
988368
Sat, Jun 20, 2026

Volume 24, Issue 1 (March 2026)
Iranian Rehabilitation Journal 2026, 24(1): 99-112 |
Back to browse issues page



Ethics code: IR.IUMS.REC.1401.246
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Reaei P, Amini M, Saneii S H, Khalafbeigi M, Shahebrahimi S P, Ehteshami S. Neurodevelopmental Handling Skills for Parents of Children With Cerebral Palsy: A Randomized Control Trial. Iranian Rehabilitation Journal 2026; 24 (1) :99-112
URL: http://irj.uswr.ac.ir/article-1-2431-en.html
URL: http://irj.uswr.ac.ir/article-1-2431-en.html
Pooya Reaei1 

 , Malek Amini *1 , Seyed Hassan Saneii1 , Mitra Khalafbeigi1 , Seyyed Pedram Shahebrahimi1 , Sahar Ehteshami2
, Malek Amini *1 , Seyed Hassan Saneii1 , Mitra Khalafbeigi1 , Seyyed Pedram Shahebrahimi1 , Sahar Ehteshami2
, Malek Amini *1 , Seyed Hassan Saneii1 , Mitra Khalafbeigi1 , Seyyed Pedram Shahebrahimi1 , Sahar Ehteshami2
1- Department of Occupational Therapy, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Occupational Therapy, School of Rehabilitation Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Occupational Therapy, School of Rehabilitation Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 702 kb]
(163 Downloads)
| Abstract (HTML) (1127 Views)
Full-Text: (14 Views)
Introduction
Cerebral palsy (CP) is a group of motor disorders often accompanied by sensory, cognitive, communication, perception, and behavioral issues, as well as epilepsy, nutrition, dysphagia, and oral motor dysfunction [1]. The neurodevelopmental approach is a fundamental strategy in addressing motor development for individuals with CP, with handling techniques serving as a primary therapeutic modality [2]. These techniques aim to enhance neurotransmitter input to the brain, fostering the creation of neural maps through stimulating proprioception and facilitating the neurodevelopmental process [3]. Therapists employ specialized manipulation techniques to reinforce postural reactions and movements in children, providing a more natural sensory and motor experience alongside therapeutic activities [4].
Handling and positioning are critical components of the neurodevelopmental approach because they help facilitate natural movement patterns, improve postural control, and enhance motor learning. Proper positioning and handling techniques can improve alignment, stability, and increase mobility [3, 5]. This approach considers the unique needs and abilities of each child, with the techniques used in handling and positioning being tailored to the specific disorders and goals of the individual [2, 6].
The desired output resulting from the application of the neurodevelopmental approach and its various techniques is often used in the clinical environment by therapists, which is possible only during a few limited sessions during the week. Children with CP spend significant hours of the day in a non-therapeutic environment with their families, highlighting the crucial role family participation plays in implementing prescribed exercises by the therapist outside the therapeutic environment, allowing children with CP to continually benefit from necessary interventions [7].
Sharif Azar et al. (2015) conducted a study in the same field that pointed to the greater effectiveness of home-based interventions compared to interventions based in medical centers [8]. Many studies have been conducted, particularly among Iranian families with children with CP, which indicate the necessity of empowering this group of parents, which can be achieved with positive and all-round support from occupational therapists [7, 9-12]. Empowerment can be interpreted as an individual’s capacity to take responsibility for one’s life [13]. Parents of children with CP are affected by their child’s health conditions in many aspects, such as time management, occupational balance, and quality of life [7, 12, 14]. These parents require positive support and increased satisfaction with their child’s treatment sessions to better manage existing conditions [11, 15]. Studies show that guiding mothers with children who have CP in the field of occupational implementation can be effective in increasing their self-sufficiency, and, as a result, empowering them through intervention [16]. A study conducted provided a family empowerment program to families with children with CP and achieved similar results [17].
Despite these previous studies, there remains a need to investigate the effectiveness of group training in handling skills for parents of children with CP. This study aims to address this gap by examining the impact of such training on children’s functional mobility, a critical aspect of independent living. The specific research questions are:
1) Is 8 weeks of group handling training to parents of children with CP effective at improving children’s gross motor function and mobility function? 2) Are any benefits maintained 8 weeks after the period of intervention? 3) Can group handling training empower parents?
By addressing these questions, this study can contribute to the existing literature on CP interventions, potentially leading to improved therapeutic approaches and better outcomes for children with CP and their families.
Materials and Methods
Study design and participants
Our single-blinded, randomized controlled trial was conducted between 2023 and 2024 at the Tavanyab Charity Center in Tehran City, Iran. Forty-six children with spastic CP aged 3-10 years were recruited through referrals and included in the study. An independent recruiter screened the participants, performed initial measurements, and stratified them into three classes based on the gross motor function classification system (GMFCS): GMFCS 1-2, GMFCS 3, and GMFCS 4-5. Participants were then randomly assigned to either the control or intervention group, and groups were homogenized based on GMFCS level to minimize the impact of random variables in statistical analysis. We included two additional participants per group to account for potential dropouts. The inclusion criteria comprised families with sufficient command of the Persian language, effective presence of the mother during intervention, and no plans for specialized surgery during the intervention period. The exclusion criteria included vision problems, unwillingness to continue participating in the study, and the occurrence of illness or other issues during the intervention.
Study intervention
The control group received 8 weeks of routine occupational therapy interventions delivered by an occupational therapist with at least one year of pediatric physical disability experience. In addition to routine interventions, the intervention group received specialized group training, which involved 5 workshop sessions addressing family awareness and appropriate handling and positioning techniques. The control group was offered specialized group training after the trial’s completion.
Outcomes were measured at baseline (before the intervention), 1 month after the intervention start, at the end of the intervention (the eighth week), and twice under follow-up (1 and 2 months after intervention completion) by a blinded assessor. Post-training, parents implemented acquired skills at home for 2 months, with continuous monitoring via phone calls and face-to-face interactions.
Group training sessions
The sessions were as follows:
1) Overview session: It covered the nature, causes, types, and symptoms of CP, functional levels, prognosis, associated disorders, and common occupational therapy interventions. 2) Discussion session: It facilitated a forum for parents to discuss challenges related to handling their children, musculoskeletal pains, and disruptions to their quality of life. 3) Functional problems session: It explored children’s functional problems, inviting parents to articulate challenges faced in various occupational areas. 4 & 5) Intervention preparation sessions: It was based on analyses from prior discussions, the researcher formulated targeted interventions presented in subsequent workshops, and parents practiced handling and positioning techniques.
Assessment tools and measures
The gross motor function measure-88 (GMFM-88), developed by Russell et al. (1989), serves as a reliable instrument for evaluating the gross motor performance of children [18]. It comprises five distinct subscales: lying and rolling, sitting, crawling and kneeling, standing, and walking, running, and jumping. Each item within these subscales is assigned a score ranging from 0 to 4, indicative of varying degrees of motor proficiency. Salehi et al. (2015) validated and established the tool’s reliability, reporting intra-examiner and inter-examiner correlation coefficients of 0.99 and an internal consistency Cronbach α ranging from 0.78 to 0.94 [19].
The pediatric evaluation of disability inventory (PEDI), developed by Haley (2000), assesses children’s performance across three scales: functional skill, caregiver assistance, and modification [20]. The self-care dimension of the functional skill scale, containing 73 items, measures the child’s ability to perform daily activities independently. Grading options include zero and one [21]. Abbasabadi et al. (2015) confirmed the questionnaire’s reliability, reporting Cronbach α values between 0.94 and 0.97 and test re-test reliability of 0.97 for the functional skill scale and 0.96 for the modifications scale [22].
The family empowerment scale (FES), introduced by Koren et al, measures family empowerment. Comprising three subscales (family, service system, and community/political), this tool scores items on a scale from 1 to 5 [23]. Rajabi and Zolmajd validated and confirmed the reliability of the Persian FES through a test re-test method, reporting reliability coefficients of 0.86 and Cronbach α of internal consistency of 0.94 [24].
The GMFCS is an observational standard classification system designed to categorize children with CP up to the age of 18. This classification is based on their present gross motor abilities, limitations in gross motor function, and the necessity for assistive technology and wheeled mobility. The system stratifies individuals into 5 distinct levels, where level 1 signifies maximum independence, and level 5 indicates the minimum level of independence in performance [25]. The GMFCS has been translated and validated in Iran by Dehghan et al. (2011), affirming its applicability and relevance in diverse settings [26]. The demographic information questionnaire utilized in this study systematically gathers vital demographic data, encompassing the child’s age and gender, as well as parental details such as age and education level.
Statistical analysis
All measures were analyzed using an intention-to-treat analysis. Descriptive statistics were calculated for all variables at 5 time points: Weeks 0, 4, 8, 12, and 16. Descriptive statistics, including the calculation of mean and standard deviation for quantitative variables and frequency and percentage for qualitative variables, were employed to present a comprehensive overview of data distribution and changes. The normal distribution of quantitative variables was assessed using the Shapiro-Wilk test.
Analysis of covariance (ANCOVA) was utilized to evaluate the significance and impact of the intervention on the studied outcomes. This statistical method enables the comparison of average scores between the control and intervention groups during and after the intervention while controlling for influential variables and baseline values.
The effect size, measured through partial eta square (η2p), was computed and reported for the ANCOVA model. Interpretation of η2p values is as follows: 0.01-0.06 represents a small effect size, 0.06-0.14 indicates a medium effect size, and values exceeding 0.14 signify a large effect size.
Statistical analysis was conducted using SPSS software, version 16, with a predetermined significance level of 0.05.
