
988368
Thu, Jul 30, 2026

Volume 23, Issue 1 (March 2025)
Iranian Rehabilitation Journal 2025, 23(1): 65-76 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Anwar Fadhel Z, Naji Al- Hamoodi A A. The Relationship Between Psychophysical Indicators and Hostile Behavior Among School-aged Children. Iranian Rehabilitation Journal 2025; 23 (1) :65-76
URL: http://irj.uswr.ac.ir/article-1-2319-en.html
URL: http://irj.uswr.ac.ir/article-1-2319-en.html



1- Psychiatric and Mental Health Nursing Branch, College of Nursing, University of Kufa, Kufa, Iraq.
Keywords: Psychophysical indicators, Psychological indicators, Physical indicators, Hostile behaviors, School-age children
Full-Text [PDF 529 kb]
(621 Downloads)
| Abstract (HTML) (3854 Views)
Full-Text: (444 Views)
Introduction
Psychophysical indicators are the most crucial criteria for detecting the health state of children, especially at the school-age stage [1]. Therefore, this stage is vital in a child’s life because it exposes him to various factors and affects his growth and development [2]. It is also essential in shaping a child’s personality traits and academic journey [3]. Psychophysical indicators encompass various aspects related to the health state of children, including the main psychological aspects, such as cognitive and learning features, language and understanding [4], attention, emotions [5], and social relationships [6]. The language domain is vital for evaluation because it is an essential indicator of the level of knowledge and cognitive skills [7]. The cognitive domain is crucial for children’s academic success, social interaction, and overall wellbeing [8]. Together, these domains reflect children’s psychological health and are associated with their thriving and success in school and life [9]. These indicators help determine whether a child is developing problematic or non-problematic and predict the children’s future psychological health [10]. The physical aspects included body mass index (BMI) percentile, heart rate, breathing, and movement indicators. The BMI percentile is crucial for children’s health [11]. Some studies showed that children who have abnormal weight may be more prone to hostile behavior, low self-esteem, and difficulties in relationships with others [12] [13]. Developing fine motor skills in childhood is crucial for overall development, impacting a child’s academic and practical abilities and social connections throughout life [14].
Hostile behavior can lead to health, psychological, and social impacts on the child, family, and peers, and hostile children are at risk of experiencing emotional distress, such as phobias, depression and panic attacks [15]. Thus distresses can harm themselves or others, and children need more health services and support than normal children in schools, homes, and communities [16, 17].
This study aims to assess hostile behavior and psychophysical indicators among school-age children and determine the relationship between psychophysical indicators and hostile behavior.
Materials and Methods
Study design
A cross-sectional study design was used to fit the study objectives. This design achieved its objectives by providing valuable insights into population traits and detecting correlations for further research.
Setting of study
This study was conducted in Al-Najaf Province, Iraq, and included primary governmental schools. Al-Najaf governorate is located in the middle of Iraq and is one of the crucial holy provinces in Iraq and the Islamic world. Al-Najaf governorate had six main sectors, and the researchers of one sector were randomly selected to conduct the study. This study was conducted from December 1, 2023, to the end of February 2024.
Al-Najaf primary schools had more than (571) governmental and private schools (17), but the study sample included only (21) girls’ and boys’ primary schools. These schools include only governmental schools located in the southern sector. By 2023, these primary schools accommodated more than 200 thousand children, but the number of new schools has increased. All children who participated in the study informed their parents about the study’s aims and the importance of their participation before meeting the child. Data were collected using a modified Arabic version of the hostile behavior and psychophysical indicators scale for school-aged children.
Sample size
The study sample was a cluster sample, including 384 children who studied in the southern sector of Al-Najaf primary schools and whose parents agreed to participate. The sample was selected using a simple sampling method (luck lottery) and all children in all governmental primary schools were allowed to participate in the study. This study included this category because this class is a transition stage in a child’s life between childhood and adolescence, which is crucial in developing physical and mental health, personal traits, behaviors and dealing with peers and educated teachers.
The sample size of the study was calculated 6 294 children according to the size of the population target (school-aged children) in governmental schools in the southern sector of Al-Najaf Province, therefore the sample size was equal to 384 children according to the calculated size tables [18]. The study depended on the objectives and criteria of the study sample to reduce the bias that could occur and give all school-age children an equal chance to exhibit in the study.
Study instruments
The study variables included the vital aspects of psychophysical indicators in this stage, including the severity of hostile behavior among children and demographic characteristics related to and affecting these variables, such as age, order among siblings, sex and stage study.
The study used the adopted tool to measure the study variables and included three main parts: demographic characteristics of children, such as age, order among siblings, sex, and stage study and the hostile behavior scale of the Arabic version of the manual of psychological and educational standards and tests, designed each scale of the Arabic environment. The hostile behavior scale was designed to detect the severity of hostile behavior in children or those suspected of having symptoms. The scale had three rated responses: Always to never (3-1). The explanation by cutting the points of the symptoms and severity of hostility can be assessed from normal to severe.
The second part related to the psychophysical indicators scale included the first two sub-parts related to the psychological indicators scale (33) with items, including five crucial aspects, such as cognitive problems (8 items), attention problems (6 items), language problems (10 items), social problems (5 items), emotional problems (4 items) and the second sub-part related to physical indicators, including BMI percentile (weight, height with birth date), heart rate, breath rate and movement aspect (10 items), which explained their score using the score and cut of points for each indicator with the final scale.
Validity and reliability of the instrument
The instrument’s validity was examined using content validity and about 13 experts in the psychology and psychiatric fields and modified with study variables. The reliability of hostile behavior (0.92) and psychophysical indicators (0.88) was obtained using Cronbach’s α compared to studies of Buss and Bint Ibrahim Al-Omar (0.78) [19, 20].
Data analysis
The study results were analyzed using SPSS software, version 24 and Microsoft Excel to input the data. The data were tested using descriptive and inferential statistics tools to achieve the study aims, such as frequency, mean, analysis of variance (ANOVA), Cronbach’s α, standard deviation, and the mean of scores to variables of study and cut of points according to rated responses for each one (cut-off points, mean of scores [M.S], normal [mean of scores 1-1.5], abnormal or symptomatic [mean of scores equal or more than 1.51]; however, the assessment of scores included all domains except BMI percentile, normal assessment extended between [1.67-2.33] and the value of M.S. if less or more this range was considered as abnormal assessment).
