
988368
Wed, May 27, 2026

Volume 22, Issue 2 (June 2024)
Iranian Rehabilitation Journal 2024, 22(2): 295-306 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Siddiq A, Kumar. I N. Physiotherapists' Pain Beliefs and Treatment Selection for Low Back Pain: A Cross-sectional Study. Iranian Rehabilitation Journal 2024; 22 (2) :295-306
URL: http://irj.uswr.ac.ir/article-1-1914-en.html
URL: http://irj.uswr.ac.ir/article-1-1914-en.html



1- Department of Physiotherapy, Faculty of Allied Health and Basic Sciences, Sri Devaraj URS Academy of Higher Education and Research, Kolar, India.
Full-Text [PDF 882 kb]
(1316 Downloads)
| Abstract (HTML) (3375 Views)
Full-Text: (711 Views)
Introduction
Chronic low back ache constitutes a significant public health crisis worldwide [1, 2]. It is the leading cause of absenteeism from work and limits participation in daily activities [3–5]. Chronic low back pain (CLBP) is characterized by pain or discomfort in the lower part of the trunk and gluteus region that can sometimes extend to the legs and last for >12 weeks [6]. This type of pain is considered non-specific if the causes cannot be identified. CLBP places a significant financial burden on the healthcare system and patients often feel ignored and misunderstood by healthcare professionals [7, 8].
The biomedical model has been the traditional approach to treating CLBP; however, a recent comprehensive review revealed a negative correlation between this approach and patient education, treatment adherence, and reported work and activity recommendations.
Contrastingly, the bio-psychosocial approach underscores the significance of social and psychological factors in the onset and persistence of chronic pain [9–12].
The rehabilitation of individuals dealing with chronic pain is intricately influenced by psychosocial factors, encompassing cognitive, emotional and social aspects [13]. These factors can be divided into work-related and non-work-related factors and are linked to a higher incidence of chronic pain [14]. Guidelines for clinical practice in the UK and Italy about low back pain recommend the inclusion of psychosocial factors in the comprehensive assessment and treatment of patients grappling with CLBP [15, 16].
Even though the significance of psychosocial factors in addressing CLBP is acknowledged, integrating these elements into clinical practice poses a challenge for some therapists [17]. Individuals experiencing elevated pain-related fears often hold the belief that engaging in physical activity will exacerbate their pain and constrain their daily functioning [18]. Such beliefs have the potential to forecast disability in both daily and occupational activities, impact treatment outcomes, and influence the ability to return to work.
Previous studies reported that the treatment selection for CLBP is not solely influenced by physiotherapists’ fear-avoidance beliefs but is instead influenced by various factors, such as their understanding of pain, education, and other individual and environmental factors [19, 20]. Accordingly, this study discerns the beliefs and attitudes of Indian physiotherapists regarding the choice of treatments for low back pain and its correlation with the selected models of pain.
Materials and Methods
Study design
This research adopted a cross-sectional design to evaluate the attitudes and beliefs of physiotherapists concerning non-specific chronic low back pain (NSCLBP). Approval for the study was obtained from the University Ethics Committee.
Sample size
A total of 107 participants were included in the study, selected through a statistical power of 85%, a 95% confidence interval (CI) and a population size of 50 000 people with a margin of error of 10%.
Study participants
The participants comprised intern students and graduated physiotherapists engaged in either clinical settings (such as hospitals, clinics and rehabilitation centers) or academic settings (such as universities and colleges) in India. Intern students were incorporated to explore whether their beliefs about low back pain were formed during their education or post-graduation.
Exclusion criteria
Physiotherapists who were not working in clinical or hospital settings, who had not treated patients with lower back pain for the past 2 years, and who were not exposed to patients with lower back pain were excluded from the study. Similarly, undergraduate students before their internship were also excluded from the study.
Study procedure
The study design was presented in a departmental expert review meeting and comments were obtained for correction. The questionnaire was distributed through a Google Form to physiotherapist contacts via social media platforms, e-mail, WhatsApp, etc. on 2020/06/20. The description of the study and the patient’s consent were included in the Google Form. The participants were given 20 days to respond to the form, and two reminders were sent after 7 days to ensure maximum response. The response to the Google Form was closed after 20 days (2022/07/10) and the data was extracted from the form in an Excel format for statistical analysis.
Data collection
The Google Form was structured into three distinct sections as follows:
Demographic information
The demographic information segment encompassed eight items, extracting information about the participant’s gender, age, nationality, highest educational level, primary work setting, work category, years of experience, and whether they had received specialized training in treating low back pain.
Physiotherapist pain attitude and belief scale
The physiotherapist pain attitude and belief scale (PABS-PT) as a validated questionnaire was employed to gauge physiotherapists’ attitudes and beliefs about pain management. The reliability of the PABS-PT was established through high internal consistency and robust test-retest reliability. Its validity was substantiated by content validity through expert review and construct validity through significant correlations with measures of pain-related fear and disability. Discriminant validity was confirmed through notable differences observed between physiotherapists with varying levels of experience and training [21–23].
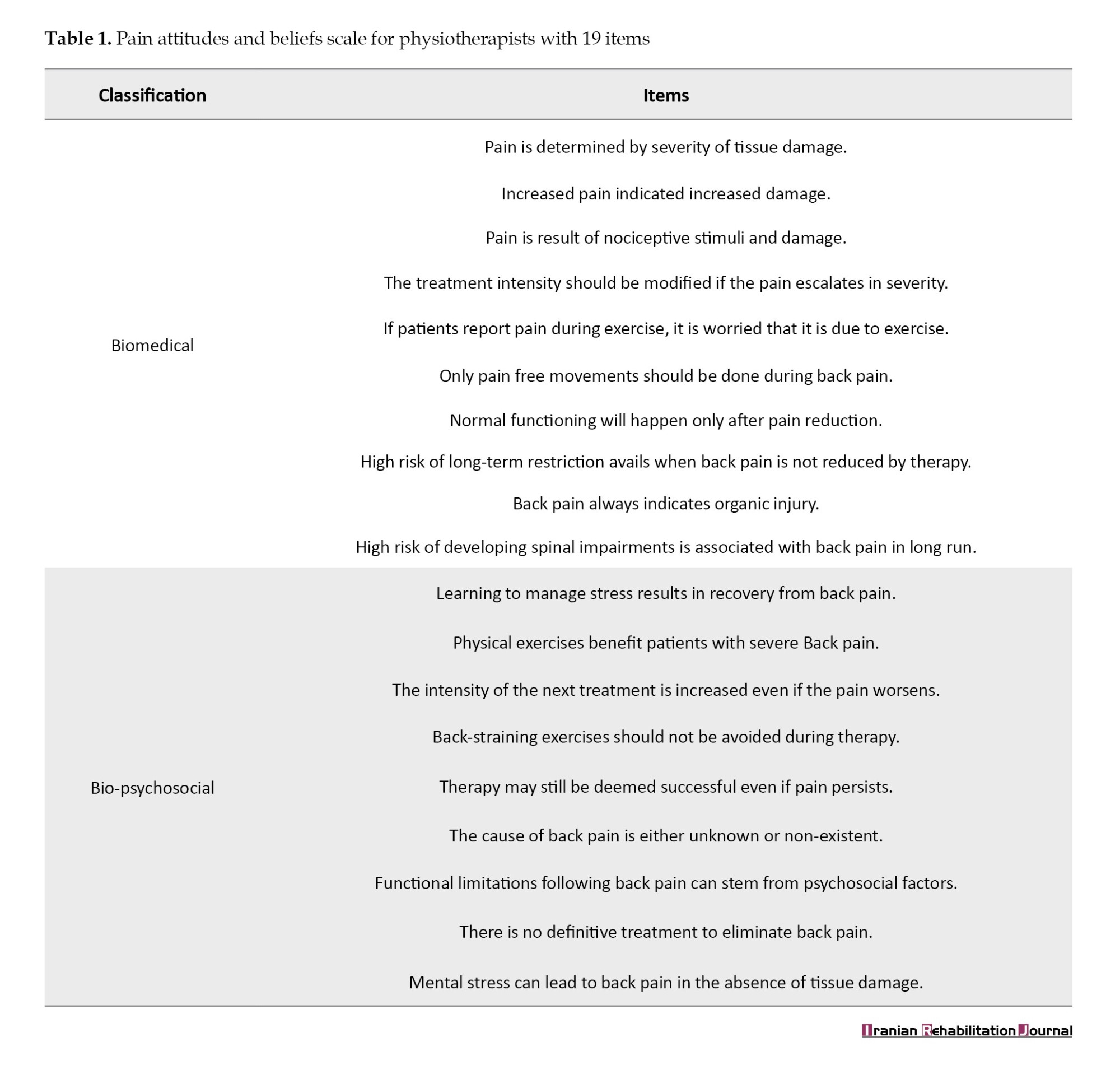
In this part, the participants’ attitudes toward NSCLBP and their comprehension of pain were assessed using PABS-PT. The PABS-PT instrument comprised 19 items graded on a 6-point Likert scale (ranging from completely agree=1 to entirely disagree=6) and explores two factors as follows: A focus on biomedical treatment and a focus on bio-psychosocial treatment. The maximum total score for the bio-psychosocial treatment orientation was set at 54, while the maximum total score for the entire PABS-PT instrument was 114. Specifically, the biomedical treatment orientation section encompassed 10 questions with a maximum total score of 60 (Table 1).