Results
Individual and clinical characteristics of study participants
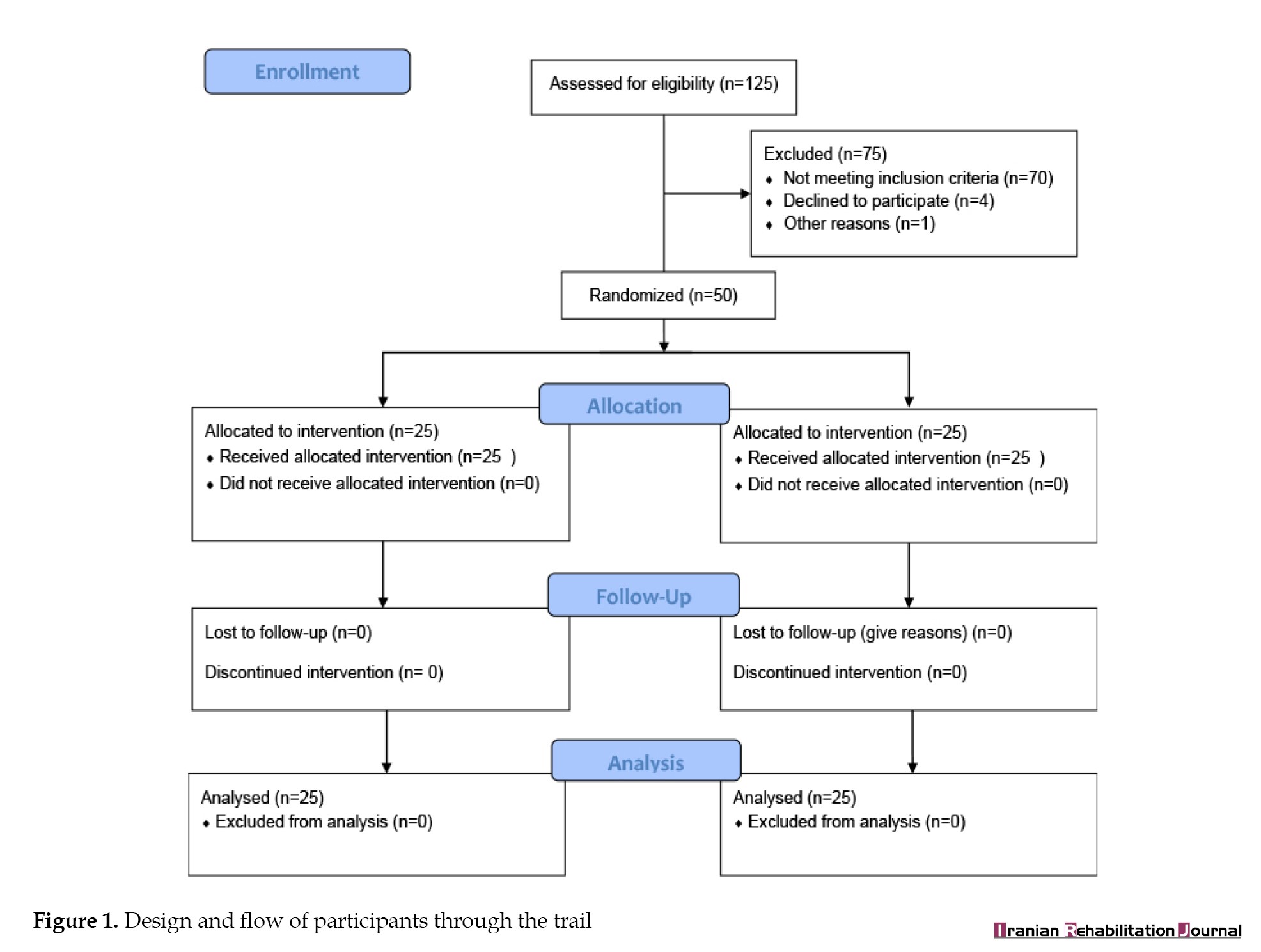
A total of 125 children with CP were screened for eligibility (Figure 1).
Cerebral palsy (CP) is a group of motor disorders often accompanied by sensory, cognitive, communication, perception, and behavioral issues, as well as epilepsy, nutrition, dysphagia, and oral motor dysfunction [1]. The neurodevelopmental approach is a fundamental strategy in addressing motor development for individuals with CP, with handling techniques serving as a primary therapeutic modality [2]. These techniques aim to enhance neurotransmitter input to the brain, fostering the creation of neural maps through stimulating proprioception and facilitating the neurodevelopmental process [3]. Therapists employ specialized manipulation techniques to reinforce postural reactions and movements in children, providing a more natural sensory and motor experience alongside therapeutic activities [4].
Handling and positioning are critical components of the neurodevelopmental approach because they help facilitate natural movement patterns, improve postural control, and enhance motor learning. Proper positioning and handling techniques can improve alignment, stability, and increase mobility [3, 5]. This approach considers the unique needs and abilities of each child, with the techniques used in handling and positioning being tailored to the specific disorders and goals of the individual [2, 6].
The desired output resulting from the application of the neurodevelopmental approach and its various techniques is often used in the clinical environment by therapists, which is possible only during a few limited sessions during the week. Children with CP spend significant hours of the day in a non-therapeutic environment with their families, highlighting the crucial role family participation plays in implementing prescribed exercises by the therapist outside the therapeutic environment, allowing children with CP to continually benefit from necessary interventions [7].
Sharif Azar et al. (2015) conducted a study in the same field that pointed to the greater effectiveness of home-based interventions compared to interventions based in medical centers [8]. Many studies have been conducted, particularly among Iranian families with children with CP, which indicate the necessity of empowering this group of parents, which can be achieved with positive and all-round support from occupational therapists [7, 9-12]. Empowerment can be interpreted as an individual’s capacity to take responsibility for one’s life [13]. Parents of children with CP are affected by their child’s health conditions in many aspects, such as time management, occupational balance, and quality of life [7, 12, 14]. These parents require positive support and increased satisfaction with their child’s treatment sessions to better manage existing conditions [11, 15]. Studies show that guiding mothers with children who have CP in the field of occupational implementation can be effective in increasing their self-sufficiency, and, as a result, empowering them through intervention [16]. A study conducted provided a family empowerment program to families with children with CP and achieved similar results [17].
Despite these previous studies, there remains a need to investigate the effectiveness of group training in handling skills for parents of children with CP. This study aims to address this gap by examining the impact of such training on children’s functional mobility, a critical aspect of independent living. The specific research questions are:
1) Is 8 weeks of group handling training to parents of children with CP effective at improving children’s gross motor function and mobility function? 2) Are any benefits maintained 8 weeks after the period of intervention? 3) Can group handling training empower parents?
By addressing these questions, this study can contribute to the existing literature on CP interventions, potentially leading to improved therapeutic approaches and better outcomes for children with CP and their families.
Materials and Methods
Study design and participants
Our single-blinded, randomized controlled trial was conducted between 2023 and 2024 at the Tavanyab Charity Center in Tehran City, Iran. Forty-six children with spastic CP aged 3-10 years were recruited through referrals and included in the study. An independent recruiter screened the participants, performed initial measurements, and stratified them into three classes based on the gross motor function classification system (GMFCS): GMFCS 1-2, GMFCS 3, and GMFCS 4-5. Participants were then randomly assigned to either the control or intervention group, and groups were homogenized based on GMFCS level to minimize the impact of random variables in statistical analysis. We included two additional participants per group to account for potential dropouts. The inclusion criteria comprised families with sufficient command of the Persian language, effective presence of the mother during intervention, and no plans for specialized surgery during the intervention period. The exclusion criteria included vision problems, unwillingness to continue participating in the study, and the occurrence of illness or other issues during the intervention.
Study intervention
The control group received 8 weeks of routine occupational therapy interventions delivered by an occupational therapist with at least one year of pediatric physical disability experience. In addition to routine interventions, the intervention group received specialized group training, which involved 5 workshop sessions addressing family awareness and appropriate handling and positioning techniques. The control group was offered specialized group training after the trial’s completion.
Outcomes were measured at baseline (before the intervention), 1 month after the intervention start, at the end of the intervention (the eighth week), and twice under follow-up (1 and 2 months after intervention completion) by a blinded assessor. Post-training, parents implemented acquired skills at home for 2 months, with continuous monitoring via phone calls and face-to-face interactions.
Group training sessions
The sessions were as follows:
1) Overview session: It covered the nature, causes, types, and symptoms of CP, functional levels, prognosis, associated disorders, and common occupational therapy interventions. 2) Discussion session: It facilitated a forum for parents to discuss challenges related to handling their children, musculoskeletal pains, and disruptions to their quality of life. 3) Functional problems session: It explored children’s functional problems, inviting parents to articulate challenges faced in various occupational areas. 4 & 5) Intervention preparation sessions: It was based on analyses from prior discussions, the researcher formulated targeted interventions presented in subsequent workshops, and parents practiced handling and positioning techniques.
Assessment tools and measures
The gross motor function measure-88 (GMFM-88), developed by Russell et al. (1989), serves as a reliable instrument for evaluating the gross motor performance of children [18]. It comprises five distinct subscales: lying and rolling, sitting, crawling and kneeling, standing, and walking, running, and jumping. Each item within these subscales is assigned a score ranging from 0 to 4, indicative of varying degrees of motor proficiency. Salehi et al. (2015) validated and established the tool’s reliability, reporting intra-examiner and inter-examiner correlation coefficients of 0.99 and an internal consistency Cronbach α ranging from 0.78 to 0.94 [19].
The pediatric evaluation of disability inventory (PEDI), developed by Haley (2000), assesses children’s performance across three scales: functional skill, caregiver assistance, and modification [20]. The self-care dimension of the functional skill scale, containing 73 items, measures the child’s ability to perform daily activities independently. Grading options include zero and one [21]. Abbasabadi et al. (2015) confirmed the questionnaire’s reliability, reporting Cronbach α values between 0.94 and 0.97 and test re-test reliability of 0.97 for the functional skill scale and 0.96 for the modifications scale [22].
