
988368
Wed, May 27, 2026

Volume 22, Issue 3 (September 2024)
Iranian Rehabilitation Journal 2024, 22(3): 411-422 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Baghban K, Asadi M, Zarifian T, Derakhshandeh F. Temporal Aspects of Velopharyngeal Coarticulation in Persian-speaking Adults With and Without Cleft Palate. Iranian Rehabilitation Journal 2024; 22 (3) :411-422
URL: http://irj.uswr.ac.ir/article-1-1946-en.html
URL: http://irj.uswr.ac.ir/article-1-1946-en.html



1- Department of Speech Therapy, School of Rehabilitation Sciences, Hamadan University of Medical Sciences, Hamadan, Iran.
2- Department of Speech Therapy, Neuromuscular Rehabilitation Research Center, School of Rehabilitation Sciences, Semnan University of Medical Sciences, Semnan, Iran.
3- Department of Speech Therapy, Pediatric Neurorehabilitation Research Center, School of Rehabilitation, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Craniofacial and Cleft Research Center, Isfahan University of Medical Sciences, Isfahan, Iran.
2- Department of Speech Therapy, Neuromuscular Rehabilitation Research Center, School of Rehabilitation Sciences, Semnan University of Medical Sciences, Semnan, Iran.
3- Department of Speech Therapy, Pediatric Neurorehabilitation Research Center, School of Rehabilitation, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Craniofacial and Cleft Research Center, Isfahan University of Medical Sciences, Isfahan, Iran.
Full-Text [PDF 565 kb]
(834 Downloads)
| Abstract (HTML) (3222 Views)
Full-Text: (743 Views)
Introduction
Proficient control of articulatory movements during speech production is evident through the precise coordination of coarticulation, which pertains to the concurrent articulatory actions of neighboring phonemes in spoken language [1]. Articulatory gestures inherently possess temporal characteristics that overlap during speech, with the degree of coarticulation influenced by a multitude of factors, encompassing speech rate and linguistic constraints [2].
Velopharyngeal coarticulation denotes the influence of nasal consonants on preceding (i.e. anticipatory) or subsequent (i.e. carryover) segments within continuous speech [3]. In the context of nasal consonants, the velopharyngeal port should remain open to facilitate the propagation of acoustic energy within the nasal cavity. Consequently, misalignment in the timing of velopharyngeal movements, in concert with other articulatory elements, can precipitate an imbalance in oral-nasal resonance [4, 5, 6]. Aerodynamic investigations have established that the temporal patterns of velopharyngeal valve actions significantly impact the perception of nasal resonance [6, 7]. Prolonged durations for the opening and closing of the velopharyngeal valve preceding and succeeding a nasal consonant, beyond typical norms, are associated with the perception of hypernasal speech quality [8].
Hypernasality represents a prevalent form of nasality disorder, commonly observed in people presenting cleft palate, either with or without concomitant cleft lip, characterized by an excessive nasal quality in the production of standard vowel sounds [9].
Research in the realm of speech motor control has extensively explored coarticulatory phenomena across various components of the speech apparatus, including the larynx, velopharyngeal subsystem, tongue, jaw, and lips. Numerous investigations employing diverse observational methods have documented instances of velopharyngeal coarticulation [1].
Studies conducted by Warren et al. (1985, 1990) and Dalston (1991) have revealed a significant increase in airflow duration as the severity of velopharyngeal insufficiency escalates in individuals afflicted with cleft palate [5-7]. Dotevall et al. (2001, 2002) have established a connection between the timing characteristics of airflow through the nasal passages during the phase of velopharyngeal closure in speech and the perception of hypernasality [8]. Furthermore, Jones (2000) has elucidated that misalignment in the timing of the movements of the velopharyngeal mechanism concerning the initiation and conclusion of voicing can lead to an exaggerated perception of nasalization [9].
Zajac and Hackett (2002) have discerned distinct temporal patterns in the aerodynamic aspects of speech among pediatric and adult populations, both with and without cleft palate, utilizing the method of pressure-flow analysis [10]. Meanwhile, Jones (2006) has underscored the potential for subtle differences in both structural and motor aspects between normal and cleft palates individuals to manifest in the spatiotemporal demands of intricate velopharyngeal movements, potentially resulting in more conspicuous oral-nasal impedance ratios [11].
Incorporating nanometer measurements, Bae et al. (2007) have empirically substantiated the notable influence of vowel sounds on the temporal patterns of nasalization [12]. Moreover, several investigations have delved into the temporal attributes of nasalization in both American English and Korean speakers with and without cleft palate. Their analyses of oral and nasal cavity acoustic energy have revealed that cleft palate individuals with hypernasality exhibit extended nasalization durations compared to their non-cleft palate counterparts [3, 4, 13].
Numerous investigations have revealed variations in the coarticulatory nasalization patterns and the temporal dynamics of velopharyngeal movements across different age groups and linguistic contexts [4, 13]. While Baghban et al. (2015) demonstrated an extended duration of nasalization in children with cleft palate who speak Persian compared to their typically developing peers [14], there exists a notable absence of information concerning the temporal characteristics of velopharyngeal coarticulation in Persian-speaking adults, both with and without cleft palate. Accordingly, the results are inconclusive in surveying the speech motor control development and velopharyngeal coarticulation in the Persian language. This research was structured to fulfill the following two objectives: 1) To investigate velopharyngeal coarticulation in Persian-speaking adults with and without cleft palate; 2) To contrast the temporal aspects of nasalization in Persian-speaking adults with and without cleft palate.
Materials and Methods
The current investigation constituted a descriptive-analytical cross-sectional study.
Study participants
This research was carried out on a sample of 14 adults who had undergone cleft palate repair, with or without cleft lip (comprising 11 males and 3 females). These individuals were selected from speech therapy clinics located in Tehran City, Iran. Additionally, 14 adults without cleft palate (consisting of 11 males and 3 females) were recruited from the academic community of the University of Social Welfare and Rehabilitation Sciences, in Tehran City, Iran. All participants in this study were monolingual adults who spoke Persian as their primary language. The participants’ ages ranged from 18 to 50 years, with a Mean±SD age of 31.8±2.1 years for adults with cleft palate and 31.2±1.8 years for adults without cleft palate. The type of cleft among adults with cleft palate was divided into 4 diagnostic categories, which are presented in Table 1.
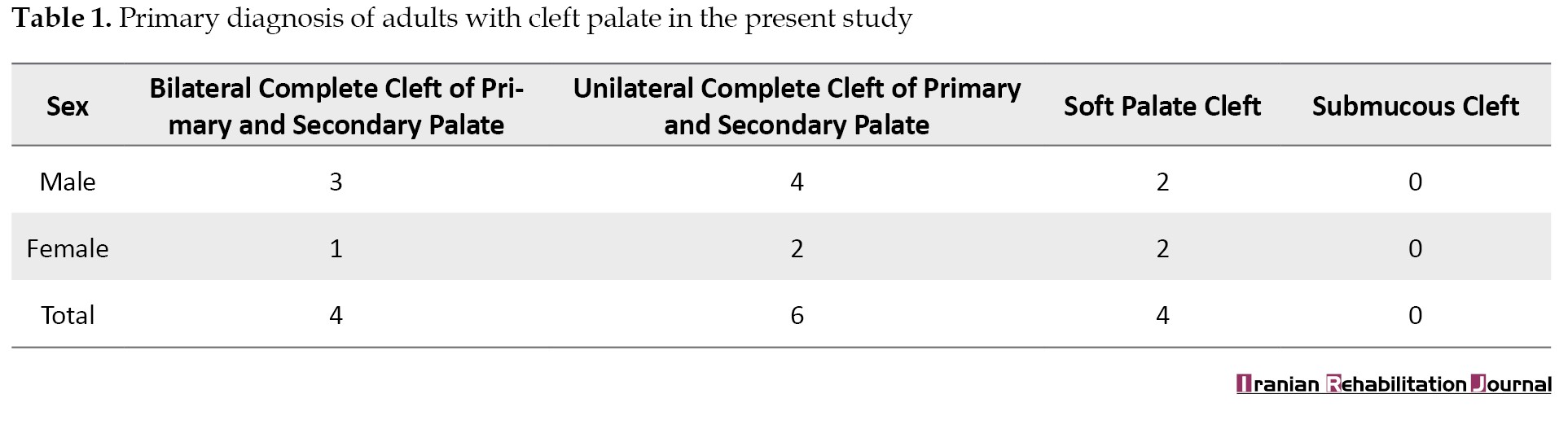
All adults with cleft palate had normal hearing based on their audiograms and medical records and normal receptive language based on the implemented assessment by the first author. Every participant with cleft palate exhibited varying degrees of hypernasality, ranging from moderate to severe. The assessment of hypernasality was conducted utilizing single terms and phrases containing consonants with high pressure, following the universal parameters guidelines and the Cleft audit protocol for speech-augmented (CAPS-A) [15, 16].