Treatment selection
The final segment of the questionnaire delved into the most frequently employed physiotherapy treatments for NSCLBP. The provided treatment options encompassed bed rest, lumbar support, electrotherapy (e.g. transcutaneous electrical nerve stimulation, ultrasound, laser), hydrotherapy, hot/cold therapy, spinal traction, spinal mobilization/manipulation, specific back exercises (e.g. strengthening, flexibility, range of motion, etc.), home exercises, physical activity-based interventions (e.g. walking), pain coping skill training, cognitive functional therapy, mechanical diagnosis and treatment (McKenzie Method), treatment-based classification approach and pathoanatomy-based interventions.
Statistical analysis
The data collected via the Google Form underwent analysis using the SPSS software, version 26. Descriptive statistics were employed to assess participants’ characteristics within their responses. The Mean±SD of PABS-PT were computed. The Pearson correlation coefficient was determined to evaluate the relationship between the PABS-PT biomedical and bio-psychosocial subscales. Logistic regression analysis was conducted to identify associations between participant characteristics and PABS-PT scores, treatment selection and PABS-PT scores and participant characteristics, with a 95% CI. A significance level of P<0.05 was adopted to establish the statistical significance of the results.
Results
The study garnered a total of 107 responses from Indian physiotherapists via a Google Form. The observed treatment orientation revealed 43.4% biomedical and 30.7% bio-psychosocial, indicating a predominant biomedical focus in the clinical practices of physiotherapists in India. Accordingly, bio-psychosocial scores were found to be comparatively low.
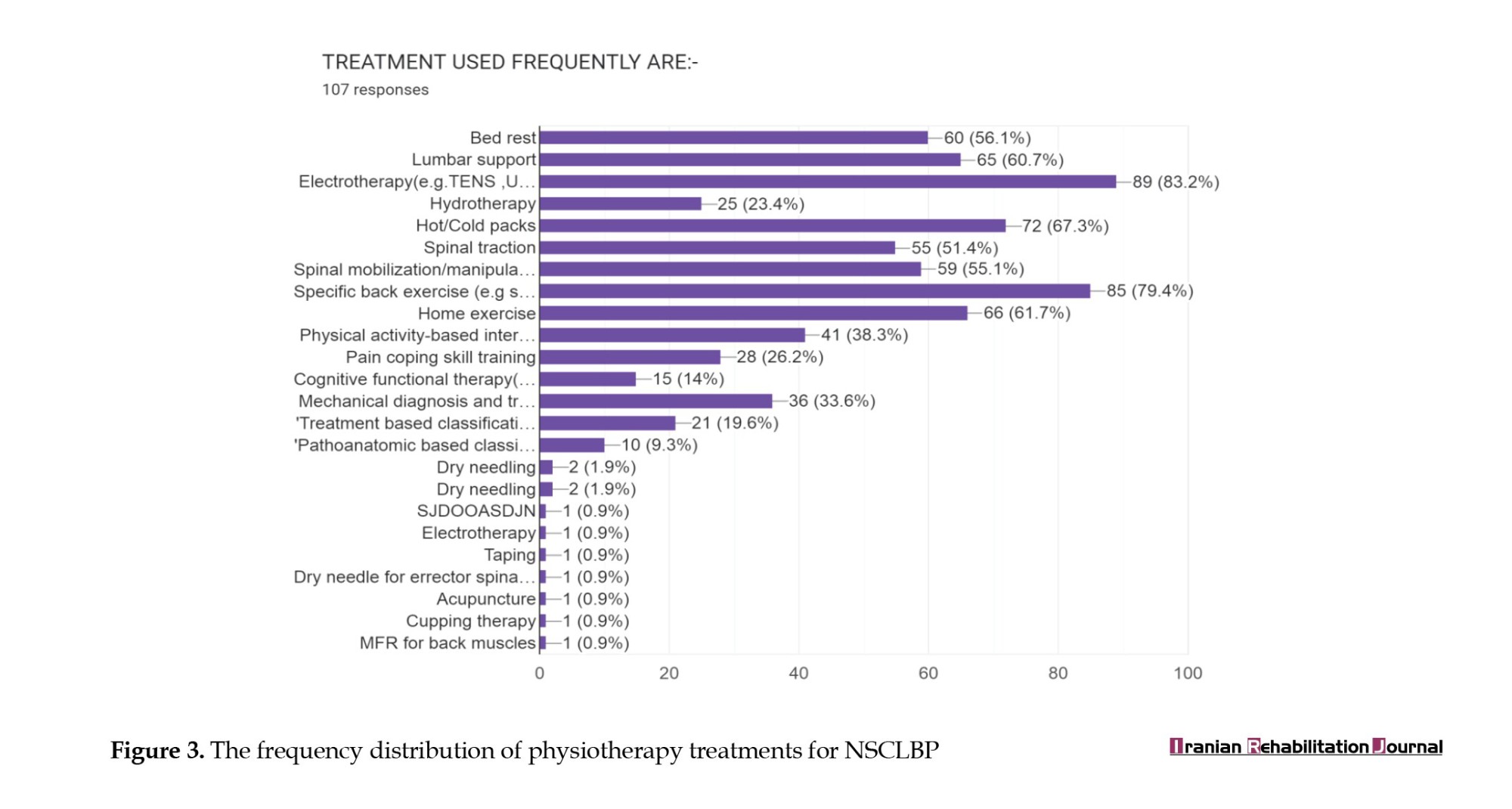
Among the frequently used treatments, electrotherapy (84%), specific back exercises (81%), hot/cold packs (70%), home exercises (63%), lumbar support (62%), spinal mobilization (57%), bed rest (56%), and spinal traction (52%) emerged as the most common. Conversely, pain coping skills (27%), hydrotherapy (24%), pathoanatomic-based classification (9%) and dry needling (2%) were less frequently employed.