The family empowerment scale (FES), introduced by Koren et al, measures family empowerment. Comprising three subscales (family, service system, and community/political), this tool scores items on a scale from 1 to 5 [23]. Rajabi and Zolmajd validated and confirmed the reliability of the Persian FES through a test re-test method, reporting reliability coefficients of 0.86 and Cronbach α of internal consistency of 0.94 [24].
The GMFCS is an observational standard classification system designed to categorize children with CP up to the age of 18. This classification is based on their present gross motor abilities, limitations in gross motor function, and the necessity for assistive technology and wheeled mobility. The system stratifies individuals into 5 distinct levels, where level 1 signifies maximum independence, and level 5 indicates the minimum level of independence in performance [25]. The GMFCS has been translated and validated in Iran by Dehghan et al. (2011), affirming its applicability and relevance in diverse settings [26]. The demographic information questionnaire utilized in this study systematically gathers vital demographic data, encompassing the child’s age and gender, as well as parental details such as age and education level.
Statistical analysis
All measures were analyzed using an intention-to-treat analysis. Descriptive statistics were calculated for all variables at 5 time points: Weeks 0, 4, 8, 12, and 16. Descriptive statistics, including the calculation of mean and standard deviation for quantitative variables and frequency and percentage for qualitative variables, were employed to present a comprehensive overview of data distribution and changes. The normal distribution of quantitative variables was assessed using the Shapiro-Wilk test.
Analysis of covariance (ANCOVA) was utilized to evaluate the significance and impact of the intervention on the studied outcomes. This statistical method enables the comparison of average scores between the control and intervention groups during and after the intervention while controlling for influential variables and baseline values.
The effect size, measured through partial eta square (η2p), was computed and reported for the ANCOVA model. Interpretation of η2p values is as follows: 0.01-0.06 represents a small effect size, 0.06-0.14 indicates a medium effect size, and values exceeding 0.14 signify a large effect size.
Statistical analysis was conducted using SPSS software, version 16, with a predetermined significance level of 0.05.
Results
Individual and clinical characteristics of study participants
A total of 125 children with CP were screened for eligibility (Figure 1).
Of these, 75 were excluded and 50 invited and were enrolled in the trial. Of these, 25 were randomized to the experimental group and 25 to the control group.
Table 1 presents the individual and clinical characteristics of the children and their parents involved in the study.
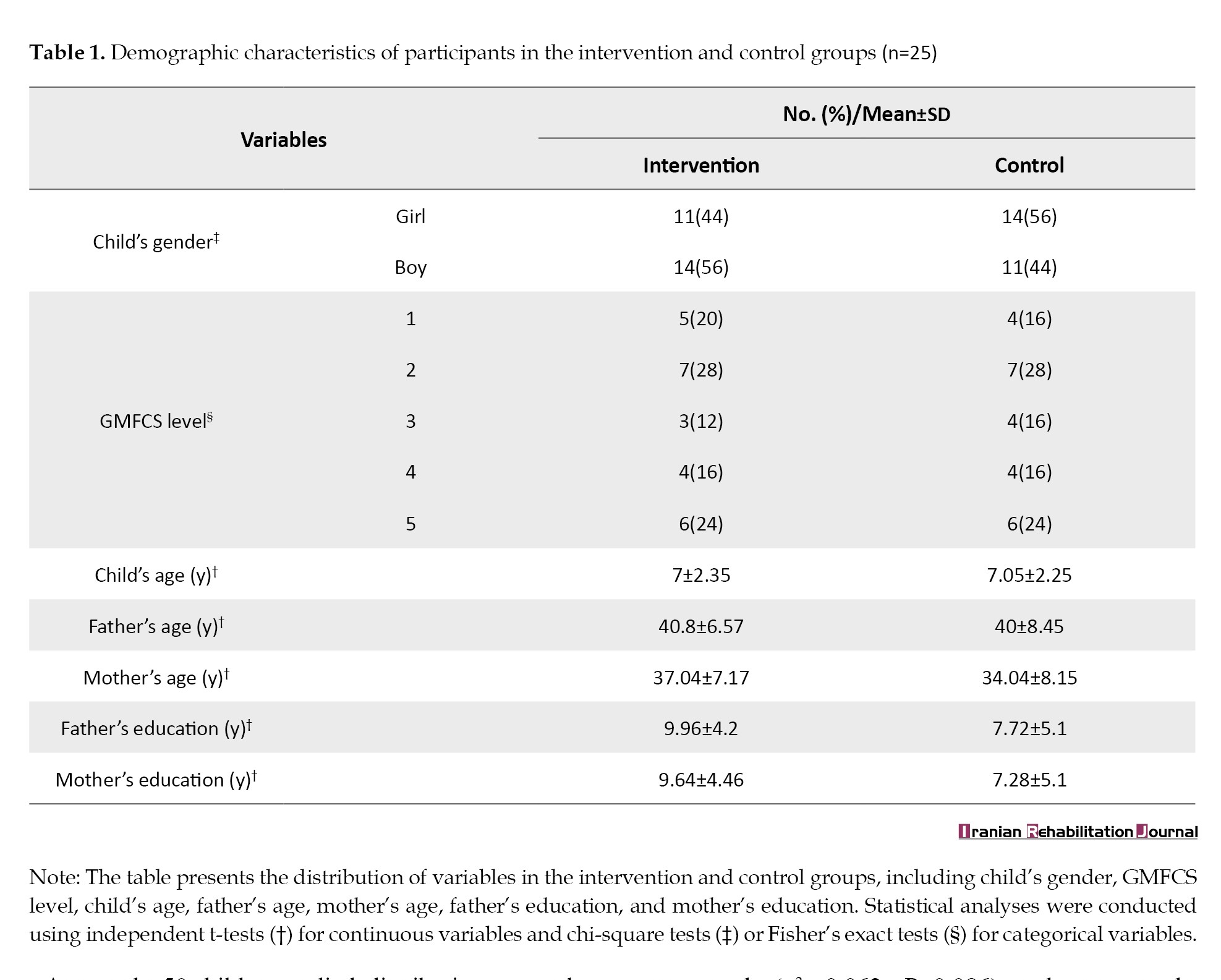
The average age of the studied children was 7.02±2.27 years, with a gender distribution of 50.0% boys. Fathers had an average age of 40.40±7.50 years, mothers had an average age of 35.54±7.75 years, and both parents had an average education level of 8.84±4.76 and 8.8±4.89 years, respectively.
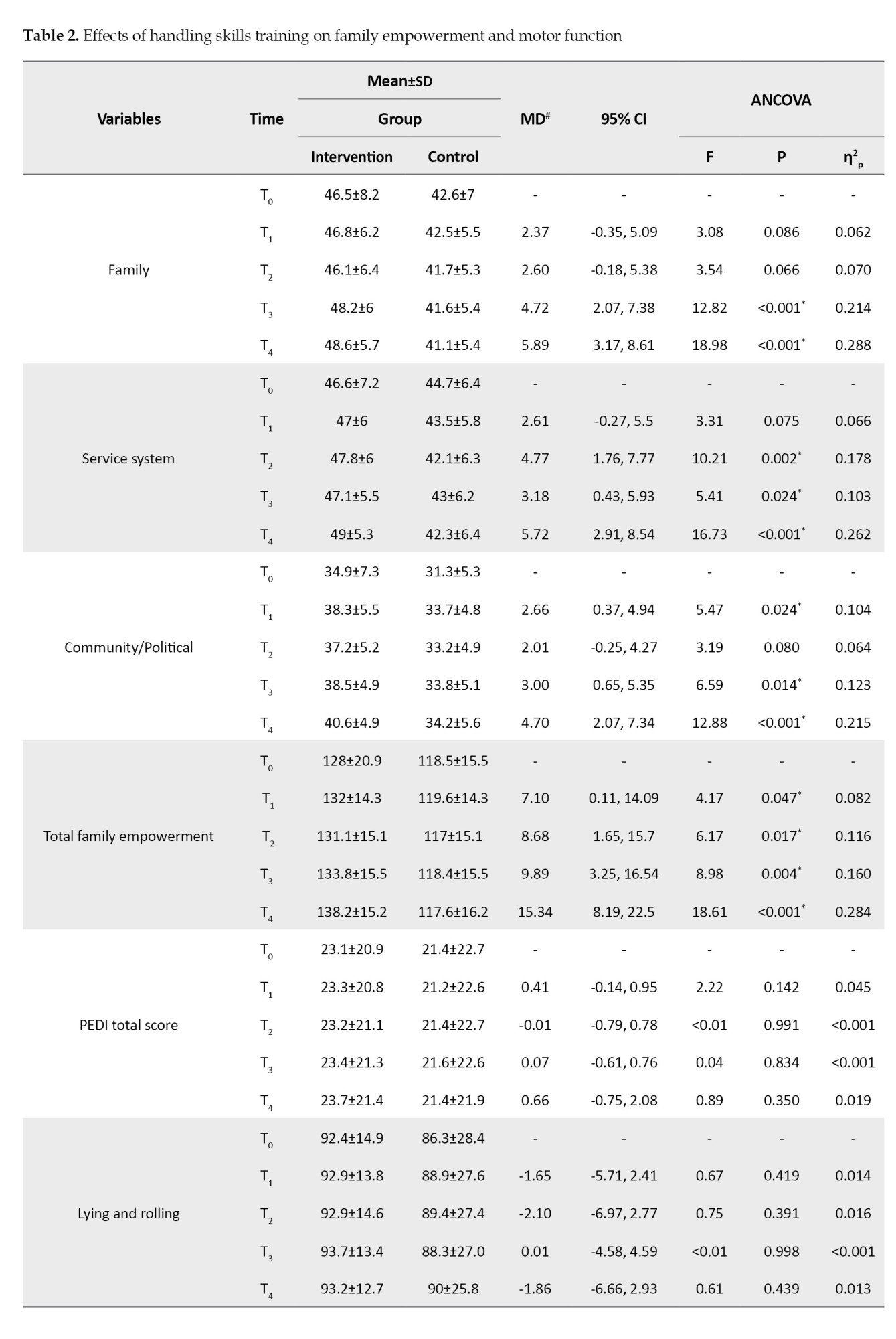
Among the 50 children studied, distributions were observed in terms of GMFCS levels. For instance, 24% of children exhibited GMFCS level 5. Table 1 demonstrates the homogeneity between the control and intervention groups across all individual and clinical variables, ensuring comparable participant characteristics in both groups. Data for 5 measurement occasions are presented in Table 2 for all outcome measures.
