
988368
Sat, Jun 20, 2026

Volume 24, Issue 1 (March 2026)
Iranian Rehabilitation Journal 2026, 24(1): 65-78 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Poursaeid Z, Mohsenpour M, Ghasisin L. Iranian Speech Therapists’ Experiences of Barriers and Facilitators to Aphasia Therapy: A Qualitative Study. Iranian Rehabilitation Journal 2026; 24 (1) :65-78
URL: http://irj.uswr.ac.ir/article-1-2517-en.html
URL: http://irj.uswr.ac.ir/article-1-2517-en.html



1- Student Research Committee, School of Rehabilitation, Isfahan University of Medical Sciences, Isfahan, Iran.
2- Nursing and Midwifery Care Research Centre, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Speech Therapy, Musculoskeletal Research Center, School of Rehabilitation, Isfahan University of Medical Sciences, Isfahan, Iran.
2- Nursing and Midwifery Care Research Centre, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Speech Therapy, Musculoskeletal Research Center, School of Rehabilitation, Isfahan University of Medical Sciences, Isfahan, Iran.
Full-Text [PDF 593 kb]
(116 Downloads)
| Abstract (HTML) (1174 Views)
Full-Text: (15 Views)
Introduction
Brain strokes are the third leading cause of death, the second leading cause of dementia, as well as the primary cause of adult disability in Western countries [1]. In Iran, it ranked as the second leading cause of death in 2016 [2]. Stroke survivors frequently face various complications [3], with aphasia being a common manifestation that can appear within hours of the event [1]. Aphasia is an acquired language disorder that impacts all aspects of language functioning, including comprehension, expression, reading, and writing [4]. While stroke is the most prevalent cause, other neurological impairments can also result in aphasia [4]. Due to its significant effects on communication, aphasia is regarded as a major communication disability that influences daily activities, social participation, and social roles of people with aphasia (PWA) [5, 6]. The negative ramifications of aphasia often endure for a lifetime [7] and also significantly affect families, who may come across physical, emotional, and financial challenges [8-11].
As there are limited medical treatments available to mitigate the effects of aphasia, rehabilitation serves as the cornerstone of recovery for PWA [12]. Evidence supports the effectiveness of rehabilitation [11], particularly when initiated early in the recovery process [12]. Most treatments for PWA are provided through clinical sessions by qualified speech therapists to address communication problems [11, 13].
As the population ages and more individuals survive strokes [13], the prevalence of chronic disabilities, such as aphasia is projected to increase, highlighting the necessity for evidence-based care [14]. However, research reveals a notable disconnection between recommended practices and the actual delivery of services [15]. For instance, in Australia, 75% of PWA who were eligible for speech therapy did not receive any treatment during their hospitalization [16]. Furthermore, even when speech therapy is available, its frequency and intensity often fall short of the recommended guidelines [13]. Additionally, although PWA can benefit from being involved in the goal-setting process [17], they are rarely included in this stage [18]. Speech therapists have identified several barriers to delivering high-quality services, including insufficient training and a lack of confidence among professionals [19-21], as well as constraints, such as limited time and resources, a focus on dysphagia, and brief hospital stays [13]. Conversely, certain factors can facilitate the provision of effective treatment. These factors include the application of the International Classification of Functioning, Disability and Health (ICF) framework [22], availability of insurance coverage [13], and the satisfaction of PWA with their speech therapist [23].
Emerging evidence has begun to explore the barriers and facilitators associated with providing rehabilitation to PWA [15]. However, the factors influencing treatment vary significantly from country to country [19].
In Iran, there is currently no comprehensive data concerning the status, barriers, or facilitators of speech therapy for PWA. It appears that we are still far from delivering the evidence-based treatments necessary to enhance the communicative abilities of those affected [13]. Since its introduction in 1974, speech therapy education has expanded, now offered at the bachelor of science (BS), master of science (MSc), and doctor of philosophy (PhD) levels. Speech therapists are employed in hospitals and rehabilitation centers nationwide [24].
Local studies indicate that the incidence of stroke is higher and occurs at a younger age compared to Western countries [20]. Demographic forecasts suggest that by 2031, 25–30% of Iran’s population will be aged 50 or older [25]. Since most strokes occur in individuals aged 65 and above [3, 26], the burden of stroke and aphasia is expected to increase significantly in Iran. The ICF framework offers a comprehensive model for understanding the functional impact of aphasia [6, 22, 23]. However, despite its importance, knowledge regarding how rehabilitation services in Iran cater to the needs of PWA remains limited. This research aims to investigate the barriers and facilitators within this context.
To enhance services for individuals with disabilities in the community, it is essential to evaluate the current state of these services [27]. Gaining this insight enables us to assess whether care for PWA is being delivered optimally, which has significant implications for practice planning and future research [20, 22]. Therefore, this study aimed to explore the barriers and facilitators of speech therapy for aphasia as perceived by Iranian speech therapists.
Materials and Methods
This study aimed to explore the barriers and facilitators impacting the provision of speech therapy services from the perspective of speech therapists. A qualitative approach was adopted, utilizing content analysis, which is particularly effective when existing theory or literature on a phenomenon is limited. In this method, the researcher immerses themselves in the data to gain fresh insights into the phenomenon under investigation, with findings directly drawn from the data [28, 29]. The rationale for selecting this method was to achieve an in-depth understanding of the participants’ lived experiences with speech therapy services for aphasia. Data were gathered through semi-structured individual interviews with open-ended questions. Interviews are a standard method of data collection in qualitative research, and the use of open-ended questions allows interviewees to respond in their own words, enabling them to share their feelings, thoughts, and experiences without restraint [30, 31]. Interviews can vary along a continuum from unstructured to structured formats [30]. In semi-structured interviews, a set of prepared questions is utilized, although the order of these questions may be adjusted based on the flow of conversation and the responses of interviewees [31].