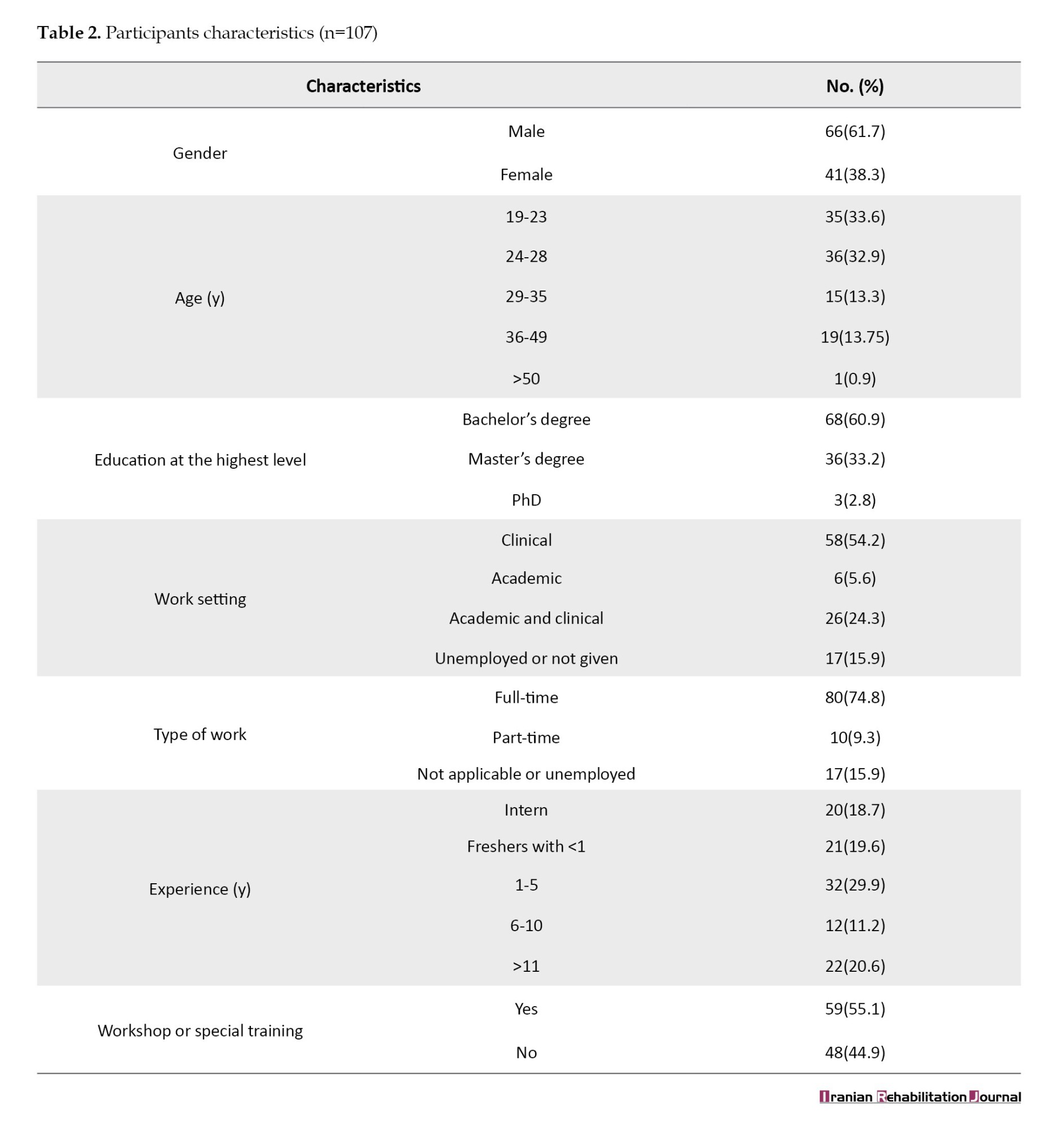
In terms of participant characteristics, 61.7% were male, and 38.3% were female. The majority fell within the age range of 24-28 years, with over 60% holding a bachelor’s degree in physiotherapy and 33.2% possessing a master’s degree. A significant portion worked in a clinical setting (54.2%), while only 5.6% were in an academic setting. The majority were full-time workers (74.8%), with 29.9% having 1-5 years of experience. More than half had received specialized training or workshops in the treatment of low back pain (Table 2).
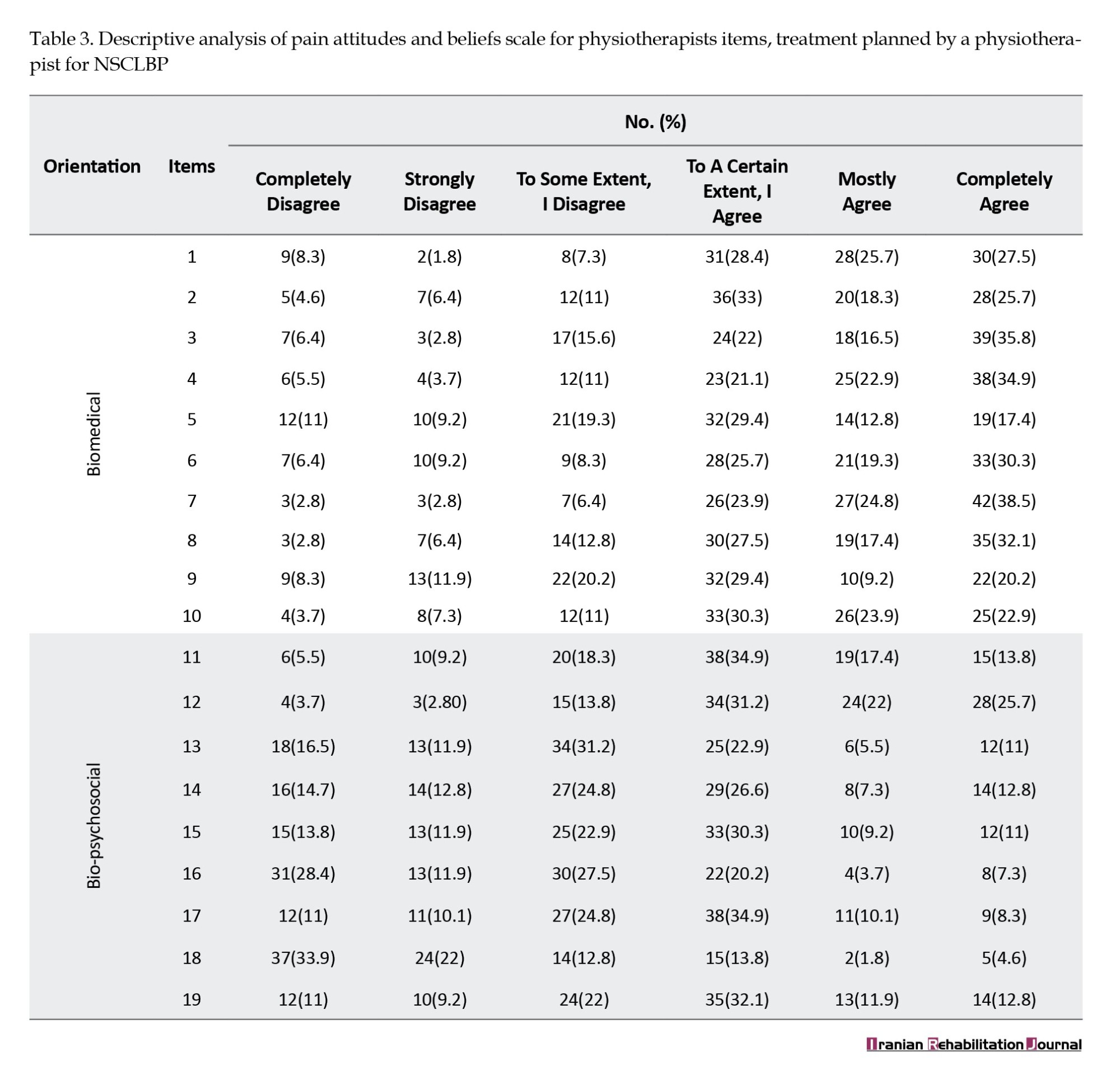
The Mean±SD score for biomedical treatment orientation was 43.49±1.3 and the Mean±SD score for bio-psychosocial treatment orientation was 30.7±1.3, resulting in a combined mean score of 74.09 (Table 3).
