
988368
Thu, Jul 30, 2026

Volume 23, Issue 4 (December 2025)
Iranian Rehabilitation Journal 2025, 23(4): 407-418 |
Back to browse issues page


Ethics code: IR.BASU.REC.1401.026
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ashoury H, Yalfani A, Azizian M. Aquatic and Kinetic Chain Exercises for Rehabilitation of Chronic Non-specific Low Back Pain. Iranian Rehabilitation Journal 2025; 23 (4) :407-418
URL: http://irj.uswr.ac.ir/article-1-2563-en.html
URL: http://irj.uswr.ac.ir/article-1-2563-en.html



1- Department of Physical Education and Sport Sciences, Payame Noor University, Tehran, Iran.
2- Department of Exercise Rehabilitation, Faculty of Sport Sciences, Bu-Ali Sina University, Hamadan, Iran.
2- Department of Exercise Rehabilitation, Faculty of Sport Sciences, Bu-Ali Sina University, Hamadan, Iran.
Full-Text [PDF 694 kb]
(1240 Downloads)
| Abstract (HTML) (1776 Views)
Full-Text: (332 Views)
Introduction
Low back pain (LBP) is a critical global public health issue with a negative impact on quality of life (QoL) and a remarkable social and economic burden [1]. Epidemiological research has revealed that LBP affects 43%-83% of individuals across various societies [2, 3]. Approximately 70%-85% of individuals experience LBP in their lifetime [2, 3]. LBP is one of the primary causes of disability, healthcare utilization, and work absenteeism worldwide [2]. This problem has been reported to be the second most common reason for medical visits, the third most common reason for surgeries, and the fifth most common reason for hospitalization [3]. According to the World Health Organization (WHO) statement, LBP is one of the top ten high-impact conditions and can be experienced during daily life activities, with negative impacts on health, QoL, and daily activities [4].
Studies indicate that a precise pathoanatomical diagnosis is only attainable in 8-15% of individuals with lower back pain. Consequently, most LBP cases are designated as chronic nonspecific lower back pain (CNSLBP), a classification denoting pain that persists for three months or more [5]. The main complaint of patients with CNSLBP when they visit a physician is movement restriction in the lumbar spine, which often contributes to discomfort and functional impairment. This exacerbates patients’ daily activities and QoL [6]. Reduced ROM in the lumbar region is often observed in individuals experiencing chronic LBP [7]. Previous studies have highlighted the importance of improving ROM in chronic LBP patients to enhance their physical capabilities and alleviate pain symptoms [8, 9]. Interventions targeting flexibility and ROM in the lumbar region significantly manage chronic LBP and improve overall functionality and well-being [10]. Limited ROM in patients with LBP changes the muscle sensitivity to tension, followed by pain sensation, which does not allow the muscles to reach their full ROM [11]. This changes the movement pattern and contraction of back muscles, which are the primary stabilizers of this region [12], thus leading to muscle imbalance and negatively affecting lumbopelvic stability [13].
Aquatic exercise (AE) is a valuable intervention for psychological problems (e.g. depression, stress, and anxiety) [14], and promotes overall well-being [15]. Immersing and performing physical exercises in water can improve mood, generate relaxation responses, improve well-being, and offer an opportunity to attend to the emotional aspects of rehabilitation [15]. The properties of water, such as buoyancy and support, can alleviate anxiety and promote a relaxed mental state [16].
Open-chain AEs (OCAEs) and closed-chain AEs (CCAEs) have gained remarkable attention as valuable and efficient rehabilitation techniques [17]. Closed kinetic chain (CKC) happens when the foot supports weight on the ground, stabilizing the lower limb’s distal segment [18]. Conversely, an open kinetic chain (OKC) occurs when the distal section is movable [18]. OCAE and CCAE have both benefits and drawbacks in rehabilitation [18], and the decision to select between them depends on the treatment goals [19]. The CCAE offers advantages, such as heightened joint compressive forces, enhanced joint stability, lower shear forces, diminished acceleration forces, greater resistance, better proprioception, and superior dynamic stability [19]. Conversely, the benefits of OCAE include higher rotational and distraction forces, lower resistance forces, increased acceleration forces, enhanced joint and muscle mechanoreceptor deformation, enhanced concentric acceleration and eccentric deceleration forces, and increased backing for functional tasks [19]. A major benefit of AE for rehabilitation is the capacity to start treatments sooner than on land [14]. Earlier AE for chronic LBP patients can be helpful as buoyancy decreases pressure on the spinal column and hydrostatic pressure together with water temperature, improves balance, reduces pain, and prevents muscle atrophy [20]. AE is crucial for enhancing the QoL of individuals with LBP. They can be essential in comprehensive therapeutic programs for individuals [21]. It remains unclear how OKC and CKC exercises can be combined in rehabilitation programs for chronic LBP. Most studies have investigated the effects of performing these exercises on land, while few studies have been conducted for closed- and open-chain exercises in water [22]. Consequently, musculoskeletal and central nervous system (CNS) involvement should be considered when creating treatment plans. Considering this, a randomized controlled trial (RCT) was conducted to examine the possible advantages of incorporating aquatic therapy into the open and closed chain exercises within a comprehensive rehabilitation protocol for individuals with LBP. AE is recognized for its advantages in LBP; the question is whether balance and ROM change after AE. Therefore, this study aimed to investigate the effects of OCAE and CCAE on dynamic balance, ROM, and self-reported pain in male patients with CNSLBP.
Materials and Methods
Study design
This was a three-arm, double-blind RCT (blinding of evaluators and patients). To prevent patient bias, the participants in each group were also unaware of the other group’s existence and the results of their tests until after the post-test stage. The trial adhered to the CONSORT 2010 guidelines to ensure methodological rigor and transparency [23].
Participants
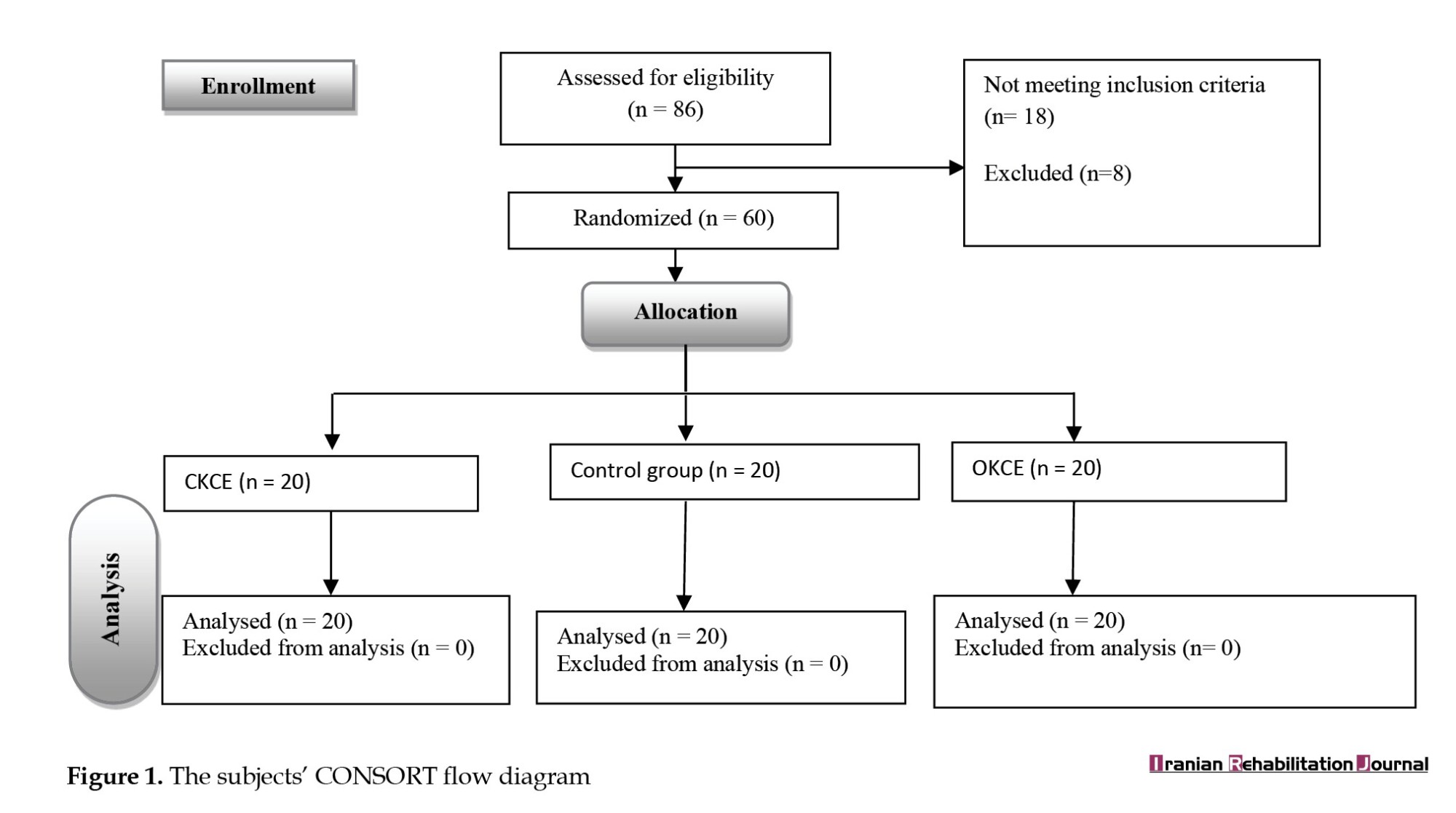
Participants in this study were men aged 40-60 years who had been diagnosed with CNSLBP by a spine specialist, they freely participated in the trial. They were assigned at random using sequentially numbered opaque sealed envelopes to hide their allocation, divided into three groups using software that generates random numbers: OCAE (n=20), CCAE (n=20), and a control group (n=20). In this random allocation method, based on the sample size, each of the randomly produced sequences was recorded on a card, which was then put into one of the prepared envelopes. Finally, after the evaluation, each patient opened one of the envelopes to specify their group. The minimum sample size was calculated utilizing G*Power software, version 3.1.9.2 (effect size=0.8, α=0.05, and power of the test=0.95) for multivariate analysis of variance, one-way analysis of variance (ANOVA) test, and and analysis of covariance (ANCOVA) (demographic information). The study included 86 men with LBP, of whom 18 were eliminated because they did not meet the inclusion criteria. Additionally, eight participants did not adhere to the rehabilitation process. Finally, based on the inclusion and exclusion criteria, 60 participants were chosen to make up the statistical sample. Ultimately, there were 20 patients with CNSLBP in the OCAE group, 20 in the CCAE group, and 20 in the control group (Figure 1). All patients had CNSLBP, which was confirmed by a neurosurgeon. The inclusion criteria included being aged 40-60, having a history of pain for over 12 weeks, and having no history of spinal surgery or hip replacement. The exclusion criteria included pain in other body parts, involvement in therapeutic activities, sciatic pain, lower and upper limb deformities, physiotherapy use throughout the past 12 months, and spondylolysis and respiratory problems [24]. The experimental groups performed CKCE and OKCE for eight weeks, three sessions per week, while the control group received no intervention. Patients were instructed not to inform the evaluators about their group assignments to preserve blinding. The participants were provided with an explanation of the processes and goals. Under the Declaration of Helsinki, all participants and/or their legal guardians provided informed consent before participating in the study and, when appropriate, before information or photos were published in an online open-access publication [25]. Ethical approval was obtained from the Ethics Committee o Bu-Ali Sina University for this study. The study was registered at the Iranian Registry of Clinical Trials (IRCT).