Family empowerment (FES) total score and subscale scores)
FES total score: The intervention group exhibited significantly higher FES total scores 1month post-intervention (η2p=0.082, P=0.047), persisting at 2 months (η2p=0.116, P=0.017), 1-month post-intervention conclusion (η2p=0.160, P=0.004), and 2 months post-intervention conclusion (η2p=0.284, P<0.001). These findings underscore the sustained positive influence of the intervention on the FES total score.
Family subscale scores: Covariance analysis, adjusting for pre-intervention values, revealed no statistically significant differences in family subscale scores one month (η2p=0.062, P=0.086) and two months (η2p=0.070, P=0.066) after initiation. However, post-intervention saw a notable increase in the intervention group’s family subscale scores. One-month post-intervention witnessed a substantial 4.72-unit rise (η2p=0.214, P<0.001), persisting at two months with a 5.89-unit increase (η2p=0.288, P=0.001), emphasizing the intervention’s positive impact on family-related outcomes.
Service systems subscale scores: While one-month post-intervention showed no significant difference (η2p=0.066, P=0.075), the intervention group demonstrated a marked increase in service systems subscale scores compared to the control group (η2p=0.178; P=0.002; 95% CI, 1.76%). This superiority persisted at 1 month (η2p=0.103, P=0.024) and two months (η2p=0.262, P<0.001), highlighting the positive influence of the intervention on service systems-related outcomes.
Community/political subscale score: Covariance analysis, adjusting for pre-intervention values, revealed a significant increase in the intervention group’s community/political subscale scores 1-month post-intervention (η2p=0.104, P=0.024), persisting at 1 month (η2p=0.123, P=0.014) and 2 months (η2p=0.215, P<0.001) after intervention conclusion. The intervention consistently led to significantly higher scores compared to the control group, indicating positive influence.
Mobility function (PEDI) total score
PEDI total score: Covariance analysis showed no significant differences in total PEDI scores between control and intervention groups one month (η2p=0.045, P=0.142) and 2 months (η2p=0.019, P=0.350) post-intervention. Comparable impact was observed, indicating no statistically significant differences in this outcome measure.
Gross motor function (GMFM-88) total score and subscale scores)
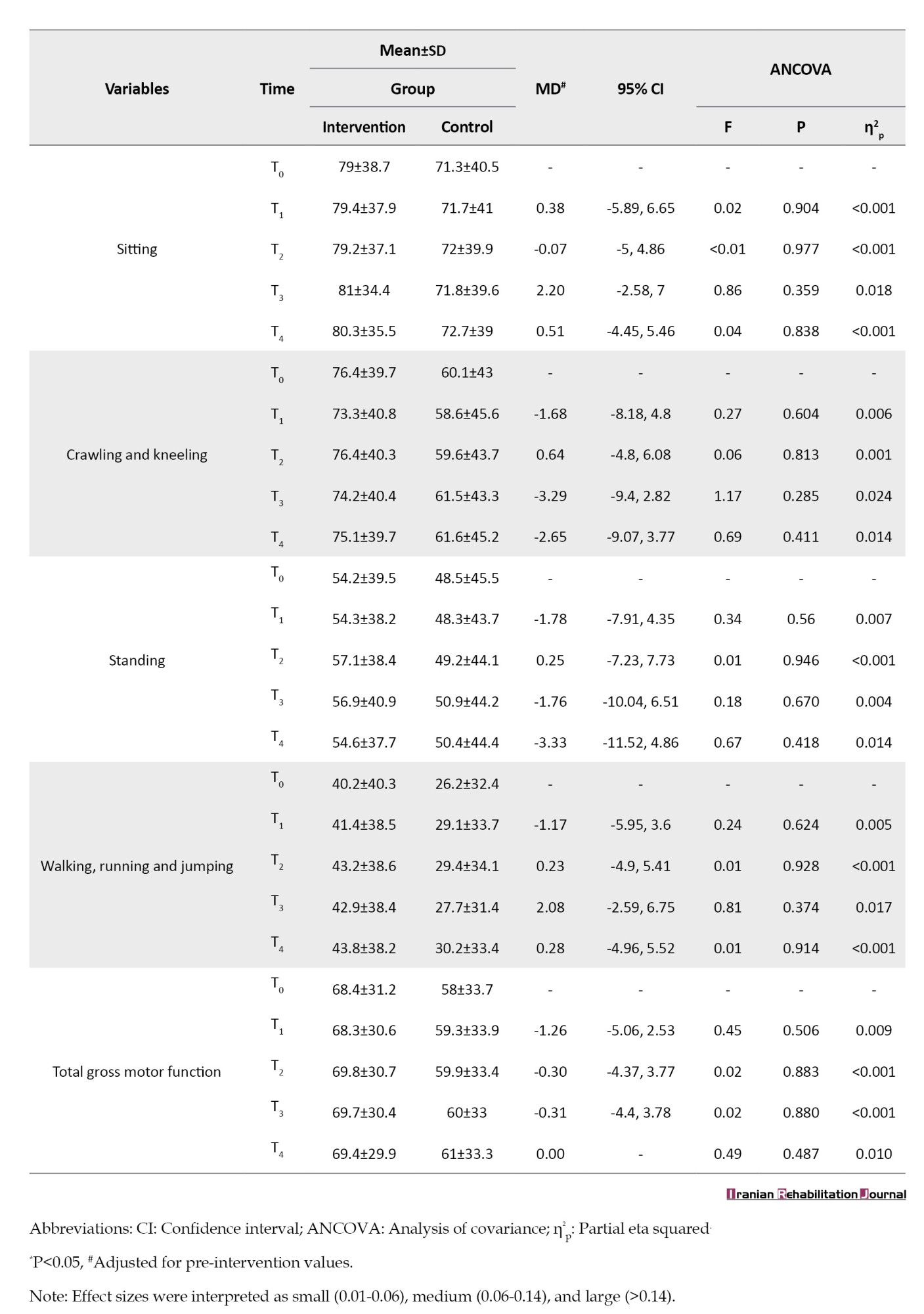
GMFM-88 total score: No statistically significant impact on GMFM-88 total scores was identified between control and intervention groups 1 month (η2p=0.009, P=0.506) and two months (η2p=0.010, P=0.487) post-intervention. Consistency in outcomes was observed across the study duration.
Lying and rolling score: No significant differences in lying and rolling scores were observed between groups 1 month (η2p=0.014, P=0.419) and 2 months (η2p=0.013, P=0.439) post-intervention. Outcomes remained comparable, suggesting the intervention did not yield significant differences in this aspect.
Sitting score: No significant differences in sitting scores were noted between groups one month (η2p<0.001, P=0.904) and two months (η2p<0.001, P=0.977) post-intervention. Consistent outcomes were maintained, indicating no significant impact on sitting scores.
Crawling and kneeling scores: No significant differences in crawling and kneeling scores were identified between groups 1 month (η2p=0.006, P=0.604) and 2 months (η2p=0.014, P=0.411) post-intervention. Similar outcomes were sustained, suggesting no significant impact on crawling and kneeling scores.
Standing scores: No significant variations in standing scores were found between groups one month (η2p=0.007, P=0.562) and 2 months (η2p=0.014, P=0.418) post-intervention. Consistency in outcomes indicated no significant impact on standing scores.
Walking, running, and jumping scores: No significant variations in walking, running, and jumping scores were observed between groups one month (η2p=0.005, P=0.624) and two months (η2p<0.001, P=0.914) post-intervention. Consistent outcomes suggested no significant impact on these scores.
Discussion
This systematic study sought to explore the consequences of group training in handling skills on multiple aspects related to children diagnosed with CP. By examining the domains of gross motor function, functional mobility, and parental capabilities, this investigation contributes to the existing body of literature on interventions for CP.
Effect of intervention on parental ability
An examination of parental ability reveals nuanced results. Covariance analysis conducted within the first month of intervention initiation indicates no significant differences in the family subscale score between the intervention and control groups. This initial observation suggests limited short-term intervention effects on family subscale scores. However, a noteworthy shift is discernible 1-month post-intervention cessation, with the intervention group displaying significantly higher average family subscale scores compared to the control group. This improvement persists two months post-intervention conclusion, substantiating a sustained positive impact on family subscale scores.
As it was said in the explanation of the concept of the family subscale in the assessment tools section, this subscale deals with the parents’ understanding of the child’s conditions, the ability of the parents to acquire the necessary knowledge and skills and use them to solve the child’s potential problems in the implementation of daily activities and, according to the topic of each of the group training sessions of the present study, in which the participating mothers were taught information about the general conditions of CP, accompanying disorders, how to handle children in each of the frequently used situations of life, it can be seen that after one month of the beginning of the trainings No significant difference was observed in the family subscale between the intervention and control groups, but with the passage of another month after the intervention and the completion of the aforementioned handling training to the mothers of the intervention group, the difference in the family subscale gradually became noticeable and significant. We witnessed a significant improvement in the decision-making ability and effective action of the parents of the intervention group in facing their children’s daily situations and problems.