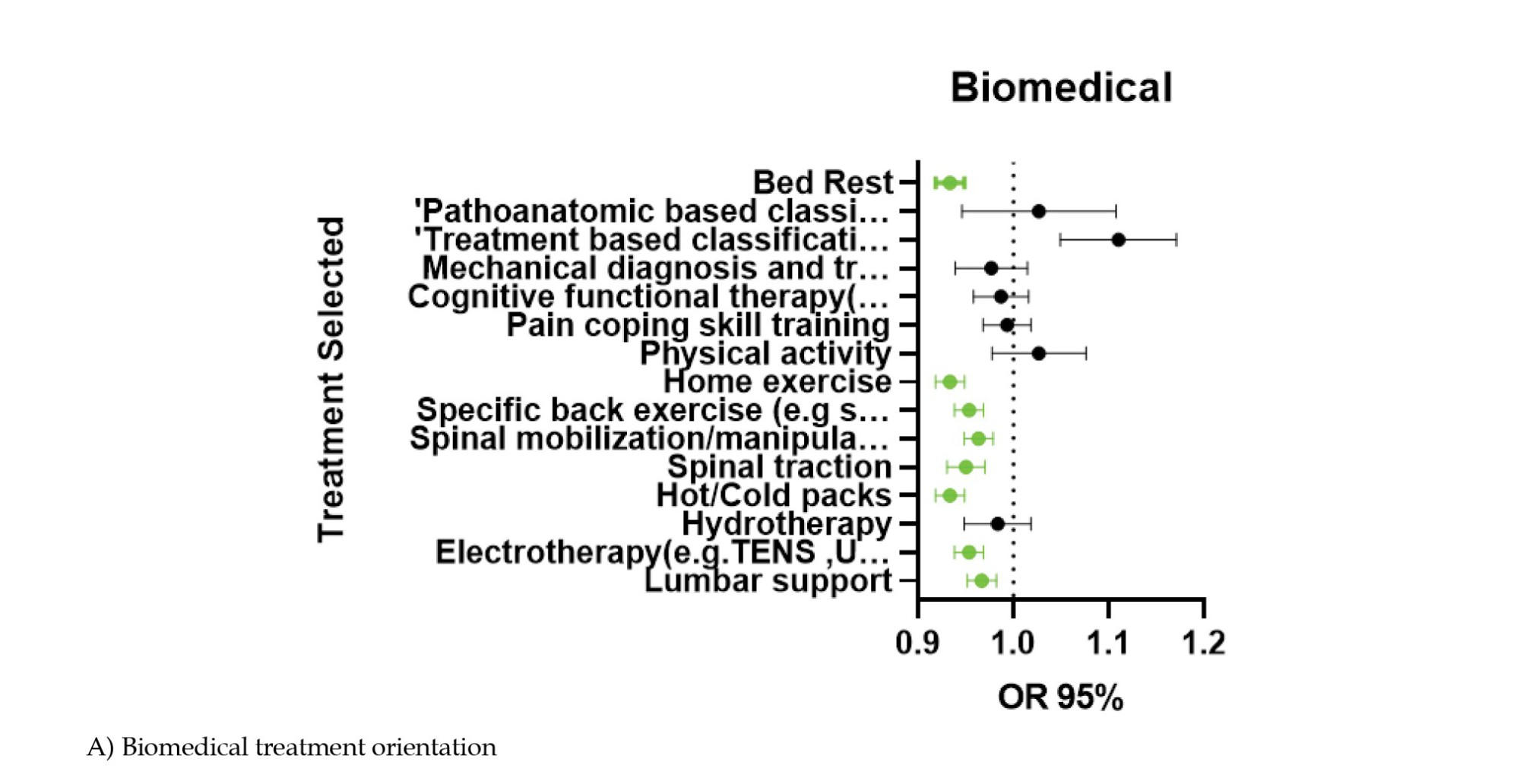
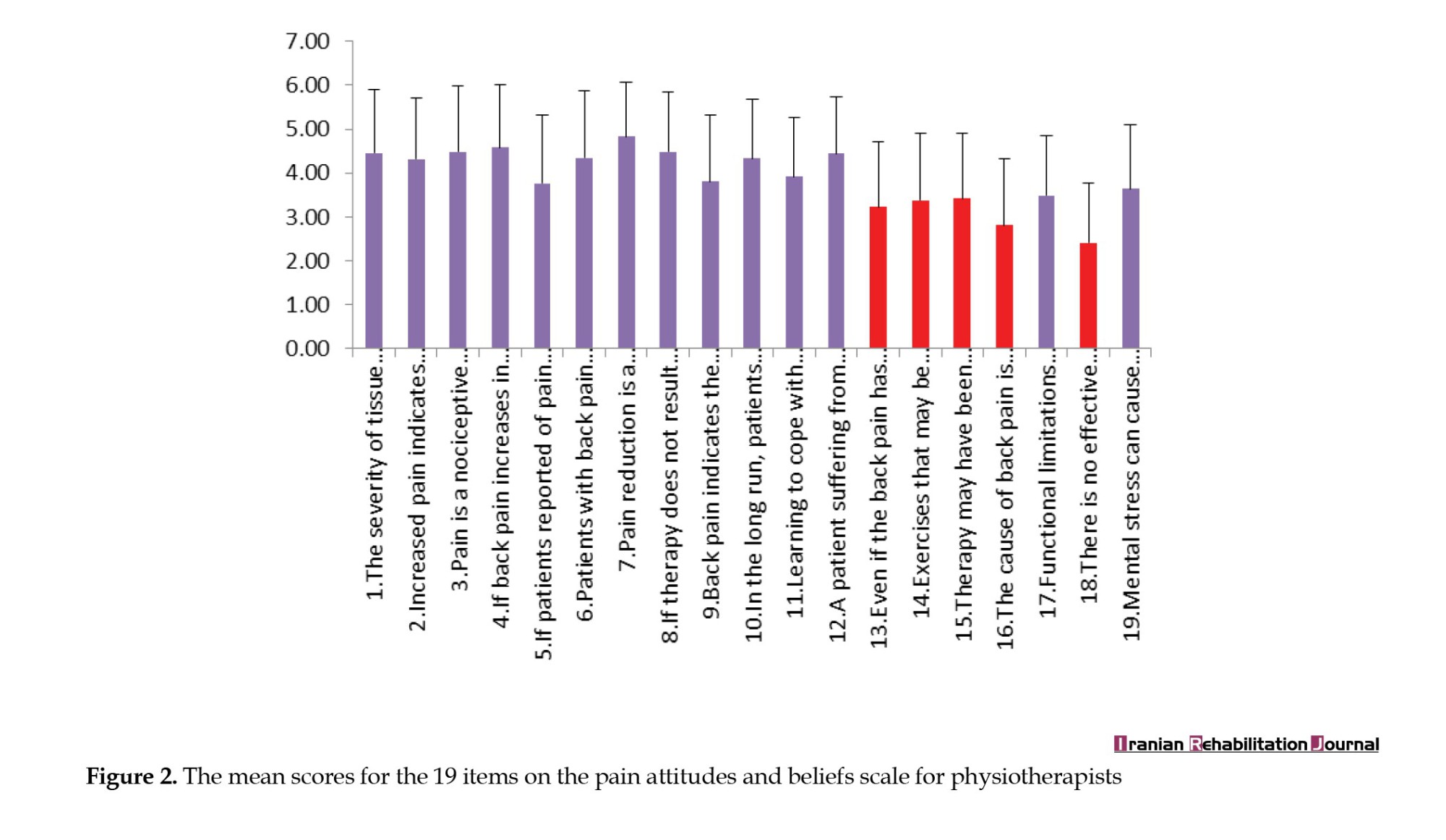
The three PABS-PT items with the lowest mean scores pertained to bio-psychosocial treatment orientation. Correlations were identified between physiotherapists’ PABS-PT scores and their treatment selection (Tables 4 and 5), indicating that a stronger biomedical orientation led to the use of specialized back exercises, bed rest, lumbar support, electrotherapy, hot/cold packs, spinal traction, and home exercises.
