Follestad T, Andersson S, Lind O, Øygarden J, Nordgård S. Normative data for diagnosing auditory processing disorder in Norwegian children aged 7-12 years. International journal of audiology. 2018; 57(1):10-20. [DOI:10.1080/14992027.2017.1366670] [PMID]
Article type: Original Research Articles |
Subject:
Audiology
Received: 2024/03/31 | Accepted: 2024/07/20 | Published: 2025/03/1
Received: 2024/03/31 | Accepted: 2024/07/20 | Published: 2025/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