Study materials and procedures
CAPS-A
In the present investigation, the rate of hypernasality was conducted using the CAPS-A. This instrument is recognized for its validity and reliability, rendering it suitable for conducting cross-center evaluations of speech results in cleft palate individuals. The average agreement percentage for criterion validity across the various sections was determined to be 87%, with a range spanning from 70% to 100%. The CAPS-A also exhibited commendable levels of both intra-rater and inter-rater reliability, with measures ranging from good to very good (Kappa=0.61 to 1.00) across seven sections, while three sections exhibited moderate reliability (Kappa=0.41 to 0.60) [16].
In this study, we employed subgroup 3a of the CAPS-A assessment, which specifically targets hypernasality in speech. Hypernasality within the CAPS-A is evaluated using a 5-point scale, with ratings as follows: 0: The absence of hypernasality, 1: Borderline condition, 2: Mild hypernasality, 3: Moderate level, and 4: Severe hypernasality.
Speech sample
The speech samples comprised a set of three disyllabic sequences with the /CVCVC/ structure, specifically/pamap/, /pumup/ and /pimip/. These sequences, involving the alternation of consonants /m/ and /p/ preceding and succeeding vowels in speech tasks, facilitate the velopharyngeal port’s opening and closing dynamics. Both nasal /m/ and oral /p/ consonants are produced in the lip position. While it is recognized that the primary factor contributing to hypernasality lies in the coupling of the oral and nasal cavities, the tongue’s placement and the level of tension in the glottal structures can also influence the balance of oral-nasal resonance. Therefore, not all vowels are equally susceptible to the effects of oral-nasal interconnection due to variations in their respective tongue placement within the oral cavity [17, 18]. Consequently, to explore distinct timing parameters among vowels, three specific vowels, namely /i/, /u/ and /a/, which articulated at various locations of constriction along the vocal tract, were deliberately selected.
Data collection
Speech samples were recorded individually within an acoustically controlled environment. Following the participants’ completion of the informed consent process and initial communication, the test procedure was explained to them. They were then instructed to produce speech samples that closely matched a standardized audio model, adhering to the conventional pitch and loudness associated with the standard Persian accent of Tehran. Each participant was provided with the audio model, which represented the standard Persian accent of Tehran, and had the opportunity to listen to it up to three times for reference.
The participants’ acoustic data were simultaneously recorded using microphones situated in both the oral and nasal cavities, facilitated by an MSI-cx 620 laptop equipped with an Onyx Blackjack Premium 2×2 USB recording interface. To record the speech data accurately, a pair of high-quality microphones was affixed to the participants’ heads, comprising two microphones, one placed near the mouth and the other positioned beneath the right nostril. These microphones, namely the Shure-Beta 54 model, were manufactured in the United States. The microphone of the oral cavity was situated at a distance of approximately 3 cm from the right aspect of the participant’s mouth. Also, the microphone of the nasal cavity was carefully positioned beneath the right nostril.
Data extraction
The acquired acoustic signals from both the nasal and oral sources were subjected to analysis through the utilization of the Praat software, version 6.1.50. This analysis involved the utilization of two distinct channels in the software. The initial channel was employed to scrutinize signals captured by the microphone situated beneath the nostril, while the subsequent channel was dedicated to the analysis of signals collected by the microphone positioned in front of the mouth.
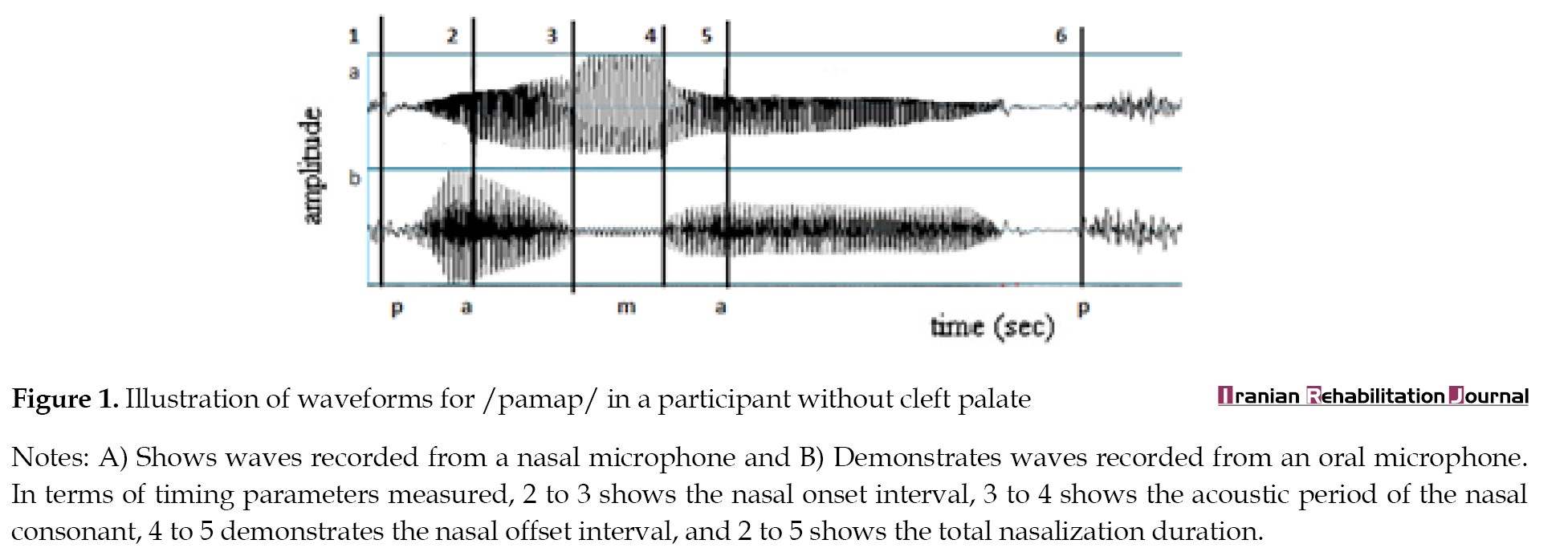
Several temporal parameters, including the nasal onset interval, nasal offset interval, acoustic duration of the nasal consonant and the overall nasalization duration, were computed for every of the speech samples encompassing /pamap/, /pimip/ and /pumup/. These calculations were based on distinctive features extracted from acoustic waveforms, spectrograms and energy contours derived from the data recorded by the two aforementioned channels. The specific definitions and graphical representation of these timing measurements are detailed in Figure 1.
Nasal onset interval
The nasal onset interval is defined as the temporal span between the moment when there is a noticeable rise in nasal acoustic energy coupled with a decline in oral acoustic energy, and the commencement of the acoustic phase corresponding to the nasal consonant. According to Figure 1, this interval is delineated by time points “2” and “3.”
Acoustic period of the nasal consonant
Within this timing measurement, distinctive spectral features are observed, including reduced intensity in the formants as depicted on the spectrograms derived from the oral microphone data. This interval pertains to the temporal segment encompassed by time points “3” and “4” as illustrated in Figure 1.
Nasal offset interval
This duration is measured from the termination of the acoustic segment linked to the nasal consonant to the point where a rise in oral acoustic energy aligns with a reduction in nasal acoustic energy, indicating the initiation of the oral aperture for the ensuing vowel articulation. The nasal offset interval is defined by time points “4” and “5” in Figure 1.
Total nasalization duration
The total duration of nasalization encompassed the combined durations of the nasal onset interval, the acoustic period of the nasal consonant, and the nasal offset interval. According to Figure 1, this interval is represented by the time points “2” to “5."