Experimental intervention
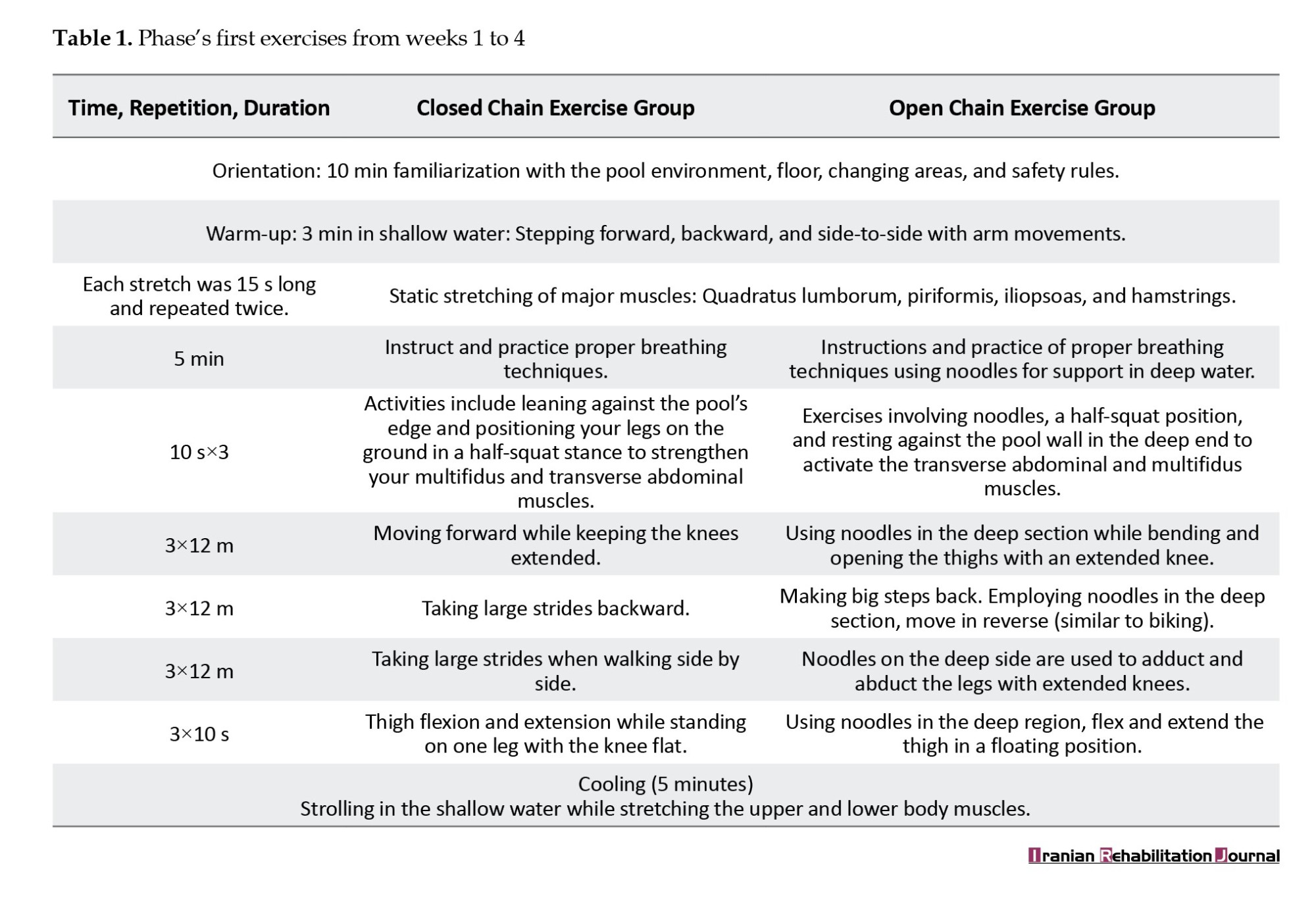
After evaluating the listed variables, exercises were performed for eight weeks in two stages. The first stage (first four weeks) aimed to familiarize participants with water, examine breathing patterns, train and perform breathing correctly, use swimming in a pool to strengthen the transverse abdominal muscles and multifidus, and maintain proper posture and breathing throughout daily activities (Table 1).
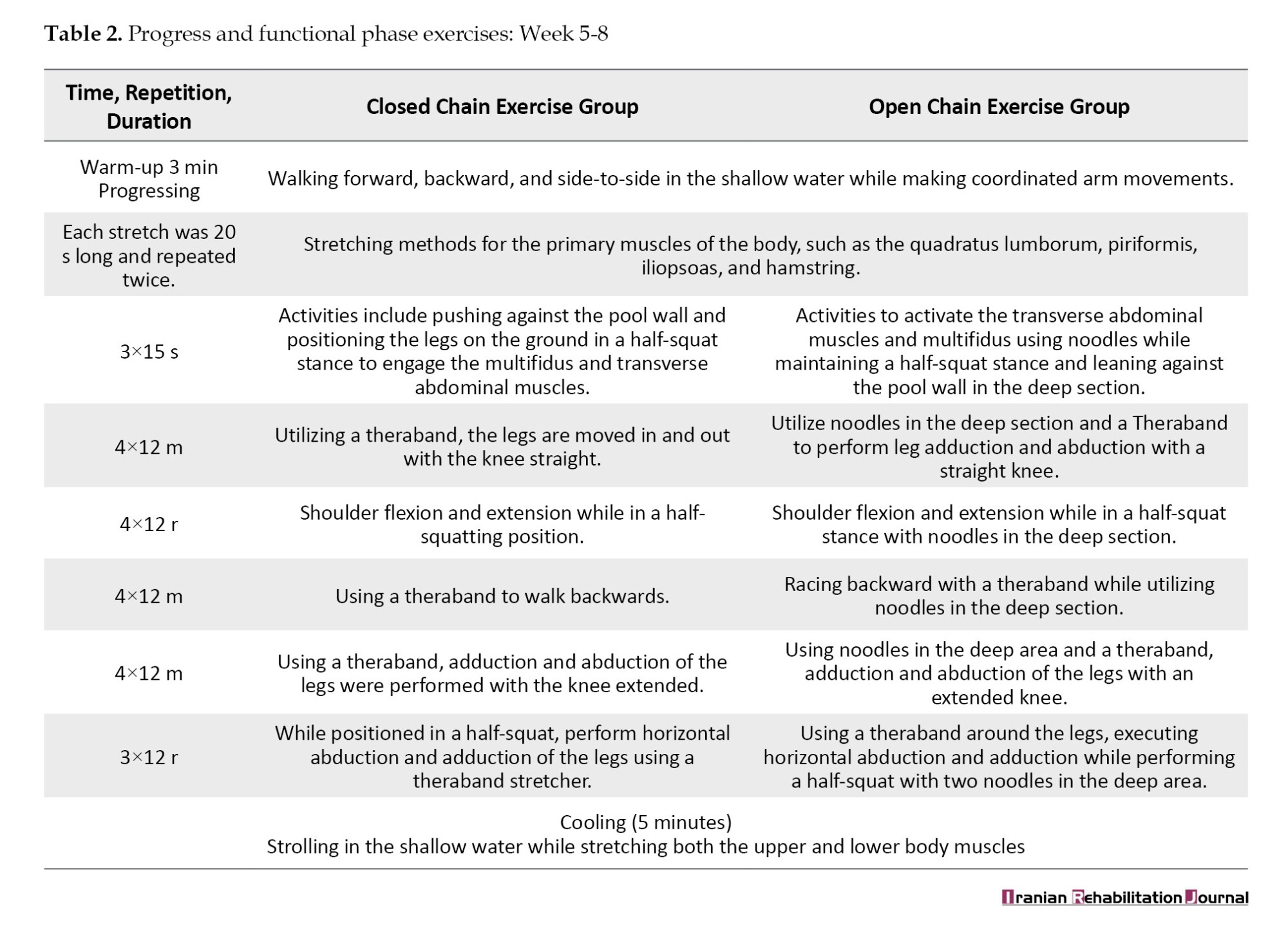
The second stage (last four weeks) comprised functional progress and aimed to enhance endurance and muscle strength by incorporating a resistance threshold into the exercises (Table 2). A hydrotherapy specialist and researcher supervised all exercise sessions conducted three times a week. Each session lasted approximately 60 minutes., starting with five minutes of general warm-up followed by 50 minutes of core workouts. OCAE group exercises, such as the abdominal drawing-in maneuver, are specifically intended to activate the deep core stabilizers, the transverse abdominis and multifidus muscles. In the deep water, the following exercises were performed using pool noodles (for support) and theraband (for resistance): Leg abduction and adduction, which involve moving the legs apart and together with the knees extended; and hip flexion and extension, which consist of bending and straightening the thigh at the hip while in a floating position. The CCAE group was trained in proper breathing techniques and performed core-stabilizing exercises. These included a supported half-squat against the pool wall with feet on the floor to target the transverse abdominis and multifidus muscles. The program included various walking drills: Forward, backward, and sideways with long steps and extended knees, along with single-leg balance practice that involved moving the other leg forward and back, ending with five minutes of cooling (stretching exercises). The training regimen expanded in volume, intensity, duration, and repetition over successive weeks (Tables 1 and 2). The CCAE group exercised in shallow water, while the OCAE group used noodles in deep water (supervised by a lifeguard) (depth to chest area). The protocols for both groups were performed by a skilled physiotherapist specializing in hydrotherapy [6, 19, 26].