Results
The study included all children in governmental primary schools in the southern sector of Al-Najaf Province selected using the luck lottery approach and Table 1 presents their demographic characteristics.
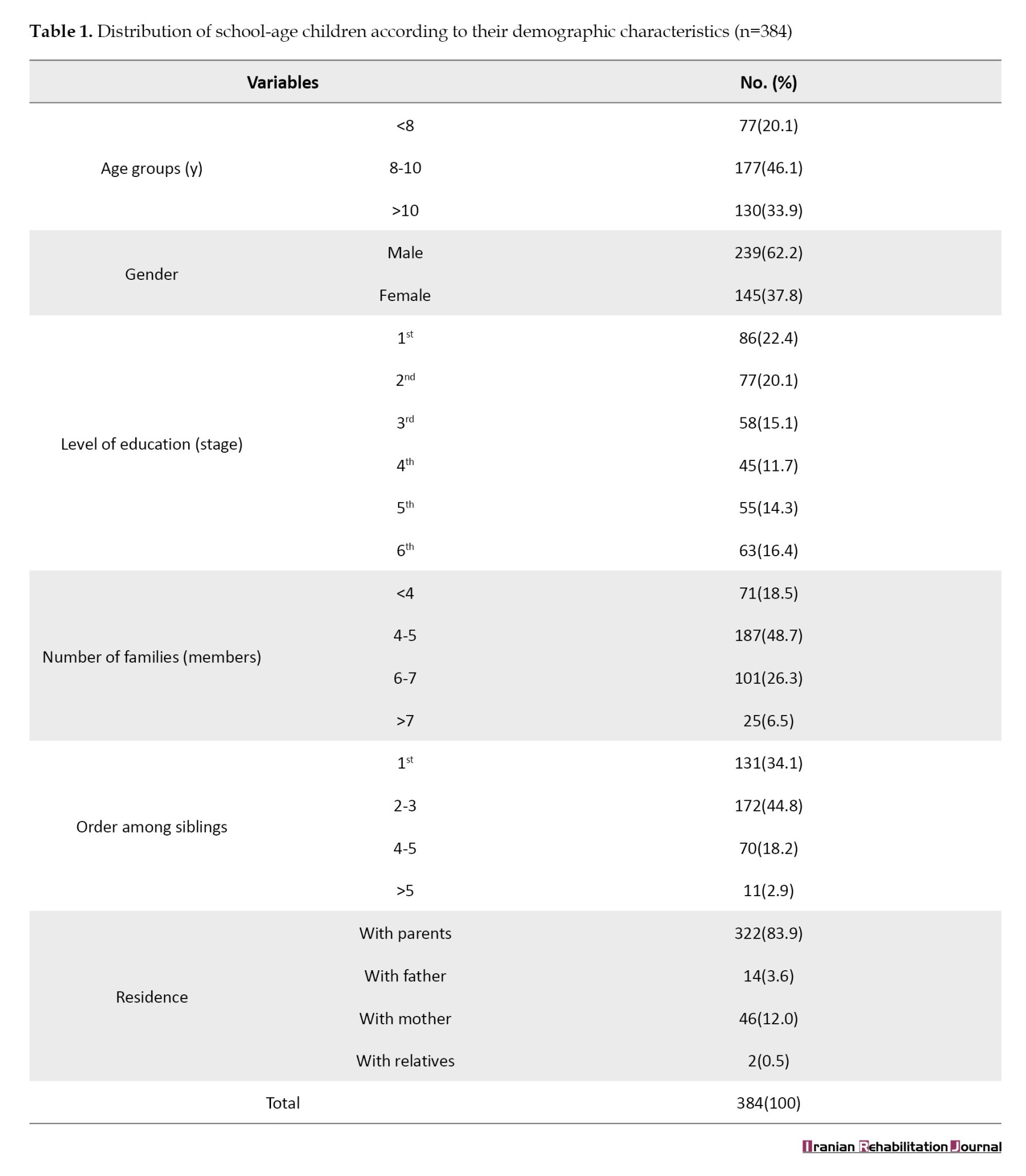
Most children were male (62.2%) and aged between (8-10) years (46.1%), with stage education in the first stage (22.4%), while less stage education of children is the fourth stage (11.7%), about half of the sample is the number of family members between (4-5) people with parents (48.7%) and only (6.5%) is a family number more than (7) people, while order among siblings is (2-3) approximately (44.8%).
This study included two variables: hostile behavior and psychophysical indicators. Table 2 shows that about (48.2%) of the sample exhibited normal behavior.
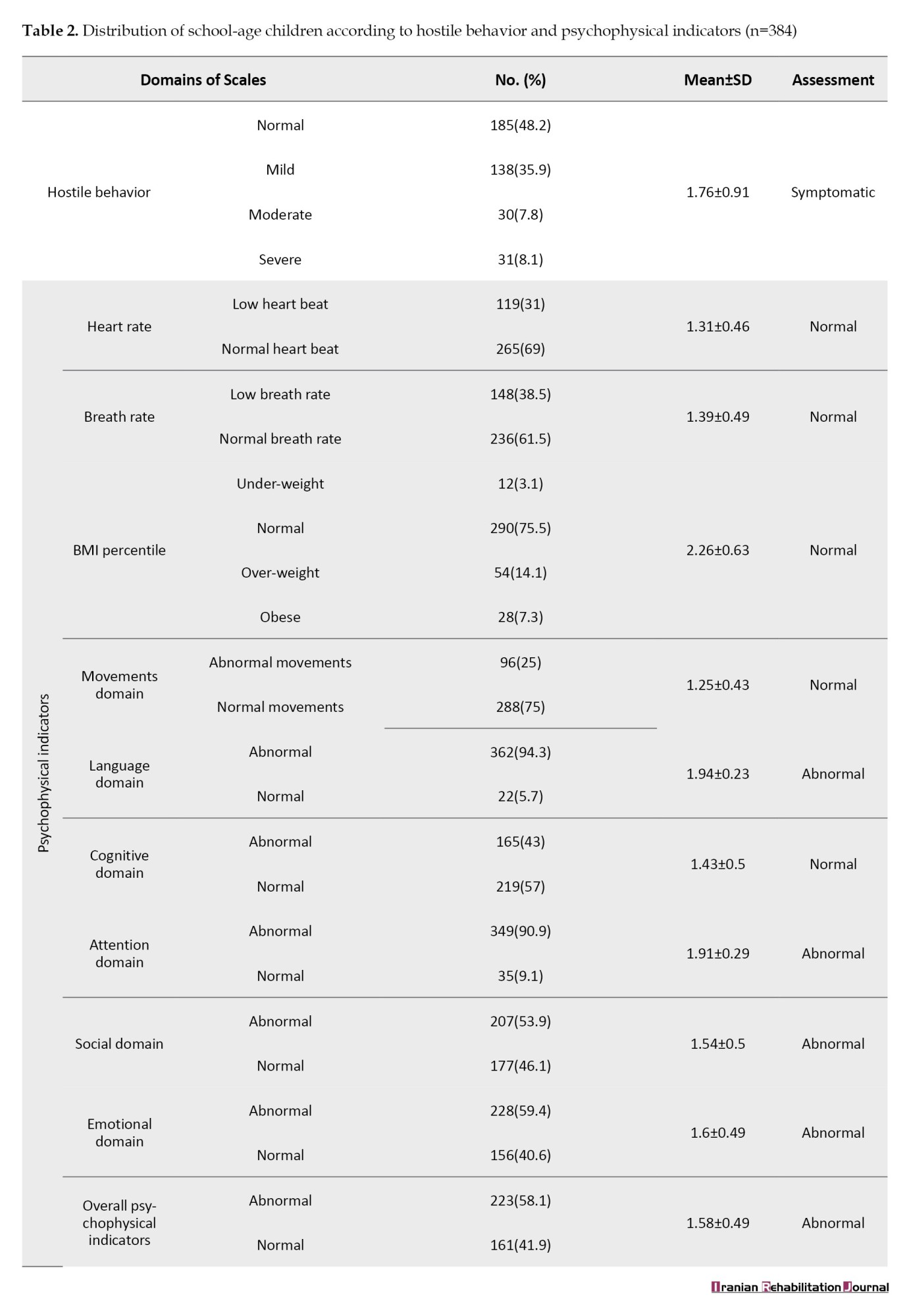
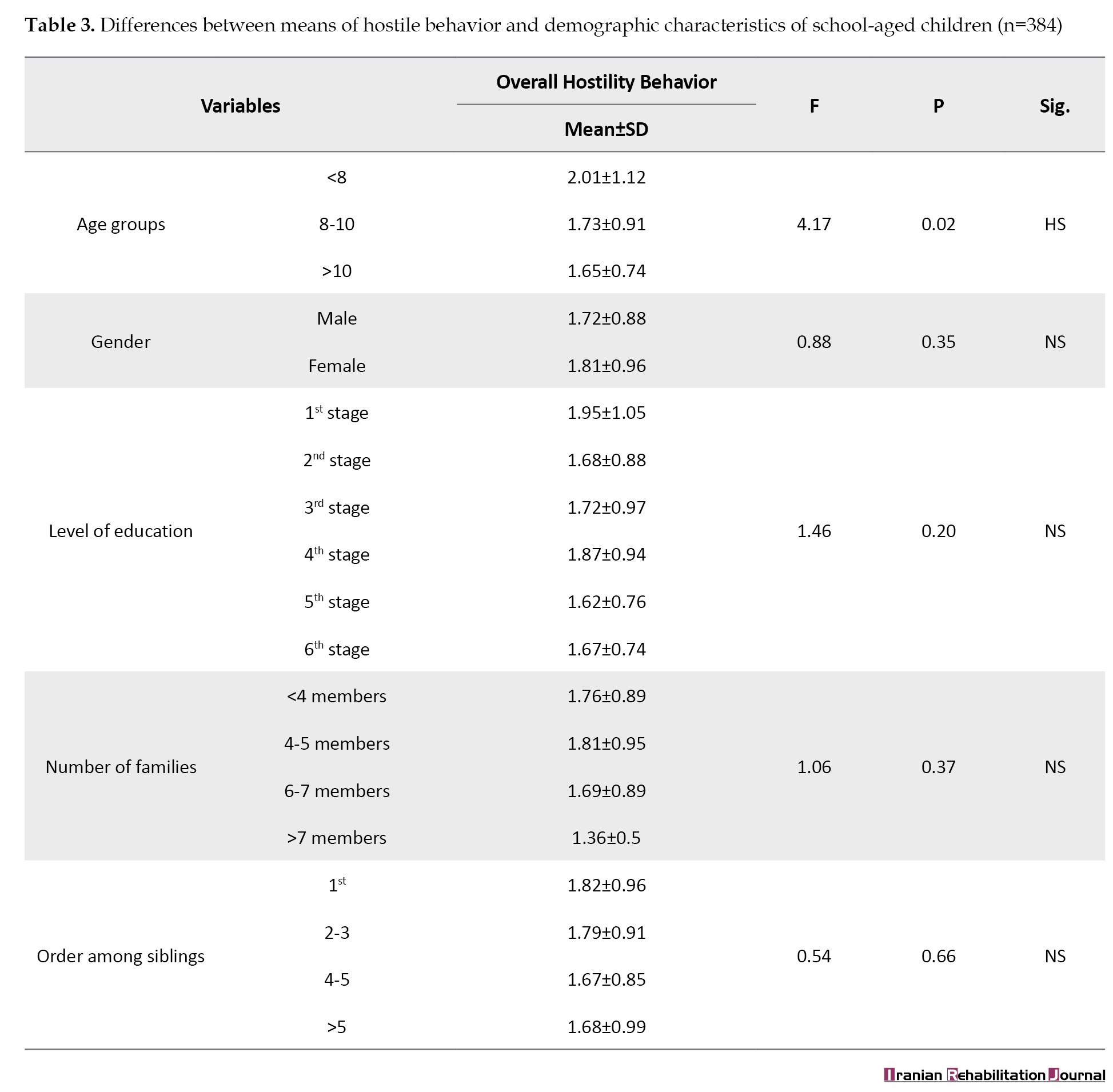
In comparison, the residual percentage of children with symptoms of hostile behavior and severity extending from mild severity (35.9%) to severe is lower (8.1%); however, according to the mean score, the assessment is symptomatic behavior. While physical indicators are normal in assessment among children, psychological indicators are normal in cognitive aspects only and abnormal in all other psychological indicators, such as language, attention, emotion, social, and overall. Table 3 shows that the differences between the mean hostile behavior and demographic characteristics of children are highly significant with age group only, while it had no significant meaning with gender, level of education, residence, and number of families.
On the other hand, Table 4 showed that psychophysical indicators had a highly significant meaning with age group and level of education at P=0.05; however, they had no significant meaning with gender, residence and number of families at P=0.05.