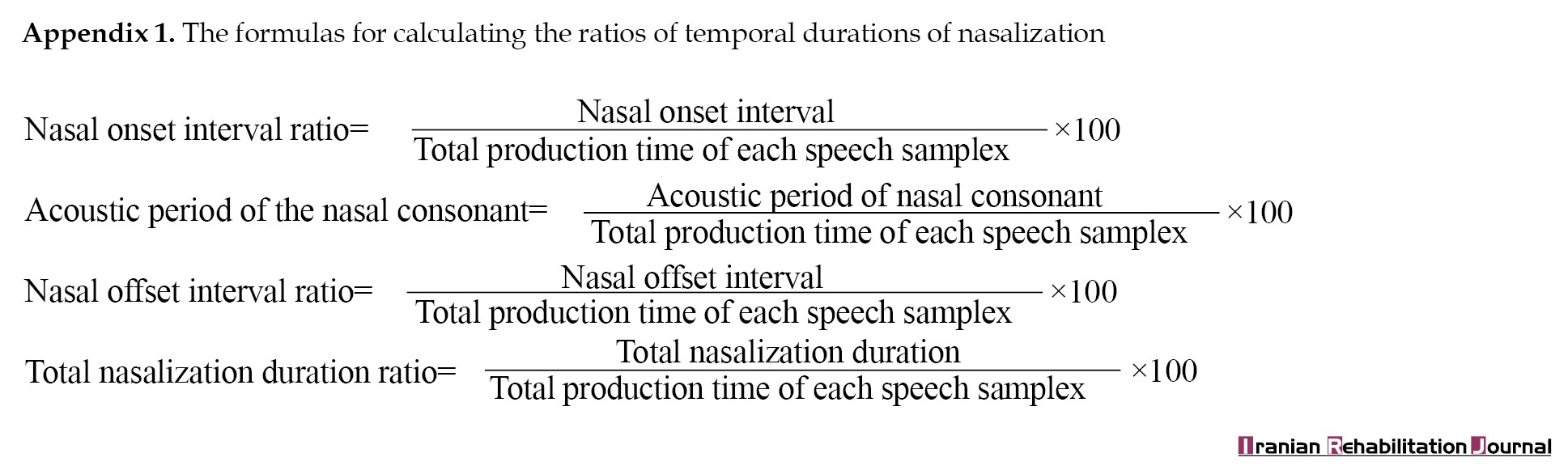
To account for variations in speech rates in both the cleft palate and control groups, we computed the temporal duration ratios of nasalization using the formulas provided in Appendix 1.
Reliability analysis
Two speech therapists specialized in cleft speech with 8 and 5 years of respective experience, independently rated all speech samples using the CAPS-A. The two assessments were conducted with a three-week interval between them. To assess the reliability of hypernasality ratings, the Spearman correlation coefficient was employed for both intra-rater and inter-rater assessments. The Spearman correlation coefficients for intra-rater reliability exhibited a value of 0.81 for each of the raters. Additionally, the Spearman correlation coefficient for inter-rater reliability was calculated to be 0.75.
Statistical analysis
The statistical analysis was performed using the SPSS software, version 22, using a significance level (α) of 0.05. To assess the normal distribution of the desired parameters, the Shapiro-Wilk test was performed. The results of the Shapiro-Wilk test for the nasal onset interval ratio, nasal offset interval ratio, acoustic duration of the nasal consonant, and total nasalization duration ratio yielded values of 0.75, 0.68, 0.55 and 0.79, respectively. Given that these values exceeded 0.05, the data were considered to follow a normal distribution.
To compare the four measures of nasalization duration across individuals with and without cleft palate in the /pamap/, /pumup/ and /pimip/ contexts, a two-way mixed analysis of variance with repeated measures, involving 2 groups×3 contexts, was employed. Furthermore, the Duncan multiple comparison post hoc test was employed to investigate statistically significant distinctions in the three temporal parameters across the /i/, /u/ and /a/ vowel contexts within each group of participants. The test power was determined using the R2 software, version 3.6.2.
Results
Table 2 presents the findings of the temporal duration analysis for all three tasks in the two subject groups.
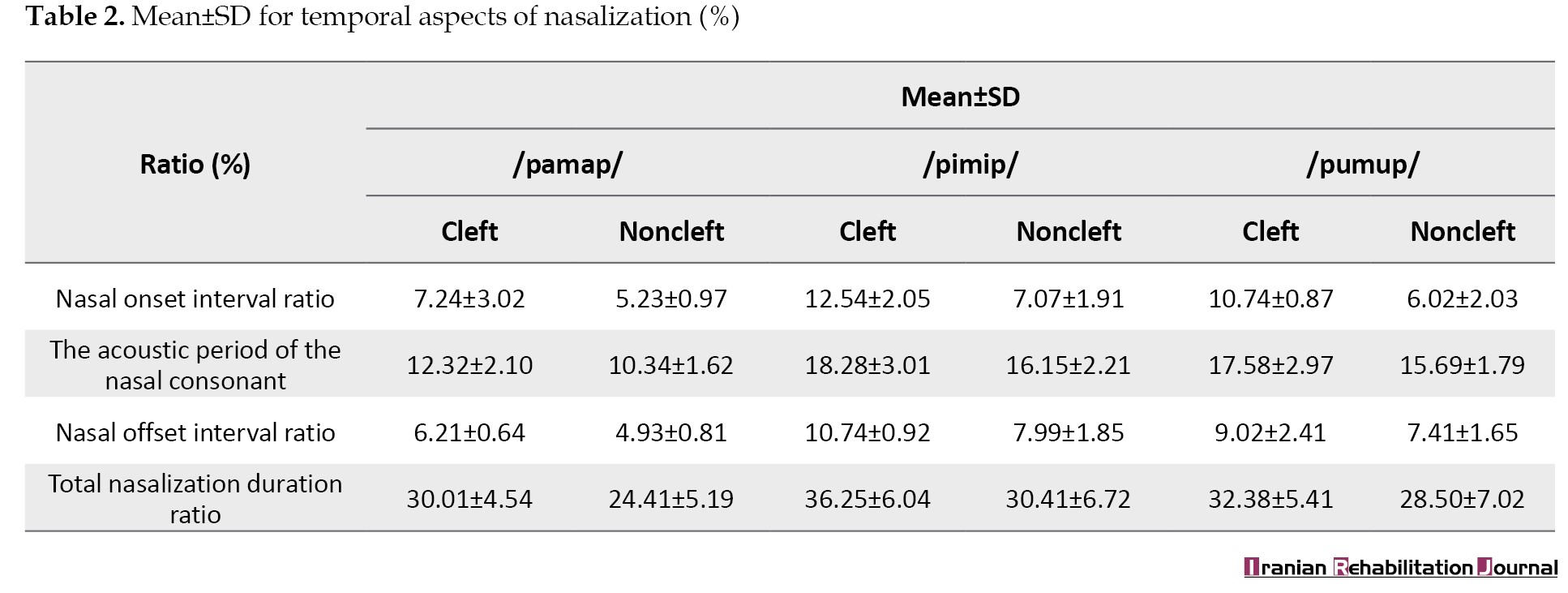
In both groups, the most extended durations were consistently observed across the nasal onset interval ratio, nasal offset interval ratio, acoustic duration of the nasal consonant, and total nasalization duration ratio for the /i/ context, as detailed in Table 2. For both groups, the pattern indicated that the total nasalization duration ratio followed an ascending order of /i/, /u/ and /a/. In simpler terms, the high vowel contexts consistently exhibited a more protracted total nasalization duration in contrast to the contexts involving low vowels in both subject groups. The power of the test was calculated as 0.905 using the R2 software.
The 2×2 mixed analysis of variance conducted on the nasal onset interval ratio within the /pimip/, /pamap/, and /pumup/ contexts, considering both subject groups, revealed significant effects for group (F(1, 170)=34.56, P<0.001), context (F(2, 170)=46.75, P<0.001), and the interaction between group and context (F(2, 170)=16.51, P<0.001). Furthermore, the nasal onset interval ratio exhibited a significantly higher value in cleft palate adults when compared to the control group across all three vowel contexts. Subsequent Duncan multiple comparison testing demonstrated that, within both groups, the nasal onset interval ratio of the vowel context of /i/ meaningfully exceeded those of the vowel contexts of /u/ and /a/, while the nasal onset interval ratio of the vowel context of /u/ demonstrated a notable superiority when compared to the vowel context of /a/.
The 2×2 mixed analysis of variance conducted on the acoustic duration of the nasal consonant ratio within the /pimip/, /pamap/ and /pumup/ contexts, involving both subject groups, yielded significant effects for group (F(1, 170)=41.25, P<0.001) and context (F(2, 170)=70.22, P<0.001). However, it did not reveal any significant interaction between the contextual and group variables (F(2, 170)=6.42, P>0.05). Additionally, the acoustic duration of the nasal consonant ratio was significantly greater in cleft palate adults compared to the control group across all three vowel contexts. Subsequent analysis using the Duncan multiple comparison test demonstrated that, within both groups, the acoustic duration of the nasal consonant ratio in the vowel context of /i/ significantly exceeded that of the /u/ and /a/ vowel contexts. Furthermore, the acoustic duration of the nasal consonant ratio within the /u/ vowel context exhibited a significant extension compared to that of the /a/ vowel context.