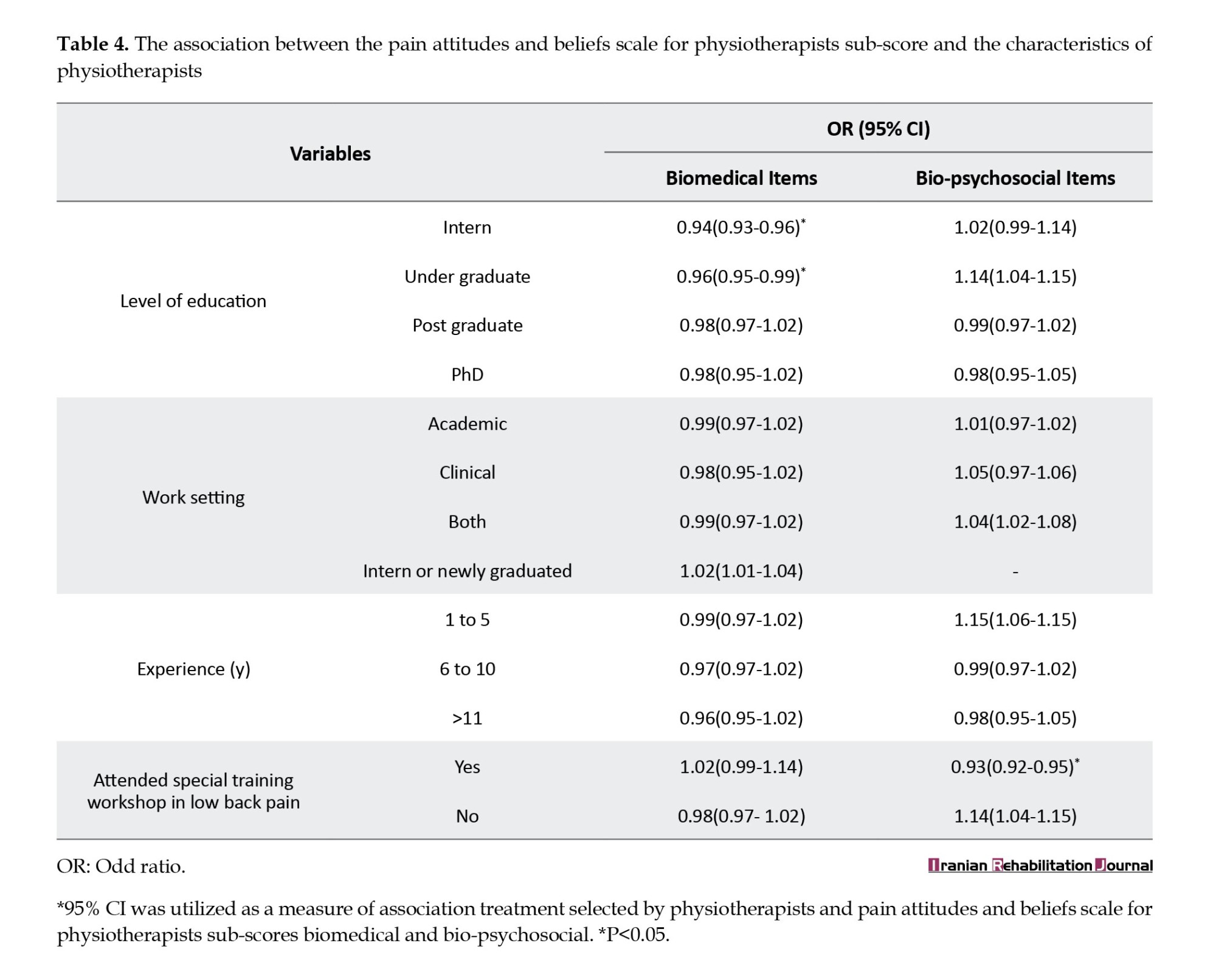
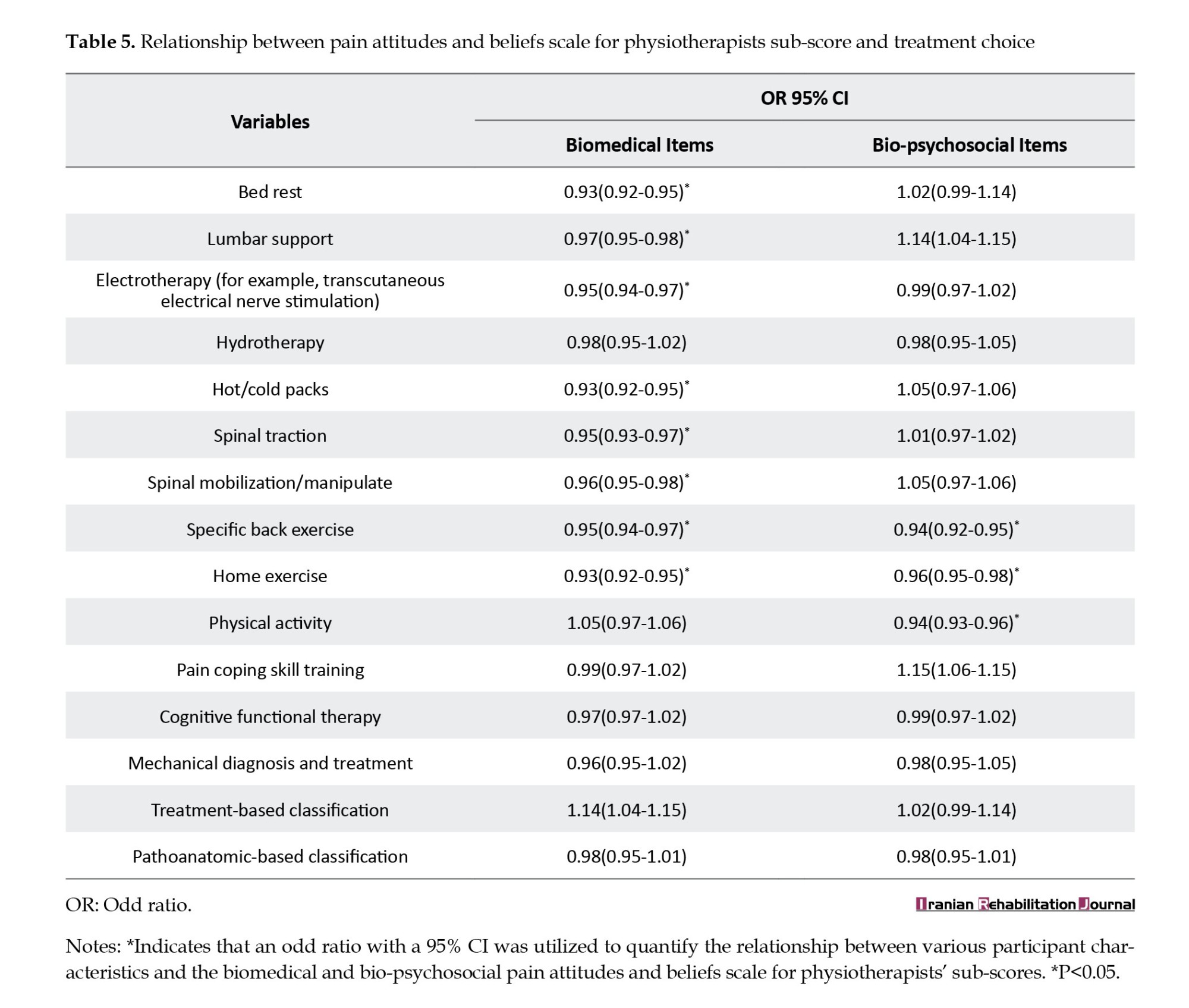
Conversely, a stronger bio-psychosocial orientation was associated with greater utilization of targeted back exercises, at-home exercises and activity-based interventions. Further correlations were found between participant characteristics and PABS-PT sub-scores, with interns and graduated physiotherapists scoring higher in biomedical treatment orientation, and those who attended special training or workshops in managing low back pain scoring higher in bio-psychosocial treatment orientation (Figure 1).