Study participants
In qualitative research, sampling continues until data saturation is achieved. Data saturation refers to the point at which information becomes repetitive and no new insights are gathered [30]. In the current study, data saturation was reached after 20 interviews, as the analysis of the final interviews revealed no additional information compared to earlier ones. To ensure this, we continuously compared new data with existing categories and confirmed that subsequent interviews yielded only repetitive information.
Twenty speech therapists participated in the study, all of whom had experience providing treatment to PWA in Iran. Table 1 lists the characteristics of speech therapists.
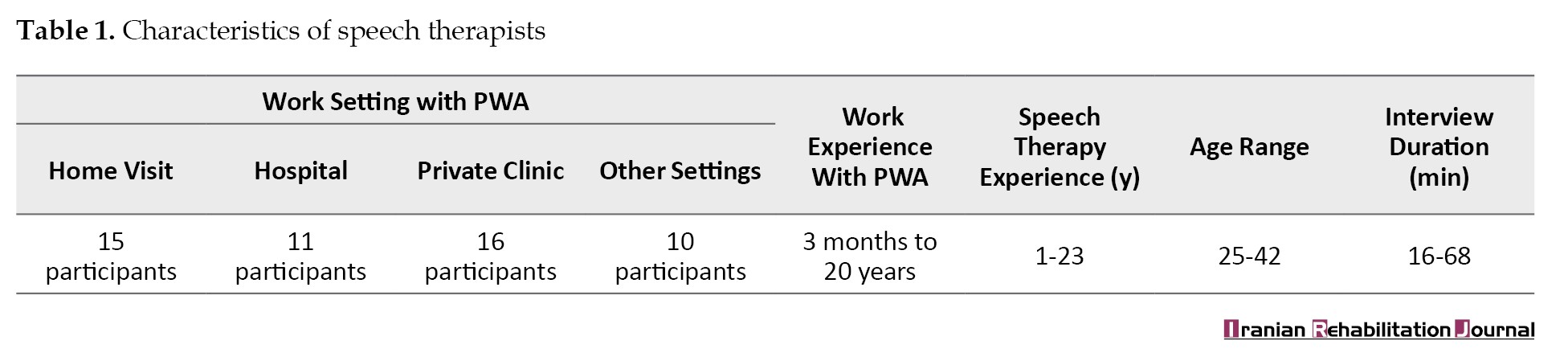
Of the participants, 13 were females and 7 were males. Fifteen had experience in home visits, 11 in hospitals, 16 in private clinics, and 10 in other settings, such as university-affiliated and public clinics. All participants worked in urban areas. Their working experience with PWA ranged from a minimum of 3 months to a maximum of 20 years, with an average experience of 14 years. In qualitative research, the goal is to identify cases that are rich in information—ones that can provide insights into the phenomenon being studied [32]. The purposive sampling method is the most effective approach for gaining new insights into the subject or achieving a deep understanding of a complex experience or event [33]. Therefore, in this study, the purposive sampling method was employed to select participants based on their experience providing speech therapy services for PWA.
The inclusion criteria required participants to sign the informed consent form, possess at least a bachelor’s degree in speech therapy, and have experience working with at least one individual with aphasia. All participants verified the accuracy of their interview transcripts; consequently, no interviews were excluded from the study.
Sampling
The interviews were conducted online, with each participant participating in a single session that included multiple interactions. Initially, the research team posted an announcement on virtual networks associated with speech therapy, outlining the procedure and inviting eligible speech therapists to express their interest via phone. Before the interviews, the team reached out to each participant by phone to explain the process and establish initial contact. Afterwards, a follow-up message was sent to the speech therapists, asking them to specify a convenient time for the interview if they desired to participate. At the scheduled time, the interviews were held online. At the outset of each interview, the interviewer provided a brief summary of the study and addressed any questions from the speech therapists. Permission to record the interview was subsequently obtained.
The interviews took place between November 29, 2022, and August 28, 2023. Each session began with general questions, and then progressed to more specific ones, adapted from a similar study by Chow [27]. Since a semi-structured interview was employed, the questions did not require modification. The interviewer initiated the interview with a specific question (e.g. “what makes it difficult or easy for you to admit PWA?”). The full list of questions can be found in the Appendix 1.
Appendix 1
Date of interview:
Name of interviewee: Ethnicity:
Method of visiting PWA:
Work address:
Phone: Email:
Experience of working with PWA:
1. What makes it difficult/easy for you to admit PWA?
2. In your opinion, what things make it difficult/easy at the beginning of the treatment for PWA?
3. What makes it difficult/easy for you to treat PWA (working with them)?
(deciding on PWA admission, factors affecting the selection of the target, choosing the treatment method, deciding on the frequency and duration of the sessions)
4. In your opinion, what factors hinder/help PWA to attend the sessions?
5. What factors influence your decision about the time of discharge? What factors make your decision-making more difficult and make it easier?
6. What factors make treating these PWA easier/harder for you?
Additional questions were posed based on participants’ responses, for instance “Could you please elaborate on the emotional support?” One of the speech therapists on the research team conducted the interview, which continued until data saturation was reached after interviewing 20 participants. All interviews were audio-recorded.
