
988368
Sun, Sep 1, 2024

Volume 21, Issue 2 (June 2023)
Iranian Rehabilitation Journal 2023, 21(2): 231-238 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sheikh S, Poursadeghian M, Rohaninasab M, Vatani J, Akhlaghi Pirposhteh E, Ahmadi-Mazhin S, et al . The Incidence of Lung Cancer and Smoking in Iran, Turkey, England, and the USA: A Comparative Study. Iranian Rehabilitation Journal 2023; 21 (2) :231-238
URL: http://irj.uswr.ac.ir/article-1-1593-en.html
URL: http://irj.uswr.ac.ir/article-1-1593-en.html
Samira Sheikh1 

 , Mohsen Poursadeghian2 , Marzieh Rohaninasab3 , Javad Vatani4 , Elham Akhlaghi Pirposhteh5 , Sadegh Ahmadi-Mazhin6 , Ali Salehi Sahlabadi7 , Maliheh Eshaghzadeh8 , Amir Hassan Dehghan Nayeri1 , Alireza Khammar * 9
, Mohsen Poursadeghian2 , Marzieh Rohaninasab3 , Javad Vatani4 , Elham Akhlaghi Pirposhteh5 , Sadegh Ahmadi-Mazhin6 , Ali Salehi Sahlabadi7 , Maliheh Eshaghzadeh8 , Amir Hassan Dehghan Nayeri1 , Alireza Khammar * 9
, Mohsen Poursadeghian2 , Marzieh Rohaninasab3 , Javad Vatani4 , Elham Akhlaghi Pirposhteh5 , Sadegh Ahmadi-Mazhin6 , Ali Salehi Sahlabadi7 , Maliheh Eshaghzadeh8 , Amir Hassan Dehghan Nayeri1 , Alireza Khammar * 9
1- Student Research Committee, Semnan University of Medical Scienses, Semnan, Iran.
2- Department of Occupational Health Engineering, Ardabil University of Medical Sciences, Tehran, Iran.
3- Department of Aestetic and Restorative, School of Dental, International Campus, Tehran University of Medical Sciences,Tehran, Iran.
4- Department of Occupational Health Engineering, Guilan Road Trauma Research Center, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
5- Department of Occupational Health Engineering, School of Medical Sciences, Tarbiat Modares University, Tehran, Iran.
6- Department of Public Health, School of Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
7- Department of Occupational Health Engineering, School of Health and Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
8- Department of Nursing, Faculty of Nursing and Midwifery, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran.
9- Department of Occupational Health Engineering, Toxicology and Addiction Research Center, School of Health, Zabol University of Medical Sciences, Zabol, Iran.
2- Department of Occupational Health Engineering, Ardabil University of Medical Sciences, Tehran, Iran.
3- Department of Aestetic and Restorative, School of Dental, International Campus, Tehran University of Medical Sciences,Tehran, Iran.
4- Department of Occupational Health Engineering, Guilan Road Trauma Research Center, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
5- Department of Occupational Health Engineering, School of Medical Sciences, Tarbiat Modares University, Tehran, Iran.
6- Department of Public Health, School of Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
7- Department of Occupational Health Engineering, School of Health and Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
8- Department of Nursing, Faculty of Nursing and Midwifery, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran.
9- Department of Occupational Health Engineering, Toxicology and Addiction Research Center, School of Health, Zabol University of Medical Sciences, Zabol, Iran.
Full-Text [PDF 922 kb]
(405 Downloads)
| Abstract (HTML) (1591 Views)
Full-Text: (176 Views)
Introduction
Despite efforts to control and prevent infectious diseases in recent decades, the incidence and prevalence of chronic diseases have increased significantly [1]. After cardiovascular disease and accidents, cancer is the third leading cause of death in Iran [2]. Also, cancer is considered one of the most important health problems in many developed and developing countries [3, 4].
