
988368
Thu, Jul 30, 2026

Volume 23, Issue 3 (September 2025)
Iranian Rehabilitation Journal 2025, 23(3): 257-266 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gharib M, Razavipour M, Amini P M. The Upper Limb Functional Index: Cross-cultural Adaptation for Iranian Patients. Iranian Rehabilitation Journal 2025; 23 (3) :257-266
URL: http://irj.uswr.ac.ir/article-1-2531-en.html
URL: http://irj.uswr.ac.ir/article-1-2531-en.html



1- Orthopedic Research Center, Mazandaran University of Medical Sciences, Sari, Iran.
2- Student Research Committee, Mazandaran University of Medical Sciences, Sari, Iran.
2- Student Research Committee, Mazandaran University of Medical Sciences, Sari, Iran.
Full-Text [PDF 539 kb]
(490 Downloads)
| Abstract (HTML) (2454 Views)
Full-Text: (360 Views)
Introduction
The upper limb plays a crucial role in performing daily activities, from fundamental tasks, such as writing and eating, to more complex activities, including the use of technical tools and sports [1]. Musculoskeletal disorders affecting the upper limb can involve various structures, including tendons, muscles, ligaments, nerves, and spinal segments [2]. These conditions can significantly impair an individual’s range of motion, muscle strength, and overall quality of life [3]. Common symptoms, such as swelling, pain, tingling, and functional limitations, can severely restrict daily activities and independence [4, 5].
Several outcome measures have been developed to assess upper limb function and evaluate the impact of therapeutic interventions [6, 7]. The upper limb functional index (ULFI) is a widely used instrument designed to assess functional limitations in individuals with upper limb disorders [8]. This self-reported questionnaire not only quantifies patients’ ability to engage in daily and social activities but also serves as a valuable tool for clinicians and therapists to measure treatment effectiveness and track patient recovery [9].
Originally developed by Gabel et al. in 2006, the ULFI was designed to provide a precise and comprehensive assessment of upper limb function. Its brevity and ease of scoring make it particularly accessible to individuals with varying literacy levels. In 2010, Gabel et al. further refined the instrument by introducing an intermediate response option to enhance its sensitivity and specificity, replacing the conventional binary (yes/no) response format [10, 11].
Translation and cultural adaptation of validated instruments are essential in healthcare research and clinical practice. Such adaptations ensure that assessment tools maintain their reliability and validity across diverse populations, thereby facilitating accurate diagnosis, treatment planning, and international comparability of findings [12]. Developing a culturally adapted and psychometrically validated Persian version of the ULFI could significantly enhance the evaluation of upper limb function in the Iranian population and improve rehabilitation outcomes, particularly for individuals with musculoskeletal conditions.
The ULFI has been successfully adapted into several languages, including Spanish [13], Turkish [14], French-Canadian [15], Brazilian Portuguese [16], German [17], Arabic [18], Urdu [19], and Greek [20].
Given the absence of a Persian-adapted ULFI, this study aimed to address this gap by translating, adapting, and validating the questionnaire for use in Iranian patients. Establishing a culturally relevant tool will contribute to more precise functional assessments and enhance the quality of care for individuals with upper limb disorders in Iran.
Materials and Methods
Study design
This cross-sectional study aimed to translate, culturally adapt, and validate the Persian version of the ULFI for use in Iranian patients with upper limb musculoskeletal disorders. The adaptation process followed internationally recognized guidelines for cross-cultural validation of self-report instruments, incorporating translation, back-translation, expert review, and pilot testing [21]. The study was conducted in two phases. Translation and cultural adaptation to ensure linguistic and conceptual equivalence. Psychometric validation includes assessments of reliability, validity, and responsiveness. Additionally, confirmatory factor analysis (CFA) was conducted to validate the factorial structure of the Persian version of the ULFI.
Participants
A total of 200 Iranian outpatients and rehabilitation patients diagnosed with upper limb musculoskeletal disorders were recruited. The inclusion criteria included age ≥18 years, clinically diagnosed upper limb musculoskeletal disorders (e.g. rotator cuff injuries, carpal tunnel syndrome, and tendinitis), the ability to read and write in Persian, and willingness to provide informed consent.
The exclusion criteria included cognitive impairments that could hinder comprehension of the questionnaire, the presence of major systemic diseases that could confound results, and recent upper limb surgery, which could introduce variability in functional assessment.
Translation and cultural adaptation
The translation and cultural adaptation process adhered to the guidelines proposed by Beaton et al. [21] for cross-cultural adaptation of self-report measures. The process consisted of the following steps:
Forward translation: Two bilingual health science professionals independently translated the original English version of the ULFI into Persian. The two translations were compared, and discrepancies were resolved to create a single, harmonized Persian version.
Backward translation: Two additional bilingual translators, blinded to the original ULFI, independently back-translated the Persian version into English. This step ensured conceptual equivalence, rather than literal translation.
Expert panel review: A panel comprising physiotherapists, occupational therapists, and linguists reviewed the translated version to assess clarity, cultural relevance, and conceptual accuracy. Discrepancies were resolved through discussion, and a pre-final version was created.
Pilot testing: The pre-final version was administered to 20 patients with upper limb disorders to evaluate comprehension, ease of use, and potential difficulties. Feedback was incorporated, leading to the development of the final Persian version of the ULFI.
Measurements
ULFI
The ULFI is a 10-item patient-reported questionnaire assessing upper limb function in individuals with musculoskeletal disorders. Each item is scored on a 3-point Likert scale: 0) No difficulty, 1) Some difficulty, and 2) Unable to perform the activity. The total ULFI score ranges from 0 to 20, with higher scores indicating greater impairment.
Disabilities of the arm, shoulder, and hand (DASH) questionnaire
To assess convergent validity, the Persian version of the DASH questionnaire was used as a reference. The DASH is a 30-item instrument that evaluates physical function, symptoms, and social participation in patients with upper limb disorders. Scores range from 0 to 100, with higher scores indicating a greater degree of disability. The Persian DASH has been previously validated and has strong psychometric properties in Iranian populations [22].
Psychometric validation
Reliability
Internal consistency: Assessed using Cronbach’s α, with values ≥0.7 considered acceptable for reliability.