Data analysis
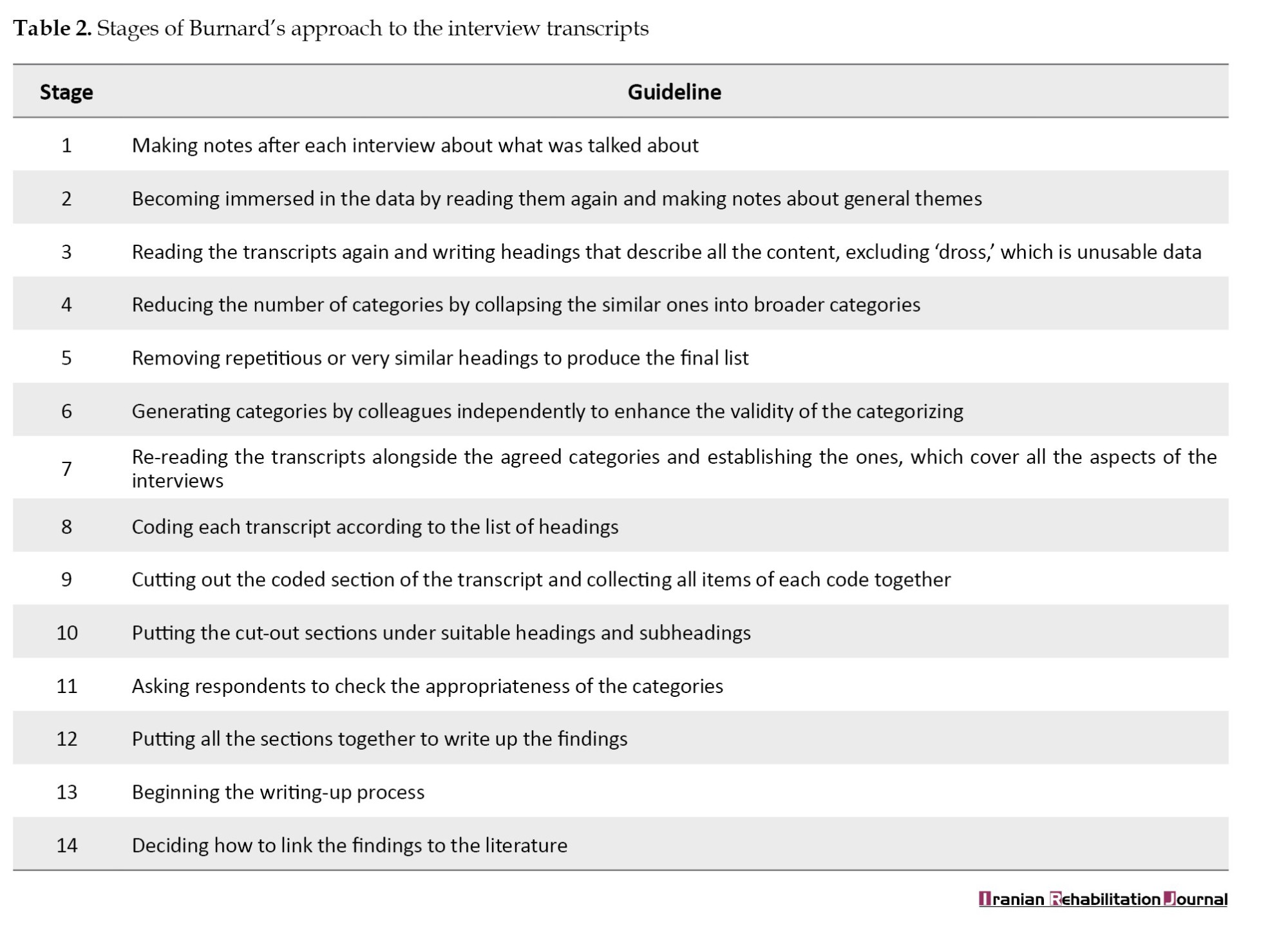
The qualitative content analysis method based on Burnard’s approach was utilized to analyze the data. This approach is specifically designed for semi-structured, open-ended interviews that are fully recorded and consists of 14 stages, as outlined in Table 2 [34].
The first author, a speech therapist with clinical experience in working with PWA, brought a heightened sensitivity to subtle communication nuances during the interviews, which informed the interpretation of the participants’ narratives. However, this professional background may have also introduced certain biases shaped by clinical experiences. To enhance reflexivity and minimize potential bias, the researcher wrote reflective field notes after each interview and discussed emergent interpretations with colleagues outside speech and language therapy, ensuring that alternative perspectives informed the analysis. At the conclusion of each interview, key points from the dialogue were noted, and subsequently, the interviews were transcribed. Two members of the research team independently reviewed the interview transcripts, adhering to the stages of Burnard’s approach (Table 2).
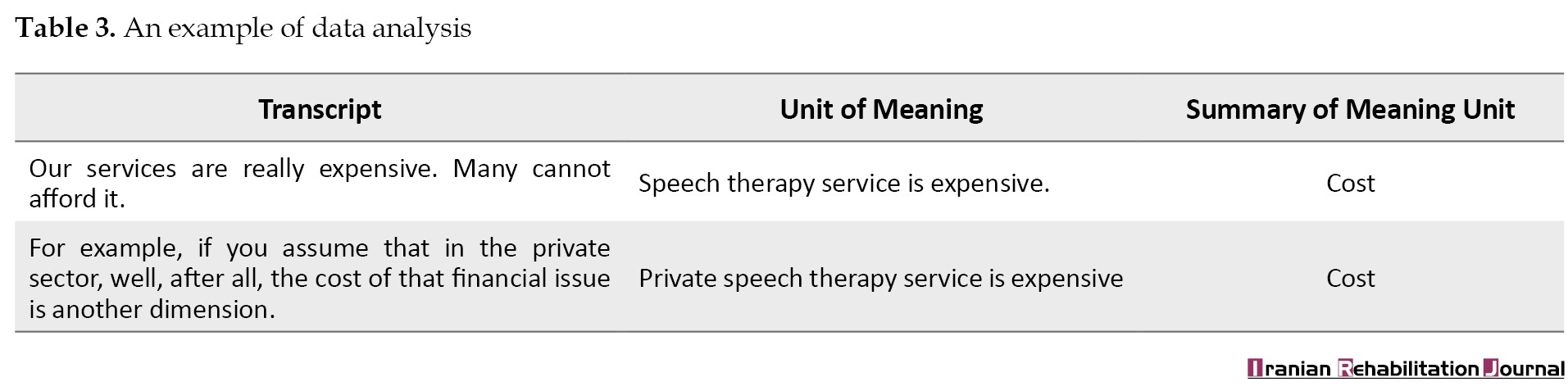
Initially, the two researchers involved in the analysis carefully reviewed the interview transcripts multiple times. Each of them documented the general categories and became immersed in data. They proceeded to extract meaning units, defined as segments of participants’ statements that conveyed specific insights. These meaning units were then summarized and categorized based on their similarities and differences. Subsequently, subcategories and main categories were identified and labeled (Table 3).