Similar to the family subscale scores, the service systems subscale exhibits no significant differences within the first month of intervention. However, a contrasting picture emerges post-intervention, with the intervention group exhibiting a remarkable increase in scores. This figure exceeds the control group’s average scores by 5.7 and 4.1 points, 1 and 2 months post-intervention, respectively, corroborating the positive influence and improvement of service systems subscale scores over time. The community/political subscale demonstrates a similar trend, with significant score increases observed one month post-intervention, persisting over the long term.
The total FES score manifests a considerable increase within one month of intervention initiation in the intervention group, contrasting with the control group. This positive influence persists post-intervention, maintaining statistically higher scores in the intervention group one and two months thereafter.
Overall impact and long-term efficacy
Totally, the results of this research demonstrate that within one month after the start of the intervention, the average total FES score in the intervention group was significantly higher than in the control group. These findings confirm the positive effect and improvement of the FES total score due to the effectiveness of the intervention. Moreover, the positive impact of the intervention on the total FES score was maintained in the intervention group after the end of the intervention and one and two months thereafter, with the average score remaining significantly higher than the control group.
Overall, the results of this study indicate that the group training intervention of handling skills positively affects parental ability. The effectiveness of this intervention across various FES subscales, including family, service, and social/political systems, suggests that the intervention successfully enhances multiple aspects of family and social life. Additionally, the long-term effectiveness of the intervention has been observed, highlighting the stability of these effects over time.
These findings align with previous research in the field. Lorentzen et al. (2015) demonstrated that interactive educational programs at home can improve parental ability and involvement in the treatment of children with CP [27]. Similarly, Chiu et al. (2014) reached a comparable conclusion [28]. In general, the results of this study, corroborating previous studies, confirm the enhancement of parental ability in children with CP [29-31]. These findings address the need for evaluating the effectiveness of home-based programs, as emphasized by Beckers et al. (2020), who highlighted a strong recommendation for implementing such programs despite the lack of sufficient research [32].
A notable difference between the current study and previous research is the measurement of the long-term effects of training provided to mothers, extending up to two months after the conclusion of interventions. This unique aspect of the study reveals the stability of the training’s impact on family empowerment over an extended period, which had not been previously examined. Earlier studies focused on evaluations conducted at the completion of interventions, lacking a long-term follow-up assessment.
Effect of intervention on PEDI total score
In assessing the impact of the intervention on the PEDI total score, the study reveals an absence of statistically significant differences between the intervention and control groups within the first month of intervention initiation. This lack of significance persists at 2 months post-intervention initiation, 1 month after the intervention’s conclusion, and 2 months post-intervention. These findings suggest a limited impact of the intervention on the total PEDI score during various periods following its implementation, diverging from some previous studies that affirm the efficacy of the neurodevelopmental approach in enhancing occupational performance and addressing feeding and swallowing activities in children with CP [33, 34].
Effect of intervention on gross motor function measure (GMFM-88)
The results show that 1 month after the start of the intervention and by controlling the values before the intervention, there is no statistically significant difference between the intervention group and the control group in the GMFM-88 total score. Also, no statistically significant difference was found in 2 months after the start of the study, 1 month after the end of the intervention and 2 months after the end of the intervention.
Regarding the effect of intervention on gross motor function and functional mobility using GMFM-88, similar results have been obtained with PEDI. Here, too, there are differences between the present study and previous studies. It has been reported in some studies that the neurodevelopmental approach and its techniques can significantly improve gross motor function, walking and balance in children with CP [35-38].
However, the results of the present study show that the group training intervention of handling skills did not have a significant effect on the scores of GMFM-88 subscales.
These differences can originate from the difference in conducting the intervention, access to the required resources and equipment, or the special needs of the children under study. There is also a possibility that the interventions provided on the functional mobility and gross movements of children with CP need to be continued and repeated more by mothers at home in order to show their effect. However, it is worth considering the alignment of the results of the present study with the meta-analysis conducted by Velde et al. (2022) who investigated the effectiveness of the neurodevelopmental approach in children and infants with CP or at high risk of CP [37]. This meta-analysis included data analysis of 34 studies, including 1332 participants. The findings showed no significant difference in motor performance between the groups receiving neurodevelopmental therapy and the control group. In other words, the application of the neurodevelopmental approach did not show a significant effect on the improvement of motor performance compared to control interventions. It is worth noting that this study showed that activity-based approaches and interventions that target body function and structure were more effective than neurodevelopmental therapy. These alternative interventions yielded more positive results in terms of improved motor performance. Finally, this meta-analysis provided a strong recommendation against the use of neurodevelopmental therapy regardless of the dose or intensity of the intervention.
The results of the present study showed that group training of handling skills to mothers with children with CP had no significant effect on the functional mobility and gross motor performance of children, but as mentioned in the initial part of the discussion, we witnessed a significant improvement in the ability of the family. Since in the training that was given to the mothers of the intervention group, the handling skills during the execution of the child’s daily tasks and the methods of facilitating these tasks for the child were also presented, it can be concluded that despite the fact that during the study period, there was a significant effect on motor functions. The child has not been observed, but these teachings and their implementation in the home environment have helped to reduce the exhaustion and fatigue of the family in helping as a child’s caregiver and have enabled the family to solve problems related to children’s daily affairs in a more optimal way. Several studies have been conducted in the field of burden of caregivers or families with children with CP, which show that their caregivers face a lot of physical, mental, and financial exhaustion caused by caring for and helping children with CP in doing their daily tasks [39, 40]. The result of Colak and Kahriman study to measure burden and its related factors on 518 parents of disabled children is consistent with the result of a study conducted by Ozturk and Alemdar with the same aim on 280 mothers with disabled children [41, 42]. Both studies came to the conclusion that while there is attrition that affects caregivers of disabled children, this attrition increases fatigue and decreases the quality of life in caregivers. In continuation of these two studies, another study was conducted in 2024 by Garcia-Grau et al. with the goal of investigating the relationship between the burden of the families of disabled children, their quality of life and self-confidence among 58 families. The result of this study showed that by increasing the self-confidence of families, we can expect an increase in the quality of life and a decrease in their burnout. The family’s self-confidence is the family’s understanding of its potential abilities in solving problems and implementing its desired affairs; in a way that feels worthy and sufficient [43, 44]. Family self-confidence is the result of the support of health and treatment systems and specialists in this field [43] and this is exactly the same as the “service systems” subscale of the FES that was used to measure the output values of this study and the same As mentioned, the interventions presented in the present study led to improvement in the scores of mothers in the intervention group in this scale and all its subscales. Therefore, the teaching of handling skills to mothers with children with CP during the implementation of the present study did not have a significant effect on the functional mobility and gross motor performance of the children participating in the intervention group compared to the children in the control group, but the mothers who were in the intervention group Compared to the mothers of the control group, there was a significant growth in the ability, self-confidence and self-efficacy of the family, and their fatigue and burden decreased as caregivers of their children. It should also be mentioned that based on the hierarchy of inferences mentioned above, providing the mentioned interventions to the mothers of the intervention group led to an increase in their quality of life.
Comparative analysis and considerations
Observed discrepancies in the effectiveness of interventions for children with CP across different studies underscore the complexity of evaluation criteria, intervention types, and environmental conditions. The meta-analysis by Velde et al. (2022) further supports the notion that alternative interventions emphasizing body function and structure may yield more favorable outcomes than traditional neurodevelopmental therapy [37]. Future research in this field would benefit from symmetrical and controlled designs to enhance the accuracy and validity of results.
Conclusion
This study demonstrated that group training in handling skills significantly improved parental abilities of children with CP. The observed positive effects across various subscales emphasize the intervention’s effectiveness. Despite variations in study outcomes, factors such as intervention type, duration, and environmental conditions were found to influence results. Conducting future research with symmetrical and controlled designs is crucial for ensuring accuracy and reliability. Notably, the positive effects of the intervention persisted over an extended period following the intervention. This finding underscores the continued support for parents of children with CP. Further research is essential for refining interventions and promoting sustained well-being for both parents and children in this context.
Limitations of the research
Concluding the thesis discussion necessitates acknowledging and examining the limitations that surfaced during the study, which influence the interpretation and generalization of the results. Given the study’s nature and outcomes, these limitations play a crucial role in shaping interpretations and offering recommendations for future research and practical applications. One significant limitation pertains to the study’s sampling, as the samples were confined to specific populations under unique conditions. This constraint potentially restricts the applicability of the findings to the broader spectrum of children with spastic CP. Therefore, generalizing these results to other populations must involve careful consideration of this limitation. Furthermore, the study’s reliance on standard measurement tools for motor performance and functional mobility, without incorporating a wider variety of tools, raises concerns regarding the accuracy and comprehensiveness of the results. The absence of diverse assessment instruments may inadvertently introduce bias or overlook certain aspects of the intervention’s impact. The failure to control environmental variables, such as the home environment and family support during interventions, adds a layer of complexity to result interpretation. These uncontrolled factors may introduce confounding variables affecting the study outcomes. Consequently, considering these limitations is paramount for the accurate interpretation of the study’s results. To address these limitations, future studies are encouraged to involve larger and more diverse cohorts of children with spastic CP, fostering collaboration among various medical and research centers. This approach would deepen the understanding of intervention impacts on this specific group. Moreover, employing extended and longitudinal study designs can facilitate continuous follow-up on interventions, shedding light on their sustained long-term outcomes. In addition, future studies should focus on designing and evaluating interventions tailored to the specific needs and priorities of parents and families of children with spastic CP. By adhering to these recommendations, future research endeavors can take progressive steps in refining interventions for this population, ultimately enhancing their performance and overall quality of life.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.REC.1401.246). This study was registered by the Iranian Registry of Clinical Trials (IRCT) (Code: RCT20220630055330N1). Informed consent was obtained from all parents or caregivers after receiving detailed project explanations.