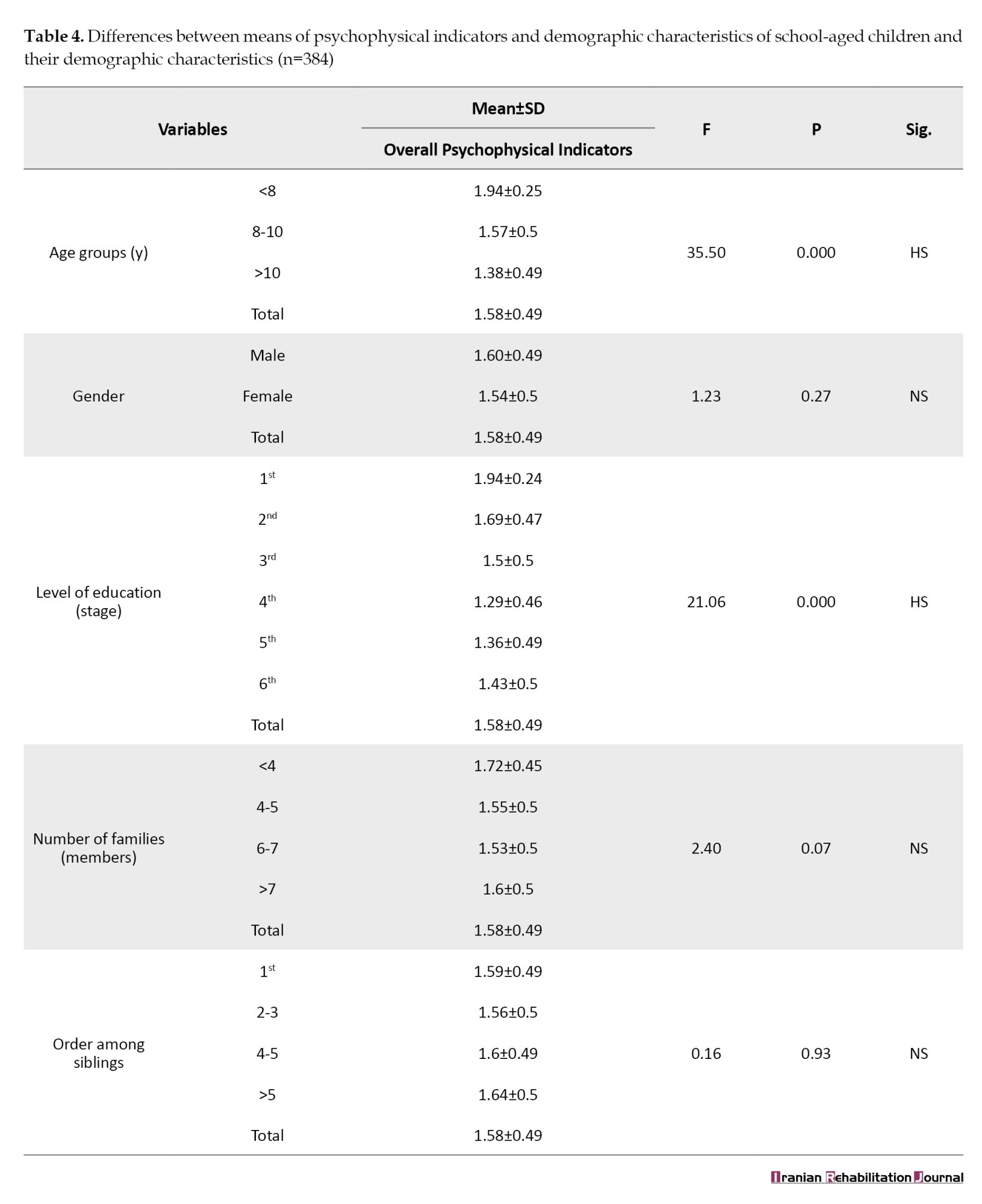
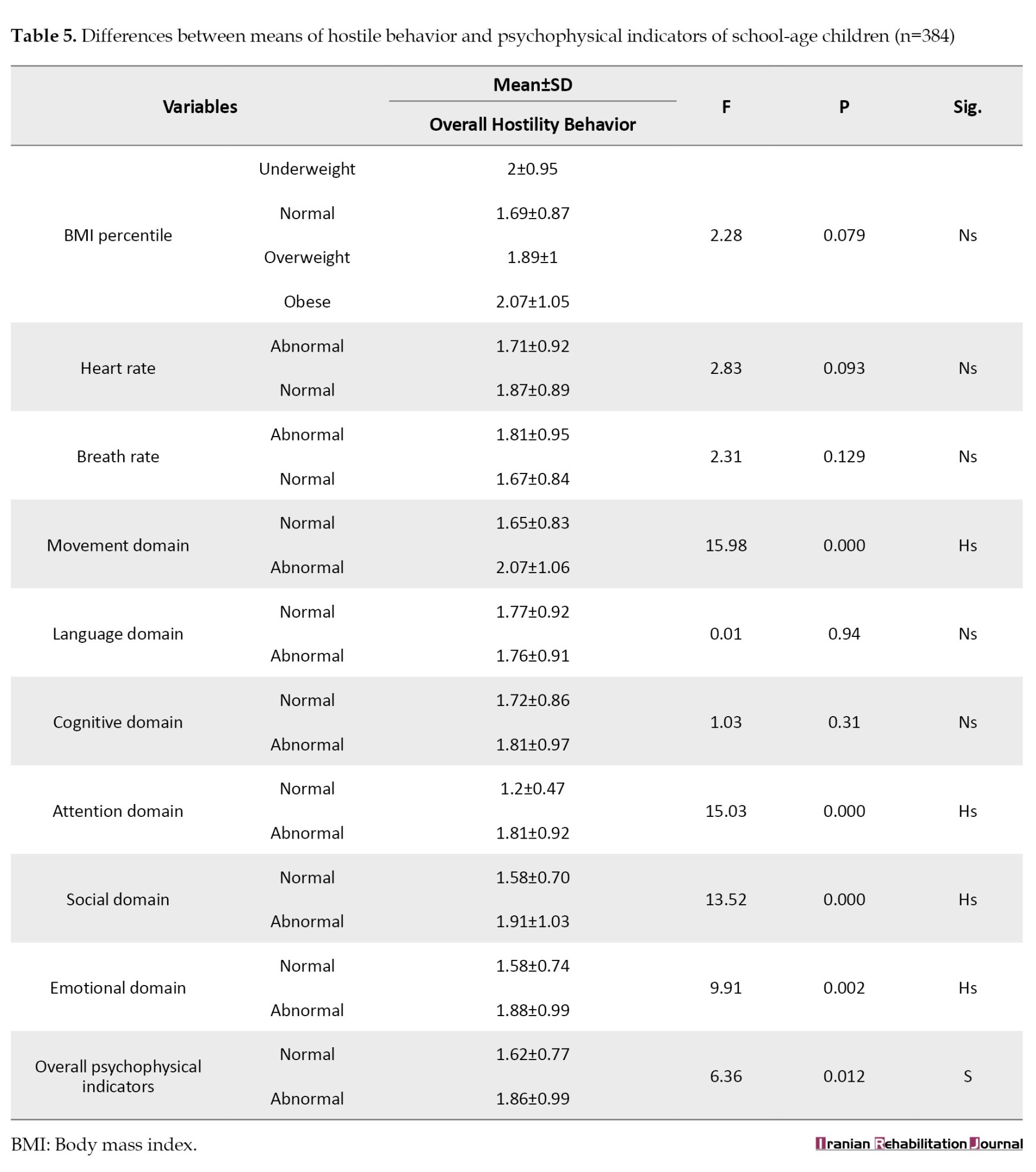
Table 5 showed no significant relationship between children’s hostile behavior and their psychophysical indicators and between hostile behavior and BMI, heart rate, breath rate, language and cognitive at (0.05), but a highly significant relationship between hostility with their movement, attention, social, and emotional behavior and a significant relationship with overall psychophysical indicators at (P=0.003).