Two members of the research team compiled the final list of subcategories and categories. This list was then reviewed and discussed by the entire research team. Ultimately, both researchers reached a consensus on the finalized categories and subcategories, which were subsequently documented. Throughout this process, the original data and earlier versions were referenced multiple times, and the categories were regularly revisited to ensure that the results accurately reflected the content of the data. The categories were organized using Microsoft OneNote software, version 2007. Although OneNote software, version 2007 is not specifically tailored for qualitative analysis, it provided adequate functionality, such as data organization, coding, categorization, and retrieval, to meet the requirements of this study. The emphasis of the analysis was on the systematic approach of the researchers rather than on the software itself. Therefore, the use of OneNote was entirely suitable for the purposes of this research.
Trustworthiness
There are 3 primary perspectives for evaluating data in qualitative studies, with the most recognized being articulated by Guba and Lincoln (1994) [35]. Instead of using the terms validity and reliability, they introduce the concept of trustworthiness or credibility to assess the quality of qualitative research. Trustworthiness reflects the degree to which the results of qualitative research can be trusted. They identify four key criteria: Credibility, dependability, confirmability, and transferability.
Credibility refers to whether the findings accurately capture the intended messages of the participants. Dependability relates to the consistency of findings over time, akin to the concept of reliability in quantitative research. Employing a uniform methodology from the beginning to the end of the coding process and meticulously documenting each step can aid other researchers in replicating the study, even if they do not arrive at identical results [36]. Confirmability assesses the degree to which the findings genuinely represent the data characteristics, as opposed to the researchers’ biases. Finally, transferability pertains to the extent to which the findings can be generalized to other settings or contexts [36].
In this study, the rigor of dependability was reinforced through multiple measures. Two researchers conducted independent reviews of the interview transcripts, deriving categories and subcategories on their own. The results of their analyses were then compared and discussed, with similar categories being retained and differing ones undergoing further examination. Necessary adjustments were made based on this discussion. Additionally, interviewees were invited to review their transcripts to confirm their accuracy, which further bolstered the credibility of the data. Peer checking and member checking were also implemented, with both participants and an audit affirming the findings’ reliability. The “Participants and Methods” section provided a detailed description of the study setting and participant characteristics to enhance transferability.
Results
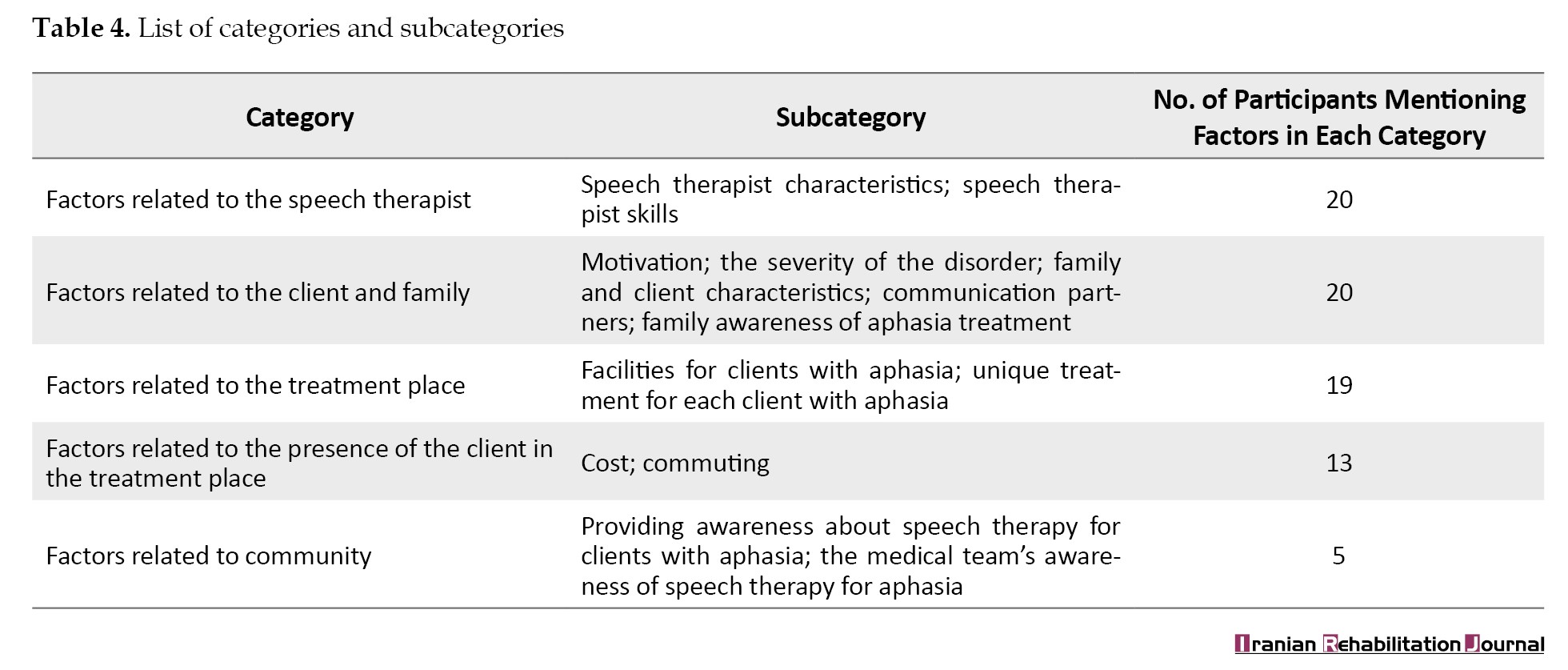
Based on the data analysis, several barriers and facilitators to providing speech therapy services for PWA were identified. These factors often overlapped and were organized into 5 categories and 13 subcategories. Table 4 provides a comprehensive overview of all categories and subcategories.
The facilitators are detailed below, with the absence of these factors indicating a barrier to the provision of speech therapy services for PWAs. Participant quotations are included to illustrate the findings, with de-identified participant codes following each quote to maintain anonymity (i.e. speech therapists are labelled as ‘P’ followed by a number, such as P. 2).