Test, re-test reliability: Evaluated by administering the Persian ULFI to 30 participants twice, 7 days apart. The intraclass correlation coefficient (ICC) was calculated, with values ≥0.75 indicating good reliability.
Validity
Construct validity: Assessed via convergent validity, by examining correlations between the Persian ULFI and DASH scores. Pearson’s correlation coefficient (r) was calculated, with values ≥0.50 considered acceptable for convergent validity.
CFA: A one-factor model was tested using AMOS (version 24). Model fit was evaluated using the following goodness-of-fit indices: chi-square/df ratio (χ²/df), comparative fit index (CFI), Tucker-Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Additionally, standardized factor loadings were examined for each item.
Responsiveness
The sensitivity of the Persian ULFI to detect functional changes over time was evaluated by administering the questionnaire to 50 patients before and after a 4-week rehabilitation program. Two measures of responsiveness were calculated, effect size (ES) and standardized response mean (SRM).
Statistical analysis
All statistical analyses were performed using SPSS software, version 26 and AMOS software, version 24.
Descriptive statistics were used to summarize the participants’ characteristics. Cronbach’s α, ICC, and Pearson’s correlation coefficient (r) were calculated to assess reliability and validity. CFA was conducted to validate the factor structure of the Persian ULFI. Statistical significance was set at P<0.05.
Results
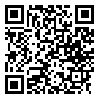
A total of 200 participants diagnosed with upper limb musculoskeletal disorders were enrolled in the study. The mean age of the participants was 45.3±12.7 years, with 58% of the subjects being female and 42% male. The most prevalent diagnoses included rotator cuff injuries (32%), carpal tunnel syndrome (28%), and tendonitis (22%). Additionally, a majority of participants (76%) reported chronic symptoms persisting for more than six months. Table 1 presents the detailed demographic and clinical characteristics.
Reliability
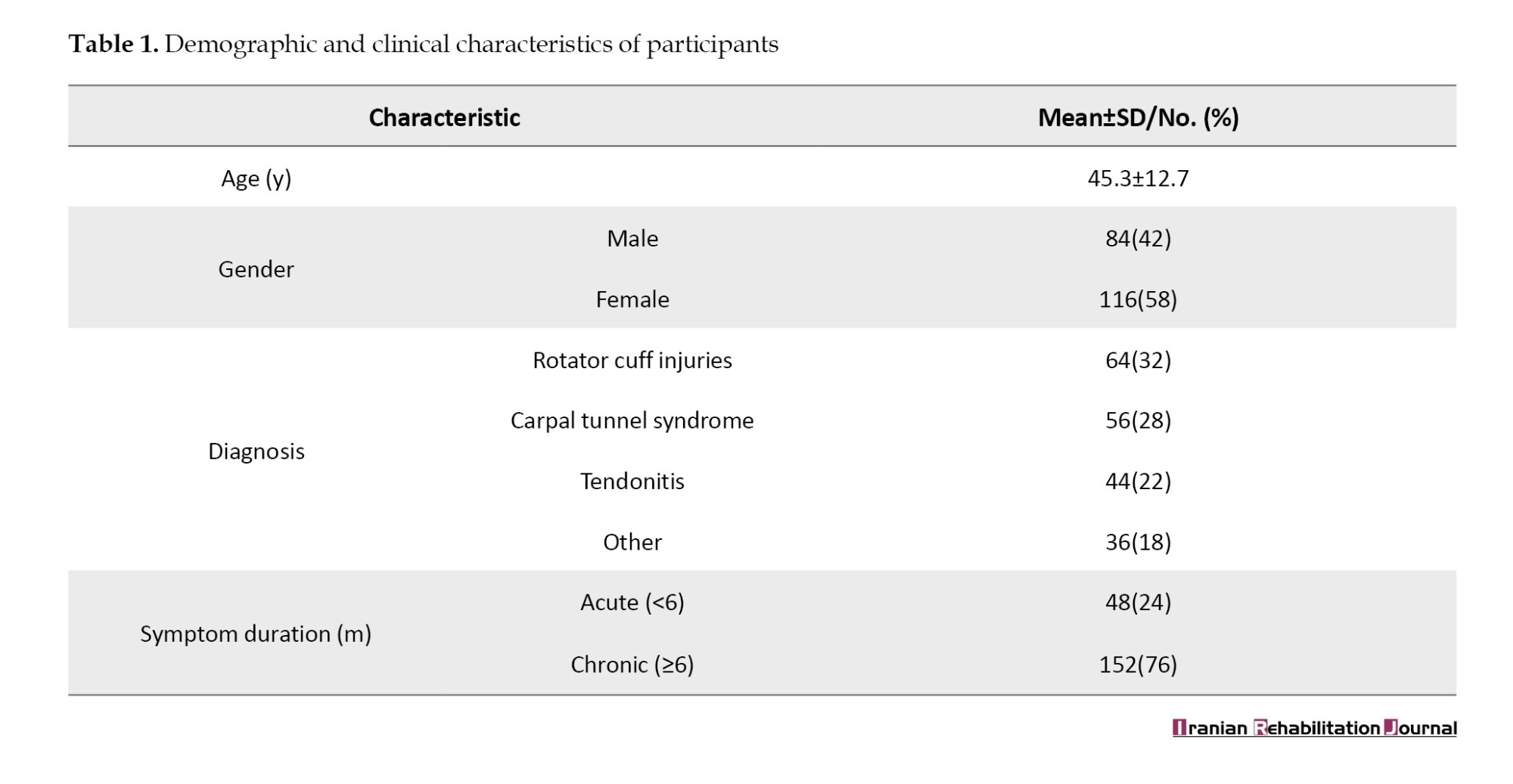
The Persian ULFI demonstrated excellent internal consistency, with Cronbach’s α=0.91, indicating high reliability. Test, re-test reliability, assessed using the ICC, yielded a value of 0.88 (95% CI, 0.82%, 0.93%), suggesting strong temporal stability of the questionnaire (Table 2).
Validity
The Persian ULFI exhibited strong convergent validity compared with the DASH questionnaire. Pearson’s correlation coefficient (r) was 0.76 (P<0.001), confirming that the Persian ULFI aligns well with the established measure of upper limb function (Table 3).