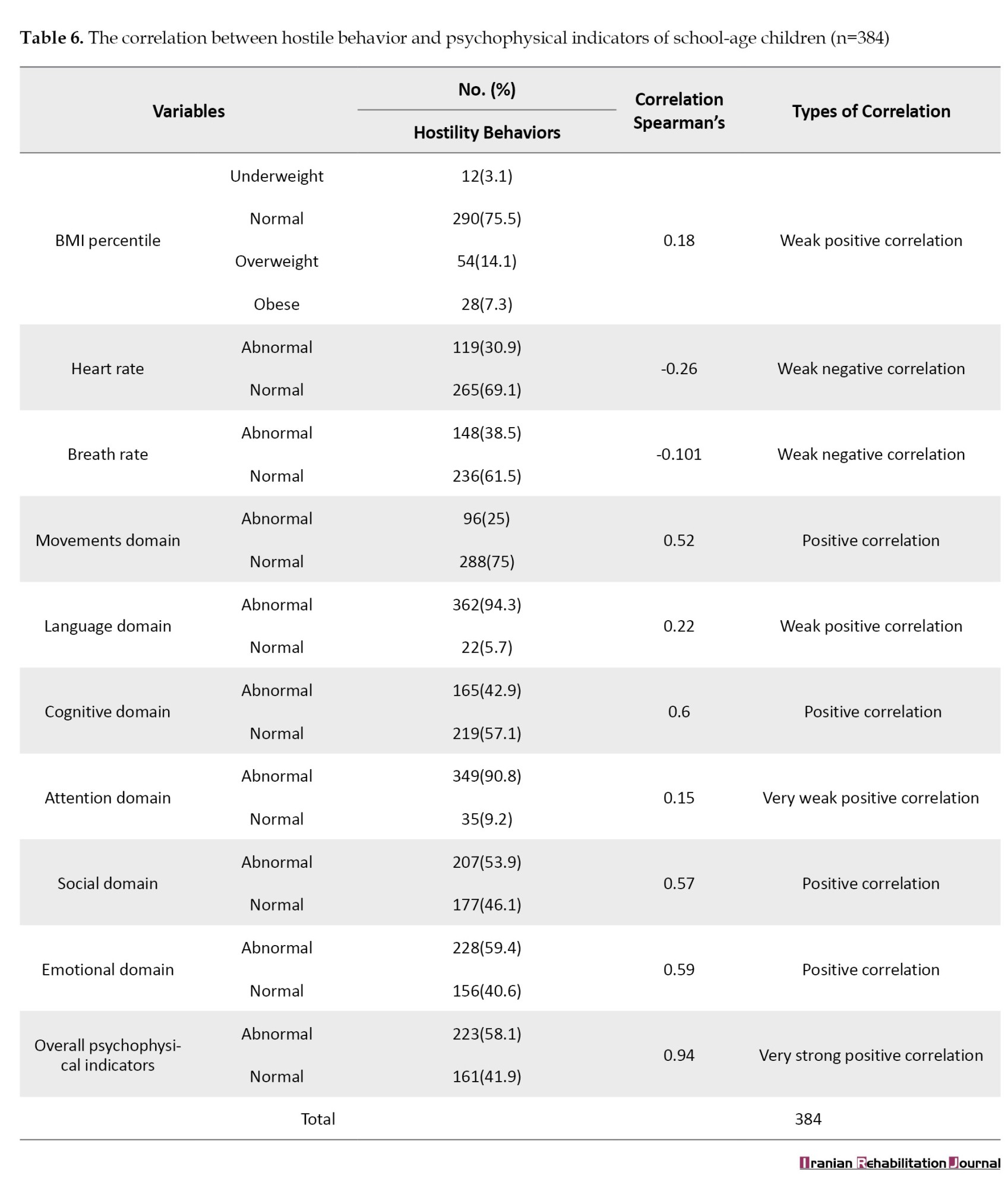
Finally, Table 6 shows a weak correlation between hostility and psychophysical indicators in most domains, except for cognitive, movement, social and emotional domains, and a high correlation with the overall psychophysical indicator domains of school-aged children.
Discussion
Hostility behaviors and psychophysical indicators affect children and their parents during the early school-age period because they are crucial in forming the personality, impressions, and development of their physical and psychological health [21]. However, only a few studies have examined these variables in Iraq.
Therefore, this study focused on school-aged children to establish an essential background for future studies. Growth in children is a crucial process related to many indicators that every child should achieve normal and healthy mental and physical growth. This study revealed the psychophysical indicators normally in all measured physical indicators, such as BMI percentile, heart rate, breathing, and their motors and movements, and psychological aspects were normally in cognitive indicators only. However other psychological indicators were found to be abnormal in assessment, such as attention, language and understanding, emotions, social relationships, and assessment of overall psychophysical indicators. Perhaps because the culture of Iraqi society focuses on the physical aspects of the child and neglects the psychological aspects due to their lack of awareness, in addition to the fact that most parents have a low level of education, which negatively reflects the child’s psychological health, which is consistent with the results of Alhamoodi [22].