Among cancers, lung cancer is the most common and deadly cancer worldwide. More than 13% of the world’s cancer diagnoses in 2012 were related to lung cancer. Of 10.9 million newly diagnosed cancers, 1.35 million are related to lung cancer. Of 6.7 million deaths from cancers, 1.18 million occur in people with lung cancers [5]. New estimates from the International Agency for Research on Cancer (IARC) show that the number of cancer deaths worldwide was more than 1.8 million in 2007, and this number may reach 10 million deaths per year in 2030, with the highest increase in developing countries (70% of cancer deaths) [6]. It is estimated that 229000 cases of lung cancer and 160000 deaths due to it occurred in the United States in 2013 [7]. This figure is about 27% of all deaths from all types of cancer; in other words, one in three or four deaths from cancer is due to lung cancer. Scientific studies estimate that 7% of people born in the future will develop lung cancer, and 6% will die out of it [8].
In Iran, cancer is the third leading cause of death. More than 30000 die from cancer each year. On the other hand, with increasing life expectancy and aging in Iran, technological advances, and moving away from a clean, healthy environment without industrial carcinogens, cancer incidence is expected to double in the next two decades. The World Health Organization (WHO) predicts that cancer in Iran will reach 86947 cases in 2025 in the total population and the death rate due to cancer to 62897 cases. According to the latest National Program of Cancer Registries (NPCR), lung cancer is among the 10 most common and deadliest cancers. Lung cancer is the third leading cause of cancer mortality. The number of lung cancer patients in 2019 was 5051, which accounts for about 4%-6% of cancers [9].
Cigarettes and old age are major risk factors for lung cancer, but other factors such as air pollution, genetics, radon gas, and asbestos are effective in causing lung cancer. All studies have identified smoking as a major risk factor for lung cancer [8]. The major contribution of lung cancer to overall cancer mortality (1.3 million deaths per year) and its dependence on smoking suggest that primary lung cancer is a major health problem with a poor prognosis in general. Therefore, understanding the status and trend of lung cancer and its changes in recent years can pave the way for prevention and even treatment in the future for lung cancer. The control of lung cancer is one of the WHO goals and one of the important challenges of the Iranian health system [9].
Despite increasing public awareness of cancer control, this problem has not yet gained priority among other public health problems. Many cancers can be prevented and diagnosed with definitive treatment for many of them. This comparative study aimed to investigate the incidence of lung cancer and smoking in Iran, Turkey, England, and the USA due to the importance of smoking as an important and preventable risk factor for lung cancer.
Materials and Methods
Data sources
The population data, the age-standardized rate (ASR) of lung cancer, and the percentage of smokers in Iran for 2002–2021 were obtained from the Iran Ministry of Health and Medical Education, the World Bank database, the Organization for Economic Co-operation and Development (OECD) Health Statistics, and WHO. Moreover, published studies were scanned to identify additional records. For the USA, England, and Turkey, we obtained the population data, ASR of lung cancer, and percentage of smokers for 2002–2021 from the World Bank Open Data, the OECD Health Statistics, and WHO. A search of literature was also conducted to find more records.
The age-standardized rate is a summarized rate that will be observed for a population, provided that we have that population’s age-specific rates and the target population’s age composition is considered similar to the reference population (standard population). The age-standardized rate is calculated according to the Equation 1:
.jpg)
Where i represents the age groups, di represents the number of disease cases, yi denotes the number of person-years at risk, and wi represents the number of people (or weight) of the i age group in the standard population used [10].
Data analysis
We calculated the percentage of smokers in each country by dividing the number of smokers by the sum of people in the country. The SPSS software, version 21 was used to analyze the data.
Results
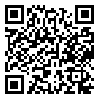
Table 1 presents the studied indicators in the selected countries [8, 11-13].
England, with an ASR of 46, has the highest lung cancer rate, and Iran (ASR=21) has the lowest rate. Among the countries studied, the lowest population is related to the United Kingdom (67880000), and the highest to the United States (331890000). The highest percentage of smokers is in Turkey (29.3%), and the lowest rate is in Iran (20%) [8, 11-13].