Funding
This paper was extracted from the master's thesis of Pooya Reaei, approved by the Department of Occupational Therapy, school of School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their sincere appreciation to the study participants and their families for their invaluable involvement in this research. Gratitude is expressed to the Tavanyab Charity Center in Tehran for their collaborative efforts and unwavering support throughout the study’s duration. Special recognition is given to the research assistant of the Faculty of Rehabilitation Sciences at Iran University of Medical Sciences for their instrumental role in facilitating the necessary arrangements. The authors also acknowledge the ethical clearance granted by the graduate education unit of the Faculty of Rehabilitation Sciences, which significantly contributed to the realization of this study.
Table 1 presents the individual and clinical characteristics of the children and their parents involved in the study.
The average age of the studied children was 7.02±2.27 years, with a gender distribution of 50.0% boys. Fathers had an average age of 40.40±7.50 years, mothers had an average age of 35.54±7.75 years, and both parents had an average education level of 8.84±4.76 and 8.8±4.89 years, respectively.
Among the 50 children studied, distributions were observed in terms of GMFCS levels. For instance, 24% of children exhibited GMFCS level 5. Table 1 demonstrates the homogeneity between the control and intervention groups across all individual and clinical variables, ensuring comparable participant characteristics in both groups. Data for 5 measurement occasions are presented in Table 2 for all outcome measures.
Family empowerment (FES) total score and subscale scores)
FES total score: The intervention group exhibited significantly higher FES total scores 1month post-intervention (η2p=0.082, P=0.047), persisting at 2 months (η2p=0.116, P=0.017), 1-month post-intervention conclusion (η2p=0.160, P=0.004), and 2 months post-intervention conclusion (η2p=0.284, P<0.001). These findings underscore the sustained positive influence of the intervention on the FES total score.
Family subscale scores: Covariance analysis, adjusting for pre-intervention values, revealed no statistically significant differences in family subscale scores one month (η2p=0.062, P=0.086) and two months (η2p=0.070, P=0.066) after initiation. However, post-intervention saw a notable increase in the intervention group’s family subscale scores. One-month post-intervention witnessed a substantial 4.72-unit rise (η2p=0.214, P<0.001), persisting at two months with a 5.89-unit increase (η2p=0.288, P=0.001), emphasizing the intervention’s positive impact on family-related outcomes.
Service systems subscale scores: While one-month post-intervention showed no significant difference (η2p=0.066, P=0.075), the intervention group demonstrated a marked increase in service systems subscale scores compared to the control group (η2p=0.178; P=0.002; 95% CI, 1.76%). This superiority persisted at 1 month (η2p=0.103, P=0.024) and two months (η2p=0.262, P<0.001), highlighting the positive influence of the intervention on service systems-related outcomes.
Community/political subscale score: Covariance analysis, adjusting for pre-intervention values, revealed a significant increase in the intervention group’s community/political subscale scores 1-month post-intervention (η2p=0.104, P=0.024), persisting at 1 month (η2p=0.123, P=0.014) and 2 months (η2p=0.215, P<0.001) after intervention conclusion. The intervention consistently led to significantly higher scores compared to the control group, indicating positive influence.
Mobility function (PEDI) total score
PEDI total score: Covariance analysis showed no significant differences in total PEDI scores between control and intervention groups one month (η2p=0.045, P=0.142) and 2 months (η2p=0.019, P=0.350) post-intervention. Comparable impact was observed, indicating no statistically significant differences in this outcome measure.
Gross motor function (GMFM-88) total score and subscale scores)
GMFM-88 total score: No statistically significant impact on GMFM-88 total scores was identified between control and intervention groups 1 month (η2p=0.009, P=0.506) and two months (η2p=0.010, P=0.487) post-intervention. Consistency in outcomes was observed across the study duration.
Lying and rolling score: No significant differences in lying and rolling scores were observed between groups 1 month (η2p=0.014, P=0.419) and 2 months (η2p=0.013, P=0.439) post-intervention. Outcomes remained comparable, suggesting the intervention did not yield significant differences in this aspect.
Sitting score: No significant differences in sitting scores were noted between groups one month (η2p<0.001, P=0.904) and two months (η2p<0.001, P=0.977) post-intervention. Consistent outcomes were maintained, indicating no significant impact on sitting scores.
Crawling and kneeling scores: No significant differences in crawling and kneeling scores were identified between groups 1 month (η2p=0.006, P=0.604) and 2 months (η2p=0.014, P=0.411) post-intervention. Similar outcomes were sustained, suggesting no significant impact on crawling and kneeling scores.
Standing scores: No significant variations in standing scores were found between groups one month (η2p=0.007, P=0.562) and 2 months (η2p=0.014, P=0.418) post-intervention. Consistency in outcomes indicated no significant impact on standing scores.
Walking, running, and jumping scores: No significant variations in walking, running, and jumping scores were observed between groups one month (η2p=0.005, P=0.624) and two months (η2p<0.001, P=0.914) post-intervention. Consistent outcomes suggested no significant impact on these scores.
Discussion
This systematic study sought to explore the consequences of group training in handling skills on multiple aspects related to children diagnosed with CP. By examining the domains of gross motor function, functional mobility, and parental capabilities, this investigation contributes to the existing body of literature on interventions for CP.
Effect of intervention on parental ability
An examination of parental ability reveals nuanced results. Covariance analysis conducted within the first month of intervention initiation indicates no significant differences in the family subscale score between the intervention and control groups. This initial observation suggests limited short-term intervention effects on family subscale scores. However, a noteworthy shift is discernible 1-month post-intervention cessation, with the intervention group displaying significantly higher average family subscale scores compared to the control group. This improvement persists two months post-intervention conclusion, substantiating a sustained positive impact on family subscale scores.
As it was said in the explanation of the concept of the family subscale in the assessment tools section, this subscale deals with the parents’ understanding of the child’s conditions, the ability of the parents to acquire the necessary knowledge and skills and use them to solve the child’s potential problems in the implementation of daily activities and, according to the topic of each of the group training sessions of the present study, in which the participating mothers were taught information about the general conditions of CP, accompanying disorders, how to handle children in each of the frequently used situations of life, it can be seen that after one month of the beginning of the trainings No significant difference was observed in the family subscale between the intervention and control groups, but with the passage of another month after the intervention and the completion of the aforementioned handling training to the mothers of the intervention group, the difference in the family subscale gradually became noticeable and significant. We witnessed a significant improvement in the decision-making ability and effective action of the parents of the intervention group in facing their children’s daily situations and problems.
Similar to the family subscale scores, the service systems subscale exhibits no significant differences within the first month of intervention. However, a contrasting picture emerges post-intervention, with the intervention group exhibiting a remarkable increase in scores. This figure exceeds the control group’s average scores by 5.7 and 4.1 points, 1 and 2 months post-intervention, respectively, corroborating the positive influence and improvement of service systems subscale scores over time. The community/political subscale demonstrates a similar trend, with significant score increases observed one month post-intervention, persisting over the long term.
The total FES score manifests a considerable increase within one month of intervention initiation in the intervention group, contrasting with the control group. This positive influence persists post-intervention, maintaining statistically higher scores in the intervention group one and two months thereafter.
Overall impact and long-term efficacy
Totally, the results of this research demonstrate that within one month after the start of the intervention, the average total FES score in the intervention group was significantly higher than in the control group. These findings confirm the positive effect and improvement of the FES total score due to the effectiveness of the intervention. Moreover, the positive impact of the intervention on the total FES score was maintained in the intervention group after the end of the intervention and one and two months thereafter, with the average score remaining significantly higher than the control group.
Overall, the results of this study indicate that the group training intervention of handling skills positively affects parental ability. The effectiveness of this intervention across various FES subscales, including family, service, and social/political systems, suggests that the intervention successfully enhances multiple aspects of family and social life. Additionally, the long-term effectiveness of the intervention has been observed, highlighting the stability of these effects over time.
These findings align with previous research in the field. Lorentzen et al. (2015) demonstrated that interactive educational programs at home can improve parental ability and involvement in the treatment of children with CP [27]. Similarly, Chiu et al. (2014) reached a comparable conclusion [28]. In general, the results of this study, corroborating previous studies, confirm the enhancement of parental ability in children with CP [29-31]. These findings address the need for evaluating the effectiveness of home-based programs, as emphasized by Beckers et al. (2020), who highlighted a strong recommendation for implementing such programs despite the lack of sufficient research [32].
A notable difference between the current study and previous research is the measurement of the long-term effects of training provided to mothers, extending up to two months after the conclusion of interventions. This unique aspect of the study reveals the stability of the training’s impact on family empowerment over an extended period, which had not been previously examined. Earlier studies focused on evaluations conducted at the completion of interventions, lacking a long-term follow-up assessment.
Effect of intervention on PEDI total score
In assessing the impact of the intervention on the PEDI total score, the study reveals an absence of statistically significant differences between the intervention and control groups within the first month of intervention initiation. This lack of significance persists at 2 months post-intervention initiation, 1 month after the intervention’s conclusion, and 2 months post-intervention. These findings suggest a limited impact of the intervention on the total PEDI score during various periods following its implementation, diverging from some previous studies that affirm the efficacy of the neurodevelopmental approach in enhancing occupational performance and addressing feeding and swallowing activities in children with CP [33, 34].
Effect of intervention on gross motor function measure (GMFM-88)
The results show that 1 month after the start of the intervention and by controlling the values before the intervention, there is no statistically significant difference between the intervention group and the control group in the GMFM-88 total score. Also, no statistically significant difference was found in 2 months after the start of the study, 1 month after the end of the intervention and 2 months after the end of the intervention.