Category 1: Factors related to the speech therapist
All of the speech therapists described the facilitators within this category. Their expertise in treating PWA, along with their patience, high motivation, and familiarity with the PWAs’ language, facilitates treatment.
“There are not many updated treatments, webinars, and workshops for people with stroke in our universities (P. 3).”
“I liked it. I was interested in aphasia since my undergraduate studies. My general tendency was more toward neurology and working with adults. I thought it was fascinating. I felt that I could communicate well with older people, and I enjoyed studying their cases much more. In my mind, it was all very well organized compared to other disorders. That’s why I was interested from the beginning. It was always interesting to me (P. 20).”
Category 2: Factors related to the client and family
All participants mentioned facilitators related to the client and family. The willingness of the family and the PWA to engage in treatment and their patience, along with the low severity of the disorder, were identified as important facilitators. A higher level of family education, appropriate communication with PWAs, and familiarity with speech therapy services also facilitated the initiation of speech therapy services.
Barriers to effective speech therapy included limited family time and the negative personality traits of PWAs or their family members. The involvement of family members in therapy sessions can be beneficial, providing motivation and financial support, or it can be disruptive by causing distractions. The occupational demands and past communication needs of PWAs influenced their motivation and the outcomes of their therapy. Additionally, the value that families placed on speech ability significantly impacted both access to and continuity of treatment. For instance, if a PWA previously held a job that required strong verbal communication skills, this could enhance their motivation to engage in speech therapy sessions.
“It is very important how the family communicates with the client; they should not talk too loudly, be patient, be kind, ...(P. 8)”.
“We know that, in terms of prognostic indicators, one of the most important factors is the severity of language impairment during the acute phase. The more severe the damage, the less likely it is that the patient will return to their original condition (P. 7).”
Category 3: Factors related to the treatment place
Nineteen participants discussed this category. Designating special days for adults, using technology in speech therapy for aphasia, and the possibility of delivering group therapy sessions when needed were considered facilitators in the treatment process. “I had group sessions with PWA, it was very effective, and they were much more motivated in group sessions (P. 3).”
“People who are not familiar with devices often say that having a device is great. But for the past few years, I have been working without one. Of course, I have a physiotherapy device, and I use it for speech therapy. It depends on the therapist’s creativity; for example, with a simple physiotherapy device, a wire stimulator, one can, through creativity, perform a series of manipulations and use it similarly to Vital Stim. I am using it, and it has had a great impact on my work. I mean, having a device is necessary. You can’t rely only on books, pictures, or writing for therapy (P. 12).”
Category 4: Factors related to the presence of the client in the treatment place
Thirteen speech therapists noted that several factors, including the affordability of speech therapy services, financial support for clients, convenient transportation options, and the proximity of the clinics to the homes of PWAs, acted as facilitators in this regard. Participants observed that financial challenges hindered access to services for PWAs, while favorable financial conditions promoted service utilization.
“If there were insurance for PWA, more clients would come to us (P. 8).”
“The patient who comes to the clinic works well. We also don’t have patients on call. It doesn’t matter whether it’s 5 days a week (P. 5).”
Category 5: Factors related to community
Five of the participants discussed facilitators related to this category. A positive attitude among clinic personnel and support from the community for PWAs and their families were identified as key facilitators. Additionally, the medical team, comprising physicians and nurses, served as facilitators by referring PWAs to speech therapy services.
“PWA should be important to the government and even rehabilitation services should be mandatory for them (P. 17).”
“Look, we are doing good work now. As far as I know, many universities are involved, for example, through seminars, webinars, teamwork initiatives, and conferences. At present, doctors, nurses, and other professionals such as occupational therapists and physiotherapists, as well as our own colleagues, are engaged in these efforts. I also see that associations in every province and city are carrying out activities to raise awareness, emphasizing that teamwork is truly needed (P. 20) (Table 4).”
Discussion
This study aimed to explore the experiences of Iranian speech therapists regarding the barriers and facilitators in delivering speech therapy services for PWA. From the insights shared by the speech therapists, 5 main categories and 13 subcategories were identified. The findings not only align with the ICF framework but also contributed to the international literature by contextualizing aphasia service delivery within a sociocultural and financial landscape that has been underexplored in current research.
arriers and facilitators to providing speech therapy services to PWA
First category: Factors related to the speech therapist
According to the ICF, this category is classified as environmental factors. All participants emphasized the importance of the speech therapist’s skills, aligning with previous research indicating that the satisfaction of PWAs often correlates with their therapist’s expertise [23]. However, the present findings expose a notable gap between academic training and clinical requirements in Iran. Similar discrepancies have been observed globally. A 2018 review from Australia highlighted that despite counselling being a vital aspect of speech therapy services, many speech therapists receive inadequate training in this area, resulting in limited knowledge, skills, and confidence in counselling practices [22]. This issue appears particularly prominent in environments where opportunities for professional training are scarce and post-graduation workshops are not routinely available. Therefore, enhancing clinical training and providing structured exposure to PWA during undergraduate programs may be crucial in Iran. Several factors contribute to this expertise. For example, in the present study, speech therapists noted that their own assessments of PWA act as a facilitator in the therapeutic process. Similarly, a study focused on goal setting [37] highlights that ongoing evaluation is a crucial element of therapy. It enables speech therapists to recognize small changes in PWA and make necessary adjustments to the direction of therapy. Providing appropriate educational programs and opportunities for speech therapy students to work directly with individuals who communicate without speech (e.g. PWA) can stimulate a deeper interest in this field. As a result, students are likely to engage in more intensive study, gain practical experience, and develop their expertise. These experiences ultimately lead to the cultivation of more skilled speech therapists and improved treatment outcomes for PWA. Additionally, post-graduation training workshops can further enhance speech therapists’ knowledge and skills in this area. Another notable contribution is that, despite the linguistic diversity in Iran, language differences were seldom perceived as barriers. This finding contrasts with Singapore, where multilingualism and multiculturalism were reported to undermine speech therapists’ confidence [20]. This disparity may be indicative of Iranian therapists’ propensity to operate within their own local linguistic communities, which lessens, though does not entirely eliminate, communication challenges.