Range of motion (ROM)
This study assessed the ROM of the lumbar region through left and right lateral trunk flexion. During the test, the individual stands comfortably and bends to the left or right by lowering their hand along the side of the leg, and the distance from the middle fingertip to the ground was measured (Figure 1). The validity and reliability were found to be high for left and right lateral flexion (intraclass correlation [ICC]: 0.985; 95% CI, 0.969%, 0.993%) [27].
Y-dynamic balance
The Y test is a reliable method for evaluating dynamic balance. It has been reported that this test’s reliability coefficient is (0.91-0.99). In this test, the subject stands with the dominant leg in the middle (Y angle between the arms: 135°, 90°, and 135°). The participant is instructed to reach with the opposite foot’s toes in three directions (anterior, posterolateral, and posteromedial) while maintaining balance on one leg. The participant was kept balanced, the supporting foot’s heel was kept from lifting off the ground, the reaching toes made slight contact with the ground without bearing weight, and the foot was brought back to its standing posture without making contact. They did not implement these cases; it was considered an error, and the test was repeated after a two-minute rest. Balance scores were normalized based on leg length (the separation between the medial malleolus and the anterior superior iliac spine when supine), and the final test score was the average of three repetitions [14, 28].
Pain
A visual analog scale (VAS) measuring 10 centimeters was used to quantify pain perception. Participants were asked to indicate their pain level by marking a scale within this range. Pain intensity was measured on a scale of 0 (no pain) to 10 (worst pain) [29, 30].
Statistical analysis
Data pertaining to all three groups were collected in the pre-test, post-test, and statistical analysis was then carried out to examine how CKCE and OKCE affected study indicators. The Shapiro-Wilk test was used to assess the η2 normal distribution of data related to variables and demographic characteristics, and the Levene test was used to assess the homogeneity of variances. Analysis of variance (ANOVA) was used to compare the pre-test values of groups, the t-dependent test to examine intra-group differences, and the ANCOVA method was used to compare the post-test values between groups with effect size analysis. Data were analyzed using SPSS software, version 26. The significance level was set at 0.05 (P<0.05). The effect of the interventions was considered using eta coefficients (η2): Low (0.01), medium (0.06), and large (0.14).
Results
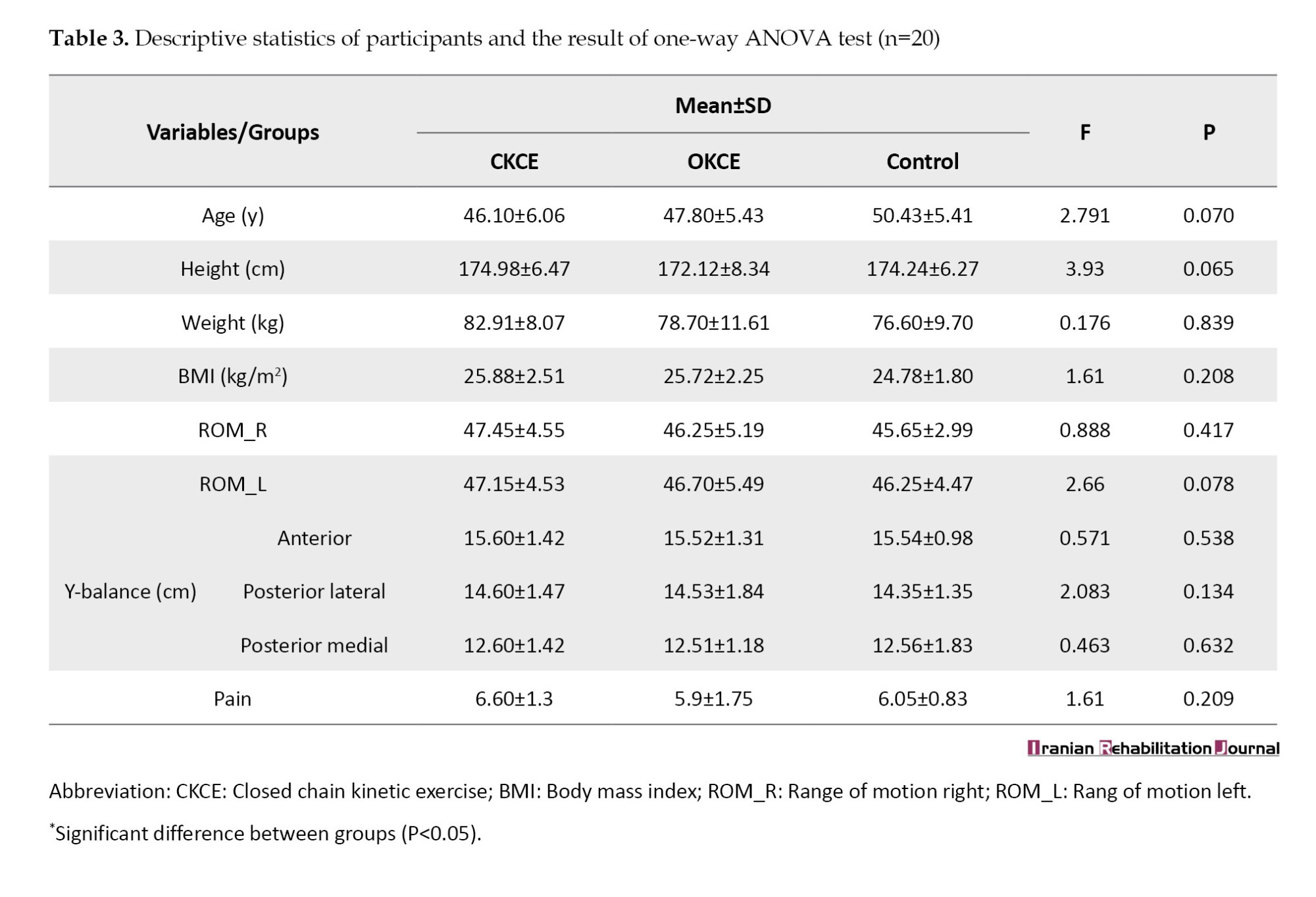
Demographic characteristics, such as age, height, weight, and body mass index (BMI), were reported as Mean±SD (P>0.05) (Table 3). At baseline, no statistically significant differences were observed between the groups regarding demographic characteristics (age, weight, height, BMI) or outcome measures (ROM, dynamic balance, and pain), (P>0.05 for all) (Table 3).