Regarding the effect of intervention on gross motor function and functional mobility using GMFM-88, similar results have been obtained with PEDI. Here, too, there are differences between the present study and previous studies. It has been reported in some studies that the neurodevelopmental approach and its techniques can significantly improve gross motor function, walking and balance in children with CP [35-38].
However, the results of the present study show that the group training intervention of handling skills did not have a significant effect on the scores of GMFM-88 subscales.
These differences can originate from the difference in conducting the intervention, access to the required resources and equipment, or the special needs of the children under study. There is also a possibility that the interventions provided on the functional mobility and gross movements of children with CP need to be continued and repeated more by mothers at home in order to show their effect. However, it is worth considering the alignment of the results of the present study with the meta-analysis conducted by Velde et al. (2022) who investigated the effectiveness of the neurodevelopmental approach in children and infants with CP or at high risk of CP [37]. This meta-analysis included data analysis of 34 studies, including 1332 participants. The findings showed no significant difference in motor performance between the groups receiving neurodevelopmental therapy and the control group. In other words, the application of the neurodevelopmental approach did not show a significant effect on the improvement of motor performance compared to control interventions. It is worth noting that this study showed that activity-based approaches and interventions that target body function and structure were more effective than neurodevelopmental therapy. These alternative interventions yielded more positive results in terms of improved motor performance. Finally, this meta-analysis provided a strong recommendation against the use of neurodevelopmental therapy regardless of the dose or intensity of the intervention.
The results of the present study showed that group training of handling skills to mothers with children with CP had no significant effect on the functional mobility and gross motor performance of children, but as mentioned in the initial part of the discussion, we witnessed a significant improvement in the ability of the family. Since in the training that was given to the mothers of the intervention group, the handling skills during the execution of the child’s daily tasks and the methods of facilitating these tasks for the child were also presented, it can be concluded that despite the fact that during the study period, there was a significant effect on motor functions. The child has not been observed, but these teachings and their implementation in the home environment have helped to reduce the exhaustion and fatigue of the family in helping as a child’s caregiver and have enabled the family to solve problems related to children’s daily affairs in a more optimal way. Several studies have been conducted in the field of burden of caregivers or families with children with CP, which show that their caregivers face a lot of physical, mental, and financial exhaustion caused by caring for and helping children with CP in doing their daily tasks [39, 40]. The result of Colak and Kahriman study to measure burden and its related factors on 518 parents of disabled children is consistent with the result of a study conducted by Ozturk and Alemdar with the same aim on 280 mothers with disabled children [41, 42]. Both studies came to the conclusion that while there is attrition that affects caregivers of disabled children, this attrition increases fatigue and decreases the quality of life in caregivers. In continuation of these two studies, another study was conducted in 2024 by Garcia-Grau et al. with the goal of investigating the relationship between the burden of the families of disabled children, their quality of life and self-confidence among 58 families. The result of this study showed that by increasing the self-confidence of families, we can expect an increase in the quality of life and a decrease in their burnout. The family’s self-confidence is the family’s understanding of its potential abilities in solving problems and implementing its desired affairs; in a way that feels worthy and sufficient [43, 44]. Family self-confidence is the result of the support of health and treatment systems and specialists in this field [43] and this is exactly the same as the “service systems” subscale of the FES that was used to measure the output values of this study and the same As mentioned, the interventions presented in the present study led to improvement in the scores of mothers in the intervention group in this scale and all its subscales. Therefore, the teaching of handling skills to mothers with children with CP during the implementation of the present study did not have a significant effect on the functional mobility and gross motor performance of the children participating in the intervention group compared to the children in the control group, but the mothers who were in the intervention group Compared to the mothers of the control group, there was a significant growth in the ability, self-confidence and self-efficacy of the family, and their fatigue and burden decreased as caregivers of their children. It should also be mentioned that based on the hierarchy of inferences mentioned above, providing the mentioned interventions to the mothers of the intervention group led to an increase in their quality of life.
Comparative analysis and considerations
Observed discrepancies in the effectiveness of interventions for children with CP across different studies underscore the complexity of evaluation criteria, intervention types, and environmental conditions. The meta-analysis by Velde et al. (2022) further supports the notion that alternative interventions emphasizing body function and structure may yield more favorable outcomes than traditional neurodevelopmental therapy [37]. Future research in this field would benefit from symmetrical and controlled designs to enhance the accuracy and validity of results.
Conclusion
This study demonstrated that group training in handling skills significantly improved parental abilities of children with CP. The observed positive effects across various subscales emphasize the intervention’s effectiveness. Despite variations in study outcomes, factors such as intervention type, duration, and environmental conditions were found to influence results. Conducting future research with symmetrical and controlled designs is crucial for ensuring accuracy and reliability. Notably, the positive effects of the intervention persisted over an extended period following the intervention. This finding underscores the continued support for parents of children with CP. Further research is essential for refining interventions and promoting sustained well-being for both parents and children in this context.
Limitations of the research
Concluding the thesis discussion necessitates acknowledging and examining the limitations that surfaced during the study, which influence the interpretation and generalization of the results. Given the study’s nature and outcomes, these limitations play a crucial role in shaping interpretations and offering recommendations for future research and practical applications. One significant limitation pertains to the study’s sampling, as the samples were confined to specific populations under unique conditions. This constraint potentially restricts the applicability of the findings to the broader spectrum of children with spastic CP. Therefore, generalizing these results to other populations must involve careful consideration of this limitation. Furthermore, the study’s reliance on standard measurement tools for motor performance and functional mobility, without incorporating a wider variety of tools, raises concerns regarding the accuracy and comprehensiveness of the results. The absence of diverse assessment instruments may inadvertently introduce bias or overlook certain aspects of the intervention’s impact. The failure to control environmental variables, such as the home environment and family support during interventions, adds a layer of complexity to result interpretation. These uncontrolled factors may introduce confounding variables affecting the study outcomes. Consequently, considering these limitations is paramount for the accurate interpretation of the study’s results. To address these limitations, future studies are encouraged to involve larger and more diverse cohorts of children with spastic CP, fostering collaboration among various medical and research centers. This approach would deepen the understanding of intervention impacts on this specific group. Moreover, employing extended and longitudinal study designs can facilitate continuous follow-up on interventions, shedding light on their sustained long-term outcomes. In addition, future studies should focus on designing and evaluating interventions tailored to the specific needs and priorities of parents and families of children with spastic CP. By adhering to these recommendations, future research endeavors can take progressive steps in refining interventions for this population, ultimately enhancing their performance and overall quality of life.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.REC.1401.246). This study was registered by the Iranian Registry of Clinical Trials (IRCT) (Code: RCT20220630055330N1). Informed consent was obtained from all parents or caregivers after receiving detailed project explanations.
Funding
This paper was extracted from the master's thesis of Pooya Reaei, approved by the Department of Occupational Therapy, school of School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their sincere appreciation to the study participants and their families for their invaluable involvement in this research. Gratitude is expressed to the Tavanyab Charity Center in Tehran for their collaborative efforts and unwavering support throughout the study’s duration. Special recognition is given to the research assistant of the Faculty of Rehabilitation Sciences at Iran University of Medical Sciences for their instrumental role in facilitating the necessary arrangements. The authors also acknowledge the ethical clearance granted by the graduate education unit of the Faculty of Rehabilitation Sciences, which significantly contributed to the realization of this study.