The 2×2 mixed analysis of variance applied to assess the nasal offset interval ratio in the /pimip/, /pamap/ and /pumup/ contexts across both subject groups revealed significant effects for group (FF(1, 170)=34.06, P<0.000), context (F(2, 170)=65.41, P<0.000) and a significant interaction between contextual and group variables (F(2, 170)=43.28, P<0.001). Furthermore, the nasal offset interval ratio was significantly higher in cleft palate adults compared control group across all three vowel contexts. Subsequent examination using the Duncan multiple comparison test indicated that, within both groups, the nasal offset interval ratio of the /i/ vowel context was significantly greater than that of the /u/ and /a/ vowel contexts. Additionally, the nasal offset interval ratio of the /u/ vowel context exhibited a significant extension compared to that of the /a/ vowel context.
The 2×2 mixed analysis of variance conducted to assess the total nasalization duration ratio within the /pimip/, /pamap/ and /pumup/ contexts across both subject groups revealed significant effects for group (F(1, 170)=98.11, P<0.000), context (F(2, 170)=26.54, P<0.001) and a significant interaction between contextual and group variables (F(2, 170)=9.62, P<0.001). Additionally, the total nasalization duration ratio was notably higher in adults with cleft palate compared to adults without cleft palate across all three vowel contexts. Further investigation using the Duncan multiple comparison test indicated that, within both groups, the total nasalization duration ratio of the /i/ vowel context was significantly greater than those of the /u/ and /a/ vowel contexts, and the total nasalization duration ratio of the /u/ vowel context exhibited a significant extension compared to that of the /a/ vowel context.
Discussion
This study investigated the temporal characteristics of velopharyngeal coarticulation in Persian-speaking adults, comparing subjects with and without cleft palate. The outcomes unveiled that adults with cleft palate exhibited notably extended nasal onset interval ratios, nasal offset interval ratios, and total nasalization duration ratios across various vowel contexts. These findings align with prior research by Warren et al. (1985, 1990), Dalston et al. (1991) and Dotevall et al. (2002), which similarly reported significant distinctions in nasal airflow duration between normal and cleft palate subjects [5, 6, 7, 8]. The observation of prolonged velopharyngeal openness in Persian-speaking adults with cleft palate underscores the need for targeted interventions. Armed with insights into the temporal aspects of velopharyngeal closure, clinicians can develop precise clinical assessments and tailored intervention strategies for Persian-speaking adults with cleft palate.
The acoustic parameters derived from the analysis conducted in this study revealed alterations in the interaction between oral and nasal acoustic impedance, offering indirect insights into the timing dimensions of velopharyngeal coarticulation related to the movements of lips. Specifically, our research focused on examining temporal aspects when producing combinations of nasal-to-stop consonants. Measurements of temporal aspects in bilabial and velar positions revealed a close relationship between hypernasality in perceptual assessments and velopharyngeal function. Consequently, the phase of velopharyngeal closure may reflect the temporal characteristics of the pharyngeal valve, which are essential for understanding hypernasality in perceptual assessments in clinics.
From a coarticulation model perspective, the nasal onset interval ratio can be interpreted as indicative of anticipatory velopharyngeal coarticulation, while the nasal offset interval ratio aligns with carryover velopharyngeal coarticulation. Specifically, the nasal onset interval signifies the duration from the initiation of the opening of the velopharyngeal port to the closure of the oral cavity, whereas the nasal offset interval denotes the duration from the opening of the oral cavity to the closing of the velopharyngeal port. The comprehensive duration of velopharyngeal opening and closing can be deducted through the measurement of total nasalization duration [4].
According to the results, in the Persian language, adults with cleft palate demonstrate an earlier initiation of velopharyngeal port opening for nasal consonants and delayed closure of velopharyngeal port for oral consonants after nasal consonants, compared to the control group. This observation aligns with the research conducted by Baghban et al. (2015) concerning temporal aspects of nasalization in Persian-speaking children with and without cleft palate [14]. Essentially, this suggests that the patterns of velopharyngeal coarticulation exhibit similarities between Persian-speaking children and adults, both with and without cleft palate. Nevertheless, temporal intervals in adults, both with and without cleft palate, are shorter than those in children, both with and without cleft palate, across all three vowel contexts in the Persian language. The differences in temporal patterns of nasalization durations between adults and children, with and without cleft palate, may be partly attributed to variations in speech rates between these groups [2, 4].
The findings of this study were subjected to comparison with the research conducted by Baghban et al. (2015), revealing potential divergent underlying mechanisms governing how Persian-speaking adults and children, both with and without cleft palate, anticipate and carry over velopharyngeal coarticulation. This observation aligns with previous studies that have reported disparities in the temporal aspects of coarticulation between individuals of different age groups [2, 4, 13]. Coarticulation research literature consistently indicates a consensus that anticipatory and carryover coarticulation entail distinct underlying mechanisms. The mechanical inertia of the velum, leading to carryover velopharyngeal coarticulation, might remain consistent in both adults and children, whereas anticipatory velopharyngeal coarticulation could reflect developmental aspects involving the reorganization of neuromotor control for segmental articulations. Consequently, adults and children may exhibit differing temporal patterns within the domain of anticipatory velopharyngeal coarticulation [4, 13, 19].
In the case of adults with cleft palate, the nasal onset interval ratio, nasal offset ratio and total nasalization duration ratio exhibited significant variations across the three vowel contexts within each respective group. Furthermore, the outcomes of this study illuminated the presence of notable interactions between the subject groups and the specific vowel types concerning the three temporal durations. This implies that the nature and extent of group disparities in these temporal durations are influenced by the vowel categories under consideration. The temporal durations were ranked in ascending order as follows: /a/, /i/ and /u/. This outcome underscored that temporal duration ratios in high vowel contexts exceeded those observed in low vowel contexts. The heightened oral constriction associated with high vowel contexts likely contributed to longer nasal onset intervals, nasal offset intervals and total nasalization durations compared to those evident in low vowel contexts. This finding aligns with the results reported by Ha et al. and Ha and Kuehn (2004, 2011) in the context of Korean and American English [3, 13]. Additionally, it parallels the findings of Cho et al. (2000), where high vowels were found to exhibit a more pronounced and sensitive degree of nasalization about nasal-coupling balance compared to low vowels [20].
Within the scope of the present investigation, it became evident that the /pimip/ context exhibited the most pronounced disparities between the two groups. In a manner consistent with the findings of Baghban et al. (2015) concerning the timing aspects of nasalization in Persian-speaking children, our study likewise underscores that the temporal metrics of nasalization derived from the vowel context of /i/offer further discerning insights into the distinctions between groups with and without cleft palate. These temporal dissimilarities in nasalization during vowel production could potentially related to the perceived degree of nasalization [14]. This observation aligns with prior studies indicating that the /i/ context tends to be perceived as having a greater degree of nasal resonance compared to the /a/ context [3, 4, 13].
The acoustic spectrum of the /m/ nasal consonant is characterized by a prevalence of sound energy characterized by low frequency. Consequently, when the /i/ vowel and /m/ consonant, both featuring comparable formant placements, are articulated consecutively, the resonance near the nasal formant becomes more pronounced, thereby intensifying the perception of nasal resonance [4].
Kuehn and Moon (1995) conducted a study demonstrating that cleft palate participants exhibit elevated levels of levator veli palatini activation during speech production when in comparison to normal participants. This finding suggests that those with cleft palate may necessitate increased exertion to achieve velopharyngeal closure and could be more susceptible to fatigue during speech articulation [21]. The extended nasalization durations observed in the cleft palate group in our research could be indicative of atypical speech motor skills and anatomical disparities in the structure of the palate. Previous investigations have yielded similar data, but their outcomes have not consistently concurred. This variability underscores the potential for temporal characteristics of nasalization to vary among different languages. Therefore, a noteworthy strength of our study lies in the selection of our specific language for investigation.
Ultimately, the results garnered from our present study can offer valuable supplementary insights into the movements of the velum and lips, particularly in the context of imaging techniques like x-ray, magnetic resonance imaging, and ultrasound [22, 23].