Discussion
The primary objective of this study was to delve into the attitudes and beliefs held by Indian physiotherapists concerning the management of NSCLBP. Additionally, this study uncovered the intricate relationship between these attitudes and the specific treatments chosen for addressing NSCLBP. Results from the 107 responses received showed that a majority of participants were male, as shown in Figure 2 and Table 2. The majority of participants agreed on all questions related to the biomedical orientation, while they disagreed on the bio-psychosocial model.
The most commonly used physiotherapy treatments for NSCLBP were found to be electrotherapy, specific back exercises, hot/cold packs, bed rest, spinal traction and spinal mobilization. A robust correlation was observed between the scores on PABS-PT and the participants’ characteristics. Meanwhile, recently graduated and intern physiotherapists exhibited a higher proficiency in biomedical treatment orientation when compared to their counterparts who had undergone specialized training in the treatment of low back pain (Figure 3).
The findings of this study align closely with previous research conducted in various countries, including the UK, Canada, and New Zealand. In those studies, the mean scores for the biomedical and bio-psychosocial subscales were consistently reflected at 30.7 and 43.4, respectively, showcasing a level of consistency across different geographical contexts [9, 20–22]. However, other studies reported slightly different findings, with some studies reporting a higher score for the bio-psychosocial subscale and a lower score for the biomedical subscale. The relationship between the participant’s physiotherapist-specific traits and their biological or bio-psychosocial orientation was investigated in previous studies, with some finding a substantial correlation between the adoption of the biomedical method in the treatment of NSCLBP and the gender and level of expertise of the physiotherapists [23, 24]. In the current study, no significant relationship was uncovered between the bio-psychosocial and biological approaches and participant variables such as sex, age, and years of experience. However, a notable exception emerged, indicating that individuals who had attended a specialized training or workshop in managing low back pain exhibited higher scores about the bio-psychosocial therapeutic orientation.
The results of this study diverged from prior research in terms of the approaches employed by physiotherapists for treating low back pain. Physiotherapists in India exhibited a higher inclination toward treatments like electrotherapy, targeted back exercises, bed rest, and spinal traction. In contrast, physiotherapists in other countries, such as New Zealand and Brazil, tended to favor different therapeutic modalities like spinal mobilization, postural counseling, global posture reeducation, and osteopathy.
The study’s strengths lie in being the inaugural examination of physiotherapists’ beliefs and attitudes and their correlation with the selected treatments in India. Additionally, the use of the PABS-PT survey showcased a commendable level of reliability in assessing physiotherapists’ attitudes and beliefs regarding low back pain. However, it is essential to acknowledge certain limitations, including the use of convenience sampling, which may not accurately represent the entirety of the physiotherapy population.
Conclusion
This study discerned that the attitudes and beliefs of physiotherapists in India regarding NSCLBP predominantly lean toward biomedical aspects. This underscores a potential necessity for additional education and training in the bio-psychosocial approach to pain management, potentially resulting in enhanced treatment outcomes and heightened patient satisfaction. Subsequent research endeavors are warranted to delve deeper into these factors and formulate effective strategies for fostering a more comprehensive approach to pain management among physiotherapists in India.
Ethical Considerations
Compliance with ethical guidelines
This research was approved by the Ethical Committee of Sri Devaraj URS Academy of Higher Education and Research (Code: DMC/KLR/IEC/92/2022-23).
Funding
The paper was extracted from the BPT thesis of Ayeesha Siddiq, approved by Department of Physiotherapy, Faculty of Allied Health and Basic Sciences, Sri Devaraj URS Academy of Higher Education and Research.
Authors' contributions
Data collection, data analysis, methodology, writing and final approval: All authors; Study design: Ayeesha Siddiq; Conceptualization, supervision, interpretation: Naveen Kumar.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their appreciation to Sri Devaraj Urs Academy of Higher Education and Research for the support and facilities that facilitated the execution of this study. Additionally, heartfelt gratitude is expressed to the participating physiotherapists whose valuable contributions played a pivotal role in advancing this research.
References
Chronic low back ache constitutes a significant public health crisis worldwide [1, 2]. It is the leading cause of absenteeism from work and limits participation in daily activities [3–5]. Chronic low back pain (CLBP) is characterized by pain or discomfort in the lower part of the trunk and gluteus region that can sometimes extend to the legs and last for >12 weeks [6]. This type of pain is considered non-specific if the causes cannot be identified. CLBP places a significant financial burden on the healthcare system and patients often feel ignored and misunderstood by healthcare professionals [7, 8].
The biomedical model has been the traditional approach to treating CLBP; however, a recent comprehensive review revealed a negative correlation between this approach and patient education, treatment adherence, and reported work and activity recommendations.
Contrastingly, the bio-psychosocial approach underscores the significance of social and psychological factors in the onset and persistence of chronic pain [9–12].
The rehabilitation of individuals dealing with chronic pain is intricately influenced by psychosocial factors, encompassing cognitive, emotional and social aspects [13]. These factors can be divided into work-related and non-work-related factors and are linked to a higher incidence of chronic pain [14]. Guidelines for clinical practice in the UK and Italy about low back pain recommend the inclusion of psychosocial factors in the comprehensive assessment and treatment of patients grappling with CLBP [15, 16].
Even though the significance of psychosocial factors in addressing CLBP is acknowledged, integrating these elements into clinical practice poses a challenge for some therapists [17]. Individuals experiencing elevated pain-related fears often hold the belief that engaging in physical activity will exacerbate their pain and constrain their daily functioning [18]. Such beliefs have the potential to forecast disability in both daily and occupational activities, impact treatment outcomes, and influence the ability to return to work.
Previous studies reported that the treatment selection for CLBP is not solely influenced by physiotherapists’ fear-avoidance beliefs but is instead influenced by various factors, such as their understanding of pain, education, and other individual and environmental factors [19, 20]. Accordingly, this study discerns the beliefs and attitudes of Indian physiotherapists regarding the choice of treatments for low back pain and its correlation with the selected models of pain.
Materials and Methods
Study design
This research adopted a cross-sectional design to evaluate the attitudes and beliefs of physiotherapists concerning non-specific chronic low back pain (NSCLBP). Approval for the study was obtained from the University Ethics Committee.
Sample size
A total of 107 participants were included in the study, selected through a statistical power of 85%, a 95% confidence interval (CI) and a population size of 50 000 people with a margin of error of 10%.
Study participants
The participants comprised intern students and graduated physiotherapists engaged in either clinical settings (such as hospitals, clinics and rehabilitation centers) or academic settings (such as universities and colleges) in India. Intern students were incorporated to explore whether their beliefs about low back pain were formed during their education or post-graduation.
Exclusion criteria
Physiotherapists who were not working in clinical or hospital settings, who had not treated patients with lower back pain for the past 2 years, and who were not exposed to patients with lower back pain were excluded from the study. Similarly, undergraduate students before their internship were also excluded from the study.
Study procedure
The study design was presented in a departmental expert review meeting and comments were obtained for correction. The questionnaire was distributed through a Google Form to physiotherapist contacts via social media platforms, e-mail, WhatsApp, etc. on 2020/06/20. The description of the study and the patient’s consent were included in the Google Form. The participants were given 20 days to respond to the form, and two reminders were sent after 7 days to ensure maximum response. The response to the Google Form was closed after 20 days (2022/07/10) and the data was extracted from the form in an Excel format for statistical analysis.