Pain
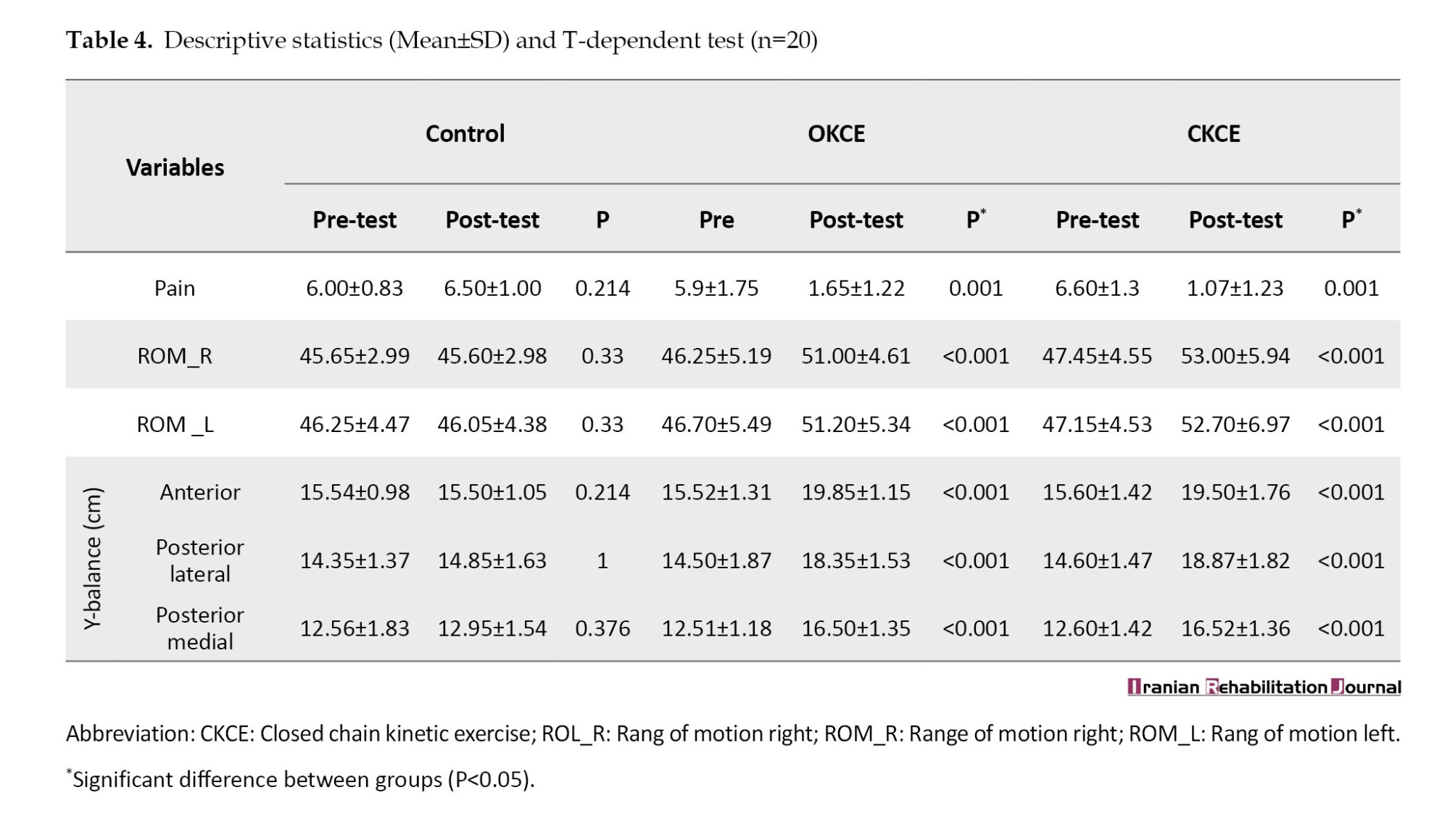
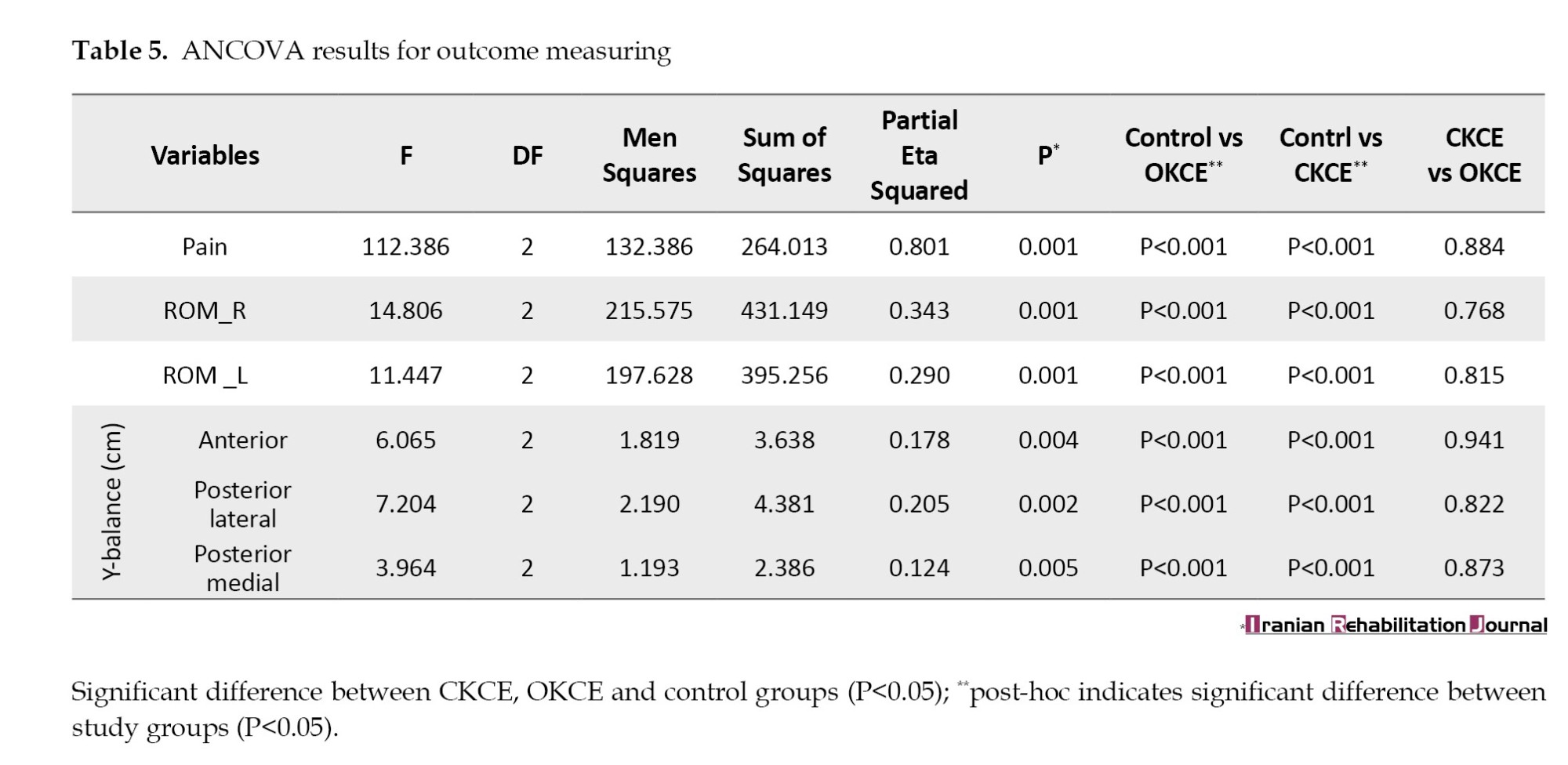
The statistical analysis results using paired t-tests showed a significant difference in pain levels between the participants in the CCAE and OKCE test groups (P<0.05). This suggests that CCAE and OCAE may be more effective in alleviating pain in individuals with CNSLBP. No significant difference was observed in scores in the control group between the pre-and post-tests (P>0.05) (Table 4). Additionally, ANCOVA revealed a substantial effect size with a significant difference in pain levels among the groups (F2=112.386, P=0.001, η2=0.801). This finding supports the efficacy of exercise interventions in reducing pain and highlights the potential for implementing CCAE and OCAE as a therapeutic approach for patients with CNSLBP.
ROM
The results of the statistical analysis using paired t-tests showed a significant difference in right and left ROM before and after the intervention in the CKCE and OKCE test groups (P<0.05). This indicates that both exercise modalities effectively enhance mobility among individuals with CNSLBP. No significant difference was observed in scores in the control between the pre- and post-tests (P>0.05) (Table 4). In addition, the ANCOVA test indicated a small effect size significant difference between CCAE and OCAE groups with the control group in left ROM (F2=11.447, P=0.001, η2=0.29), right ROM (F2=14.806, P=0.001, η2=0.343) (Table 5). These findings indicate a substantial effect of both exercise interventions on improving ROM. Post-hoc test for ANCOVA showed the difference between the control group and the CCAE and OCAE groups for right ROM (P<0.001 for both) and left ROM (P=0.001 and 0.002, respectively). Also, no significant difference was observed between the CCAE and OCAE groups. These results underscore the efficacy of incorporating both CCAE and OCAE into rehabilitation protocols for patients with CNSLBP, as they contribute to improved mobility and functional outcomes. Future studies should examine the causes and long-term impacts of these advancements.
Dynamic balance
The results of the statistical analysis using paired t-tests showed a significant difference in dynamic balance (anterior), dynamic balance (posterior-lateral), and dynamic balance (posterior-medial) between the participants in the CCAE and OCAE test groups (P<0.05). This indicates that both exercise modalities positively influence dynamic balance, a critical component in functional mobility for individuals with chronic CNSLBP. No significant difference was observed in scores in the control group between the pre- and post-tests (P>0.05) (Table 4). ANCOVA indicated a small effect size significant difference between CCAE and OCAE groups and control group for dynamic balance (anterior) (F2=6.065, P=0.004, η2=0.178), and dynamic balance (posterior-lateral) (F2=7.204, P=0.002, η2=0.204), dynamic balance (posterior-medial) (F2=3.964, P=0.005, η2=0.124) (Table 5). These results indicate that CKCE and OKCE significantly enhanced dynamic balance compared to no intervention, with the effect sizes suggesting a meaningful clinical impact. Post-hoc test for ANCOVA showed a difference between the control and CKCE and OKCE groups for dynamic balance (anterior) (P<0.004 for both), dynamic balance (posterior-lateral) (P<0.002 for both), and dynamic balance(posterior-medial) (P<0.004 for both). These findings underscore the importance of incorporating CCAE and OCAE into rehabilitation programs for patients with CNSLBP, as both interventions significantly enhance dynamic balance, which is crucial for preventing falls and improving functional mobility. Future studies should explore the long-term effects of these interventions and their implications for broader rehabilitation strategies.
Discussion
This RCT investigated the effects of AE combined with OKC and CKC exercises on dynamic balance, pain, and ROM in men with CNSLBP. This study aimed to investigate the effect of OCAE and CCAE on dynamic balance, ROM, and self-reported pain in men with CNSLBP. The findings demonstrated that dynamic balance was enhanced by both training program types in the anterior, posterior-lateral, and posterior-medial postural control indices. Additionally, no significant difference was observed in the effectiveness of OCAE and CCAE in posterolateral, posteromedial, pain, and ROM indices. Therefore, AE for eight weeks seems useful for reducing the pain of patients with CNSLBP. These results are consistent with those of Yalfani et al. (2020), Brech et al. (2012), Khodaveisi et al. (2008) and Aluko et al. (2013), who have shown the beneficial effects of rehabilitation exercises in lowering pain levels in patients with CNSLBP [27, 31-36].
Dynamic balance is essential for functional mobility and is often compromised in individuals with CNSLBP [34-36]. The enhancement in anterior balance indicates improved forward stability, which is crucial for activities, such as walking, running, and reaching [37, 38]. CCAE and OCAE improve balance through several mechanisms. Both modalities enhance proprioceptive feedback by activating sensory receptors that provide information about body position and movement, improving body awareness and spatial orientation [39, 40]. The CCAE emphasizes weight-bearing movements that engage stabilizing muscles, while the OCAE utilizes the buoyancy of water to promote muscle coactivation and coordination without impacting the joints [11, 41]. These exercises also enhance neuromuscular control through repetitive practice and reflexive responses to perturbations, while building muscle strength and endurance [42]. Additionally, a safe aquatic environment reduces the risk of injury, allowing individuals to practice dynamic movements that mimic daily activities, ultimately fostering better balance and functional mobility, especially in those with CNSLBP [6, 43].