References
- Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, Damiano D, et al. A report: The definition and classification of cerebral palsy April 2006. Developmental Medicine and Child Neurology. 2007; 109:8-14. [PMID]
- Kramer P. Frames of reference for pediatric occupational therapy. Waltham:Wolters Kluwer Health; 2018. [Link]
- Solomon JW, Jane Clifford O. Pediatric skills for occupational therapy assistants. Maryland: Mosby eBooks; 2015. [Link]
- Shamsoddini, A.Comparison between the effect of neurodevelopmental treatment and sensory integration therapy on gross motor function in children with cerebral palsy. Iranian Journal of Child Neurology. 2010; 4(1):31-8. [Link]
- Anderson J, Auster-Liebhaber J. Developmental therapy in the neonatal intensive care unit. Physical & Occupational Therapy in Pediatrics. 1984; 4(1):89-106. [DOI:10.1080/j006v04n01_09]
- Paludo T, Zardo F, de Mattos BTP, Frata B, Ling CC, de Castro Barroso G, et al. Measuring muscle activation using electromyography during neurodevelopmental treatment in individuals with severe cerebral palsy. Journal of Back and Musculoskeletal Rehabilitation. 2023; 36(3):691-700. [DOI:10.3233/bmr-220113] [PMID]
- Dalvand H, Hosseini SA, Rassafiani M, Samadi SA, Khankeh HR, Kelly G. Co-occupations: The caregiving challenges of mothers of children with cerebral palsy. British Journal of Occupational Therapy. 2015; 78(7):450-9. [DOI:10.1177/0308022614562793]
- Sharif Azar E, Ravanbakhsh M, Torabipour A, Amiri E, Haghighyzade MH. Home-based versus center-based care in children with cerebral palsy: A cost-effectiveness analysis. Journal of Medicine and Life. 2015; 8(Spec Iss 4):245-51. [PMID]
- Dalvand H, Dehghan L, Rassafiani M, Hosseini SA. Exploring the process of mothering co-occupations in caring of children with cerebral palsy at home. Directory of Open Access Journals. 2018; 6(2):7129-40. [DOI:10.22038/ijp.2017.23911.2020]
- Dehghan L, Dalvandi A, Rassafiani M, Hosseini SA, Dalvand H, Baptiste S. Social participation experiences of mothers of children with cerebral palsy in an Iranian context. Australian Occupational Therapy Journal. 2015; 62(6):410-9. [DOI:10.1111/1440-1630.12215] [PMID]
- Johari S, Rassafiani M, Fatorehchy S, Dalvand H. Reviewing the determinant factors of parental satisfaction in occupational therapy home programs. Middle Eastern Journal of Disability Studies. 2013; 3(1):52-61. [Link]
- Rassafiani M, Kahjoogh MA, Hosseini A, Sahaf R. Time use in mothers of children with cerebral palsy: A comparison study. Hong Kong Journal of Occupational Therapy. 2012; 22(2):70-4. [DOI:10.1016/j.hkjot.2012.11.001]
- Werbrouck A, Swinnen E, Kerckhofs E, Buyl R, Beckwée D, De Wit L. How to empower patients? A systematic review and meta-analysis. Translational Behavioral Medicine. 2018; 8(5):660-74. [DOI:10.1093/tbm/iby064] [PMID]
- Kahjoogh MA, Rassafiani M, Tahmasebi A, Kahjoogh HA, Sahaf R. The relationship between gross motor function ability and time use in mothers of children with cerebral palsy. British Journal of Occupational Therapy. 2016; 79(3):172-7. [DOI:10.1177/0308022615616974]
- Ghashghaee M, Mohammadi F, Rassafiani M, Hosseini S, Sahaf R. Clarifying facilitator factors of parental adherence to a home-based educational special caring program for children with cerebral palsy: A content analysis of parent's educational experiences. Journal of Research in Rehabilitation Sciences. 2014; 10(1):158-70. [DOI:10.22122/jrrs.v10i1.1037]
- Kahjoogh MA, Kessler D, Hosseini SA, Rassafiani M, Akbarfahimi N, Khankeh HR, et al. Randomized controlled trial of occupational performance coaching for mothers of children with cerebral palsy. British Journal of Occupational Therapy. 2018; 82(4):213-19. [DOI:10.1177/0308022618799944]
- Eo YS. [Effects of an empowerment program on the burden of mothers having a child with cerebral palsy (Korean)]. Taehan Kanho Hakhoe Chi. 2005; 35(1):154-64. [DOI:10.4040/jkan.2005.35.1.154] [PMID]
- Russell DJ, Rosenbaum PL, Cadman DT, Gowland C, Hardy S, Jarvis S. The gross motor function measure: A means to evaluate the effects of physical therapy. Developmental Medicine and Child Neurology. 1989; 31(3):341-52. [DOI:10.1111/j.1469-8749.1989.tb04003.x] [PMID]
- Salehi R, Keshavarz A, Negahban H, Saeedi A, Shiravi A, Ghorbani, S, et al. Development of the Persian version of gross motor function measure-88 (GMFM-88): A study of reliability. Trends in Medical Research. 2015; 10(3):69-74. [DOI:10.3923/tmr.2015.69.74]
- Haley SM, Coster WJ, Ludlow LH, Haltiwanger JT, Andrellos PJ. Pediatric evaluation of disability inventory (PEDI). Physical and Occupational Therapy in Pediatrics. 1992; 12(2):1-29.
- Berg M, Jahnsen R, Frøslie KF, Hussain A. Reliability of the pediatric evaluation of disability inventory (PEDI). Physical & Occupational Therapy in Pediatrics. 2004; 24(3):61-77. [DOI:10.1300/j006v24n03_05] [PMID]
- Abbasabadi, MM, Fahimi NA, Hosseini SA, Rezasoltani P. Reliability of the Persian version of the pediatric evaluation of disability inventory in 3 to 9 year old children with cerebral palsy. Journal of Mazandaran University of Medical Sciences. 215; 25(130):129-37. [Link]
- Koren PE, DeChillo N, & Friesen BJ. Measuring empowerment in families whose children have emotional disabilities: A brief questionnaire. Rehabilitation Psychology. 1992; 37(4):305-21. [DOI:10.1037/h0079106]
- Rajabi G, Zolmajd Z. Psychometric properties of the Persian version of the family empowerment scale. Iranian Journal of Psychiatry and Clinical Psychology. 2018; 24(2):216-29. [DOI:10.32598/ijpcp.24.2.216]
- Riahi A, Rassafiani M, Binesh M. The cross-cultural validation and test-retest and inter-rater reliability of the Persian translation of parent version of the gross motor function classification system for children with cerebral palsy. Archives of Rehabilitation. 2013; 13:25-30. [Link]
- Dehghan L, Abdolvahab M, Bagheri H, Dalvand H. Inter rater reliability of Persian version of gross motor function classification system expanded and revised in patients with cerebral palsy. Daneshvar Medicine. 2011; 18(6):37-44. [Link]
- Lorentzen J, Greve LZ, Kliim-Due M, Rasmussen B, Bilde PE, Nielsen JB. Twenty weeks of home-based interactive training of children with cerebral palsy improves functional abilities. BMC Neurology. 2015; 15:75. [DOI:10.1186/s12883-015-0334-0] [PMID]
- Chiu HC, Ada L, Lee HM. Upper limb training using Wii Sports Resort for children with hemiplegic cerebral palsy: A randomized, single-blind trial. Clinical Rehabilitation. 2014; 28(10):1015-24. [DOI:10.1177/0269215514533709] [PMID]
- Deyhoul N, Vasli P, Rohani C, Shakeri N, Hosseini M. The effect of family-centered empowerment program on the family caregiver burden and the activities of daily living of Iranian patients with stroke: A randomized controlled trial study. Aging Clinical and Experimental Research. 2020; 32(7):1343-52. [DOI:10.1007/s40520-019-01321-4] [PMID]
- Habib-Hasan Z, Sheikh MS, Hoodbhoy Z, Azam I, O'Neil M. Early intervention physical therapy using "parent empowerment program" for children with Down syndrome in Pakistan: A feasibility study. Journal of Pediatric Rehabilitation Medicine. 2020; 13(3):233-40. [DOI:10.3233/prm-190605] [PMID]
- Sayed MA, Abdelmonem HH, Ahmed FA. Effect of empowerment program for caregivers on quality life of children with cerebral palsy. Egyptian Journal of Health Care. 2021; 12(1):140-55. [DOI:10.21608/ejhc.2021.138611]
- Beckers LWME, Geijen MME, Kleijnen J, A A Rameckers E, L A P Schnackers M, J E M Smeets R, Janssen-Potten YJM. Feasibility and effectiveness of home-based therapy programmes for children with cerebral palsy: A systematic review. BMJ Open. 2020; 10(10):e035454. [DOI:10.1136/bmjopen-2019-035454] [PMID]
- Acar G, Ejraei N, Turkdoğan D, Enver N, Öztürk G, Aktaş G. The effects of neurodevelopmental therapy on feeding and swallowing activities in children with cerebral palsy. Dysphagia. 2022; 37(4):800-811. [DOI:10.1007/s00455-021-10329-w] [PMID]
- Kolit Z, Ekici G. Effect of the cognitive orientation to daily occupational performance (CO-OP) approach for children with cerebral palsy: A randomized controlled trial. Journal of Pediatric Rehabilitation Medicine. 2023; 16(1):59-70. [DOI:10.3233/prm-210085] [PMID]
- Franki I, Desloovere K, De Cat J, Feys H, Molenaers G, Calders P, et al. The evidence-base for conceptual approaches and additional therapies targeting lower limb function in children with cerebral palsy: A systematic review using the ICF as a framework. Journal of Rehabilitation Medicine. 2012; 44(5):396-405. [DOI:10.2340/16501977-0984] [PMID]
- Kalaichadran K, Swarnakumari P. Neuro developmental treatment (NDT) for cerebral palsy: A clinical study. International Journal of Innovative Science and Research Technology. 2019; 4(5):33-4. [Link]
- Te Velde A, Morgan C, Finch-Edmondson M, McNamara L, McNamara M, Paton MCB, et al. Neurodevelopmental therapy for cerebral palsy: A meta-analysis. Pediatrics. 2022; 149(6):e2021055061. [DOI:10.1542/peds.2021-055061] [PMID]
- Warutkar VB, Krishna Kovela R. Review of sensory integration therapy for children with cerebral palsy. Cureus. 2022; 14(10):e30714. [DOI:10.7759/cureus.30714] [PMID]
- Lowes L, Clark TS, Noritz G. Factors associated with caregiver experience in families with a child with cerebral palsy. Journal of Pediatric Rehabilitation Medicine. 2016; 9(1):65-72. [DOI:10.3233/prm-160362] [PMID]
- Majnemer A, Shevell M, Law M, Poulin C, Rosenbaum P. Indicators of distress in families of children with cerebral palsy. Disability and Rehabilitation. 2012; 34(14):1202-7. [DOI:10.3109/09638288.2011.638035] [PMID]
- Çolak, B, Kahriman İ. Evaluation of family burden and quality of life of parents with children with disability. American Journal of Family Therapy. 2021; 51(2):113-33. [DOI:10.1080/01926187.2021.1941421]
- Öztürk M, Küçük Alemdar D. The care burden of mothers of children with disability: Association between family quality of life and fatigue. Journal of Pediatric Nursing. 2023; 73:e418-25. [DOI:10.1016/j.pedn.2023.10.010] [PMID]
- García-Grau P, Martínez-Rico G, González-García RJ, Escorcia-Mora CT, Cañadas-Pérez M. Caregiver burden and family quality of life in early intervention: The role of mothers and family confidence. European Journal of Investigation in Health, Psychology and Education. 2024; 14(5):1325-37. [DOI:10.3390/ejihpe14050087] [PMID]
- Swanson J, Raab M, Dunst, CJ. Strengthening family capacity to provide young children everyday natural learning opportunities. Journal of Early Childhood Research. 2011; 9(1):66-80. [DOI:10.1177/1476718x10368588]
Article type: Original Research Articles |
Subject:
Occupational therapy
Received: 2024/12/22 | Accepted: 2025/12/6 | Published: 2026/03/1
Received: 2024/12/22 | Accepted: 2025/12/6 | Published: 2026/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