Responsiveness
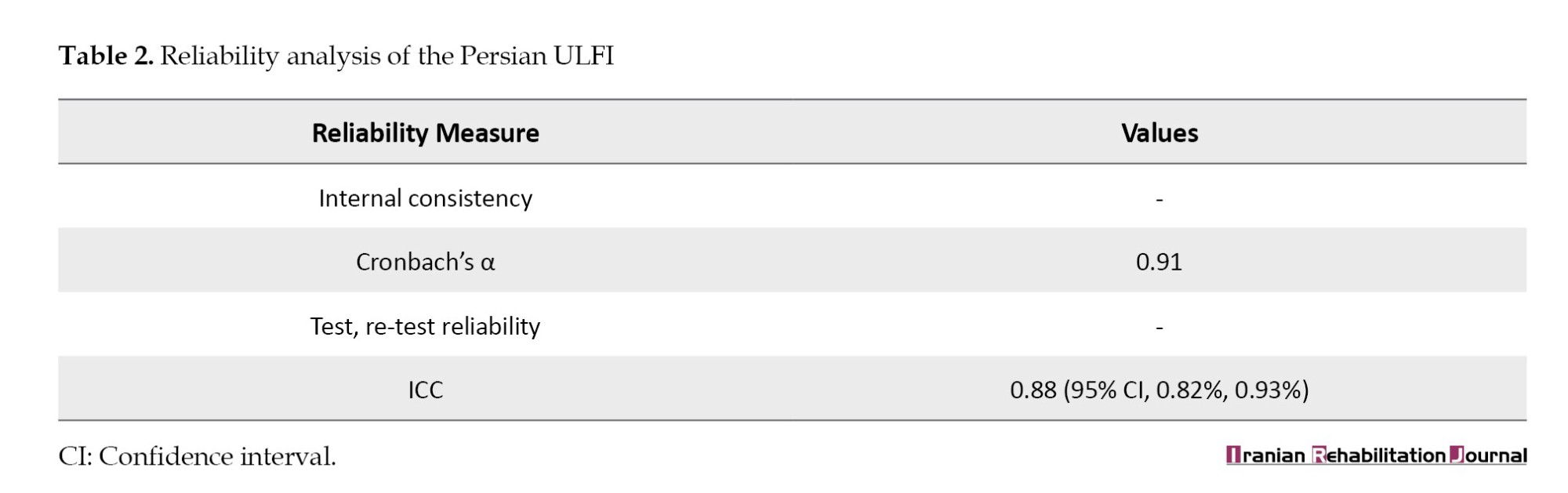
The responsiveness of the Persian ULFI was evaluated by measuring changes in scores following a 4-week rehabilitation program. A statistically significant improvement was observed (P<0.001), with the mean ULFI scores being 42.3±10.5 (pre-intervention) to 29.8±8.7 (post-intervention). The ES was 0.89, and the SRM was 1.12, indicating a strong ability to detect functional improvements over time (Table 4).
Factor structure and CFA
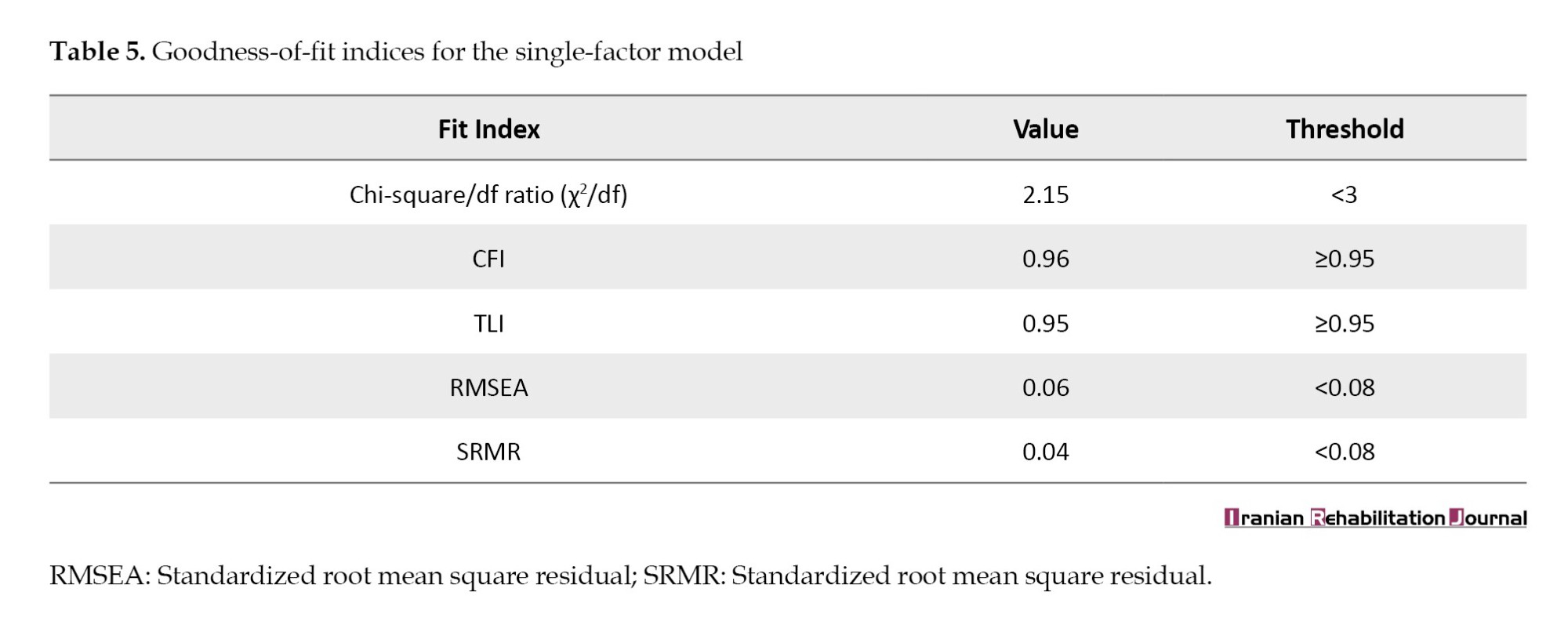
CFA supported the one-factor model of the Persian ULFI, demonstrating good model fit with the following fit indices:
Chi-square/df=2.15; CFI=0.96; TLI=0.95; RMSEA=0.06; SRMR=0.04.