The significant reduction in pain reported by participants in both exercise groups underscores the therapeutic potential of these interventions. The AE alleviates pain through the buoyancy effect, which reduces mechanical stress on the spine and surrounding musculature [24, 44]. Similarly, AE may enhance pain relief by promoting muscle strengthening and improving functional movement patterns, contributing to better spinal stability and reduced discomfort during daily activities [5]. AE, such as that performed in the OCAE and CCAE groups, has been shown to alleviate pain through several mechanisms. The buoyancy effect of water plays a crucial role in this process [11, 41, 45]. By reducing the gravitational load on the body, buoyancy minimizes mechanical stress on the spine and surrounding musculature [46, 47]. This allows individuals to engage in movements that might otherwise exacerbate pain on land [48, 49]. The hydrostatic pressure of water also promotes circulation, which can improve the way nutrients and oxygen reach tissues while making it easier to eliminate waste products from metabolism [11, 50, 51]. This improved circulation decrease inflammation and muscle soreness, reducing pain [48, 53]. In summary, the pain reduction observed in this study highlights the efficacy of both aquatic and CKC exercises as therapeutic interventions for individuals with CNSLBP. The unique properties of AE, combined with the strength-building focus of CCAE, create a comprehensive approach to pain management. Together, these modalities alleviate pain and empower individuals to regain control over their physical functions and improve their overall well-being.
The enhancement in trunk lateral flexion ROM was a pivotal finding of this study, as an increased ROM is critical for the execution of daily activities and preservation of overall functional independence. The buoyant properties of OCAE allow individuals to achieve a greater ROM without the gravitational constraints typically encountered on land [51, 53]. Studies have shown that AE can increase flexibility and improve overall physical function in CLBP patients [21, 24, 26, 54]. This unique environment facilitates stretching and mobility exercises that may be challenging for individuals with pain or stiffness, promoting greater flexibility and functional capacity [12, 55]. In contrast, the superior effectiveness of CCAE in improving ROM can be attributed to its targeted focus on strengthening the musculature involved in lateral flexion and spinal stabilization [25]. By enhancing both muscular strength and endurance, CCAE contributes to improved flexibility and mobility in the lumbar region, enabling participants to perform lateral movements with greater efficiency and reduced discomfort. Furthermore, the integration of both OCAE and CCAE within rehabilitation protocols is substantiated by neurophysiological evidence indicating that distinct sensory modalities elicit different neural processes [43]. This suggests that the synergistic combination of OCAE and CCAE may optimize neuromuscular adaptations, thus enhancing overall rehabilitation outcomes [39, 49, 56]. This dual approach is likely to improve proprioception, coordination, and muscle activation patterns, which are essential for effective balance and pain management [11, 57]. Consequently, this comprehensive methodology holds significant potential for improving functional performance and enhancing the QoL of individuals with CNSLBP. Furthermore, AE regulates neuromuscular postural control to a stable state, which is essential for improving muscle function. The exercises offered in this study seem to target neuromuscular issues related to CNSLBP, potentially resulting in enhanced ROM, pain relief, and dynamic balance. These findings have implications for health organizations to implement AE programs to improve mental health in patients with LBP.
Conclusion
This study showed that aquatic therapy positively affects dynamic balance, pain, ROM, and mental health in patients with CNSLBP. The primary objective of aquatic therapy is to instruct patients to utilize water as a supplementary treatment for recovering patients with LBP. Therefore, aquatic therapy can play a role in patient recovery. Healthcare professionals, including doctors, physiotherapists, and occupational therapists, can incorporate open and CKC exercises in water into a thorough therapeutic program for patients with LB.
Limitation
Our study has several limitations that should be acknowledged: the absence of female participants, the lack of long-term follow-up, potential selection bias, and the omission of a comparator group involving land-based exercises. Furthermore, the uncontrolled variables of participants’ age and BMI may influence the results and restrict how widely the results can be used.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Bu-Ali Sina University, Hamadan, Iran (Code: IR.BASU.REC.1401.026). The study was registered at the Iranian Registry of Clinical Trials (IRCT), Tehran, Iran (Code: IRCT20230430058033N1).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design, Hossein Ashoury; Drafting of article: Hossein Ashoury and Ali Yalfani; Critical revision: Hossein Ashoury and Masoud Azizian; monitoring progress: Ali Yalfani; Data analysis, interpretation and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all participants for their cooperation in the study.
References
Low back pain (LBP) is a critical global public health issue with a negative impact on quality of life (QoL) and a remarkable social and economic burden [1]. Epidemiological research has revealed that LBP affects 43%-83% of individuals across various societies [2, 3]. Approximately 70%-85% of individuals experience LBP in their lifetime [2, 3]. LBP is one of the primary causes of disability, healthcare utilization, and work absenteeism worldwide [2]. This problem has been reported to be the second most common reason for medical visits, the third most common reason for surgeries, and the fifth most common reason for hospitalization [3]. According to the World Health Organization (WHO) statement, LBP is one of the top ten high-impact conditions and can be experienced during daily life activities, with negative impacts on health, QoL, and daily activities [4].
Studies indicate that a precise pathoanatomical diagnosis is only attainable in 8-15% of individuals with lower back pain. Consequently, most LBP cases are designated as chronic nonspecific lower back pain (CNSLBP), a classification denoting pain that persists for three months or more [5]. The main complaint of patients with CNSLBP when they visit a physician is movement restriction in the lumbar spine, which often contributes to discomfort and functional impairment. This exacerbates patients’ daily activities and QoL [6]. Reduced ROM in the lumbar region is often observed in individuals experiencing chronic LBP [7]. Previous studies have highlighted the importance of improving ROM in chronic LBP patients to enhance their physical capabilities and alleviate pain symptoms [8, 9]. Interventions targeting flexibility and ROM in the lumbar region significantly manage chronic LBP and improve overall functionality and well-being [10]. Limited ROM in patients with LBP changes the muscle sensitivity to tension, followed by pain sensation, which does not allow the muscles to reach their full ROM [11]. This changes the movement pattern and contraction of back muscles, which are the primary stabilizers of this region [12], thus leading to muscle imbalance and negatively affecting lumbopelvic stability [13].
Aquatic exercise (AE) is a valuable intervention for psychological problems (e.g. depression, stress, and anxiety) [14], and promotes overall well-being [15]. Immersing and performing physical exercises in water can improve mood, generate relaxation responses, improve well-being, and offer an opportunity to attend to the emotional aspects of rehabilitation [15]. The properties of water, such as buoyancy and support, can alleviate anxiety and promote a relaxed mental state [16].
Open-chain AEs (OCAEs) and closed-chain AEs (CCAEs) have gained remarkable attention as valuable and efficient rehabilitation techniques [17]. Closed kinetic chain (CKC) happens when the foot supports weight on the ground, stabilizing the lower limb’s distal segment [18]. Conversely, an open kinetic chain (OKC) occurs when the distal section is movable [18]. OCAE and CCAE have both benefits and drawbacks in rehabilitation [18], and the decision to select between them depends on the treatment goals [19]. The CCAE offers advantages, such as heightened joint compressive forces, enhanced joint stability, lower shear forces, diminished acceleration forces, greater resistance, better proprioception, and superior dynamic stability [19]. Conversely, the benefits of OCAE include higher rotational and distraction forces, lower resistance forces, increased acceleration forces, enhanced joint and muscle mechanoreceptor deformation, enhanced concentric acceleration and eccentric deceleration forces, and increased backing for functional tasks [19]. A major benefit of AE for rehabilitation is the capacity to start treatments sooner than on land [14]. Earlier AE for chronic LBP patients can be helpful as buoyancy decreases pressure on the spinal column and hydrostatic pressure together with water temperature, improves balance, reduces pain, and prevents muscle atrophy [20]. AE is crucial for enhancing the QoL of individuals with LBP. They can be essential in comprehensive therapeutic programs for individuals [21]. It remains unclear how OKC and CKC exercises can be combined in rehabilitation programs for chronic LBP. Most studies have investigated the effects of performing these exercises on land, while few studies have been conducted for closed- and open-chain exercises in water [22]. Consequently, musculoskeletal and central nervous system (CNS) involvement should be considered when creating treatment plans. Considering this, a randomized controlled trial (RCT) was conducted to examine the possible advantages of incorporating aquatic therapy into the open and closed chain exercises within a comprehensive rehabilitation protocol for individuals with LBP. AE is recognized for its advantages in LBP; the question is whether balance and ROM change after AE. Therefore, this study aimed to investigate the effects of OCAE and CCAE on dynamic balance, ROM, and self-reported pain in male patients with CNSLBP.
Materials and Methods
Study design
This was a three-arm, double-blind RCT (blinding of evaluators and patients). To prevent patient bias, the participants in each group were also unaware of the other group’s existence and the results of their tests until after the post-test stage. The trial adhered to the CONSORT 2010 guidelines to ensure methodological rigor and transparency [23].
Participants
Participants in this study were men aged 40-60 years who had been diagnosed with CNSLBP by a spine specialist, they freely participated in the trial. They were assigned at random using sequentially numbered opaque sealed envelopes to hide their allocation, divided into three groups using software that generates random numbers: OCAE (n=20), CCAE (n=20), and a control group (n=20). In this random allocation method, based on the sample size, each of the randomly produced sequences was recorded on a card, which was then put into one of the prepared envelopes. Finally, after the evaluation, each patient opened one of the envelopes to specify their group. The minimum sample size was calculated utilizing G*Power software, version 3.1.9.2 (effect size=0.8, α=0.05, and power of the test=0.95) for multivariate analysis of variance, one-way analysis of variance (ANOVA) test, and and analysis of covariance (ANCOVA) (demographic information). The study included 86 men with LBP, of whom 18 were eliminated because they did not meet the inclusion criteria. Additionally, eight participants did not adhere to the rehabilitation process. Finally, based on the inclusion and exclusion criteria, 60 participants were chosen to make up the statistical sample. Ultimately, there were 20 patients with CNSLBP in the OCAE group, 20 in the CCAE group, and 20 in the control group (Figure 1). All patients had CNSLBP, which was confirmed by a neurosurgeon. The inclusion criteria included being aged 40-60, having a history of pain for over 12 weeks, and having no history of spinal surgery or hip replacement. The exclusion criteria included pain in other body parts, involvement in therapeutic activities, sciatic pain, lower and upper limb deformities, physiotherapy use throughout the past 12 months, and spondylolysis and respiratory problems [24]. The experimental groups performed CKCE and OKCE for eight weeks, three sessions per week, while the control group received no intervention. Patients were instructed not to inform the evaluators about their group assignments to preserve blinding. The participants were provided with an explanation of the processes and goals. Under the Declaration of Helsinki, all participants and/or their legal guardians provided informed consent before participating in the study and, when appropriate, before information or photos were published in an online open-access publication [25]. Ethical approval was obtained from the Ethics Committee o Bu-Ali Sina University for this study. The study was registered at the Iranian Registry of Clinical Trials (IRCT).