However, hostile behavior is a common problem among children, especially among Iraqi children, because the nurturing of parents depends on the punishments and nerviness, especially toward boys than girls, and it often extends to violence; this result of the study revealed that more than half of the children had hostile behavior extending from mild (35.9%) to severe (8.1%) and lived with their biological parents about (83.9%), which is consistent with the results of Kamphuis et al. as well as with studies by Rahayu and Putera, which examined the relationship between hostile behaviors with some habits among school-age children [23, 24].
Finally, the study confirmed the importance of studying hostility as a problem needed to treat children in this age group because it has profound impacts on the child in the future and on parents and society in the present; many factors may arise from this behavior among children, such as psychophysical indicators, which have a significant effect on exhibiting hostile behavior when the child has psychological and physical health problems. Also, the severity of hostile behavior among children when they are exposed to bullying or family neglect should be considered. Moreover, hostile behavior increases when a child has many problems with psychophysical indicators. On the other hand, this issue is not only in Iraq, but worldwide. Other factors can be attributed to the increase in hostile behavior, such as lack of parental nurturing and educational systems, life stresses, and modernization aspects, such as social media, video games, and non-purposeful movies. This result is consistent with that reported by Owens et al. [25].
Conclusion
This study concluded that more than half of the children had symptoms of hostile behavior and had problems with overall psychophysical indicators; however, some indicators were normal, such as BMI percentile, heart rate, breathing, and cognitive and movement indicators. Also, the study concluded that when psychophysical indicators are poor or abnormal among children, the severity and symptoms of hostile behavior increase. The study recommends increasing parents’ awareness of mental health by teaching them how to nurture their children and integrating programs in the education system, especially in the primary school curriculum, how to control the child’s anger, and accepting a situation that triggers hostile behavior and prevents it.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of College of Medicine, University of Kufa, Kufa, Iraq (Code: MEC-0081-2023). After receiving the study’s title, objectives and questionnaire, the medical Ethics Committee evaluated and approved the study’s instruments (questionnaire). The study was conducted by the Declaration of Helsinki.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Investigation, data collection and writing the original draft: Zahra Anwar Fadhel; Conceptualization: Astabrak Ali Naji; Final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors appreciate the support of the elementary schools in Al-Najaf Province’s south sector, education staff, parents and participating pupils.
References
Psychophysical indicators are the most crucial criteria for detecting the health state of children, especially at the school-age stage [1]. Therefore, this stage is vital in a child’s life because it exposes him to various factors and affects his growth and development [2]. It is also essential in shaping a child’s personality traits and academic journey [3]. Psychophysical indicators encompass various aspects related to the health state of children, including the main psychological aspects, such as cognitive and learning features, language and understanding [4], attention, emotions [5], and social relationships [6]. The language domain is vital for evaluation because it is an essential indicator of the level of knowledge and cognitive skills [7]. The cognitive domain is crucial for children’s academic success, social interaction, and overall wellbeing [8]. Together, these domains reflect children’s psychological health and are associated with their thriving and success in school and life [9]. These indicators help determine whether a child is developing problematic or non-problematic and predict the children’s future psychological health [10]. The physical aspects included body mass index (BMI) percentile, heart rate, breathing, and movement indicators. The BMI percentile is crucial for children’s health [11]. Some studies showed that children who have abnormal weight may be more prone to hostile behavior, low self-esteem, and difficulties in relationships with others [12] [13]. Developing fine motor skills in childhood is crucial for overall development, impacting a child’s academic and practical abilities and social connections throughout life [14].
Hostile behavior can lead to health, psychological, and social impacts on the child, family, and peers, and hostile children are at risk of experiencing emotional distress, such as phobias, depression and panic attacks [15]. Thus distresses can harm themselves or others, and children need more health services and support than normal children in schools, homes, and communities [16, 17].
This study aims to assess hostile behavior and psychophysical indicators among school-age children and determine the relationship between psychophysical indicators and hostile behavior.
Materials and Methods
Study design
A cross-sectional study design was used to fit the study objectives. This design achieved its objectives by providing valuable insights into population traits and detecting correlations for further research.
Setting of study
This study was conducted in Al-Najaf Province, Iraq, and included primary governmental schools. Al-Najaf governorate is located in the middle of Iraq and is one of the crucial holy provinces in Iraq and the Islamic world. Al-Najaf governorate had six main sectors, and the researchers of one sector were randomly selected to conduct the study. This study was conducted from December 1, 2023, to the end of February 2024.
Al-Najaf primary schools had more than (571) governmental and private schools (17), but the study sample included only (21) girls’ and boys’ primary schools. These schools include only governmental schools located in the southern sector. By 2023, these primary schools accommodated more than 200 thousand children, but the number of new schools has increased. All children who participated in the study informed their parents about the study’s aims and the importance of their participation before meeting the child. Data were collected using a modified Arabic version of the hostile behavior and psychophysical indicators scale for school-aged children.
Sample size
The study sample was a cluster sample, including 384 children who studied in the southern sector of Al-Najaf primary schools and whose parents agreed to participate. The sample was selected using a simple sampling method (luck lottery) and all children in all governmental primary schools were allowed to participate in the study. This study included this category because this class is a transition stage in a child’s life between childhood and adolescence, which is crucial in developing physical and mental health, personal traits, behaviors and dealing with peers and educated teachers.
The sample size of the study was calculated 6 294 children according to the size of the population target (school-aged children) in governmental schools in the southern sector of Al-Najaf Province, therefore the sample size was equal to 384 children according to the calculated size tables [18]. The study depended on the objectives and criteria of the study sample to reduce the bias that could occur and give all school-age children an equal chance to exhibit in the study.
Study instruments
The study variables included the vital aspects of psychophysical indicators in this stage, including the severity of hostile behavior among children and demographic characteristics related to and affecting these variables, such as age, order among siblings, sex and stage study.
The study used the adopted tool to measure the study variables and included three main parts: demographic characteristics of children, such as age, order among siblings, sex, and stage study and the hostile behavior scale of the Arabic version of the manual of psychological and educational standards and tests, designed each scale of the Arabic environment. The hostile behavior scale was designed to detect the severity of hostile behavior in children or those suspected of having symptoms. The scale had three rated responses: Always to never (3-1). The explanation by cutting the points of the symptoms and severity of hostility can be assessed from normal to severe.