These results confirm that the Persian ULFI has a strong factorial structure (Table 5).
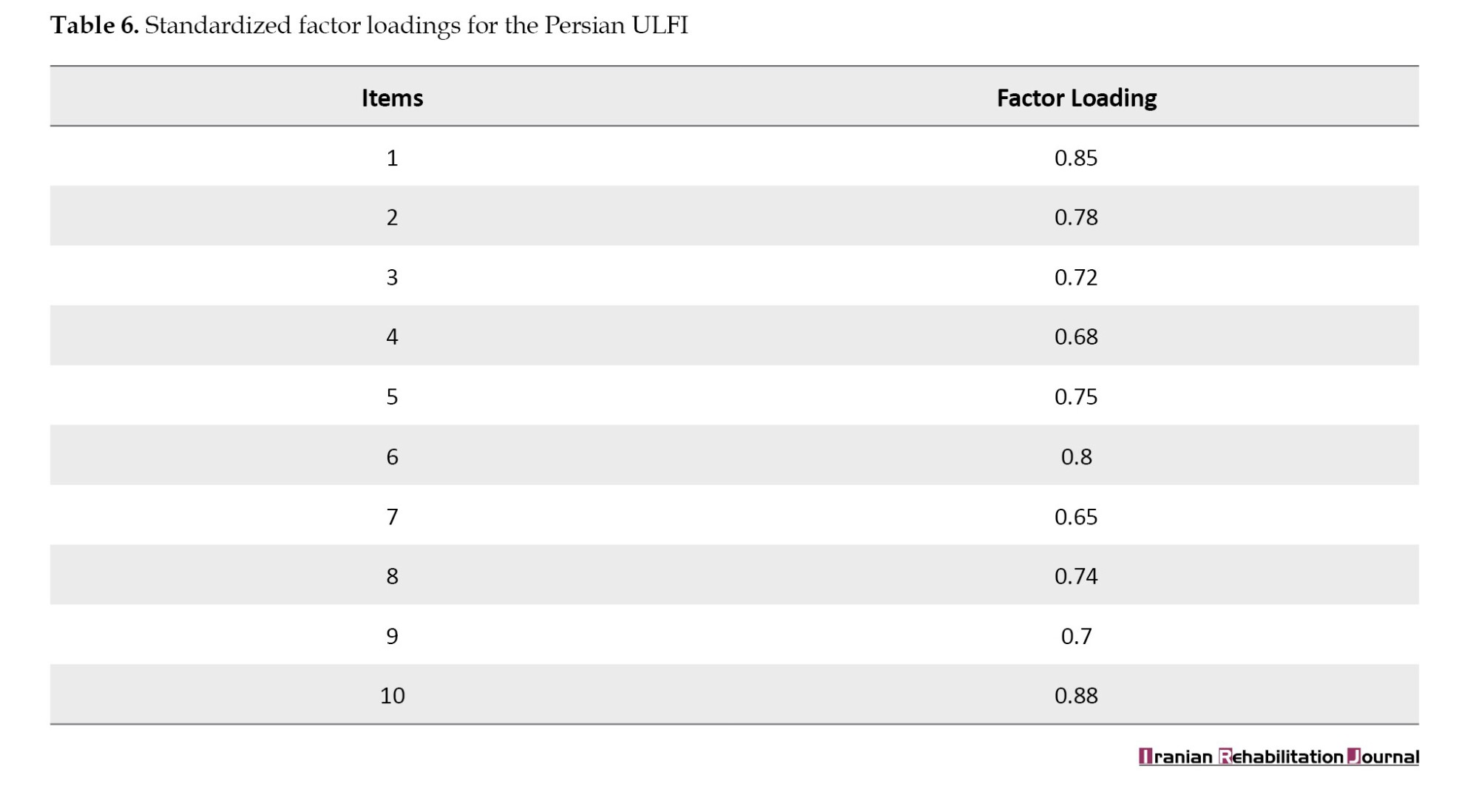
Furthermore, all items loaded significantly onto a single latent factor, with standardized factor loadings ranging from 0.65 to 0.88, indicating robust construct validity (Table 6).
Discussion
The validation of the Persian version of the ULFI represents a significant advancement in assessing upper limb function in Iranian individuals with musculoskeletal disorders. Our findings confirm that the Persian ULFI is a reliable, valid, and responsive instrument, comparable to the original English version and other culturally adapted translations. Below, we discuss the key findings in the broader context of existing literature and highlight their research and clinical implications.
The rigorous translation and cultural adaptation process ensured that the Persian ULFI maintained conceptual equivalence with the original English version while being linguistically and culturally appropriate for Iranian patients. The high content validity index underscores the strong consensus among experts regarding the clarity, relevance, and comprehensibility of translated items. This aligns with previous adaptations of the ULFI, such as those in Spanish [13] and Turkish [14], where cultural relevance was emphasized to enhance measurement accuracy across diverse populations. The successful adaptation of the ULFI into Persian highlights the importance of culturally sensitive modifications when implementing health assessment instruments internationally.
The Persian ULFI demonstrated excellent internal consistency, with a Cronbach’s α of 0.91, which is comparable to the original English version [10] and other validated translations [9, 17]. These results indicate that the items in the questionnaire are highly interrelated, effectively measuring upper limb function as a single construct. Moreover, test re-test reliability confirmed the stability of the Persian ULFI over time, making it a reliable tool for longitudinal assessment. These findings are consistent with prior research, further reinforcing the robust psychometric properties of the ULFI across different cultural contexts [10, 13, 14].
The strong correlation between the Persian ULFI and DASH questionnaires provides compelling evidence for the construct validity of the instrument. This correlation is consistent with previous findings where the ULFI exhibited moderate to strong associations with other upper limb function measures, supporting its clinical relevance and convergent validity [14, 16, 19].
CFA further validated the one-factor structure of the Persian ULFI, with excellent model-fit indices. These results support the unidimensional nature of the ULFI, confirming that it effectively captures the overall impact of musculoskeletal disorders on upper limb function without requiring subscales. Moreover, the high standardized factor loadings further substantiate the sufficiency of the single-factor model, a finding that aligns with previous language adaptations [13, 14, 16].