Experimental intervention
After evaluating the listed variables, exercises were performed for eight weeks in two stages. The first stage (first four weeks) aimed to familiarize participants with water, examine breathing patterns, train and perform breathing correctly, use swimming in a pool to strengthen the transverse abdominal muscles and multifidus, and maintain proper posture and breathing throughout daily activities (Table 1).
The second stage (last four weeks) comprised functional progress and aimed to enhance endurance and muscle strength by incorporating a resistance threshold into the exercises (Table 2). A hydrotherapy specialist and researcher supervised all exercise sessions conducted three times a week. Each session lasted approximately 60 minutes., starting with five minutes of general warm-up followed by 50 minutes of core workouts. OCAE group exercises, such as the abdominal drawing-in maneuver, are specifically intended to activate the deep core stabilizers, the transverse abdominis and multifidus muscles. In the deep water, the following exercises were performed using pool noodles (for support) and theraband (for resistance): Leg abduction and adduction, which involve moving the legs apart and together with the knees extended; and hip flexion and extension, which consist of bending and straightening the thigh at the hip while in a floating position. The CCAE group was trained in proper breathing techniques and performed core-stabilizing exercises. These included a supported half-squat against the pool wall with feet on the floor to target the transverse abdominis and multifidus muscles. The program included various walking drills: Forward, backward, and sideways with long steps and extended knees, along with single-leg balance practice that involved moving the other leg forward and back, ending with five minutes of cooling (stretching exercises). The training regimen expanded in volume, intensity, duration, and repetition over successive weeks (Tables 1 and 2). The CCAE group exercised in shallow water, while the OCAE group used noodles in deep water (supervised by a lifeguard) (depth to chest area). The protocols for both groups were performed by a skilled physiotherapist specializing in hydrotherapy [6, 19, 26].
Range of motion (ROM)
This study assessed the ROM of the lumbar region through left and right lateral trunk flexion. During the test, the individual stands comfortably and bends to the left or right by lowering their hand along the side of the leg, and the distance from the middle fingertip to the ground was measured (Figure 1). The validity and reliability were found to be high for left and right lateral flexion (intraclass correlation [ICC]: 0.985; 95% CI, 0.969%, 0.993%) [27].
Y-dynamic balance
The Y test is a reliable method for evaluating dynamic balance. It has been reported that this test’s reliability coefficient is (0.91-0.99). In this test, the subject stands with the dominant leg in the middle (Y angle between the arms: 135°, 90°, and 135°). The participant is instructed to reach with the opposite foot’s toes in three directions (anterior, posterolateral, and posteromedial) while maintaining balance on one leg. The participant was kept balanced, the supporting foot’s heel was kept from lifting off the ground, the reaching toes made slight contact with the ground without bearing weight, and the foot was brought back to its standing posture without making contact. They did not implement these cases; it was considered an error, and the test was repeated after a two-minute rest. Balance scores were normalized based on leg length (the separation between the medial malleolus and the anterior superior iliac spine when supine), and the final test score was the average of three repetitions [14, 28].
Pain
A visual analog scale (VAS) measuring 10 centimeters was used to quantify pain perception. Participants were asked to indicate their pain level by marking a scale within this range. Pain intensity was measured on a scale of 0 (no pain) to 10 (worst pain) [29, 30].
Statistical analysis
Data pertaining to all three groups were collected in the pre-test, post-test, and statistical analysis was then carried out to examine how CKCE and OKCE affected study indicators. The Shapiro-Wilk test was used to assess the η2 normal distribution of data related to variables and demographic characteristics, and the Levene test was used to assess the homogeneity of variances. Analysis of variance (ANOVA) was used to compare the pre-test values of groups, the t-dependent test to examine intra-group differences, and the ANCOVA method was used to compare the post-test values between groups with effect size analysis. Data were analyzed using SPSS software, version 26. The significance level was set at 0.05 (P<0.05). The effect of the interventions was considered using eta coefficients (η2): Low (0.01), medium (0.06), and large (0.14).
Results
Demographic characteristics, such as age, height, weight, and body mass index (BMI), were reported as Mean±SD (P>0.05) (Table 3). At baseline, no statistically significant differences were observed between the groups regarding demographic characteristics (age, weight, height, BMI) or outcome measures (ROM, dynamic balance, and pain), (P>0.05 for all) (Table 3).
Pain
The statistical analysis results using paired t-tests showed a significant difference in pain levels between the participants in the CCAE and OKCE test groups (P<0.05). This suggests that CCAE and OCAE may be more effective in alleviating pain in individuals with CNSLBP. No significant difference was observed in scores in the control group between the pre-and post-tests (P>0.05) (Table 4). Additionally, ANCOVA revealed a substantial effect size with a significant difference in pain levels among the groups (F2=112.386, P=0.001, η2=0.801). This finding supports the efficacy of exercise interventions in reducing pain and highlights the potential for implementing CCAE and OCAE as a therapeutic approach for patients with CNSLBP.
ROM
The results of the statistical analysis using paired t-tests showed a significant difference in right and left ROM before and after the intervention in the CKCE and OKCE test groups (P<0.05). This indicates that both exercise modalities effectively enhance mobility among individuals with CNSLBP. No significant difference was observed in scores in the control between the pre- and post-tests (P>0.05) (Table 4). In addition, the ANCOVA test indicated a small effect size significant difference between CCAE and OCAE groups with the control group in left ROM (F2=11.447, P=0.001, η2=0.29), right ROM (F2=14.806, P=0.001, η2=0.343) (Table 5). These findings indicate a substantial effect of both exercise interventions on improving ROM. Post-hoc test for ANCOVA showed the difference between the control group and the CCAE and OCAE groups for right ROM (P<0.001 for both) and left ROM (P=0.001 and 0.002, respectively). Also, no significant difference was observed between the CCAE and OCAE groups. These results underscore the efficacy of incorporating both CCAE and OCAE into rehabilitation protocols for patients with CNSLBP, as they contribute to improved mobility and functional outcomes. Future studies should examine the causes and long-term impacts of these advancements.
Dynamic balance
The results of the statistical analysis using paired t-tests showed a significant difference in dynamic balance (anterior), dynamic balance (posterior-lateral), and dynamic balance (posterior-medial) between the participants in the CCAE and OCAE test groups (P<0.05). This indicates that both exercise modalities positively influence dynamic balance, a critical component in functional mobility for individuals with chronic CNSLBP. No significant difference was observed in scores in the control group between the pre- and post-tests (P>0.05) (Table 4). ANCOVA indicated a small effect size significant difference between CCAE and OCAE groups and control group for dynamic balance (anterior) (F2=6.065, P=0.004, η2=0.178), and dynamic balance (posterior-lateral) (F2=7.204, P=0.002, η2=0.204), dynamic balance (posterior-medial) (F2=3.964, P=0.005, η2=0.124) (Table 5). These results indicate that CKCE and OKCE significantly enhanced dynamic balance compared to no intervention, with the effect sizes suggesting a meaningful clinical impact. Post-hoc test for ANCOVA showed a difference between the control and CKCE and OKCE groups for dynamic balance (anterior) (P<0.004 for both), dynamic balance (posterior-lateral) (P<0.002 for both), and dynamic balance(posterior-medial) (P<0.004 for both). These findings underscore the importance of incorporating CCAE and OCAE into rehabilitation programs for patients with CNSLBP, as both interventions significantly enhance dynamic balance, which is crucial for preventing falls and improving functional mobility. Future studies should explore the long-term effects of these interventions and their implications for broader rehabilitation strategies.
Discussion
This RCT investigated the effects of AE combined with OKC and CKC exercises on dynamic balance, pain, and ROM in men with CNSLBP. This study aimed to investigate the effect of OCAE and CCAE on dynamic balance, ROM, and self-reported pain in men with CNSLBP. The findings demonstrated that dynamic balance was enhanced by both training program types in the anterior, posterior-lateral, and posterior-medial postural control indices. Additionally, no significant difference was observed in the effectiveness of OCAE and CCAE in posterolateral, posteromedial, pain, and ROM indices. Therefore, AE for eight weeks seems useful for reducing the pain of patients with CNSLBP. These results are consistent with those of Yalfani et al. (2020), Brech et al. (2012), Khodaveisi et al. (2008) and Aluko et al. (2013), who have shown the beneficial effects of rehabilitation exercises in lowering pain levels in patients with CNSLBP [27, 31-36].
Dynamic balance is essential for functional mobility and is often compromised in individuals with CNSLBP [34-36]. The enhancement in anterior balance indicates improved forward stability, which is crucial for activities, such as walking, running, and reaching [37, 38]. CCAE and OCAE improve balance through several mechanisms. Both modalities enhance proprioceptive feedback by activating sensory receptors that provide information about body position and movement, improving body awareness and spatial orientation [39, 40]. The CCAE emphasizes weight-bearing movements that engage stabilizing muscles, while the OCAE utilizes the buoyancy of water to promote muscle coactivation and coordination without impacting the joints [11, 41]. These exercises also enhance neuromuscular control through repetitive practice and reflexive responses to perturbations, while building muscle strength and endurance [42]. Additionally, a safe aquatic environment reduces the risk of injury, allowing individuals to practice dynamic movements that mimic daily activities, ultimately fostering better balance and functional mobility, especially in those with CNSLBP [6, 43].