The second part related to the psychophysical indicators scale included the first two sub-parts related to the psychological indicators scale (33) with items, including five crucial aspects, such as cognitive problems (8 items), attention problems (6 items), language problems (10 items), social problems (5 items), emotional problems (4 items) and the second sub-part related to physical indicators, including BMI percentile (weight, height with birth date), heart rate, breath rate and movement aspect (10 items), which explained their score using the score and cut of points for each indicator with the final scale.
Validity and reliability of the instrument
The instrument’s validity was examined using content validity and about 13 experts in the psychology and psychiatric fields and modified with study variables. The reliability of hostile behavior (0.92) and psychophysical indicators (0.88) was obtained using Cronbach’s α compared to studies of Buss and Bint Ibrahim Al-Omar (0.78) [19, 20].
Data analysis
The study results were analyzed using SPSS software, version 24 and Microsoft Excel to input the data. The data were tested using descriptive and inferential statistics tools to achieve the study aims, such as frequency, mean, analysis of variance (ANOVA), Cronbach’s α, standard deviation, and the mean of scores to variables of study and cut of points according to rated responses for each one (cut-off points, mean of scores [M.S], normal [mean of scores 1-1.5], abnormal or symptomatic [mean of scores equal or more than 1.51]; however, the assessment of scores included all domains except BMI percentile, normal assessment extended between [1.67-2.33] and the value of M.S. if less or more this range was considered as abnormal assessment).
Results
The study included all children in governmental primary schools in the southern sector of Al-Najaf Province selected using the luck lottery approach and Table 1 presents their demographic characteristics.
Most children were male (62.2%) and aged between (8-10) years (46.1%), with stage education in the first stage (22.4%), while less stage education of children is the fourth stage (11.7%), about half of the sample is the number of family members between (4-5) people with parents (48.7%) and only (6.5%) is a family number more than (7) people, while order among siblings is (2-3) approximately (44.8%).
This study included two variables: hostile behavior and psychophysical indicators. Table 2 shows that about (48.2%) of the sample exhibited normal behavior.
In comparison, the residual percentage of children with symptoms of hostile behavior and severity extending from mild severity (35.9%) to severe is lower (8.1%); however, according to the mean score, the assessment is symptomatic behavior. While physical indicators are normal in assessment among children, psychological indicators are normal in cognitive aspects only and abnormal in all other psychological indicators, such as language, attention, emotion, social, and overall. Table 3 shows that the differences between the mean hostile behavior and demographic characteristics of children are highly significant with age group only, while it had no significant meaning with gender, level of education, residence, and number of families.
On the other hand, Table 4 showed that psychophysical indicators had a highly significant meaning with age group and level of education at P=0.05; however, they had no significant meaning with gender, residence and number of families at P=0.05.
Table 5 showed no significant relationship between children’s hostile behavior and their psychophysical indicators and between hostile behavior and BMI, heart rate, breath rate, language and cognitive at (0.05), but a highly significant relationship between hostility with their movement, attention, social, and emotional behavior and a significant relationship with overall psychophysical indicators at (P=0.003).
Finally, Table 6 shows a weak correlation between hostility and psychophysical indicators in most domains, except for cognitive, movement, social and emotional domains, and a high correlation with the overall psychophysical indicator domains of school-aged children.
Discussion
Hostility behaviors and psychophysical indicators affect children and their parents during the early school-age period because they are crucial in forming the personality, impressions, and development of their physical and psychological health [21]. However, only a few studies have examined these variables in Iraq.
Therefore, this study focused on school-aged children to establish an essential background for future studies. Growth in children is a crucial process related to many indicators that every child should achieve normal and healthy mental and physical growth. This study revealed the psychophysical indicators normally in all measured physical indicators, such as BMI percentile, heart rate, breathing, and their motors and movements, and psychological aspects were normally in cognitive indicators only. However other psychological indicators were found to be abnormal in assessment, such as attention, language and understanding, emotions, social relationships, and assessment of overall psychophysical indicators. Perhaps because the culture of Iraqi society focuses on the physical aspects of the child and neglects the psychological aspects due to their lack of awareness, in addition to the fact that most parents have a low level of education, which negatively reflects the child’s psychological health, which is consistent with the results of Alhamoodi [22].
However, hostile behavior is a common problem among children, especially among Iraqi children, because the nurturing of parents depends on the punishments and nerviness, especially toward boys than girls, and it often extends to violence; this result of the study revealed that more than half of the children had hostile behavior extending from mild (35.9%) to severe (8.1%) and lived with their biological parents about (83.9%), which is consistent with the results of Kamphuis et al. as well as with studies by Rahayu and Putera, which examined the relationship between hostile behaviors with some habits among school-age children [23, 24].
Finally, the study confirmed the importance of studying hostility as a problem needed to treat children in this age group because it has profound impacts on the child in the future and on parents and society in the present; many factors may arise from this behavior among children, such as psychophysical indicators, which have a significant effect on exhibiting hostile behavior when the child has psychological and physical health problems. Also, the severity of hostile behavior among children when they are exposed to bullying or family neglect should be considered. Moreover, hostile behavior increases when a child has many problems with psychophysical indicators. On the other hand, this issue is not only in Iraq, but worldwide. Other factors can be attributed to the increase in hostile behavior, such as lack of parental nurturing and educational systems, life stresses, and modernization aspects, such as social media, video games, and non-purposeful movies. This result is consistent with that reported by Owens et al. [25].
Conclusion
This study concluded that more than half of the children had symptoms of hostile behavior and had problems with overall psychophysical indicators; however, some indicators were normal, such as BMI percentile, heart rate, breathing, and cognitive and movement indicators. Also, the study concluded that when psychophysical indicators are poor or abnormal among children, the severity and symptoms of hostile behavior increase. The study recommends increasing parents’ awareness of mental health by teaching them how to nurture their children and integrating programs in the education system, especially in the primary school curriculum, how to control the child’s anger, and accepting a situation that triggers hostile behavior and prevents it.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of College of Medicine, University of Kufa, Kufa, Iraq (Code: MEC-0081-2023). After receiving the study’s title, objectives and questionnaire, the medical Ethics Committee evaluated and approved the study’s instruments (questionnaire). The study was conducted by the Declaration of Helsinki.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Investigation, data collection and writing the original draft: Zahra Anwar Fadhel; Conceptualization: Astabrak Ali Naji; Final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors appreciate the support of the elementary schools in Al-Najaf Province’s south sector, education staff, parents and participating pupils.