Clinical and research implications
The current investigation has furnished more precise insights into the functioning of the velopharyngeal mechanism, thus enhancing the potential for more precise clinical evaluations and practical intervention strategies. Essentially, this research underscores the significance of carefully selecting speech patterns when evaluating and addressing velopharyngeal function, especially in the context of perceptual speech attributes like the phonetic placement of target phonemes. Our study has unveiled that among Persian-speaking adults, those with cleft palate tend to exhibit extended durations of nasalization compared to their non-cleft palate counterparts. Consequently, when appraising hypernasality in cleft speech and speech therapy settings, it is imperative to recognize that the temporal dimensions of nasalization can be influenced by the degree of hypernasality in adults with cleft palate. These findings hold relevance not only for speech and language pathologists but also for linguists and other specialists collaborating within cleft palate teams.
Conclusion
In this investigation, Persian adults with cleft palate demonstrated significantly prolonged nasalization durations in comparison to their non-cleft palate counterparts. The analysis undertaken in this study delved not only into the acoustic energy ratios but also into the acoustic events linked to the temporal dimensions of velopharyngeal coarticulation, particularly about the timing of lip opening and closure throughout the articulation process. The most conspicuous disparity between these two groups emerged within the context of the vowel /i/. This research contributed acoustic evidence related to velopharyngeal coarticulation, lending support to the expectations set forth by the coproduction model regarding the extent of anticipatory and carryover coarticulation, as well as aligning with the predictions of gestural phonology concerning the nature of speech production units and the speech patterns observed in adults.
Study limitations
The data analysis approach employed in this study primarily focused on the temporal characteristics of velopharyngeal movement related to the opening and closing of the lip, rather than emphasizing the rate of acoustic energy. Future investigations could explore the connection between temporal attributes and nasalization using alternative indirect assessment tools. Given that patterns of nasalization can exhibit variability across specific languages, it is essential to recognize that the temporal aspects of velopharyngeal coarticulation in this study may have limitations specific to the Persian language. Consequently, extrapolating the results to other languages should be undertaken cautiously. An avenue for future research entails replicating this study on a more extensive scale, encompassing a significantly larger sample size, a broader age spectrum, and a more diverse array of regional dialects. The current study was confined to a limited set of speech tasks; therefore, forthcoming research should encompass additional speech samples spanning a wider array of vowels and consonants, including those with diverse places and manners of articulation. Moreover, in future research, it would be valuable to compare the temporal aspects of velopharyngeal coarticulation among groups with apraxia, dysarthria, and other resonance disorders.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Isfahan University of Medical Science (Code: IR.MUI.REC.1395.2.150). Before their involvement in the study, all participants were given a comprehensive explanation of the research procedure and its duration. Consent forms were made available to the adult participants, and their participation commenced following their informed consent.
Funding
This research was supported by the research project (No.: 295150), Funded by the Isfahan University of Medical Science.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Authors thank the Craniofacial and Cleft Research Center of the Isfahan University of Medical Science, the University of Social Welfare and Rehabilitation Sciences, and participants with and without cleft palate who participated eagerly in this study.
References
Proficient control of articulatory movements during speech production is evident through the precise coordination of coarticulation, which pertains to the concurrent articulatory actions of neighboring phonemes in spoken language [1]. Articulatory gestures inherently possess temporal characteristics that overlap during speech, with the degree of coarticulation influenced by a multitude of factors, encompassing speech rate and linguistic constraints [2].
Velopharyngeal coarticulation denotes the influence of nasal consonants on preceding (i.e. anticipatory) or subsequent (i.e. carryover) segments within continuous speech [3]. In the context of nasal consonants, the velopharyngeal port should remain open to facilitate the propagation of acoustic energy within the nasal cavity. Consequently, misalignment in the timing of velopharyngeal movements, in concert with other articulatory elements, can precipitate an imbalance in oral-nasal resonance [4, 5, 6]. Aerodynamic investigations have established that the temporal patterns of velopharyngeal valve actions significantly impact the perception of nasal resonance [6, 7]. Prolonged durations for the opening and closing of the velopharyngeal valve preceding and succeeding a nasal consonant, beyond typical norms, are associated with the perception of hypernasal speech quality [8].
Hypernasality represents a prevalent form of nasality disorder, commonly observed in people presenting cleft palate, either with or without concomitant cleft lip, characterized by an excessive nasal quality in the production of standard vowel sounds [9].
Research in the realm of speech motor control has extensively explored coarticulatory phenomena across various components of the speech apparatus, including the larynx, velopharyngeal subsystem, tongue, jaw, and lips. Numerous investigations employing diverse observational methods have documented instances of velopharyngeal coarticulation [1].
Studies conducted by Warren et al. (1985, 1990) and Dalston (1991) have revealed a significant increase in airflow duration as the severity of velopharyngeal insufficiency escalates in individuals afflicted with cleft palate [5-7]. Dotevall et al. (2001, 2002) have established a connection between the timing characteristics of airflow through the nasal passages during the phase of velopharyngeal closure in speech and the perception of hypernasality [8]. Furthermore, Jones (2000) has elucidated that misalignment in the timing of the movements of the velopharyngeal mechanism concerning the initiation and conclusion of voicing can lead to an exaggerated perception of nasalization [9].
Zajac and Hackett (2002) have discerned distinct temporal patterns in the aerodynamic aspects of speech among pediatric and adult populations, both with and without cleft palate, utilizing the method of pressure-flow analysis [10]. Meanwhile, Jones (2006) has underscored the potential for subtle differences in both structural and motor aspects between normal and cleft palates individuals to manifest in the spatiotemporal demands of intricate velopharyngeal movements, potentially resulting in more conspicuous oral-nasal impedance ratios [11].
Incorporating nanometer measurements, Bae et al. (2007) have empirically substantiated the notable influence of vowel sounds on the temporal patterns of nasalization [12]. Moreover, several investigations have delved into the temporal attributes of nasalization in both American English and Korean speakers with and without cleft palate. Their analyses of oral and nasal cavity acoustic energy have revealed that cleft palate individuals with hypernasality exhibit extended nasalization durations compared to their non-cleft palate counterparts [3, 4, 13].
Numerous investigations have revealed variations in the coarticulatory nasalization patterns and the temporal dynamics of velopharyngeal movements across different age groups and linguistic contexts [4, 13]. While Baghban et al. (2015) demonstrated an extended duration of nasalization in children with cleft palate who speak Persian compared to their typically developing peers [14], there exists a notable absence of information concerning the temporal characteristics of velopharyngeal coarticulation in Persian-speaking adults, both with and without cleft palate. Accordingly, the results are inconclusive in surveying the speech motor control development and velopharyngeal coarticulation in the Persian language. This research was structured to fulfill the following two objectives: 1) To investigate velopharyngeal coarticulation in Persian-speaking adults with and without cleft palate; 2) To contrast the temporal aspects of nasalization in Persian-speaking adults with and without cleft palate.
Materials and Methods
The current investigation constituted a descriptive-analytical cross-sectional study.
Study participants
This research was carried out on a sample of 14 adults who had undergone cleft palate repair, with or without cleft lip (comprising 11 males and 3 females). These individuals were selected from speech therapy clinics located in Tehran City, Iran. Additionally, 14 adults without cleft palate (consisting of 11 males and 3 females) were recruited from the academic community of the University of Social Welfare and Rehabilitation Sciences, in Tehran City, Iran. All participants in this study were monolingual adults who spoke Persian as their primary language. The participants’ ages ranged from 18 to 50 years, with a Mean±SD age of 31.8±2.1 years for adults with cleft palate and 31.2±1.8 years for adults without cleft palate. The type of cleft among adults with cleft palate was divided into 4 diagnostic categories, which are presented in Table 1.
All adults with cleft palate had normal hearing based on their audiograms and medical records and normal receptive language based on the implemented assessment by the first author. Every participant with cleft palate exhibited varying degrees of hypernasality, ranging from moderate to severe. The assessment of hypernasality was conducted utilizing single terms and phrases containing consonants with high pressure, following the universal parameters guidelines and the Cleft audit protocol for speech-augmented (CAPS-A) [15, 16].
Study materials and procedures
CAPS-A
In the present investigation, the rate of hypernasality was conducted using the CAPS-A. This instrument is recognized for its validity and reliability, rendering it suitable for conducting cross-center evaluations of speech results in cleft palate individuals. The average agreement percentage for criterion validity across the various sections was determined to be 87%, with a range spanning from 70% to 100%. The CAPS-A also exhibited commendable levels of both intra-rater and inter-rater reliability, with measures ranging from good to very good (Kappa=0.61 to 1.00) across seven sections, while three sections exhibited moderate reliability (Kappa=0.41 to 0.60) [16].