Data collection
The Google Form was structured into three distinct sections as follows:
Demographic information
The demographic information segment encompassed eight items, extracting information about the participant’s gender, age, nationality, highest educational level, primary work setting, work category, years of experience, and whether they had received specialized training in treating low back pain.
Physiotherapist pain attitude and belief scale
The physiotherapist pain attitude and belief scale (PABS-PT) as a validated questionnaire was employed to gauge physiotherapists’ attitudes and beliefs about pain management. The reliability of the PABS-PT was established through high internal consistency and robust test-retest reliability. Its validity was substantiated by content validity through expert review and construct validity through significant correlations with measures of pain-related fear and disability. Discriminant validity was confirmed through notable differences observed between physiotherapists with varying levels of experience and training [21–23].
In this part, the participants’ attitudes toward NSCLBP and their comprehension of pain were assessed using PABS-PT. The PABS-PT instrument comprised 19 items graded on a 6-point Likert scale (ranging from completely agree=1 to entirely disagree=6) and explores two factors as follows: A focus on biomedical treatment and a focus on bio-psychosocial treatment. The maximum total score for the bio-psychosocial treatment orientation was set at 54, while the maximum total score for the entire PABS-PT instrument was 114. Specifically, the biomedical treatment orientation section encompassed 10 questions with a maximum total score of 60 (Table 1).
Treatment selection
The final segment of the questionnaire delved into the most frequently employed physiotherapy treatments for NSCLBP. The provided treatment options encompassed bed rest, lumbar support, electrotherapy (e.g. transcutaneous electrical nerve stimulation, ultrasound, laser), hydrotherapy, hot/cold therapy, spinal traction, spinal mobilization/manipulation, specific back exercises (e.g. strengthening, flexibility, range of motion, etc.), home exercises, physical activity-based interventions (e.g. walking), pain coping skill training, cognitive functional therapy, mechanical diagnosis and treatment (McKenzie Method), treatment-based classification approach and pathoanatomy-based interventions.
Statistical analysis
The data collected via the Google Form underwent analysis using the SPSS software, version 26. Descriptive statistics were employed to assess participants’ characteristics within their responses. The Mean±SD of PABS-PT were computed. The Pearson correlation coefficient was determined to evaluate the relationship between the PABS-PT biomedical and bio-psychosocial subscales. Logistic regression analysis was conducted to identify associations between participant characteristics and PABS-PT scores, treatment selection and PABS-PT scores and participant characteristics, with a 95% CI. A significance level of P<0.05 was adopted to establish the statistical significance of the results.
Results
The study garnered a total of 107 responses from Indian physiotherapists via a Google Form. The observed treatment orientation revealed 43.4% biomedical and 30.7% bio-psychosocial, indicating a predominant biomedical focus in the clinical practices of physiotherapists in India. Accordingly, bio-psychosocial scores were found to be comparatively low.
Among the frequently used treatments, electrotherapy (84%), specific back exercises (81%), hot/cold packs (70%), home exercises (63%), lumbar support (62%), spinal mobilization (57%), bed rest (56%), and spinal traction (52%) emerged as the most common. Conversely, pain coping skills (27%), hydrotherapy (24%), pathoanatomic-based classification (9%) and dry needling (2%) were less frequently employed.
In terms of participant characteristics, 61.7% were male, and 38.3% were female. The majority fell within the age range of 24-28 years, with over 60% holding a bachelor’s degree in physiotherapy and 33.2% possessing a master’s degree. A significant portion worked in a clinical setting (54.2%), while only 5.6% were in an academic setting. The majority were full-time workers (74.8%), with 29.9% having 1-5 years of experience. More than half had received specialized training or workshops in the treatment of low back pain (Table 2).
The Mean±SD score for biomedical treatment orientation was 43.49±1.3 and the Mean±SD score for bio-psychosocial treatment orientation was 30.7±1.3, resulting in a combined mean score of 74.09 (Table 3).
The three PABS-PT items with the lowest mean scores pertained to bio-psychosocial treatment orientation. Correlations were identified between physiotherapists’ PABS-PT scores and their treatment selection (Tables 4 and 5), indicating that a stronger biomedical orientation led to the use of specialized back exercises, bed rest, lumbar support, electrotherapy, hot/cold packs, spinal traction, and home exercises.
Conversely, a stronger bio-psychosocial orientation was associated with greater utilization of targeted back exercises, at-home exercises and activity-based interventions. Further correlations were found between participant characteristics and PABS-PT sub-scores, with interns and graduated physiotherapists scoring higher in biomedical treatment orientation, and those who attended special training or workshops in managing low back pain scoring higher in bio-psychosocial treatment orientation (Figure 1).
Discussion
The primary objective of this study was to delve into the attitudes and beliefs held by Indian physiotherapists concerning the management of NSCLBP. Additionally, this study uncovered the intricate relationship between these attitudes and the specific treatments chosen for addressing NSCLBP. Results from the 107 responses received showed that a majority of participants were male, as shown in Figure 2 and Table 2. The majority of participants agreed on all questions related to the biomedical orientation, while they disagreed on the bio-psychosocial model.
The most commonly used physiotherapy treatments for NSCLBP were found to be electrotherapy, specific back exercises, hot/cold packs, bed rest, spinal traction and spinal mobilization. A robust correlation was observed between the scores on PABS-PT and the participants’ characteristics. Meanwhile, recently graduated and intern physiotherapists exhibited a higher proficiency in biomedical treatment orientation when compared to their counterparts who had undergone specialized training in the treatment of low back pain (Figure 3).
The findings of this study align closely with previous research conducted in various countries, including the UK, Canada, and New Zealand. In those studies, the mean scores for the biomedical and bio-psychosocial subscales were consistently reflected at 30.7 and 43.4, respectively, showcasing a level of consistency across different geographical contexts [9, 20–22]. However, other studies reported slightly different findings, with some studies reporting a higher score for the bio-psychosocial subscale and a lower score for the biomedical subscale. The relationship between the participant’s physiotherapist-specific traits and their biological or bio-psychosocial orientation was investigated in previous studies, with some finding a substantial correlation between the adoption of the biomedical method in the treatment of NSCLBP and the gender and level of expertise of the physiotherapists [23, 24]. In the current study, no significant relationship was uncovered between the bio-psychosocial and biological approaches and participant variables such as sex, age, and years of experience. However, a notable exception emerged, indicating that individuals who had attended a specialized training or workshop in managing low back pain exhibited higher scores about the bio-psychosocial therapeutic orientation.
The results of this study diverged from prior research in terms of the approaches employed by physiotherapists for treating low back pain. Physiotherapists in India exhibited a higher inclination toward treatments like electrotherapy, targeted back exercises, bed rest, and spinal traction. In contrast, physiotherapists in other countries, such as New Zealand and Brazil, tended to favor different therapeutic modalities like spinal mobilization, postural counseling, global posture reeducation, and osteopathy.
The study’s strengths lie in being the inaugural examination of physiotherapists’ beliefs and attitudes and their correlation with the selected treatments in India. Additionally, the use of the PABS-PT survey showcased a commendable level of reliability in assessing physiotherapists’ attitudes and beliefs regarding low back pain. However, it is essential to acknowledge certain limitations, including the use of convenience sampling, which may not accurately represent the entirety of the physiotherapy population.
Conclusion
This study discerned that the attitudes and beliefs of physiotherapists in India regarding NSCLBP predominantly lean toward biomedical aspects. This underscores a potential necessity for additional education and training in the bio-psychosocial approach to pain management, potentially resulting in enhanced treatment outcomes and heightened patient satisfaction. Subsequent research endeavors are warranted to delve deeper into these factors and formulate effective strategies for fostering a more comprehensive approach to pain management among physiotherapists in India.
Ethical Considerations
Compliance with ethical guidelines
This research was approved by the Ethical Committee of Sri Devaraj URS Academy of Higher Education and Research (Code: DMC/KLR/IEC/92/2022-23).