Regarding the rising trend of the ASR index, lung cancer in Iran and Turkey has had an upward growth, and in England and the United States, a downward trend. Regarding smoking, the upward trend is related to Iran, Turkey, and the United Kingdom; the downward trend is related to the United States (Figure 1) [11-13].
.jpg)
Discussion
England, with an ASR of 46, has the highest rate of lung cancer, and Iran, with an ASR of 21, has the lowest rate. Turkey has the highest percentage of smokers (%29.3), and the lowest percentage belongs to Iran (%20). Regarding the rising trend of the ASR index, lung cancer in Iran and Turkey has had an upward trend, and England and the United States have a downward trend.
Because the ASR of lung cancer in 2018 in Iran was 21, according to a NPCR report in 2019, lung cancer is only cancer whose ASR in Iran should have been higher than the values obtained. The three main reasons for lung cancer’s low ASR are problematic access to lung lesions and the lack of diagnostic and sampling facilities and equipment in some parts of Iran. Second, the number of some types of cancer has increased, and as a result, it has been ranked lower in the lung cancer ranking. Third, in some pathology reports with the diagnosis of lung cancer, primary or secondary cancer is not specified due to high lung metastasis cases. In this case, the center records their topographic code; thus lung cancers are eliminated from the list [9].
Although smoking prevalence has declined over the past 30 years, population growth has increased the total number of smokers, from 0.99 billion in 1990 to 1.14 billion in 2019 worldwide [14]. Tobacco kills more than 8 million people annually. More than 7 million of these deaths are due to direct smoking, while about 1.2 million are due to secondhand smoke from non-smokers [13].
One of the effective factors in the incidence of lung cancer is smoking. Smoking is directly related to lung cancer. A study of 242 people with lung cancer found that 85% of men were smokers, and another 5% were smokers. Overall, 66.5% of all patients with lung cancer were smokers, and 15.7% were smokers [15].
Accurate statistics on smoking have not been reported in Iran, but several studies have reported smoking statistics between 13% and 15% [16, 17]. Cigarette tax can significantly reduce its consumption and ASR lung cancer growth rate. In terms of the percentage of taxes allocated to the top cigarette brands, the United Kingdom, with an 82.16% tax rate, has the highest, and Iran, with a 4.83% tax rate, has the lowest cigarette tax, also the cigarette tax rate in Turkey is 82.13% and in the United States is 42.54%. In Turkey, cigarette sales have dropped significantly since 2010 due to increased cigarette taxes [18-20]. Due to the implementation of the plan to increase the smoking tax in recent years, there will not be much change in the growth chart of lung cancer so quickly. Lung cancer has also been on the rise in the United States since 1970, but with the tax rate increase of the top cigarette brands, the ASR rate of lung cancer has been declining since 2000. However, in Iran, the cigarette tax is smaller from all countries in the region except Afghanistan, and in recent years the tax rate has been declining [18]. The proposed policy is based on examining the impact of several different scenarios, according to which the application of items such as increasing the share of the budget for prevention and culture against smoking in the treatment budget, as well as increasing the price of cigarettes, can have favorable results in reducing mortality due to smoking and lung cancer [21]. Therefore, by following the example of successful countries in the field of legislation to increase the tax on cigarettes and the implementation of this program, Iran can significantly reduce smoking and, consequently, the increasing trend of lung cancer. In addition to taxes, timely and correct diagnosis of lung cancer can help substantially reduce the complications of the disease. Studies have found that more than 74% of people with lung cancer were diagnosed with stages 3 or 4 [22]. In the United Kingdom and the United States, there are programs and plans to increase the power of diagnosis and early diagnosis of the disease.
Lung cancer is the most common and deadly cancer in most countries. The most important problem concerning this cancer in Iran is the lack of accurate statistics on its prevalence and mortality. According to a recent recommendation by international organizations, including the American Cancer Society, the American College of Radiology, and the International Association for the Study of Lung Cancer (IASLC) in 2013, annual high-risk screening by low-risk dose CT is the most effective way to prevent death from lung cancer. Before implementing this program in the country, the cost-effectiveness of this project should be examined [23]. According to a study by Saba et al. (2016) on lung cancer in Iran, screening in the country will increase the number of early diagnoses 5 times [8]. Ghobadi et al. investigated the epidemiology of lung cancer and risk factors in one of the cities of Iran. This study showed that men were 4.6 times more likely than women to have lung cancer, and smoking was the most important risk factor for the disease [24].