In this study, we employed subgroup 3a of the CAPS-A assessment, which specifically targets hypernasality in speech. Hypernasality within the CAPS-A is evaluated using a 5-point scale, with ratings as follows: 0: The absence of hypernasality, 1: Borderline condition, 2: Mild hypernasality, 3: Moderate level, and 4: Severe hypernasality.
Speech sample
The speech samples comprised a set of three disyllabic sequences with the /CVCVC/ structure, specifically/pamap/, /pumup/ and /pimip/. These sequences, involving the alternation of consonants /m/ and /p/ preceding and succeeding vowels in speech tasks, facilitate the velopharyngeal port’s opening and closing dynamics. Both nasal /m/ and oral /p/ consonants are produced in the lip position. While it is recognized that the primary factor contributing to hypernasality lies in the coupling of the oral and nasal cavities, the tongue’s placement and the level of tension in the glottal structures can also influence the balance of oral-nasal resonance. Therefore, not all vowels are equally susceptible to the effects of oral-nasal interconnection due to variations in their respective tongue placement within the oral cavity [17, 18]. Consequently, to explore distinct timing parameters among vowels, three specific vowels, namely /i/, /u/ and /a/, which articulated at various locations of constriction along the vocal tract, were deliberately selected.
Data collection
Speech samples were recorded individually within an acoustically controlled environment. Following the participants’ completion of the informed consent process and initial communication, the test procedure was explained to them. They were then instructed to produce speech samples that closely matched a standardized audio model, adhering to the conventional pitch and loudness associated with the standard Persian accent of Tehran. Each participant was provided with the audio model, which represented the standard Persian accent of Tehran, and had the opportunity to listen to it up to three times for reference.
The participants’ acoustic data were simultaneously recorded using microphones situated in both the oral and nasal cavities, facilitated by an MSI-cx 620 laptop equipped with an Onyx Blackjack Premium 2×2 USB recording interface. To record the speech data accurately, a pair of high-quality microphones was affixed to the participants’ heads, comprising two microphones, one placed near the mouth and the other positioned beneath the right nostril. These microphones, namely the Shure-Beta 54 model, were manufactured in the United States. The microphone of the oral cavity was situated at a distance of approximately 3 cm from the right aspect of the participant’s mouth. Also, the microphone of the nasal cavity was carefully positioned beneath the right nostril.
Data extraction
The acquired acoustic signals from both the nasal and oral sources were subjected to analysis through the utilization of the Praat software, version 6.1.50. This analysis involved the utilization of two distinct channels in the software. The initial channel was employed to scrutinize signals captured by the microphone situated beneath the nostril, while the subsequent channel was dedicated to the analysis of signals collected by the microphone positioned in front of the mouth.
Several temporal parameters, including the nasal onset interval, nasal offset interval, acoustic duration of the nasal consonant and the overall nasalization duration, were computed for every of the speech samples encompassing /pamap/, /pimip/ and /pumup/. These calculations were based on distinctive features extracted from acoustic waveforms, spectrograms and energy contours derived from the data recorded by the two aforementioned channels. The specific definitions and graphical representation of these timing measurements are detailed in Figure 1.
Nasal onset interval
The nasal onset interval is defined as the temporal span between the moment when there is a noticeable rise in nasal acoustic energy coupled with a decline in oral acoustic energy, and the commencement of the acoustic phase corresponding to the nasal consonant. According to Figure 1, this interval is delineated by time points “2” and “3.”
Acoustic period of the nasal consonant
Within this timing measurement, distinctive spectral features are observed, including reduced intensity in the formants as depicted on the spectrograms derived from the oral microphone data. This interval pertains to the temporal segment encompassed by time points “3” and “4” as illustrated in Figure 1.
Nasal offset interval
This duration is measured from the termination of the acoustic segment linked to the nasal consonant to the point where a rise in oral acoustic energy aligns with a reduction in nasal acoustic energy, indicating the initiation of the oral aperture for the ensuing vowel articulation. The nasal offset interval is defined by time points “4” and “5” in Figure 1.
Total nasalization duration
The total duration of nasalization encompassed the combined durations of the nasal onset interval, the acoustic period of the nasal consonant, and the nasal offset interval. According to Figure 1, this interval is represented by the time points “2” to “5."
To account for variations in speech rates in both the cleft palate and control groups, we computed the temporal duration ratios of nasalization using the formulas provided in Appendix 1.
Reliability analysis
Two speech therapists specialized in cleft speech with 8 and 5 years of respective experience, independently rated all speech samples using the CAPS-A. The two assessments were conducted with a three-week interval between them. To assess the reliability of hypernasality ratings, the Spearman correlation coefficient was employed for both intra-rater and inter-rater assessments. The Spearman correlation coefficients for intra-rater reliability exhibited a value of 0.81 for each of the raters. Additionally, the Spearman correlation coefficient for inter-rater reliability was calculated to be 0.75.
Statistical analysis
The statistical analysis was performed using the SPSS software, version 22, using a significance level (α) of 0.05. To assess the normal distribution of the desired parameters, the Shapiro-Wilk test was performed. The results of the Shapiro-Wilk test for the nasal onset interval ratio, nasal offset interval ratio, acoustic duration of the nasal consonant, and total nasalization duration ratio yielded values of 0.75, 0.68, 0.55 and 0.79, respectively. Given that these values exceeded 0.05, the data were considered to follow a normal distribution.
To compare the four measures of nasalization duration across individuals with and without cleft palate in the /pamap/, /pumup/ and /pimip/ contexts, a two-way mixed analysis of variance with repeated measures, involving 2 groups×3 contexts, was employed. Furthermore, the Duncan multiple comparison post hoc test was employed to investigate statistically significant distinctions in the three temporal parameters across the /i/, /u/ and /a/ vowel contexts within each group of participants. The test power was determined using the R2 software, version 3.6.2.
Results
Table 2 presents the findings of the temporal duration analysis for all three tasks in the two subject groups.
In both groups, the most extended durations were consistently observed across the nasal onset interval ratio, nasal offset interval ratio, acoustic duration of the nasal consonant, and total nasalization duration ratio for the /i/ context, as detailed in Table 2. For both groups, the pattern indicated that the total nasalization duration ratio followed an ascending order of /i/, /u/ and /a/. In simpler terms, the high vowel contexts consistently exhibited a more protracted total nasalization duration in contrast to the contexts involving low vowels in both subject groups. The power of the test was calculated as 0.905 using the R2 software.
The 2×2 mixed analysis of variance conducted on the nasal onset interval ratio within the /pimip/, /pamap/, and /pumup/ contexts, considering both subject groups, revealed significant effects for group (F(1, 170)=34.56, P<0.001), context (F(2, 170)=46.75, P<0.001), and the interaction between group and context (F(2, 170)=16.51, P<0.001). Furthermore, the nasal onset interval ratio exhibited a significantly higher value in cleft palate adults when compared to the control group across all three vowel contexts. Subsequent Duncan multiple comparison testing demonstrated that, within both groups, the nasal onset interval ratio of the vowel context of /i/ meaningfully exceeded those of the vowel contexts of /u/ and /a/, while the nasal onset interval ratio of the vowel context of /u/ demonstrated a notable superiority when compared to the vowel context of /a/.
The 2×2 mixed analysis of variance conducted on the acoustic duration of the nasal consonant ratio within the /pimip/, /pamap/ and /pumup/ contexts, involving both subject groups, yielded significant effects for group (F(1, 170)=41.25, P<0.001) and context (F(2, 170)=70.22, P<0.001). However, it did not reveal any significant interaction between the contextual and group variables (F(2, 170)=6.42, P>0.05). Additionally, the acoustic duration of the nasal consonant ratio was significantly greater in cleft palate adults compared to the control group across all three vowel contexts. Subsequent analysis using the Duncan multiple comparison test demonstrated that, within both groups, the acoustic duration of the nasal consonant ratio in the vowel context of /i/ significantly exceeded that of the /u/ and /a/ vowel contexts. Furthermore, the acoustic duration of the nasal consonant ratio within the /u/ vowel context exhibited a significant extension compared to that of the /a/ vowel context.