The significant reduction in pain reported by participants in both exercise groups underscores the therapeutic potential of these interventions. The AE alleviates pain through the buoyancy effect, which reduces mechanical stress on the spine and surrounding musculature [24, 44]. Similarly, AE may enhance pain relief by promoting muscle strengthening and improving functional movement patterns, contributing to better spinal stability and reduced discomfort during daily activities [5]. AE, such as that performed in the OCAE and CCAE groups, has been shown to alleviate pain through several mechanisms. The buoyancy effect of water plays a crucial role in this process [11, 41, 45]. By reducing the gravitational load on the body, buoyancy minimizes mechanical stress on the spine and surrounding musculature [46, 47]. This allows individuals to engage in movements that might otherwise exacerbate pain on land [48, 49]. The hydrostatic pressure of water also promotes circulation, which can improve the way nutrients and oxygen reach tissues while making it easier to eliminate waste products from metabolism [11, 50, 51]. This improved circulation decrease inflammation and muscle soreness, reducing pain [48, 53]. In summary, the pain reduction observed in this study highlights the efficacy of both aquatic and CKC exercises as therapeutic interventions for individuals with CNSLBP. The unique properties of AE, combined with the strength-building focus of CCAE, create a comprehensive approach to pain management. Together, these modalities alleviate pain and empower individuals to regain control over their physical functions and improve their overall well-being.
The enhancement in trunk lateral flexion ROM was a pivotal finding of this study, as an increased ROM is critical for the execution of daily activities and preservation of overall functional independence. The buoyant properties of OCAE allow individuals to achieve a greater ROM without the gravitational constraints typically encountered on land [51, 53]. Studies have shown that AE can increase flexibility and improve overall physical function in CLBP patients [21, 24, 26, 54]. This unique environment facilitates stretching and mobility exercises that may be challenging for individuals with pain or stiffness, promoting greater flexibility and functional capacity [12, 55]. In contrast, the superior effectiveness of CCAE in improving ROM can be attributed to its targeted focus on strengthening the musculature involved in lateral flexion and spinal stabilization [25]. By enhancing both muscular strength and endurance, CCAE contributes to improved flexibility and mobility in the lumbar region, enabling participants to perform lateral movements with greater efficiency and reduced discomfort. Furthermore, the integration of both OCAE and CCAE within rehabilitation protocols is substantiated by neurophysiological evidence indicating that distinct sensory modalities elicit different neural processes [43]. This suggests that the synergistic combination of OCAE and CCAE may optimize neuromuscular adaptations, thus enhancing overall rehabilitation outcomes [39, 49, 56]. This dual approach is likely to improve proprioception, coordination, and muscle activation patterns, which are essential for effective balance and pain management [11, 57]. Consequently, this comprehensive methodology holds significant potential for improving functional performance and enhancing the QoL of individuals with CNSLBP. Furthermore, AE regulates neuromuscular postural control to a stable state, which is essential for improving muscle function. The exercises offered in this study seem to target neuromuscular issues related to CNSLBP, potentially resulting in enhanced ROM, pain relief, and dynamic balance. These findings have implications for health organizations to implement AE programs to improve mental health in patients with LBP.
Conclusion
This study showed that aquatic therapy positively affects dynamic balance, pain, ROM, and mental health in patients with CNSLBP. The primary objective of aquatic therapy is to instruct patients to utilize water as a supplementary treatment for recovering patients with LBP. Therefore, aquatic therapy can play a role in patient recovery. Healthcare professionals, including doctors, physiotherapists, and occupational therapists, can incorporate open and CKC exercises in water into a thorough therapeutic program for patients with LB.
Limitation
Our study has several limitations that should be acknowledged: the absence of female participants, the lack of long-term follow-up, potential selection bias, and the omission of a comparator group involving land-based exercises. Furthermore, the uncontrolled variables of participants’ age and BMI may influence the results and restrict how widely the results can be used.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Bu-Ali Sina University, Hamadan, Iran (Code: IR.BASU.REC.1401.026). The study was registered at the Iranian Registry of Clinical Trials (IRCT), Tehran, Iran (Code: IRCT20230430058033N1).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design, Hossein Ashoury; Drafting of article: Hossein Ashoury and Ali Yalfani; Critical revision: Hossein Ashoury and Masoud Azizian; monitoring progress: Ali Yalfani; Data analysis, interpretation and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all participants for their cooperation in the study.
References
- Wettstein M, Eich W, Bieber C, Tesarz J. Pain intensity, disability, and quality of life in patients with chronic low back pain: Does age matter? Pain Medicine. 2019; 20(3):464-75. [DOI:10.1093/pm/pny062] [PMID]
- Yousefzadeh Chabok S, Ezzati K, Saberi A, Hosein Zadeh J. [Evaluating the prevalence of lumbar myofascial pain syndrome in patients with non-specific chronic low back pain and a normal MRI study (Persian)]. Journal of Guilan University of Medical Sciences. 2020; 29(1):43-50. [Link]
- Roussel N, Nijs J, Truijen S, Vervecken L, Mottram S, Stassijns G. Altered breathing patterns during lumbopelvic motor control tests in chronic low back pain: A case-control study. European Spine Journal. 2009; 18(7):1066-73. [DOI:10.1007/s00586-009-1020-y] [PMID]
- Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr, Shekelle P, et al. Diagnosis and treatment of low back pain: A joint clinical practice guideline from the American College of Physicians and the American Pain Society. Annals of Internal Medicine. 2007; 147(7):478-91. [DOI:10.7326/0003-4819-147-7-200710020-00006] [PMID]
- Mills W, Kondakis N, Orr R, Warburton M, Milne N. Does hydrotherapy impact behaviours related to mental health and well-being for children with autism spectrum disorder? A randomised crossover-controlled pilot trial. International Journal of Environmental Research and Public Health. 2020; 17(2):558. [DOI:10.3390/ijerph17020558] [PMID]
- Ghafouri M, Teymourzadeh A, Nakhostin-Ansari A, Sepanlou SG, Dalvand S, Moradpour F, et al. Prevalence and predictors of low back pain among the Iranian population: Results from the Persian cohort study. Annals of Medicine and Surgery. 2022; 74:103243. [DOI:10.1016/j.amsu.2022.103243] [PMID]
- Kanaan SF, Alissa HM, Jaber AA, Almhdawi KA, Mansour ZM, Alhanada M. Knowledge related to low back pain and its associated factors in patients with low back pain: A cross-sectional study. Journal of Back and Musculoskeletal Rehabilitation. 2023; 36(1):217-25. [DOI:10.3233/BMR-220004] [PMID]
- Beyranvand R, Sahebozamani M, Daneshjoo A, Seyedjafari E. Assessment and comparison the effect of exercise in different depth of water on postural stability and balance recovery strategies of older people: A clinical trial. The Scientific Journal of Rehabilitation Medicine. 2023; 11(6):1002-15. [DOI:10.32598/SJRM.11.6.12]
- Teixeira AL, da Silva NF, da Silva Filho EM. Evaluation of functional disability and pain in patients with chronic low back pain submitted to physiotherapy. Manual Therapy, Posturology & Rehabilitation Journal. 2016; 1-6. [DOI:10.17784/mtprehabjournal.2016.14.374]
- Luomajoki H, Kool J, de Bruin ED, Airaksinen O. Movement control tests of the low back; evaluation of the difference between patients with low back pain and healthy controls. BMC Musculoskeletal Disorders. 2008; 9:170. [DOI:10.1186/1471-2474-9-170] [PMID]
- Gordon R, Bloxham S. A systematic review of the effects of exercise and physical activity on non-specific chronic low back pain. Healthcare. 2016; 4(2):22. [DOI:10.3390/healthcare4020022] [PMID]
- Delitto A, George SZ, Van Dillen L, Whitman JM, Sowa G, Shekelle P, et al. Low back pain. The Journal of Orthopaedic and Sports Physical Therapy. 2012; 42(4):A1-57. [DOI:10.2519/jospt.2012.42.4.A1] [PMID]
- Cuesta-Vargas AI, Adams N, Salazar JA, Belles A, Hazañas S, Arroyo-Morales M. Deep water running and general practice in primary care for non-specific low back pain versus general practice alone: Randomized controlled trial. Clinical Rheumatology. 2012; 31(7):1073-8. [DOI:10.1007/s10067-012-1977-5] [PMID]
- McGill S, Juker D, Kropf P. Appropriately placed surface EMG electrodes reflect deep muscle activity (psoas, quadratus lumborum, abdominal wall) in the lumbar spine. Journal of Biomechanics. 1996; 29(11):1503-7. [DOI:10.1016/0021-9290(96)84547-7] [PMID]
- Rubinstein SM, de Zoete A, van Middelkoop M, Assendelft WJJ, de Boer MR, van Tulder MW. Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain: Systematic review and meta-analysis of randomised controlled trials. BMJ. 2019; 364:l689. [DOI:10.1136/bmj.l689] [PMID]
- Hossein Abadi F, Choo LA, Elumalai G, Sankaravel M, Razli AI. Does aquatic exercise improve quality of life in obese low-back pain population? International Journal of Physiotherapy 2019; 6(4):128-33. [DOI:10.15621/ijphy/2019/v6i4/185415]