Smoking is a health problem in developed and developing countries. Smoking increases the risk of lung cancer by 5 to 10 times with a clear dose-response relationship [25]. The geographical and temporal patterns of lung cancer and mortality at the population level are largely determined by tobacco use, a major cause of lung carcinogenesis worldwide [26]. In the United States, lung cancer incidence and mortality are declining due to decades of public education and tobacco control policies. However, lung cancer incidence and mortality are increasing in other parts of the world due to the onset of the tobacco epidemic in different countries and populations in developing countries. Smoking is the most common risk factor for lung cancer [27].
In the United States, efforts have been made since 2000 to replace old therapies, such as chemotherapy, with new ones, such as targeted therapies [28]. Rezaei et al. reported that the economic burden of lung cancer has been significant for the Iranian health system. Effective interventions in smoking cessation, early detection, strengthening of cancer prevention, and implementation of new cancer treatment and medical technology can compensate for some of the costs associated with lung cancer in Iran [29]. According to the national cancer registration report, there is a lack of facilities and diagnostic and sampling devices in some parts of Iran, resulting in problems accessing lung lesions, timely diagnosis, and unscientific recording of lung cancer statistics. So, it is recommended to model successful countries using new diagnostic methods and community-based education to familiarize the community with the early symptoms of lung cancer. These measures are effective in reducing the incidence of lung cancer.
Conclusion
The results of this study show that the incidence of lung cancer in Iran and Turkey is increasing, so following the example of successful countries in the implementation of tobacco tax programs, especially cigarettes can be shared taxes to the health sector, especially for preventive activity, such as implementing educational and cultural programs to reduce smoking and lung cancer screening, as well as new diagnostic methods for lung cancer.
Ethical Considerations
Compliance with ethical guidelines
This study is aaaproved by the Research Deputy of Zabol University of Medical Sciences (Code: IR.ZBMU.REC.1401.120).
Funding
This research was supported by the research project (No.: 401000291), funded by the Zabol University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all researchers in the field which studies were used in the current study.
References
Despite efforts to control and prevent infectious diseases in recent decades, the incidence and prevalence of chronic diseases have increased significantly [1]. After cardiovascular disease and accidents, cancer is the third leading cause of death in Iran [2]. Also, cancer is considered one of the most important health problems in many developed and developing countries [3, 4].
Among cancers, lung cancer is the most common and deadly cancer worldwide. More than 13% of the world’s cancer diagnoses in 2012 were related to lung cancer. Of 10.9 million newly diagnosed cancers, 1.35 million are related to lung cancer. Of 6.7 million deaths from cancers, 1.18 million occur in people with lung cancers [5]. New estimates from the International Agency for Research on Cancer (IARC) show that the number of cancer deaths worldwide was more than 1.8 million in 2007, and this number may reach 10 million deaths per year in 2030, with the highest increase in developing countries (70% of cancer deaths) [6]. It is estimated that 229000 cases of lung cancer and 160000 deaths due to it occurred in the United States in 2013 [7]. This figure is about 27% of all deaths from all types of cancer; in other words, one in three or four deaths from cancer is due to lung cancer. Scientific studies estimate that 7% of people born in the future will develop lung cancer, and 6% will die out of it [8].
In Iran, cancer is the third leading cause of death. More than 30000 die from cancer each year. On the other hand, with increasing life expectancy and aging in Iran, technological advances, and moving away from a clean, healthy environment without industrial carcinogens, cancer incidence is expected to double in the next two decades. The World Health Organization (WHO) predicts that cancer in Iran will reach 86947 cases in 2025 in the total population and the death rate due to cancer to 62897 cases. According to the latest National Program of Cancer Registries (NPCR), lung cancer is among the 10 most common and deadliest cancers. Lung cancer is the third leading cause of cancer mortality. The number of lung cancer patients in 2019 was 5051, which accounts for about 4%-6% of cancers [9].