The 2×2 mixed analysis of variance applied to assess the nasal offset interval ratio in the /pimip/, /pamap/ and /pumup/ contexts across both subject groups revealed significant effects for group (FF(1, 170)=34.06, P<0.000), context (F(2, 170)=65.41, P<0.000) and a significant interaction between contextual and group variables (F(2, 170)=43.28, P<0.001). Furthermore, the nasal offset interval ratio was significantly higher in cleft palate adults compared control group across all three vowel contexts. Subsequent examination using the Duncan multiple comparison test indicated that, within both groups, the nasal offset interval ratio of the /i/ vowel context was significantly greater than that of the /u/ and /a/ vowel contexts. Additionally, the nasal offset interval ratio of the /u/ vowel context exhibited a significant extension compared to that of the /a/ vowel context.
The 2×2 mixed analysis of variance conducted to assess the total nasalization duration ratio within the /pimip/, /pamap/ and /pumup/ contexts across both subject groups revealed significant effects for group (F(1, 170)=98.11, P<0.000), context (F(2, 170)=26.54, P<0.001) and a significant interaction between contextual and group variables (F(2, 170)=9.62, P<0.001). Additionally, the total nasalization duration ratio was notably higher in adults with cleft palate compared to adults without cleft palate across all three vowel contexts. Further investigation using the Duncan multiple comparison test indicated that, within both groups, the total nasalization duration ratio of the /i/ vowel context was significantly greater than those of the /u/ and /a/ vowel contexts, and the total nasalization duration ratio of the /u/ vowel context exhibited a significant extension compared to that of the /a/ vowel context.
Discussion
This study investigated the temporal characteristics of velopharyngeal coarticulation in Persian-speaking adults, comparing subjects with and without cleft palate. The outcomes unveiled that adults with cleft palate exhibited notably extended nasal onset interval ratios, nasal offset interval ratios, and total nasalization duration ratios across various vowel contexts. These findings align with prior research by Warren et al. (1985, 1990), Dalston et al. (1991) and Dotevall et al. (2002), which similarly reported significant distinctions in nasal airflow duration between normal and cleft palate subjects [5, 6, 7, 8]. The observation of prolonged velopharyngeal openness in Persian-speaking adults with cleft palate underscores the need for targeted interventions. Armed with insights into the temporal aspects of velopharyngeal closure, clinicians can develop precise clinical assessments and tailored intervention strategies for Persian-speaking adults with cleft palate.
The acoustic parameters derived from the analysis conducted in this study revealed alterations in the interaction between oral and nasal acoustic impedance, offering indirect insights into the timing dimensions of velopharyngeal coarticulation related to the movements of lips. Specifically, our research focused on examining temporal aspects when producing combinations of nasal-to-stop consonants. Measurements of temporal aspects in bilabial and velar positions revealed a close relationship between hypernasality in perceptual assessments and velopharyngeal function. Consequently, the phase of velopharyngeal closure may reflect the temporal characteristics of the pharyngeal valve, which are essential for understanding hypernasality in perceptual assessments in clinics.
From a coarticulation model perspective, the nasal onset interval ratio can be interpreted as indicative of anticipatory velopharyngeal coarticulation, while the nasal offset interval ratio aligns with carryover velopharyngeal coarticulation. Specifically, the nasal onset interval signifies the duration from the initiation of the opening of the velopharyngeal port to the closure of the oral cavity, whereas the nasal offset interval denotes the duration from the opening of the oral cavity to the closing of the velopharyngeal port. The comprehensive duration of velopharyngeal opening and closing can be deducted through the measurement of total nasalization duration [4].
According to the results, in the Persian language, adults with cleft palate demonstrate an earlier initiation of velopharyngeal port opening for nasal consonants and delayed closure of velopharyngeal port for oral consonants after nasal consonants, compared to the control group. This observation aligns with the research conducted by Baghban et al. (2015) concerning temporal aspects of nasalization in Persian-speaking children with and without cleft palate [14]. Essentially, this suggests that the patterns of velopharyngeal coarticulation exhibit similarities between Persian-speaking children and adults, both with and without cleft palate. Nevertheless, temporal intervals in adults, both with and without cleft palate, are shorter than those in children, both with and without cleft palate, across all three vowel contexts in the Persian language. The differences in temporal patterns of nasalization durations between adults and children, with and without cleft palate, may be partly attributed to variations in speech rates between these groups [2, 4].
The findings of this study were subjected to comparison with the research conducted by Baghban et al. (2015), revealing potential divergent underlying mechanisms governing how Persian-speaking adults and children, both with and without cleft palate, anticipate and carry over velopharyngeal coarticulation. This observation aligns with previous studies that have reported disparities in the temporal aspects of coarticulation between individuals of different age groups [2, 4, 13]. Coarticulation research literature consistently indicates a consensus that anticipatory and carryover coarticulation entail distinct underlying mechanisms. The mechanical inertia of the velum, leading to carryover velopharyngeal coarticulation, might remain consistent in both adults and children, whereas anticipatory velopharyngeal coarticulation could reflect developmental aspects involving the reorganization of neuromotor control for segmental articulations. Consequently, adults and children may exhibit differing temporal patterns within the domain of anticipatory velopharyngeal coarticulation [4, 13, 19].
In the case of adults with cleft palate, the nasal onset interval ratio, nasal offset ratio and total nasalization duration ratio exhibited significant variations across the three vowel contexts within each respective group. Furthermore, the outcomes of this study illuminated the presence of notable interactions between the subject groups and the specific vowel types concerning the three temporal durations. This implies that the nature and extent of group disparities in these temporal durations are influenced by the vowel categories under consideration. The temporal durations were ranked in ascending order as follows: /a/, /i/ and /u/. This outcome underscored that temporal duration ratios in high vowel contexts exceeded those observed in low vowel contexts. The heightened oral constriction associated with high vowel contexts likely contributed to longer nasal onset intervals, nasal offset intervals and total nasalization durations compared to those evident in low vowel contexts. This finding aligns with the results reported by Ha et al. and Ha and Kuehn (2004, 2011) in the context of Korean and American English [3, 13]. Additionally, it parallels the findings of Cho et al. (2000), where high vowels were found to exhibit a more pronounced and sensitive degree of nasalization about nasal-coupling balance compared to low vowels [20].
Within the scope of the present investigation, it became evident that the /pimip/ context exhibited the most pronounced disparities between the two groups. In a manner consistent with the findings of Baghban et al. (2015) concerning the timing aspects of nasalization in Persian-speaking children, our study likewise underscores that the temporal metrics of nasalization derived from the vowel context of /i/offer further discerning insights into the distinctions between groups with and without cleft palate. These temporal dissimilarities in nasalization during vowel production could potentially related to the perceived degree of nasalization [14]. This observation aligns with prior studies indicating that the /i/ context tends to be perceived as having a greater degree of nasal resonance compared to the /a/ context [3, 4, 13].
The acoustic spectrum of the /m/ nasal consonant is characterized by a prevalence of sound energy characterized by low frequency. Consequently, when the /i/ vowel and /m/ consonant, both featuring comparable formant placements, are articulated consecutively, the resonance near the nasal formant becomes more pronounced, thereby intensifying the perception of nasal resonance [4].
Kuehn and Moon (1995) conducted a study demonstrating that cleft palate participants exhibit elevated levels of levator veli palatini activation during speech production when in comparison to normal participants. This finding suggests that those with cleft palate may necessitate increased exertion to achieve velopharyngeal closure and could be more susceptible to fatigue during speech articulation [21]. The extended nasalization durations observed in the cleft palate group in our research could be indicative of atypical speech motor skills and anatomical disparities in the structure of the palate. Previous investigations have yielded similar data, but their outcomes have not consistently concurred. This variability underscores the potential for temporal characteristics of nasalization to vary among different languages. Therefore, a noteworthy strength of our study lies in the selection of our specific language for investigation.
Ultimately, the results garnered from our present study can offer valuable supplementary insights into the movements of the velum and lips, particularly in the context of imaging techniques like x-ray, magnetic resonance imaging, and ultrasound [22, 23].
Clinical and research implications
The current investigation has furnished more precise insights into the functioning of the velopharyngeal mechanism, thus enhancing the potential for more precise clinical evaluations and practical intervention strategies. Essentially, this research underscores the significance of carefully selecting speech patterns when evaluating and addressing velopharyngeal function, especially in the context of perceptual speech attributes like the phonetic placement of target phonemes. Our study has unveiled that among Persian-speaking adults, those with cleft palate tend to exhibit extended durations of nasalization compared to their non-cleft palate counterparts. Consequently, when appraising hypernasality in cleft speech and speech therapy settings, it is imperative to recognize that the temporal dimensions of nasalization can be influenced by the degree of hypernasality in adults with cleft palate. These findings hold relevance not only for speech and language pathologists but also for linguists and other specialists collaborating within cleft palate teams.