- Basso JC, Suzuki WA. The effects of acute exercise on mood, cognition, neurophysiology, and neurochemical pathways: A review. Brain Plasticity. 2017; 2(2):127-52. [DOI:10.3233/BPL-160040] [PMID]
- Hassan SZ, Waqas M, Yaqub D, Asad D. Hydrotherapy: an efficient and cost-effective treatment for depression. International Journal of Community Medicine and Public Health. 2016; 4(1):274. [DOI:10.18203/2394-6040.ijcmph20164752]
- Bae W, Kim C. The effect of closed kinetic and open kinetic exercise on thickness of low back stabilization exercise using an ultrasonography imaging. Journal of The Korean Society of Integrative Medicine. 2013; 1(2):67-80. [DOI:10.15268/ksim.2013.1.2.067]
- Kwon YJ, Park SJ, Jefferson J, Kim K. The effect of open and closed kinetic chain exercises on dynamic balance ability of normal healthy adults. Journal of Physical Therapy Science. 2013; 25(6):671-4. [DOI:10.1589/jpts.25.671] [PMID]
- Sciascia A, Cromwell R. Kinetic chain rehabilitation: A theoretical framework. Rehabilitation Research and Practice. 2012; 2012:853037. [DOI:10.1155/2012/853037] [PMID]
- Mooventhan A, Nivethitha L. Scientific evidence-based effects of hydrotherapy on various systems of the body. North American Journal of Medical Sciences. 2014; 6(5):199-209.[DOI:10.4103/1947-2714.132935] [PMID]
- Dundar U, Solak O, Yigit I, Evcik D, Kavuncu V. Clinical effectiveness of aquatic exercise to treat chronic low back pain: a randomized controlled trial. Spine. 2009; 34(14):1436-40. [DOI:10.1097/BRS.0b013e3181a79618] [PMID]
- Tagesson S, Öberg B, Good L, Kvist J. A comprehensive rehabilitation program with quadriceps strengthening in closed versus open kinetic chain exercise in patients with anterior cruciate ligament deficiency: a randomized clinical trial evaluating dynamic tibial translation and muscle function. The American Journal of Sports Medicine. 2008; 36(2):298-307. [DOI:10.1177/0363546507307867] [PMID]
- Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P, Consort Group. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: explanation and elaboration. Annals of Internal Medicine. 2008; 148(4):295-309. [DOI:10.7326/0003-4819-148-4-200802190-00008] [PMID]
- Ariyoshi M, Sonoda K, Nagata K, Mashima T, Zenmyo M, Paku C, et al. Efficacy of aquatic exercises for patients with low-back pain. The Kurume Medical Journal. 1999; 46(2):91-6. [DOI:10.2739/kurumemedj.46.91] [PMID]
- Yalfani A, Raeisi Z, Koumasian Z. Effects of eight-week water versus mat pilates on female patients with chronic nonspecific low back pain: Double-blind randomized clinical trial. Journal of Bodywork and Movement Therapies. 2020; 24(4):70-75. [DOI:10.1016/j.jbmt.2020.06.002] [PMID]
- Olkoski MM, Silva MF, Guenka LC, Pelegrinelli AR, Dela Bela LF, et al. Comparing the effects of aquatic exercises with or without high intensity on the functional status, muscular endurance, and performance of patients with chronic low back pain. The Journal of Sports Medicine and Physical Fitness. 2020; 61(5):699-706. [DOI:10.23736/S0022-4707.20.11265-9] [PMID]
- Khojastehpour B, Atri AE, Javaheri SA. Comparison the effect of core stabilization training in water and on land on pain and dynamic postural stability in women with chronic non-specific low back pain. Journal of Anesthesiology and Pain. 2019; 10(2):75-90. [Link]
- Johnson M, Mulcahey MJ. Interrater reliability of spine range of motion measurement using a tape measure and goniometer. Journal of Chiropractic Medicine. 2021; 20(3):138-47. [DOI:10.1016/j.jcm.2021.09.003] [PMID]
- Begum MR, Hossain MA. Validity and reliability of visual analogue scale (VAS) for pain measurement. Journal of Medical Case Reports and Reviews. 2019; 2(11):394-402. [Link]
- Baena-Beato PÁ, Artero EG, Arroyo-Morales M, Robles-Fuentes A, Gatto-Cardia MC, Delgado-Fernández M. Aquatic therapy improves pain, disability, quality of life, body composition and fitness in sedentary adults with chronic low back pain. A controlled clinical trial. Clinical Rehabilitation. 2014; 28(4):350-60. [DOI:10.1177/0269215513504943] [PMID]
- Richardson JT. Eta squared and partial eta squared as measures of effect size in educational research. Educational Research Review. 2011; 6(2):135-47. [DOI:10.1016/j.edurev.2010.12.001]
- Brech GC, Andrusaitis SF, Vitale GF, Greve JM. Correlation of disability and pain with postural balance among women with chronic low back pain. Clinics. 2012; 67(8):959-62. [DOI:10.6061/clinics/2012(08)17] [PMID]
- Khodaveisi H, Sazvar A, Anbarian M. The effect of 12-week aquatic exercises on core stability of women with low back pain. Physical Treatments. 2018; 8(3):161-8. [DOI:10.32598/ptj.8.3.161]
- Aluko A, DeSouza L, Peacock J. The effect of core stability exercises on variations in acceleration of trunk movement, pain, and disability during an episode of acute nonspecific low back pain: A pilot clinical trial. Journal of Manipulative and Physiological Therapeutics. 2013; 36(8):497-504.e1-3. [DOI:10.1016/j.jmpt.2012.12.012] [PMID]
- Mills WL, Kunik ME, Kelly PA, Wilson NL, Starks S, Asghar-Ali A, et al. Validation of the MEDSAIL tool to screen for capacity for safe and independent living among nursing home residents. Journal of the American Medical Directors Association. 2020; 21(12):1992-6. [DOI:10.1016/j.jamda.2020.05.008]
- Psycharakis SG, Coleman SGS, Linton L, Valentin S. The water study: Which aquatic exercises increase muscle activity and limit pain for people with low back pain? Physiotherapy. 2022; 116:108. [DOI:10.1016/j.physio.2022.03.003] [PMID]
- Nemčić T, Budišin V, Vrabec-Matković D, Grazio S. Comparison of the effects of land-based and water-based therapeutic exercises on the range of motion and physical disability in patients with chronic low-back pain: Single-blinded randomized study. Acta Clinica Croatica. 2013; 52(3.):321-6. [Link]
- Yalfani A, Ahmadnezhad L, Gholami Borujeni B, Khoshnamvand Z. [The effect of six weeks core stability exercise training on balance, pain and function in women with chronic low back pain (Persian)]. Journal of Health and Care. 2017; 18(4):336-46. [Link]
- Pires D, Cruz EB, Caeiro C. Aquatic exercise and pain neurophysiology education versus aquatic exercise alone for patients with chronic low back pain: A randomized controlled trial. Clinical Rehabilitation. 2015; 29(6):538-47. [DOI:10.1177/0269215514549033] [PMID]
- Cole AJ, Becker BE. Comprehensive aquatic therapy. Oxford: Butterworth-Heinemann; 2004. [Link]
- Ploegaerts A. Water exercise rehabilitation for people suffering from non-specific chronic low back pain. Pori: SAMK; 2019. [Link]
- Benfield RD, Hortobágyi T, Tanner CJ, Swanson M, Heitkemper MM, Newton ER. The effects of hydrotherapy on anxiety, pain, neuroendocrine responses, and contraction dynamics during labor. Biological Research for Nursing. 2010; 12(1):28-36. [DOI:10.1177/1099800410361535] [PMID]
- Jackson M, Kang M, Furness J, Kemp-Smith K. Aquatic exercise and mental health: A scoping review. Complementary Therapies in Medicine. 2022; 66:102820. [DOI:10.1016/j.ctim.2022.102820] [PMID]
- Marcos-Lorenzo D, Lysandrou C, Sudres L, Gil-Martinez A, Swanenburg J, Clark JE, et al. 50% body weight loading reduces stature increases and lumbar disc expansion from 4 h hyper-buoyancy floatation versus 15 min sitting upright. Experimental Physiology. 2024. [DOI:10.1113/EP091745] [PMID]
- Rukavishnikov IV, Amirova LE, Kukoba TB, Tomilovskaya ES, Kozlovskaya IB. Effects of gravitational unloading on back muscles tone. Human Physiology. 2017; 43(3):291-300. [DOI:10.1134/S0362119717030173]
- Bullington J. Embodiment and chronic pain: Implications for rehabilitation practice. Health Care Analysis. 2009; 17(2):100-9. [DOI:10.1007/s10728-008-0109-5]
- Hodges PW, Smeets RJ. Interaction between pain, movement, and physical activity: short-term benefits, long-term consequences, and targets for treatment. The Clinical Journal of Pain. 2015; 31(2):97-107. [Link]
- Pendergast DR, Moon RE, Krasney JJ, Held HE, Zamparo P. Human physiology in an aquatic environment. Comprehensive Physiology. 2015; 5(4):1705-50. [DOI:10.1002/j.2040-4603.2015.tb00655.x]
- Jayathilakan K, Sultana K, Radhakrishna K, Bawa AS. Utilization of byproducts and waste materials from meat, poultry and fish processing industries: A review. Journal of Food Science and Technology. 2012; 49(3):278-93. [DOI:10.1007/s13197-011-0290-7]
- Dupuy O, Douzi W, Theurot D, Bosquet L, Dugué B. An evidence-based approach for choosing post-exercise recovery techniques to reduce markers of muscle damage, soreness, fatigue, and inflammation: A systematic review with meta-analysis. Frontiers in Physiology. 2018; 9:312968. [DOI:10.3389/fphys.2018.00403]
- Ellenbecker TS, Davies GJ. Closed kinetic chain exercise: A comprehensive guide to multiple joint exercise. Champaign: Human Kinetics; 2001. [Link]
- Hayden JA, Ellis J, Ogilvie R, Stewart SA, Bagg MK, Stanojevic S, et al. Some types of exercise are more effective than others in people with chronic low back pain: A network meta-analysis. Journal of physiotherapy. 2021; 67(4):252-62. [DOI:10.1016/j.jphys.2021.09.004]
- Alter MJ. Science of flexibility. Champaign: Human Kinetics; 2004. [Link]
- Adeel M, Lin BS, Chaudhary MA, Chen HC, Peng CW. Effects of strengthening exercises on human kinetic chains based on a systematic review. Journal of Functional Morphology and Kinesiology. 2024; 9(1):22. [DOI:10.1016/j.jphys.2021.09.004]
- Chiaramonte R, Bonfiglio M, Leonforte P, Coltraro GL, Guerrera CS, Vecchio M. Proprioceptive and dual-task training: the key of stroke rehabilitation, A systematic review. Journal of Functional Morphology and Kinesiology. 2022; 7(3):53. [DOI:10.3390/jfmk7030053]
Article type: Original Research Articles |
Subject:
Physical Medicine and Rehabilitation
Received: 2025/07/7 | Accepted: 2025/09/9 | Published: 2025/12/1
Received: 2025/07/7 | Accepted: 2025/09/9 | Published: 2025/12/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