The Persian ULFI exhibited high responsiveness, as evidenced by significant score reductions after a 4-week rehabilitation program. The mean ULFI score decreased from 42.3±10.5 (pre-intervention) to 29.8±8.7 (post-intervention), with an ES of 0.89 and SRM of 1.12. These findings confirm the sensitivity of the Persian ULFI in detecting meaningful functional improvements over time, making it an effective outcome measure for evaluating rehabilitation. Comparable responsiveness has been reported in previous studies, in which the ULFI effectively captured changes in upper limb function across different patient populations, including those with acute and chronic musculoskeletal conditions [14, 17].
The responsiveness of the Persian ULFI demonstrated strong sensitivity to functional changes, with an SRM of 1.12, which is quantitatively comparable to other validated versions. For example, the Turkish adaptation reported an SRM of 1.10 [14], while the Arabic version showed an SRM of 1.05 [9]. These similarities highlight the Persian ULFI’s robust ability to detect clinical improvements, aligning with findings from other cultural contexts.
The successful validation of the Persian ULFI has significant implications for clinical and research applications in Iran. In clinical practice, healthcare professionals can utilize the Persian ULFI to assess the functional impact of musculoskeletal disorders on patients’ daily activities, monitor rehabilitation progress over time, and evaluate the effectiveness of therapeutic interventions in improving upper limb function.
From a research perspective, the Persian ULFI provides a standardized tool for investigating upper limb disorders in Iranian populations, facilitating comparisons with international studies and contributing to the global body of knowledge in musculoskeletal health. By establishing psychometric equivalence across languages, the Persian ULFI allows for multinational collaboration and cross-cultural research on upper limb function.
While the ULFI is a patient-reported outcome measure (PROM), performance-based tools (grip strength tests, range of motion assessments) provide objective data on physical function [6, 7]. The ULFI complements these measures by capturing patients’ perceived limitations in daily activities, which may not always correlate directly with physical performance. For instance, a patient with adequate grip strength might still report functional difficulties due to pain or fatigue. Integrating both PROMs, such as the ULFI, and performance-based measures offers a comprehensive evaluation of upper limb function, addressing both subjective experiences and objective capabilities.
While this study provides strong evidence for the validity and reliability of the Persian ULFI, certain limitations should be acknowledged. Participants were recruited from outpatient clinics and rehabilitation centers, which may limit the applicability of findings to other populations, such as primary care patients or community-based cohorts.
The study evaluated responsiveness in a relatively small sample (n=50) undergoing a 4-week rehabilitation program. Future studies should examine responsiveness in larger, more diverse patient populations, including those with varying upper limb disorders and treatment durations.
Further research is warranted to explore the use of the Persian ULFI in specific patient subgroups, such as those with traumatic injuries, neurological conditions, or occupational musculoskeletal disorders. Additionally, longitudinal studies could assess whether the Persian ULFI can predict long-term functional outcomes, such as return to work, improvements in quality of life, and sustained rehabilitation effects. Expanding validation efforts to include larger, more diverse samples would further strengthen the generalizability and clinical utility of the instrument.
Conclusion
The Persian ULFI demonstrated strong psychometric properties, including high internal consistency, test re-test reliability, convergent validity with the DASH, and responsiveness, which are comparable to those of other adaptations. Its unidimensional structure supports its use for assessing upper limb function in Iranian clinical and research settings. Similar to other PROMs, the ULFI complements performance-based measures by capturing patient-reported limitations and enriching functional evaluations. This adaptation expands culturally validated tools for musculoskeletal rehabilitation.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1399.801). Written informed consent was obtained from all participants before enrollment. The confidentiality of the participants’ data was strictly maintained throughout the study.
Funding
This research was supported by a research project funded by Mazandaran University of Medical Sciences, Sari, Iran.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all respondents who participated in this study.
References
The upper limb plays a crucial role in performing daily activities, from fundamental tasks, such as writing and eating, to more complex activities, including the use of technical tools and sports [1]. Musculoskeletal disorders affecting the upper limb can involve various structures, including tendons, muscles, ligaments, nerves, and spinal segments [2]. These conditions can significantly impair an individual’s range of motion, muscle strength, and overall quality of life [3]. Common symptoms, such as swelling, pain, tingling, and functional limitations, can severely restrict daily activities and independence [4, 5].
Several outcome measures have been developed to assess upper limb function and evaluate the impact of therapeutic interventions [6, 7]. The upper limb functional index (ULFI) is a widely used instrument designed to assess functional limitations in individuals with upper limb disorders [8]. This self-reported questionnaire not only quantifies patients’ ability to engage in daily and social activities but also serves as a valuable tool for clinicians and therapists to measure treatment effectiveness and track patient recovery [9].
Originally developed by Gabel et al. in 2006, the ULFI was designed to provide a precise and comprehensive assessment of upper limb function. Its brevity and ease of scoring make it particularly accessible to individuals with varying literacy levels. In 2010, Gabel et al. further refined the instrument by introducing an intermediate response option to enhance its sensitivity and specificity, replacing the conventional binary (yes/no) response format [10, 11].
Translation and cultural adaptation of validated instruments are essential in healthcare research and clinical practice. Such adaptations ensure that assessment tools maintain their reliability and validity across diverse populations, thereby facilitating accurate diagnosis, treatment planning, and international comparability of findings [12]. Developing a culturally adapted and psychometrically validated Persian version of the ULFI could significantly enhance the evaluation of upper limb function in the Iranian population and improve rehabilitation outcomes, particularly for individuals with musculoskeletal conditions.
The ULFI has been successfully adapted into several languages, including Spanish [13], Turkish [14], French-Canadian [15], Brazilian Portuguese [16], German [17], Arabic [18], Urdu [19], and Greek [20].
Given the absence of a Persian-adapted ULFI, this study aimed to address this gap by translating, adapting, and validating the questionnaire for use in Iranian patients. Establishing a culturally relevant tool will contribute to more precise functional assessments and enhance the quality of care for individuals with upper limb disorders in Iran.