Cigarettes and old age are major risk factors for lung cancer, but other factors such as air pollution, genetics, radon gas, and asbestos are effective in causing lung cancer. All studies have identified smoking as a major risk factor for lung cancer [8]. The major contribution of lung cancer to overall cancer mortality (1.3 million deaths per year) and its dependence on smoking suggest that primary lung cancer is a major health problem with a poor prognosis in general. Therefore, understanding the status and trend of lung cancer and its changes in recent years can pave the way for prevention and even treatment in the future for lung cancer. The control of lung cancer is one of the WHO goals and one of the important challenges of the Iranian health system [9].
Despite increasing public awareness of cancer control, this problem has not yet gained priority among other public health problems. Many cancers can be prevented and diagnosed with definitive treatment for many of them. This comparative study aimed to investigate the incidence of lung cancer and smoking in Iran, Turkey, England, and the USA due to the importance of smoking as an important and preventable risk factor for lung cancer.
Materials and Methods
Data sources
The population data, the age-standardized rate (ASR) of lung cancer, and the percentage of smokers in Iran for 2002–2021 were obtained from the Iran Ministry of Health and Medical Education, the World Bank database, the Organization for Economic Co-operation and Development (OECD) Health Statistics, and WHO. Moreover, published studies were scanned to identify additional records. For the USA, England, and Turkey, we obtained the population data, ASR of lung cancer, and percentage of smokers for 2002–2021 from the World Bank Open Data, the OECD Health Statistics, and WHO. A search of literature was also conducted to find more records.
The age-standardized rate is a summarized rate that will be observed for a population, provided that we have that population’s age-specific rates and the target population’s age composition is considered similar to the reference population (standard population). The age-standardized rate is calculated according to the Equation 1:
Where i represents the age groups, di represents the number of disease cases, yi denotes the number of person-years at risk, and wi represents the number of people (or weight) of the i age group in the standard population used [10].
Data analysis
We calculated the percentage of smokers in each country by dividing the number of smokers by the sum of people in the country. The SPSS software, version 21 was used to analyze the data.
Results
Table 1 presents the studied indicators in the selected countries [8, 11-13].
England, with an ASR of 46, has the highest lung cancer rate, and Iran (ASR=21) has the lowest rate. Among the countries studied, the lowest population is related to the United Kingdom (67880000), and the highest to the United States (331890000). The highest percentage of smokers is in Turkey (29.3%), and the lowest rate is in Iran (20%) [8, 11-13].
Regarding the rising trend of the ASR index, lung cancer in Iran and Turkey has had an upward growth, and in England and the United States, a downward trend. Regarding smoking, the upward trend is related to Iran, Turkey, and the United Kingdom; the downward trend is related to the United States (Figure 1) [11-13].
Discussion
England, with an ASR of 46, has the highest rate of lung cancer, and Iran, with an ASR of 21, has the lowest rate. Turkey has the highest percentage of smokers (%29.3), and the lowest percentage belongs to Iran (%20). Regarding the rising trend of the ASR index, lung cancer in Iran and Turkey has had an upward trend, and England and the United States have a downward trend.
Because the ASR of lung cancer in 2018 in Iran was 21, according to a NPCR report in 2019, lung cancer is only cancer whose ASR in Iran should have been higher than the values obtained. The three main reasons for lung cancer’s low ASR are problematic access to lung lesions and the lack of diagnostic and sampling facilities and equipment in some parts of Iran. Second, the number of some types of cancer has increased, and as a result, it has been ranked lower in the lung cancer ranking. Third, in some pathology reports with the diagnosis of lung cancer, primary or secondary cancer is not specified due to high lung metastasis cases. In this case, the center records their topographic code; thus lung cancers are eliminated from the list [9].