Interpersonal aspects of therapy, such as establishing trust and building rapport, were identified as key facilitators. This finding aligns with the findings of Hersh et al. who emphasized the centrality of relational communication in therapy [37]. However, in collectivist cultures like Iran, where family and community ties are deeply valued, these relational skills may play an even stronger role in therapy engagement compared to more individualistic societies.
Second category: Factors related to client and family
According to the ICF, this category falls under the body structure and function and environmental factors construct. PWA characteristics, such as their personality traits, are considered personal factors, while families are categorized as environmental factors.
Families can act as facilitators in communication when they engage appropriately with the PWAs. Other studies have also emphasized the role of family communication. Effective facilitating behaviors include paying attention to the PWA while speaking, allowing sufficient time for responses, focusing on the content of speech rather than how it is articulated, and demonstrating patience during communication. In Howe’s study, families of PWA expressed a need for training on the best strategies for communicating with them. This finding indicates that the concept of effective communication is not sufficiently addressed in treatment sessions [23, 38-40]. Therefore, even if families understand that PWA require different communication methods, they still need training to implement these strategies effectively.
The presence of family members in treatment sessions was seen as a facilitator, encouraging PWA to perform better. Similar findings have been documented in other studies. Having family members present during speech therapy can enhance the PWA’s performance by helping them articulate their needs and facilitating interactions with the speech therapist [22, 39]. Consequently, speech therapists should provide training for families on how to participate in therapy sessions to support the treatment process actively.
High injury severity and the presence of comorbidities were identified as barriers to providing speech therapy services to PWA. Consistent with this study, other research has shown that impairments in expressive and receptive abilities, cognitive challenges, emotional control difficulties, and general issues like fatigue reduce PWA’s participation in the community [38]. Additionally, a lack of motivation among clients in Singapore has been associated with a decline in intervention [20].
Twelve speech therapists discussed family challenges, some of which arose as a result of stroke. One significant issue was financial difficulties. Families of PWA, as noted in the 2011 study by Howe and colleagues, reported new financial burdens and increased responsibilities compared to their situation prior to the stroke [8]. This finding suggests that financial concerns are a common issue. However, in contexts where insurance or state support alleviates some of the costs, Iranian families often bear the full financial responsibility for treatment. This situation exacerbates economic stress and may directly reduce access to and participation in therapy. The lack of comprehensive health insurance in Iran presents a significant barrier.
Therefore, it is essential for families of PWA to receive support from both the government and workplaces to continue treatment. Such support can alleviate financial difficulties and help families manage the additional responsibilities that come with caring for a PWA. Financial assistance, such as loans or insurance coverage, can mitigate economic stress. Additionally, allowing family members to take time off work to care for PWA and raising awareness about managing new responsibilities can further encourage families to stay engaged in the speech therapy process.
Third category: Factors related to the treatment place
All factors in this category fall under the environmental domain of the ICF. The possibility of determining the duration and frequency of the sessions according to the PWAs’ condition facilitated continuation of treatment. Research indicate that intensive therapy is particularly effective for PWA, even in chronic cases. Additionally, PWA who undergo long-term treatment tend to exhibit greater improvement [22, 41]. In the present study, the majority of participants similarly recognized high treatment frequency as a key facilitator.
Moreover, high internet speed was identified as a critical requirement for conducting telerehabilitation sessions. Correspondingly, Caughlin noted that simple, user-friendly technology customized to meet the needs and abilities of PWA enhances the telerehabilitation process and improves outcomes [42].
Fourteen speech therapists expressed concerns over barriers related to the treatment environment and the clinic’s location within the city. Likewise, other studies have identified a high noise level in treatment rooms as a significant barrier [22]. In conclusion, speech therapists should not focus solely on the scientific aspects of therapy; they must also ensure a suitable environment and provide the necessary facilities for PWA.
Fourth category: Factors related to the presence of the client in the treatment place
These factors fall within the environmental domain of ICF. In this study, the low cost of speech therapy services and financial support for PWA were identified as facilitators. Similarly, another study highlighted that having various speech therapy fees aligned with clients’ income levels also served as a facilitator [39]. The findings from these studies can help enhance the role of facilitators in practice in Iran. Additionally, in a study conducted by Howe and colleagues in 2008, 25 PWAs were interviewed regarding environmental factors that affect their social participation. The participants indicated that financial disadvantages associated with aphasia presented a significant barrier [39]. Correspondingly, a study in Singapore noted that the cost of healthcare services emerged as a crucial factor discouraging treatment for both families and PWA [20]. The findings from Iran offer an essential perspective: without widespread insurance coverage, even modest service fees can become unaffordable, especially when factoring in indirect costs like travel and lost wages. This finding puts financial strain not just as an individual obstacle, but as a systemic issue that affects overall participation. As discussed in previous sections, providing financial support for PWA and their families can help them continue speech therapy. Currently, it is crucial to develop such services in Iran.
In the subcategory of challenging commutes, speech therapists noted that transportation issues hindered PWA from accessing treatment. Likewise, many participants in Parr’s study expressed that transportation difficulties often outweighed the advantages of receiving care [43]. Comparisons with earlier data indicate that although financial and transportation barriers are commonly experienced, their impact is exacerbated in countries with limited social support systems.
Fifth category: Factors related to community
Rising awareness through speech therapists and influential institutions, along with referrals of PWA to speech therapy by medical professionals, has been reported to enhance family understanding of the condition. Governments should leverage media and other credible resources to disseminate information about aphasia and its treatments. A study identified increased awareness of aphasia as a key facilitator [23]. Similarly, in Hinckley’s study, both PWA and their caregivers noted that physicians often have limited knowledge regarding aphasia and its treatment options [44]. A significant barrier in this area is the community’s lack of support for PWA and their families. Another study revealed that families of PWA express the need for both financial and emotional assistance [8]. Moreover, a small number of participants in Hersh’s study indicated that government policies addressing the needs of PWA were insufficient [45].