Materials and Methods
Study design
This cross-sectional study aimed to translate, culturally adapt, and validate the Persian version of the ULFI for use in Iranian patients with upper limb musculoskeletal disorders. The adaptation process followed internationally recognized guidelines for cross-cultural validation of self-report instruments, incorporating translation, back-translation, expert review, and pilot testing [21]. The study was conducted in two phases. Translation and cultural adaptation to ensure linguistic and conceptual equivalence. Psychometric validation includes assessments of reliability, validity, and responsiveness. Additionally, confirmatory factor analysis (CFA) was conducted to validate the factorial structure of the Persian version of the ULFI.
Participants
A total of 200 Iranian outpatients and rehabilitation patients diagnosed with upper limb musculoskeletal disorders were recruited. The inclusion criteria included age ≥18 years, clinically diagnosed upper limb musculoskeletal disorders (e.g. rotator cuff injuries, carpal tunnel syndrome, and tendinitis), the ability to read and write in Persian, and willingness to provide informed consent.
The exclusion criteria included cognitive impairments that could hinder comprehension of the questionnaire, the presence of major systemic diseases that could confound results, and recent upper limb surgery, which could introduce variability in functional assessment.
Translation and cultural adaptation
The translation and cultural adaptation process adhered to the guidelines proposed by Beaton et al. [21] for cross-cultural adaptation of self-report measures. The process consisted of the following steps:
Forward translation: Two bilingual health science professionals independently translated the original English version of the ULFI into Persian. The two translations were compared, and discrepancies were resolved to create a single, harmonized Persian version.
Backward translation: Two additional bilingual translators, blinded to the original ULFI, independently back-translated the Persian version into English. This step ensured conceptual equivalence, rather than literal translation.
Expert panel review: A panel comprising physiotherapists, occupational therapists, and linguists reviewed the translated version to assess clarity, cultural relevance, and conceptual accuracy. Discrepancies were resolved through discussion, and a pre-final version was created.
Pilot testing: The pre-final version was administered to 20 patients with upper limb disorders to evaluate comprehension, ease of use, and potential difficulties. Feedback was incorporated, leading to the development of the final Persian version of the ULFI.
Measurements
ULFI
The ULFI is a 10-item patient-reported questionnaire assessing upper limb function in individuals with musculoskeletal disorders. Each item is scored on a 3-point Likert scale: 0) No difficulty, 1) Some difficulty, and 2) Unable to perform the activity. The total ULFI score ranges from 0 to 20, with higher scores indicating greater impairment.
Disabilities of the arm, shoulder, and hand (DASH) questionnaire
To assess convergent validity, the Persian version of the DASH questionnaire was used as a reference. The DASH is a 30-item instrument that evaluates physical function, symptoms, and social participation in patients with upper limb disorders. Scores range from 0 to 100, with higher scores indicating a greater degree of disability. The Persian DASH has been previously validated and has strong psychometric properties in Iranian populations [22].
Psychometric validation
Reliability
Internal consistency: Assessed using Cronbach’s α, with values ≥0.7 considered acceptable for reliability.
Test, re-test reliability: Evaluated by administering the Persian ULFI to 30 participants twice, 7 days apart. The intraclass correlation coefficient (ICC) was calculated, with values ≥0.75 indicating good reliability.
Validity
Construct validity: Assessed via convergent validity, by examining correlations between the Persian ULFI and DASH scores. Pearson’s correlation coefficient (r) was calculated, with values ≥0.50 considered acceptable for convergent validity.
CFA: A one-factor model was tested using AMOS (version 24). Model fit was evaluated using the following goodness-of-fit indices: chi-square/df ratio (χ²/df), comparative fit index (CFI), Tucker-Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Additionally, standardized factor loadings were examined for each item.
Responsiveness
The sensitivity of the Persian ULFI to detect functional changes over time was evaluated by administering the questionnaire to 50 patients before and after a 4-week rehabilitation program. Two measures of responsiveness were calculated, effect size (ES) and standardized response mean (SRM).
Statistical analysis
All statistical analyses were performed using SPSS software, version 26 and AMOS software, version 24.
Descriptive statistics were used to summarize the participants’ characteristics. Cronbach’s α, ICC, and Pearson’s correlation coefficient (r) were calculated to assess reliability and validity. CFA was conducted to validate the factor structure of the Persian ULFI. Statistical significance was set at P<0.05.
Results
A total of 200 participants diagnosed with upper limb musculoskeletal disorders were enrolled in the study. The mean age of the participants was 45.3±12.7 years, with 58% of the subjects being female and 42% male. The most prevalent diagnoses included rotator cuff injuries (32%), carpal tunnel syndrome (28%), and tendonitis (22%). Additionally, a majority of participants (76%) reported chronic symptoms persisting for more than six months. Table 1 presents the detailed demographic and clinical characteristics.
Reliability
The Persian ULFI demonstrated excellent internal consistency, with Cronbach’s α=0.91, indicating high reliability. Test, re-test reliability, assessed using the ICC, yielded a value of 0.88 (95% CI, 0.82%, 0.93%), suggesting strong temporal stability of the questionnaire (Table 2).
Validity
The Persian ULFI exhibited strong convergent validity compared with the DASH questionnaire. Pearson’s correlation coefficient (r) was 0.76 (P<0.001), confirming that the Persian ULFI aligns well with the established measure of upper limb function (Table 3).
Responsiveness
The responsiveness of the Persian ULFI was evaluated by measuring changes in scores following a 4-week rehabilitation program. A statistically significant improvement was observed (P<0.001), with the mean ULFI scores being 42.3±10.5 (pre-intervention) to 29.8±8.7 (post-intervention). The ES was 0.89, and the SRM was 1.12, indicating a strong ability to detect functional improvements over time (Table 4).
Factor structure and CFA
CFA supported the one-factor model of the Persian ULFI, demonstrating good model fit with the following fit indices:
Chi-square/df=2.15; CFI=0.96; TLI=0.95; RMSEA=0.06; SRMR=0.04.
These results confirm that the Persian ULFI has a strong factorial structure (Table 5).
Furthermore, all items loaded significantly onto a single latent factor, with standardized factor loadings ranging from 0.65 to 0.88, indicating robust construct validity (Table 6).
Discussion
The validation of the Persian version of the ULFI represents a significant advancement in assessing upper limb function in Iranian individuals with musculoskeletal disorders. Our findings confirm that the Persian ULFI is a reliable, valid, and responsive instrument, comparable to the original English version and other culturally adapted translations. Below, we discuss the key findings in the broader context of existing literature and highlight their research and clinical implications.