Although smoking prevalence has declined over the past 30 years, population growth has increased the total number of smokers, from 0.99 billion in 1990 to 1.14 billion in 2019 worldwide [14]. Tobacco kills more than 8 million people annually. More than 7 million of these deaths are due to direct smoking, while about 1.2 million are due to secondhand smoke from non-smokers [13].
One of the effective factors in the incidence of lung cancer is smoking. Smoking is directly related to lung cancer. A study of 242 people with lung cancer found that 85% of men were smokers, and another 5% were smokers. Overall, 66.5% of all patients with lung cancer were smokers, and 15.7% were smokers [15].
Accurate statistics on smoking have not been reported in Iran, but several studies have reported smoking statistics between 13% and 15% [16, 17]. Cigarette tax can significantly reduce its consumption and ASR lung cancer growth rate. In terms of the percentage of taxes allocated to the top cigarette brands, the United Kingdom, with an 82.16% tax rate, has the highest, and Iran, with a 4.83% tax rate, has the lowest cigarette tax, also the cigarette tax rate in Turkey is 82.13% and in the United States is 42.54%. In Turkey, cigarette sales have dropped significantly since 2010 due to increased cigarette taxes [18-20]. Due to the implementation of the plan to increase the smoking tax in recent years, there will not be much change in the growth chart of lung cancer so quickly. Lung cancer has also been on the rise in the United States since 1970, but with the tax rate increase of the top cigarette brands, the ASR rate of lung cancer has been declining since 2000. However, in Iran, the cigarette tax is smaller from all countries in the region except Afghanistan, and in recent years the tax rate has been declining [18]. The proposed policy is based on examining the impact of several different scenarios, according to which the application of items such as increasing the share of the budget for prevention and culture against smoking in the treatment budget, as well as increasing the price of cigarettes, can have favorable results in reducing mortality due to smoking and lung cancer [21]. Therefore, by following the example of successful countries in the field of legislation to increase the tax on cigarettes and the implementation of this program, Iran can significantly reduce smoking and, consequently, the increasing trend of lung cancer. In addition to taxes, timely and correct diagnosis of lung cancer can help substantially reduce the complications of the disease. Studies have found that more than 74% of people with lung cancer were diagnosed with stages 3 or 4 [22]. In the United Kingdom and the United States, there are programs and plans to increase the power of diagnosis and early diagnosis of the disease.
Lung cancer is the most common and deadly cancer in most countries. The most important problem concerning this cancer in Iran is the lack of accurate statistics on its prevalence and mortality. According to a recent recommendation by international organizations, including the American Cancer Society, the American College of Radiology, and the International Association for the Study of Lung Cancer (IASLC) in 2013, annual high-risk screening by low-risk dose CT is the most effective way to prevent death from lung cancer. Before implementing this program in the country, the cost-effectiveness of this project should be examined [23]. According to a study by Saba et al. (2016) on lung cancer in Iran, screening in the country will increase the number of early diagnoses 5 times [8]. Ghobadi et al. investigated the epidemiology of lung cancer and risk factors in one of the cities of Iran. This study showed that men were 4.6 times more likely than women to have lung cancer, and smoking was the most important risk factor for the disease [24].
Smoking is a health problem in developed and developing countries. Smoking increases the risk of lung cancer by 5 to 10 times with a clear dose-response relationship [25]. The geographical and temporal patterns of lung cancer and mortality at the population level are largely determined by tobacco use, a major cause of lung carcinogenesis worldwide [26]. In the United States, lung cancer incidence and mortality are declining due to decades of public education and tobacco control policies. However, lung cancer incidence and mortality are increasing in other parts of the world due to the onset of the tobacco epidemic in different countries and populations in developing countries. Smoking is the most common risk factor for lung cancer [27].
In the United States, efforts have been made since 2000 to replace old therapies, such as chemotherapy, with new ones, such as targeted therapies [28]. Rezaei et al. reported that the economic burden of lung cancer has been significant for the Iranian health system. Effective interventions in smoking cessation, early detection, strengthening of cancer prevention, and implementation of new cancer treatment and medical technology can compensate for some of the costs associated with lung cancer in Iran [29]. According to the national cancer registration report, there is a lack of facilities and diagnostic and sampling devices in some parts of Iran, resulting in problems accessing lung lesions, timely diagnosis, and unscientific recording of lung cancer statistics. So, it is recommended to model successful countries using new diagnostic methods and community-based education to familiarize the community with the early symptoms of lung cancer. These measures are effective in reducing the incidence of lung cancer.