From an ICF perspective, this finding underscores how environmental and personal factors intersect, with community-level deficiencies imposing additional pressure on therapists and families, thereby influencing the social participation of PWA.
Conclusion
This study examined the barriers and facilitators to providing speech therapy services for PWA from the viewpoints of Iranian speech therapists. Several factors were consistently identified across the participants’ interviews. Although the frequency of these barriers and facilitators was not the primary focus of this research, the identification of common factors underscores their significant impact on treatment outcomes. All participants noted the expertise of the speech therapist as a key facilitator. Other facilitators highlighted by nearly all participants included the involvement of the PWA, their family, and the characteristics of the treatment environment. The most frequently cited barriers involved the attributes of the PWA and their family, as well as the communication partners. In conclusion, the success of speech therapy relies heavily on the active engagement of speech therapists, PWA, families, and the broader community. As there have been no studies on the quality of speech therapy services provided to PWA in Iran, the findings of this study can assist in investigating the factors that influence these services. By analyzing the factors identified from participants’ interviews, we can develop strategies to mitigate barriers and enhance facilitators, with the support of stakeholders in this field. This approach aims to improve the quality of life for PWA and their families, while ensuring that the time and efforts of speech therapists, as well as the resources and time of PWA, are utilized more effectively.
Study limitations
This study, like other research projects, faced several limitations. First, the time constraints experienced by some speech therapists prevented them from participating in the study. Second, there is a potential for bias in the information provided by the interviewees. Third, while online interviews offered convenience, they may have inadvertently excluded therapists with limited internet access, thereby limiting participant diversity. Fourth, the self-selection of participants could have introduced bias, as those with greater interest or confidence in the topic may have been more inclined to take part. Finally, it is essential to acknowledge the limited generalizability of the findings, considering the qualitative nature of the research and the small sample size.
Key recommendations
Clinical educators should provide students with sufficient training and practical opportunities in aphasia therapy during their education. Policy makers should offer financial and structural support for PWA and their families to facilitate continuity of speech therapy. Clinic administrators should provide a suitable environment and the necessary facilities for speech therapists, as well as create opportunities for their ongoing professional development and learning. Public health authorities and professionals should raise awareness about aphasia and its treatment among both the public and healthcare providers.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences, Isfahan, Iran (Code: IR.MUI.RESEARCH.REC.1399.503). Informed consent was obtained from each participant in two copies to enter the study. We de-identified the participants by assigning a unique number to each, rather than using their names. After the analysis was completed, each individual was informed of the study’s results.
Funding
This article was extracted from the master’s thesis of Zahra Poursaeid, approved by Isfahan University of Medical Sciences, Isfahan, Iran (Code: 399531) and financially supported by Isfahan University of Medical Sciences, Isfahan, Iran.
Authors' contributions
Conceptualization, supervision, investigation, data analysis and writing: All authors; Data collection: Zahra Poursaeid and Leila Ghasisin; Funding acquisition and resources: Leila Ghasisin.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Authors are grateful to all speech therapists who cooperated in this project.
Brain strokes are the third leading cause of death, the second leading cause of dementia, as well as the primary cause of adult disability in Western countries [1]. In Iran, it ranked as the second leading cause of death in 2016 [2]. Stroke survivors frequently face various complications [3], with aphasia being a common manifestation that can appear within hours of the event [1]. Aphasia is an acquired language disorder that impacts all aspects of language functioning, including comprehension, expression, reading, and writing [4]. While stroke is the most prevalent cause, other neurological impairments can also result in aphasia [4]. Due to its significant effects on communication, aphasia is regarded as a major communication disability that influences daily activities, social participation, and social roles of people with aphasia (PWA) [5, 6]. The negative ramifications of aphasia often endure for a lifetime [7] and also significantly affect families, who may come across physical, emotional, and financial challenges [8-11].
As there are limited medical treatments available to mitigate the effects of aphasia, rehabilitation serves as the cornerstone of recovery for PWA [12]. Evidence supports the effectiveness of rehabilitation [11], particularly when initiated early in the recovery process [12]. Most treatments for PWA are provided through clinical sessions by qualified speech therapists to address communication problems [11, 13].
As the population ages and more individuals survive strokes [13], the prevalence of chronic disabilities, such as aphasia is projected to increase, highlighting the necessity for evidence-based care [14]. However, research reveals a notable disconnection between recommended practices and the actual delivery of services [15]. For instance, in Australia, 75% of PWA who were eligible for speech therapy did not receive any treatment during their hospitalization [16]. Furthermore, even when speech therapy is available, its frequency and intensity often fall short of the recommended guidelines [13]. Additionally, although PWA can benefit from being involved in the goal-setting process [17], they are rarely included in this stage [18]. Speech therapists have identified several barriers to delivering high-quality services, including insufficient training and a lack of confidence among professionals [19-21], as well as constraints, such as limited time and resources, a focus on dysphagia, and brief hospital stays [13]. Conversely, certain factors can facilitate the provision of effective treatment. These factors include the application of the International Classification of Functioning, Disability and Health (ICF) framework [22], availability of insurance coverage [13], and the satisfaction of PWA with their speech therapist [23].
Emerging evidence has begun to explore the barriers and facilitators associated with providing rehabilitation to PWA [15]. However, the factors influencing treatment vary significantly from country to country [19].
In Iran, there is currently no comprehensive data concerning the status, barriers, or facilitators of speech therapy for PWA. It appears that we are still far from delivering the evidence-based treatments necessary to enhance the communicative abilities of those affected [13]. Since its introduction in 1974, speech therapy education has expanded, now offered at the bachelor of science (BS), master of science (MSc), and doctor of philosophy (PhD) levels. Speech therapists are employed in hospitals and rehabilitation centers nationwide [24].