The rigorous translation and cultural adaptation process ensured that the Persian ULFI maintained conceptual equivalence with the original English version while being linguistically and culturally appropriate for Iranian patients. The high content validity index underscores the strong consensus among experts regarding the clarity, relevance, and comprehensibility of translated items. This aligns with previous adaptations of the ULFI, such as those in Spanish [13] and Turkish [14], where cultural relevance was emphasized to enhance measurement accuracy across diverse populations. The successful adaptation of the ULFI into Persian highlights the importance of culturally sensitive modifications when implementing health assessment instruments internationally.
The Persian ULFI demonstrated excellent internal consistency, with a Cronbach’s α of 0.91, which is comparable to the original English version [10] and other validated translations [9, 17]. These results indicate that the items in the questionnaire are highly interrelated, effectively measuring upper limb function as a single construct. Moreover, test re-test reliability confirmed the stability of the Persian ULFI over time, making it a reliable tool for longitudinal assessment. These findings are consistent with prior research, further reinforcing the robust psychometric properties of the ULFI across different cultural contexts [10, 13, 14].
The strong correlation between the Persian ULFI and DASH questionnaires provides compelling evidence for the construct validity of the instrument. This correlation is consistent with previous findings where the ULFI exhibited moderate to strong associations with other upper limb function measures, supporting its clinical relevance and convergent validity [14, 16, 19].
CFA further validated the one-factor structure of the Persian ULFI, with excellent model-fit indices. These results support the unidimensional nature of the ULFI, confirming that it effectively captures the overall impact of musculoskeletal disorders on upper limb function without requiring subscales. Moreover, the high standardized factor loadings further substantiate the sufficiency of the single-factor model, a finding that aligns with previous language adaptations [13, 14, 16].
The Persian ULFI exhibited high responsiveness, as evidenced by significant score reductions after a 4-week rehabilitation program. The mean ULFI score decreased from 42.3±10.5 (pre-intervention) to 29.8±8.7 (post-intervention), with an ES of 0.89 and SRM of 1.12. These findings confirm the sensitivity of the Persian ULFI in detecting meaningful functional improvements over time, making it an effective outcome measure for evaluating rehabilitation. Comparable responsiveness has been reported in previous studies, in which the ULFI effectively captured changes in upper limb function across different patient populations, including those with acute and chronic musculoskeletal conditions [14, 17].
The responsiveness of the Persian ULFI demonstrated strong sensitivity to functional changes, with an SRM of 1.12, which is quantitatively comparable to other validated versions. For example, the Turkish adaptation reported an SRM of 1.10 [14], while the Arabic version showed an SRM of 1.05 [9]. These similarities highlight the Persian ULFI’s robust ability to detect clinical improvements, aligning with findings from other cultural contexts.
The successful validation of the Persian ULFI has significant implications for clinical and research applications in Iran. In clinical practice, healthcare professionals can utilize the Persian ULFI to assess the functional impact of musculoskeletal disorders on patients’ daily activities, monitor rehabilitation progress over time, and evaluate the effectiveness of therapeutic interventions in improving upper limb function.
From a research perspective, the Persian ULFI provides a standardized tool for investigating upper limb disorders in Iranian populations, facilitating comparisons with international studies and contributing to the global body of knowledge in musculoskeletal health. By establishing psychometric equivalence across languages, the Persian ULFI allows for multinational collaboration and cross-cultural research on upper limb function.
While the ULFI is a patient-reported outcome measure (PROM), performance-based tools (grip strength tests, range of motion assessments) provide objective data on physical function [6, 7]. The ULFI complements these measures by capturing patients’ perceived limitations in daily activities, which may not always correlate directly with physical performance. For instance, a patient with adequate grip strength might still report functional difficulties due to pain or fatigue. Integrating both PROMs, such as the ULFI, and performance-based measures offers a comprehensive evaluation of upper limb function, addressing both subjective experiences and objective capabilities.
While this study provides strong evidence for the validity and reliability of the Persian ULFI, certain limitations should be acknowledged. Participants were recruited from outpatient clinics and rehabilitation centers, which may limit the applicability of findings to other populations, such as primary care patients or community-based cohorts.
The study evaluated responsiveness in a relatively small sample (n=50) undergoing a 4-week rehabilitation program. Future studies should examine responsiveness in larger, more diverse patient populations, including those with varying upper limb disorders and treatment durations.
Further research is warranted to explore the use of the Persian ULFI in specific patient subgroups, such as those with traumatic injuries, neurological conditions, or occupational musculoskeletal disorders. Additionally, longitudinal studies could assess whether the Persian ULFI can predict long-term functional outcomes, such as return to work, improvements in quality of life, and sustained rehabilitation effects. Expanding validation efforts to include larger, more diverse samples would further strengthen the generalizability and clinical utility of the instrument.
Conclusion
The Persian ULFI demonstrated strong psychometric properties, including high internal consistency, test re-test reliability, convergent validity with the DASH, and responsiveness, which are comparable to those of other adaptations. Its unidimensional structure supports its use for assessing upper limb function in Iranian clinical and research settings. Similar to other PROMs, the ULFI complements performance-based measures by capturing patient-reported limitations and enriching functional evaluations. This adaptation expands culturally validated tools for musculoskeletal rehabilitation.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1399.801). Written informed consent was obtained from all participants before enrollment. The confidentiality of the participants’ data was strictly maintained throughout the study.
Funding
This research was supported by a research project funded by Mazandaran University of Medical Sciences, Sari, Iran.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all respondents who participated in this study.