References
- Al-Hamoodi AAN, Al Dujaili AH. Assessing the issues of Children’s parents with autism spectrum disorders in Al-Najaf City. International Journal of Scientific and Research Publications. 2017; 7(7):597-605. [Link]
- Günaydın D. [The effects of poverty on children: Approaches to break the intergenerational poverty cycle (Turkish)]. Journal of Suleyman Demirel University Institute of Social Sciences. 2021; (41):155-83. [Link]
- Norbadalovna BT, Abduxalilova TF, Jahongirovna EO, Sodiqovna TI. Development of personality traits in school-age children. The American Journal of Social Science and Education Innovations. 2020; 02(12):318-30. [DOI:10.37547/tajssei/Volume02Issue12-55]
- Schalock RL, Borthwick-Duffy SA, Bradley VJ, Buntinx WH, Coulter DL, Craig EM, et al. Intellectual disability: Definition, classification, and systems of supports. Maryland: American Association on Intellectual and Developmental Disabilities; 2010. [Link]
- Lolk A. Neurokognitive lidelser. In: American Psychiatric Association, editor. Diagnostic and statistical manual of mental disorders. 5th ed. Virginia: American Psychiatric Association; 2013. [Link]
- Gredler GR. Bullying at school: What we know and what we can do. Psychology in the Schools. 2003; 40(6):699-700. [DOI:10.1002/pits.10114]
- Scharf RJ, Scharf GJ, Stroustrup A. Developmental milestones. Pediatrics in Review. 2016; 37(1):25-37. [DOI:10.1542/pir.2014-0103] [PMID]
- Peng P, Kievit RA. The development of academic achievement and cognitive abilities: A bidirectional perspective. Child Development Perspectives. 2020; 14(1):15-20. [DOI:10.1111/cdep.12352] [PMID]
- Thomson KC, Oberle E, Gadermann AM, Guhn M, Rowcliffe P, Schonert-Reichl KA. Measuring social-emotional development in middle childhood: The Middle Years Development Instrument. Journal of Applied Developmental Psychology. 2018; 55:107-18. [DOI:10.1016/j.appdev.2017.03.005]
- Greenwood CR, Walker D, Carta JJ, Higgins SK. Developing a general outcome measure of growth in the cognitive abilities of children 1 to 4 years old: The early problem-solving indicator. School Psychology Review. 2006; 35(4):535-51. [DOI:10.1080/02796015.2006.12087960]
- Whitlock G, Lewington S, Sherliker P, Clarke R, Emberson J, Halsey J, et al. Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet. 2009; 373(9669):1083-96. [DOI:10.1016/S0140-6736(09)60318-4] [PMID]
- Cheng S, Kaminga AC, Liu Q, Wu F, Wang Z, Wang X, et al. Association between weight status and bullying experiences among children and adolescents in schools: An updated meta-analysis. Child Abuse & neglect. 2022; 134:105833. [DOI:10.1016/j.chiabu.2022.105833] [PMID]
- Verbecque E, Coetzee D, Smits-Engelsman B. Underweight children are agile but lack power. BMC Pediatrics. 2022; 22(1):490. [DOI:10.1186/s12887-022-03544-3] [PMID]
- Maranatha JR, Briliany N. Enhancing fine motor skills in early childhood through fun cooking activities: A quasi-experimental study in Purwakarta, Indonesia. Golden Age: Jurnal Ilmiah Tumbuh Kembang Anak Usia Dini. 2023; 8(4):203-12. [DOI:10.14421/jga.2023.84-01]
- Liu J, Lewis G, Evans L. Understanding aggressive behaviour across the lifespan. Journal of Psychiatric and Mental Health Nursing. 2013; 20(2):156-68.[DOI:10.1111/j.1365-2850.2012.01902.x] [PMID]
- Akman Y. The Relationship between school climate and students' aggressive behaviors. International Journal of Progressive Education. 2021; 17(2):430-48.[DOI:10.29329/ijpe.2021.332.26]
- Birhan W, Shiferaw G, Amsalu A, Tamiru M, Tiruye H. Exploring the context of teaching character education to children in preprimary and primary schools. Social Sciences & Humanities Open. 2021; 4(1):100171. [DOI:10.1016/j.ssaho.2021.100171]
- Krejcie RV, Morgan DW. Determining sample size for research activities. Educational and Psychological Measurement. 1970; 30(3):607-10 [DOI:10.1177/001316447003000308]
- Buss DM, Shackelford TK. Human aggression in evolutionary psychological perspective. Clinical Psychology Review. 1997; 17(6):605-19. [DOI:10.1016/S0272-7358(97)00037-8] [PMID]
- Al Kabi Z, Alhamoody A. Prevalence of hostile behavior among school-age children in Al-Najaf governorate. Mosul Journal of Nursing. 2025; 13(1): 72-86. (Unpublished article)
- Al-Hamoodi AAN, Falah MA, Al-Ghrebawi RH. The relationship between sleep pattern habits with severity of disruptive behaviors among elementary school children. Iranian Rehabilitation Journal. 2024; 22(4):627-38. [DOI: 10.32598/irj.22.4.1748.4]
- Al-Hamoodi AAN. Depressive symptoms among overweight students at University of Kufa. Global Scientific Journal. 2018; 6(11):196-207. [Link]
- Kamphuis J, Meerlo P, Koolhaas JM, Lancel M. Poor sleep as a potential causal factor in aggression and violence. Sleep medicine. 2012; 13(4):327-34. [DOI:10.1016/j.sleep.2011.12.006] [PMID]
- Rahayu IS, Putera F. The relationship between exploitative show viewing habits and aggressive behaviour in adolescents. Asian Journal of Public Health and Nursing. 2024; 1(3). [DOI.10.62377/xyga9731]
- Owens JA, Dearth-Wesley T, Lewin D, Gioia G, Whitaker RC. Self-regulation and sleep duration, sleepiness, and chronotype in adolescents. Pediatrics. 2016; 138(6):e20161406. [DOI:10.1542/peds.2016-1406] [PMID]
Article type: Original Research Articles |
Subject:
Psychiatry
Received: 2024/07/15 | Accepted: 2024/08/10 | Published: 2025/03/1
Received: 2024/07/15 | Accepted: 2024/08/10 | Published: 2025/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