Conclusion
The results of this study show that the incidence of lung cancer in Iran and Turkey is increasing, so following the example of successful countries in the implementation of tobacco tax programs, especially cigarettes can be shared taxes to the health sector, especially for preventive activity, such as implementing educational and cultural programs to reduce smoking and lung cancer screening, as well as new diagnostic methods for lung cancer.
Ethical Considerations
Compliance with ethical guidelines
This study is aaaproved by the Research Deputy of Zabol University of Medical Sciences (Code: IR.ZBMU.REC.1401.120).
Funding
This research was supported by the research project (No.: 401000291), funded by the Zabol University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all researchers in the field which studies were used in the current study.
References
- Etemadi A, Sadjadi A, Semnani S, Nouraie SM, Khademi H, Bahadori M. Cancer registry in Iran: A brief overview. Archives of Iranian Medicine. 2008; 11(5):577-80. [PMID]
- Mousavi SM, Gouya MM, Ramazani R, Davanlou M, Hajsadeghi N, Seddighi Z. Cancer incidence and mortality in Iran. Annals of Oncology. 2009; 20(3):556-63. [DOI:10.1093/annonc/mdn642] [PMID]
- Cabanes A, Vidal E, Aragonés N, Pérez-Gómez B, Pollán M,Lope V, et al. Cancer mortality trends in Spain: 1980-2007. Annals of Oncology. 2010; 21 (Suppl 3):iii14-20. [DOI:10.1093/
annonc/mdq089] [PMID] - Mehrabani D, Tabei SZ, Heydari ST, Shamsina SJ, Shokrpour N, Amini M, et al. Cancer occurrence in Fars province, southern Iran. Iranian Red Crescent Medical Journal. 2008; 10(4):314-22. [Link]
- Liu J, Hu Z, Feng Y, Zeng S, Zhong M. Problems to affect long-term survival for breast cancer patients: An observational study of subsequent lung/bronchus malignancies. Medicine. 2018; 97(39):e12603. [DOI:10.1097/MD.0000000000012603] [PMID] [PMCID]
- IARC. CancerMondial, International. Lyon: International Agency for Research on Cancer; 2008. [Link]
- Wender R, Fontham ET, Barrera E Jr, Colditz GA, Church TR, Ettinger DS, et al. American cancer society lung cancer screening guidelines. CA: A Cancer Journal for Clinicians. 2013; 63(2):107-17. [DOI:10.3322/caac.21172] [PMID] [PMCID]
- Saba V. [Estimation of age standardized ratio of lung cancer in Iran in 2014 and 2030 (Persian)]. Paramedical Sciences and Military Health. 2015; 10(1):17-23. [Link]
- Litvak M. Liberty and its boundaries vis-à-vis dissent and apostasy. In: Litvak M, editor. Know thy enemy. Leiden: Brill Publishing; 2021. [DOI:10.1163/9789004444683_007]
- Bray F. Age-standardization. In: Parkin DM, Whelan SL, Ferlay J, Teppo L, Thomas DB, editors. Cancer incidence in five continents. Geneva: World Health Organization; 2002. [Link]
- OECD. OECD Health Statistics 2021. Paris: Organisation for Economic Co-operation and Development; 2021. [Link]
- IHME. Global burden of disease [Internet]. 2019 [Updated 2021 July 17]. Available from: [Link]
- World Health Organization (WHO). Tobacco [Internet]. 2021 [Updated 2022 May 24]. Available from: [Link]
- Reitsma MB, Flor LS, Mullany EC, Gupta V, Hay SI, Gakidou E. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and initiation among young people in 204 countries and territories, 1990-2019. The Lancet Public Health. 2021; 6(7):e472-81. [DOI:10.1016/S2468-2667(21)00102-X] [PMID] [PMCID]