References
- Collis JM, Signal N, Mayland E, Wright-St Clair VA. Influence of purposeful activities on upper extremity motor performance: A systematic review. OTJR: Occupation, Participation and Health. 2020; 40(4):223-34. [DOI:10.1177/1539449220912187]
- Romero-Morales C, López-López D, Almazán-Polo J, Mogedano-Cruz S, Sosa-Reina MD, García-Pérez-de-Sevilla G, et al. Prevalence, diagnosis and management of musculoskeletal disorders in elite athletes: A mini-review. Disease-a-Month. 2024; 70(1):101629. [DOI:10.1016/j.disamonth.2023.101629] [PMID]
- Şahinoğlu E, Ünver B, Yamak K. The relationship of range of motion and muscle strength to patients' perspectives in pain, disability, and health-related quality of life in patients with rotator cuff disease. Irish Journal of Medical Science. 2021; 190(1):177-83. [DOI:10.1007/s11845-020-02305-4] [PMID]
- Horsten NC, Ursum J, Roorda LD, van Schaardenburg D, Dekker J, Hoeksma AF. Prevalence of hand symptoms, impairments and activity limitations in rheumatoid arthritis in relation to disease duration. Journal of Rehabilitation Medicine. 2010; 42(10):916-21. [DOI:10.2340/16501977-0619] [PMID]
- Currie KB, Tadisina KK, Mackinnon SE. Common hand conditions: A review. JAMA. 2022; 327(24):2434-45. [DOI:10.1001/jama.2022.8481] [PMID]
- Wang S, Hsu CJ, Trent L, Ryan T, Kearns NT, Civillico EF, et al. Evaluation of performance-based outcome measures for the upper limb: A comprehensive narrative review. PM & R: The Journal of Injury, Function, and Rehabilitation. 2018; 10(9):951-962.e3. [DOI:10.1016/j.pmrj.2018.02.008] [PMID]
- Prange-Lasonder GB, Alt Murphy M, Lamers I, Hughes AM, Buurke JH, Feys P, et al. European evidence-based recommendations for clinical assessment of upper limb in neurorehabilitation (CAULIN): Data synthesis from systematic reviews, clinical practice guidelines and expert consensus. Journal of Neuroengineering and Rehabilitation. 2021; 18(1):162. [DOI:10.1186/s12984-021-00951-y] [PMID]
- Jame Bozorgi AA, Mahmodian F. [Instruments for measuring the upper limb function in musculoskeletal disorders: A review study (Persian)]. The Scientific Journal of Rehabilitation Medicine. 2024; 13(5):868-77. [DOI:10.32598/SJRM.13.5.1136]
- Albahrani YA, Alshami AM. Construct validity, test re-test reliability, and responsiveness of the Arabic version of the upper limb functional index. BMC Musculoskeletal Disorders. 2023; 24(1):855. [DOI:10.1186/s12891-023-06969-8]
- Gabel CP, Michener LA, Burkett B, Neller A. The upper limb functional index: Development and determination of reliability, validity, and responsiveness. Journal of Hand Therapy. 2006; 19(3):328-48; quiz 49. [DOI:10.1197/j.jht.2006.04.001] [PMID]
- Hefford C, Abbott JH, Arnold R, Baxter GD. The patient-specific functional scale: Validity, reliability, and responsiveness in patients with upper extremity musculoskeletal problems. The Journal of Orthopaedic and Sports Physical therapy. 2012; 42(2):56-65. [DOI:10.2519/jospt.2012.3953] [PMID]
- Al Maskari TS, Melville CA, Willis DS. Systematic review: Cultural adaptation and feasibility of screening for autism in non-English speaking countries. International Journal of Mental Health Systems. 2018; 12:22. [DOI:10.1186/s13033-018-0200-8] [PMID]
- Cuesta-Vargas AI, Gabel PC. Cross-cultural adaptation, reliability and validity of the Spanish version of the upper limb functional index. Health and Quality of Life Outcomes. 2013; 11(126):1-8. [DOI:10.1186/1477-7525-11-126]
- Tonga E, Durutürk N, Gabel PC, Tekindal A. Cross-cultural adaptation, reliability and validity of the Turkish version of the upper limb functional index (ULFI). Journal of Hand Therapy. 2015; 28(3):279-85. [DOI:10.1016/j.jht.2014.11.001]
- Hamasaki T, Demers L, Filiatrault J, Aubin G. A cross-cultural adaptation of the upper limb functional index in French Canadian. Journal of Hand Therapy. 2014; 27(3):247-52; quiz 253. [DOI:10.1016/j.jht.2013.12.005] [PMID]
- Takahasi HY, Fidelis-de-Paula-Gomes CA, Gabel CP, Dibai-Filho AV. Translation, cross-cultural adaptation and validation of the upper limb functional index (ULFI) into Brazilian Portuguese in patients with chronic upper limb musculoskeletal disorders. Musculoskeletal Science and Practice. 2021; 56:102452. [DOI:10.1016/j.msksp.2021.102452]
- Ortega-Castillo M, Cuesta-Vargas A, Melloh M, Trinidad-Fernández M. Cross-cultural adaptation and validation of the German version of the upper limb functional index. Journal of Sport Rehabilitation. 2024; 33(8):630-8. [DOI:10.1123/jsr.2023-0342] [PMID]
- Albahrani YA, Alshami AM. Cross-cultural adaptation of the upper limb functional index in Arabic. Acta Bio-Medica: Atenei Parmensis. 2022; 93(5):e2022307. [PMID]
- Arooj A, Amjad F, Tanveer F, Arslan AU, Ahmad A, Gilani SA. Translation, cross-cultural adaptation and psychometric properties of Urdu version of upper limb functional index; a validity and reliability study. BMC Musculoskeletal Disorders. 2022; 23(1):691. [DOI:10.1186/s12891-022-05628-8] [PMID]
- Chamogeorgakis G, Karanasios S, Theotokatos G, Vasilogeorgis I, Korakakis V. Cross-cultural adaptation and measurement properties of the upper limb functional index (ULFI) for Greek-Speaking Patients. Cureus. 2023; 15(6):e40029. [DOI:10.7759/cureus.40029] [PMID]
- Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000; 25(24):3186-91. [DOI:10.1097/00007632-200012150-00014] [PMID]
- Mousavi SJ, Parnianpour M, Abedi M, Askary-Ashtiani A, Karimi A, Khorsandi A, et al. Cultural adaptation and validation of the Persian version of the disabilities of the arm, shoulder and hand (DASH) outcome measure. Clinical Rehabilitation. 2008; 22(8):749-57. [DOI:10.1177/0269215508085821] [PMID]
Article type: Original Research Articles |
Subject:
Occupational therapy
Received: 2025/05/23 | Accepted: 2025/05/26 | Published: 2025/09/1
Received: 2025/05/23 | Accepted: 2025/05/26 | Published: 2025/09/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