Funding
The paper was extracted from the BPT thesis of Ayeesha Siddiq, approved by Department of Physiotherapy, Faculty of Allied Health and Basic Sciences, Sri Devaraj URS Academy of Higher Education and Research.
Authors' contributions
Data collection, data analysis, methodology, writing and final approval: All authors; Study design: Ayeesha Siddiq; Conceptualization, supervision, interpretation: Naveen Kumar.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their appreciation to Sri Devaraj Urs Academy of Higher Education and Research for the support and facilities that facilitated the execution of this study. Additionally, heartfelt gratitude is expressed to the participating physiotherapists whose valuable contributions played a pivotal role in advancing this research.
References
- Freburger JK, Holmes GM, Agans RP, Jackman AM, Darter JD, Wallace AS, et al. The rising prevalence of chronic low back pain. Archives of Internal Medicine. 2009; 169(3):251-8. [PMID]
- Wu A, March L, Zheng X, Huang J, Wang X, Zhao J, et al. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the Global Burden of Disease Study 2017. Annals of Translational Medicine. 2020; 8(6):299. [DOI:10.21037/atm.2020.02.175] [PMID]
- Kääriä S, Kaila-Kangas L, Kirjonen J, Riihimäki H, Luukkonen R, Leino-Arjas P. Low back pain, work absenteeism, chronic back disorders, and clinical findings in the low back as predictors of hospitalization due to low back disorders: A 28-year follow-up of industrial employees. Spine. 2005; 30(10):1211-8. [DOI:10.1097/01.brs.0000162283.95342.b5] [PMID]
- Vassilaki M, Hurwitz EL. Insights in public health: Perspectives on pain in the low back and neck: Global burden, epidemiology, and management. Hawai'i Journal of Medicine & Public Health. 2014; 73(4):122-6. [PMID]
- Serranheira F, Sousa-Uva M, Heranz F, Kovacs F, Sousa-Uva A. Low Back Pain (LBP), work and absenteeism. Work. 2020; 65(2):463-9. [DOI:10.3233/WOR-203073] [PMID]
- Allegri M, Montella S, Salici F, Valente A, Marchesini M, Compagnone C, et al. Mechanisms of low back pain: A guide for diagnosis and therapy. F1000Research. 2016; 5:F1000 Faculty Rev-1530. [DOI:10.12688/f1000research.8105.2] [PMID]
- Gore M, Sadosky A, Stacey BR, Tai KS, Leslie D. The burden of chronic low back pain: clinical comorbidities, treatment patterns, and health care costs in usual care settings. Spine. 2012; 37(11):E668-77. [DOI:10.1097/BRS.0b013e318241e5de] [PMID]
- Delitto A, George SZ, Van Dillen L, Whitman JM, Sowa G, Shekelle P, et al. Low Back Pain. The Journal of Orthopaedic and Sports Physical Therapy. 2012; 42(4):A1-57. [DOI:10.2519/jospt.2012.42.4.A1] [PMID]
- Alshehri MA, Alzahrani H, Alotaibi M, Alhowimel A, Khoja O. Physiotherapists’ pain attitudes and beliefs towards chronic low back pain and their association with treatment selection: A cross-sectional study. BMJ Open. 2020; 10(6):e037159. [DOI:10.1136/bmjopen-2020-037159] [PMID]
- Ibrahim AA, Akindele MO, Ganiyu SO. Effectiveness of patient education plus motor control exercise versus patient education alone versus motor control exercise alone for rural community-dwelling adults with chronic low back pain: A randomized clinical trial. BMC Musculoskeletal Disorders. 2023; 24(1):142. [DOI:10.1186/s12891-022-06108-9] [PMID]
- Bendelow G. Chronic pain patients and the biomedical model of pain. The Virtual Mentor: VM. 2013; 15(5):455-9.[DOI:10.1001/virtualmentor.2013.15.5.msoc1-1305] [PMID]
- National Research Council (US) Committee on New and Emerging Models in Biomedical and Behavioral Research. Biomedical models and resources: Current needs and future opportunities. Washington (DC): National Academies Press (US); 1998. [DOI: 10.17226/6066] [PMID]
- Edwards RR, Dworkin RH, Sullivan MD, Turk DC, Wasan AD. The role of psychosocial processes in the development and maintenance of chronic pain disorders. The Journal of Pain. 2016; 17(9 Suppl):T70-92. [DOI:10.1016/j.jpain.2016.01.001] [PMID]
- Vuong TD, Wei F, Beverly CJ. Absenteeism due to functional limitations caused by seven common chronic diseases in US Workers. Journal of Occupational and Environmental Medicine. 2015; 57(7):779-84. [DOI:10.1097/JOM.0000000000000452] [PMID]
- Koes BW, van Tulder M, Lin CW, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. European Spine Journal. 2010; 19(12):2075-94. [DOI:10.1007/s00586-010-1502-y] [PMID]
- Koes BW, van Tulder M, Lin CWC, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. European Spine Journal. 2010; 19(12):2075-94. [DOI:10.1007/s00586-010-1502-y] [PMID]
- Varrassi G, Moretti B, Pace MC, Evangelista P, Iolascon G. Common clinical practice for low back pain treatment: A modified delphi study. Pain and Therapy. 2021; 10(1):589-604. [DOI:10.1007/s40122-021-00249-w] [PMID]
- Ikemoto T, Miki K, Matsubara T, Wakao N. Psychological treatment strategy for chronic low back pain. Spine Surg Relat Res. 2018; 3(3):199-206. [DOI: 10.22603/ssrr.2018-0050] [PMID]
- Turk DC, Wilson HD. Fear of pain as a prognostic factor in chronic pain: conceptual models, assessment, and treatment implications. Current Pain and Headache Reports. 2010; 14(2):88-95. [DOI:10.1007/s11916-010-0094-x] [PMID]
- García-Martínez E, Soler-González J, Blanco-Blanco J, Rubí-Carnacea F, Masbernat-Almenara M, Valenzuela-Pascual F. Misbeliefs about non-specific low back pain and attitudes towards treatment by primary care providers in Spain: A qualitative study. BMC Primary Care. 2022; 23(1):9. [DOI:10.1186/s12875-021-01617-3] [PMID]
- Caneiro JP, Bunzli S, O’Sullivan P. Beliefs about the body and pain: The critical role in musculoskeletal pain management. Brazilian Journal of Physical Therapy. 2021; 25(1):17-29. [DOI:10.1016/j.bjpt.2020.06.003] [PMID]
- Benny E, Evans C. Ontario musculoskeletal physiotherapists’ attitudes toward and beliefs about managing chronic low back pain. Physiotherapie Canada. 2020; 72(4):355-63.[DOI:10.3138/ptc-2019-0026] [PMID]
- Christe G, Nzamba J, Desarzens L, Leuba A, Darlow B, Pichonnaz C. Physiotherapists’ attitudes and beliefs about low back pain influence their clinical decisions and advice. Musculoskeletal Science & Practice. 2021; 53:102382. [DOI:10.1016/j.msksp.2021.102382] [PMID]
- Darlow B, Fullen BM, Dean S, Hurley DA, Baxter GD, Dowell A. The association between health care professional attitudes and beliefs and the attitudes and beliefs, clinical management, and outcomes of patients with low back pain: A systematic review. European Journal of Pain (London, England). 2012; 16(1):3-17. [DOI:10.1016/j.ejpain.2011.06.006] [PMID]
- Sit RW, Yip BH, Chan DC, Wong SY. Primary care physicians’ attitudes and beliefs towards chronic low back pain: An Asian study. Plos One. 2015; 10(1):e0117521. [DOI:10.1371/journal.pone.0117521] [PMID]
Article type: Original Research Articles |
Subject:
Physiotherapy
Received: 2023/03/2 | Accepted: 2024/02/17 | Published: 2024/06/1
Received: 2023/03/2 | Accepted: 2024/02/17 | Published: 2024/06/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