- Naghan PA, Hosseini M, Alinaghi SAS, Karimi S, Bahadori M, Khodadad K, et al. A clinicopathologic study of lung cancer cases in Iran. Tanaffos. 2009; 8(3):28-36. [Link]
- Meysamie A, Ghaletaki R, Zhand N, Abbasi M. Cigarette smoking in iran. Iranian Journal of Public Health. 2012; 41(2):1-14. [PMID] [PMCID]
- Moosazadeh M, Amiresmaili M, Afshari M. Individual patient data meta-analysis of the smoking prevalence in mazandaran province of iran. Iranian Red Crescent Medical Journal. 2015; 17(2):e10294. [DOI:10.5812/ircmj.10294] [PMID] [PMCID]
- World Health Organization (WHO). WHO report on the global tobacco epidemic, 2019: Offer help to quit tobacco use[Internet]. 2019 [Updated 2019 July 25]. Available from: [Link]
- Torre LA, Siegel RL, Jemal A. Lung cancer statistics. Advances in Experimental Medicine and Biology. 2016; 893:1-19. [DOI:10.1007/978-3-319-24223-1_1] [PMID]
- Bilir N, Çakır B, Dağlı E, Ergüder T, Önder Z. Tobacco control in Turkey. Denmark: World Health Organizatione; 2009. [Link]
- Park B, Kim Y, Lee J, Lee N, Jang SH. Sex difference and smoking effect of lung cancer incidence in Asian population. Cancers. 2020; 13(1):113. [DOI:10.3390/cancers13010113] [PMID] [PMCID]
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. International Journal of Cancer. 2010; 127(12):2893-917. [PMID]
- Wade S, Weber M, Caruana M, Kang YJ, Marshall H, Manser R, et al. Estimating the cost-effectiveness of lung cancer screening with low-dose computed tomography for high-risk smokers in Australia. Journal of Thoracic Oncology. 2018; 13(8):1094-105. [DOI:10.1016/j.jtho.2018.04.006] [PMID]
- Ghobadi H, Sharghi A, Sadat-Kermani J. [Epidemiology and risk factors for lung cancer in Ardabil, Iran (Persian)]. Journal of Ardabil University of Medical Sciences. 2013; 13(2):220-8. [Link]
- Schwartz AG, Cote ML. Epidemiology of lung cancer. Advances in Experimental Medicine and Biology. 2016; 893:21-41. [DOI:10.1007/978-3-319-24223-1_2] [PMID]
- Malhotra J, Malvezzi M, Negri E, La Vecchia C, Boffetta P. Risk factors for lung cancer worldwide. The European Respiratory Journal. 2016; 48(3):889-902. [DOI:10.1183/13993003.00359-2016] [PMID]
- De Groot PM, Wu CC, Carter BW, Munden RF. The epidemiology of lung cancer. Translational Lung Cancer Research. 2018; 7(3):220-33. [DOI:10.21037/tlcr.2018.05.06] [PMID] [PMCID]
- Roth JA, Goulart BH, Ravelo A, Kolkey H, Ramsey SD. Survival gains from first-line systemic therapy in metastatic non-small cell lung cancer in the U.S., 1990-2015: Progress and opportunities. The Oncologist. 2017; 22(3):304-10. [DOI:10.1634/theoncologist.2016-0253] [PMID] [PMCID]
- Rezaei S, Akbari Sari A, Woldemichael A, Soofi M, Kazemi A, Karami Matin B. Estimating the economic burden of lung cancer in Iran. Asian Pacific Journal of Cancer Prevention. 2016; 17(10):4729-33. [DOI:10.22034/APJCP.2016.17.10.4729] [PMID] [PMCID]
Article type: Original Research Articles |
Subject:
Social Welfare
Received: 2022/02/2 | Accepted: 2023/03/14 | Published: 2023/06/7
Received: 2022/02/2 | Accepted: 2023/03/14 | Published: 2023/06/7
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