Conclusion
In this investigation, Persian adults with cleft palate demonstrated significantly prolonged nasalization durations in comparison to their non-cleft palate counterparts. The analysis undertaken in this study delved not only into the acoustic energy ratios but also into the acoustic events linked to the temporal dimensions of velopharyngeal coarticulation, particularly about the timing of lip opening and closure throughout the articulation process. The most conspicuous disparity between these two groups emerged within the context of the vowel /i/. This research contributed acoustic evidence related to velopharyngeal coarticulation, lending support to the expectations set forth by the coproduction model regarding the extent of anticipatory and carryover coarticulation, as well as aligning with the predictions of gestural phonology concerning the nature of speech production units and the speech patterns observed in adults.
Study limitations
The data analysis approach employed in this study primarily focused on the temporal characteristics of velopharyngeal movement related to the opening and closing of the lip, rather than emphasizing the rate of acoustic energy. Future investigations could explore the connection between temporal attributes and nasalization using alternative indirect assessment tools. Given that patterns of nasalization can exhibit variability across specific languages, it is essential to recognize that the temporal aspects of velopharyngeal coarticulation in this study may have limitations specific to the Persian language. Consequently, extrapolating the results to other languages should be undertaken cautiously. An avenue for future research entails replicating this study on a more extensive scale, encompassing a significantly larger sample size, a broader age spectrum, and a more diverse array of regional dialects. The current study was confined to a limited set of speech tasks; therefore, forthcoming research should encompass additional speech samples spanning a wider array of vowels and consonants, including those with diverse places and manners of articulation. Moreover, in future research, it would be valuable to compare the temporal aspects of velopharyngeal coarticulation among groups with apraxia, dysarthria, and other resonance disorders.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Isfahan University of Medical Science (Code: IR.MUI.REC.1395.2.150). Before their involvement in the study, all participants were given a comprehensive explanation of the research procedure and its duration. Consent forms were made available to the adult participants, and their participation commenced following their informed consent.
Funding
This research was supported by the research project (No.: 295150), Funded by the Isfahan University of Medical Science.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Authors thank the Craniofacial and Cleft Research Center of the Isfahan University of Medical Science, the University of Social Welfare and Rehabilitation Sciences, and participants with and without cleft palate who participated eagerly in this study.
References
- Zharkova N, Hewlett N, Hardcastle WJ. Coarticulation as an indicator of speech motor control development in children: An ultrasound study. Motor Control. 2011; 15(1):118-40. [DOI:10.1123/mcj.15.1.118] [PMID]
- Kent RD. Research on speech motor control and its disorders: A review and prospective. Journal of Communication Disorders. 2000; 33(5):391-428. [DOI:10.1016/S0021-9924(00)00023-X] [PMID]
- Ha S, Sim H, Zhi M, Kuehn DP. An acoustic study of the temporal characteristics of nasalization in children with and without cleft palate. The Cleft Palate-Craniofacial Journal. 2004; 41(5):535-43. [DOI:10.1597/02-109.1] [PMID]
- Ha S, Kuehn DP. Temporal characteristics of nasalization in speakers with and without cleft palate. The Cleft Palate-Craniofacial Journal. 2011; 48(2):134-44. [DOI:10.1597/08-140] [PMID]
- Warren DW, Dalston RM, Trier WC, Holder MB. A pressure-flow technique for quantifying temporal patterns of palatopharyngeal closure. The Cleft Palate Journal. 1985; 22(1):11-9. [PMID]
- Warren DW, Dalston RM, Dalston ET. Maintaining speech pressures in the presence of velopharyngeal impairment. Cleft Palate Journal. 1990; 27(1):53-8; discussion 58-60. [DOI:10.1597/1545-1569_1990_027_0053_mspitp_2.3.co_2] [PMID]
- Dalston RM, Warren DW, Dalston ET. The temporal characteristics of aerodynamic phenomena associated with patients manifesting varying degrees of velopharyngeal adequacy. Folia Phoniatrica et Logopaedica. 1991; 43(5):226-33. [DOI:10.1159/000266131] [PMID]
- Dotevall H, Lohmander-Agerskov A, Ejnell H, Bake B. Perceptual evaluation of speech and velopharyngeal function in children with and without cleft palate and the relationship to nasal airflow patterns. The Cleft Palate-Craniofacial Journal. 2002; 39(4):409-24. [DOI:10.1597/1545-1569_2002_039_0409_peosav_2.0.co_2] [PMID]
- Jones DL. The relationship between temporal aspects of oral-nasal balance and classification of velopharyngeal status in speakers with cleft palate. The Cleft Palate-Craniofacial Journal. 2000; 37(4):363-9. [DOI:10.1597/1545-1569_2000_037_0363_trbtao_2.3.co_2] [PMID]
- Zajac DJ, Hackett AM. Temporal characteristics of aerodynamic segments in the speech of children and adults. The Cleft Palate-Craniofacial Journal. 2002; 39(4):432-8. [DOI:10.1597/1545-1569_2002_039_0432_tcoasi_2.0.co_2] [PMID]
- Jones DL. Patterns of oral-nasal balance in normal speakers with and without cleft palate. Folia Phoniatrica et Logopaedica. 2006; 58(6):383-91. [DOI:10.1159/000094999] [PMID]
- Bae Y, Kuehn DP, Ha S. Validity of the nasometer measuring the temporal characteristics of nasalization. The Cleft Palate-Craniofacial Journal. 2007; 44(5):506-17. [DOI:10.1597/06-128.1] [PMID]
- Ha S, Kuehn D. Temporal characteristics of nasalization in children and adult speakers of American English and Korean during production of three vowel contexts. The Journal of the Acoustical Society of America. 2006; 120(3):1622-30. [DOI:10.1121/1.2225382] [PMID]
- Baghban K, Torabinezhad F, Moradi N, Asadollahpour F, Ahmadi N, Mardani N. Temporal characteristics of nasalization in Persian speaker children with and without cleft palate. International Journal of Pediatric Otorhinolaryngology. 2015; 79(4):546-52. [DOI:10.1016/j.ijporl.2015.01.026] [PMID]
- Amirian A, Derakhshandeh F, Salehi A, Soleimani B. [Evaluating intra-and inter-rater relibility for cleft palate speech assessment test based on universal parameters system-in Persian (Persian)]. Journal of Research in Rehabilitation Sciences. 2011; 7(4):470-6. [Link]
- John A, Sell D, Sweeney T, Harding-Bell A, Williams A. The cleft audit protocol for speech-augmented: A validated and reliable measure for auditing cleft speech. The Cleft Palate-Craniofacial Journal. 2006; 43(3):272-88. [DOI:10.1597/04-141.1] [PMID]
- Howard S, Lohmander A. Cleft palate speech: Assessment and intervention. New Jersey: John Wiley & Sons; 2011. [DOI:10.1002/9781118785065]
- Behrman A. Speech and voice science. San Diego: Plural Publishing; 2021. [Link]
- Cychosz M, Edwards JR, Munson B, Johnson K. Spectral and temporal measures of coarticulation in child speech. The Journal of the Acoustical Society of America. 2019; 146(6):EL516. [DOI:10.1121/1.5139201] [PMID]
- Lee DP, Yang SW, Choi WC. The relation between nasal cavity size and success rate in endonasal dacryocystorhinostomy. Journal of the Korean Ophthalmological Society. 2000; 1183-23. [Link]
- Kuehn DP, Moon JB. Levator veli palatini muscle activity in relation to intraoral air pressure variation in cleft palate subjects. The Cleft Palate-Craniofacial Journal. 1995; 32(5):376-81. [PMID]
- Sato-Wakabayashi M, Inoue-Arai MS, Ono T, Honda E, Kurabayashi T, Moriyama K. Combined fMRI and MRI movie in the evaluation of articulation in subjects with and without cleft lip and palate. The Cleft Palate-Craniofacial Journal. 2008; 45(3):309-14. [DOI:10.1597/07-070] [PMID]
- Shinagawa H, Ono T, Honda E, Kurabayashi T, Iriki A, Ohyama K. Distinctive cortical articulatory representation in cleft lip and palate: A preliminary functional magnetic resonance imaging study.The Cleft Palate-Craniofacial Journal. 2006; 43(5):620-4. [DOI:10.1597/05-027] [PMID]
Article type: Original Research Articles |
Subject:
Speech therapy
Received: 2023/04/9 | Accepted: 2023/10/23 | Published: 2024/09/1
Received: 2023/04/9 | Accepted: 2023/10/23 | Published: 2024/09/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