Local studies indicate that the incidence of stroke is higher and occurs at a younger age compared to Western countries [20]. Demographic forecasts suggest that by 2031, 25–30% of Iran’s population will be aged 50 or older [25]. Since most strokes occur in individuals aged 65 and above [3, 26], the burden of stroke and aphasia is expected to increase significantly in Iran. The ICF framework offers a comprehensive model for understanding the functional impact of aphasia [6, 22, 23]. However, despite its importance, knowledge regarding how rehabilitation services in Iran cater to the needs of PWA remains limited. This research aims to investigate the barriers and facilitators within this context.
To enhance services for individuals with disabilities in the community, it is essential to evaluate the current state of these services [27]. Gaining this insight enables us to assess whether care for PWA is being delivered optimally, which has significant implications for practice planning and future research [20, 22]. Therefore, this study aimed to explore the barriers and facilitators of speech therapy for aphasia as perceived by Iranian speech therapists.
Materials and Methods
This study aimed to explore the barriers and facilitators impacting the provision of speech therapy services from the perspective of speech therapists. A qualitative approach was adopted, utilizing content analysis, which is particularly effective when existing theory or literature on a phenomenon is limited. In this method, the researcher immerses themselves in the data to gain fresh insights into the phenomenon under investigation, with findings directly drawn from the data [28, 29]. The rationale for selecting this method was to achieve an in-depth understanding of the participants’ lived experiences with speech therapy services for aphasia. Data were gathered through semi-structured individual interviews with open-ended questions. Interviews are a standard method of data collection in qualitative research, and the use of open-ended questions allows interviewees to respond in their own words, enabling them to share their feelings, thoughts, and experiences without restraint [30, 31]. Interviews can vary along a continuum from unstructured to structured formats [30]. In semi-structured interviews, a set of prepared questions is utilized, although the order of these questions may be adjusted based on the flow of conversation and the responses of interviewees [31].
Study participants
In qualitative research, sampling continues until data saturation is achieved. Data saturation refers to the point at which information becomes repetitive and no new insights are gathered [30]. In the current study, data saturation was reached after 20 interviews, as the analysis of the final interviews revealed no additional information compared to earlier ones. To ensure this, we continuously compared new data with existing categories and confirmed that subsequent interviews yielded only repetitive information.
Twenty speech therapists participated in the study, all of whom had experience providing treatment to PWA in Iran. Table 1 lists the characteristics of speech therapists.
Of the participants, 13 were females and 7 were males. Fifteen had experience in home visits, 11 in hospitals, 16 in private clinics, and 10 in other settings, such as university-affiliated and public clinics. All participants worked in urban areas. Their working experience with PWA ranged from a minimum of 3 months to a maximum of 20 years, with an average experience of 14 years. In qualitative research, the goal is to identify cases that are rich in information—ones that can provide insights into the phenomenon being studied [32]. The purposive sampling method is the most effective approach for gaining new insights into the subject or achieving a deep understanding of a complex experience or event [33]. Therefore, in this study, the purposive sampling method was employed to select participants based on their experience providing speech therapy services for PWA.
The inclusion criteria required participants to sign the informed consent form, possess at least a bachelor’s degree in speech therapy, and have experience working with at least one individual with aphasia. All participants verified the accuracy of their interview transcripts; consequently, no interviews were excluded from the study.
Sampling
The interviews were conducted online, with each participant participating in a single session that included multiple interactions. Initially, the research team posted an announcement on virtual networks associated with speech therapy, outlining the procedure and inviting eligible speech therapists to express their interest via phone. Before the interviews, the team reached out to each participant by phone to explain the process and establish initial contact. Afterwards, a follow-up message was sent to the speech therapists, asking them to specify a convenient time for the interview if they desired to participate. At the scheduled time, the interviews were held online. At the outset of each interview, the interviewer provided a brief summary of the study and addressed any questions from the speech therapists. Permission to record the interview was subsequently obtained.
The interviews took place between November 29, 2022, and August 28, 2023. Each session began with general questions, and then progressed to more specific ones, adapted from a similar study by Chow [27]. Since a semi-structured interview was employed, the questions did not require modification. The interviewer initiated the interview with a specific question (e.g. “what makes it difficult or easy for you to admit PWA?”). The full list of questions can be found in the Appendix 1.
Appendix 1
Date of interview:
Name of interviewee: Ethnicity:
Method of visiting PWA:
Work address:
Phone: Email:
Experience of working with PWA:
1. What makes it difficult/easy for you to admit PWA?
2. In your opinion, what things make it difficult/easy at the beginning of the treatment for PWA?
3. What makes it difficult/easy for you to treat PWA (working with them)?
(deciding on PWA admission, factors affecting the selection of the target, choosing the treatment method, deciding on the frequency and duration of the sessions)
4. In your opinion, what factors hinder/help PWA to attend the sessions?
5. What factors influence your decision about the time of discharge? What factors make your decision-making more difficult and make it easier?
6. What factors make treating these PWA easier/harder for you?
Additional questions were posed based on participants’ responses, for instance “Could you please elaborate on the emotional support?” One of the speech therapists on the research team conducted the interview, which continued until data saturation was reached after interviewing 20 participants. All interviews were audio-recorded.
Data analysis
The qualitative content analysis method based on Burnard’s approach was utilized to analyze the data. This approach is specifically designed for semi-structured, open-ended interviews that are fully recorded and consists of 14 stages, as outlined in Table 2 [34].
The first author, a speech therapist with clinical experience in working with PWA, brought a heightened sensitivity to subtle communication nuances during the interviews, which informed the interpretation of the participants’ narratives. However, this professional background may have also introduced certain biases shaped by clinical experiences. To enhance reflexivity and minimize potential bias, the researcher wrote reflective field notes after each interview and discussed emergent interpretations with colleagues outside speech and language therapy, ensuring that alternative perspectives informed the analysis. At the conclusion of each interview, key points from the dialogue were noted, and subsequently, the interviews were transcribed. Two members of the research team independently reviewed the interview transcripts, adhering to the stages of Burnard’s approach (Table 2).
Initially, the two researchers involved in the analysis carefully reviewed the interview transcripts multiple times. Each of them documented the general categories and became immersed in data. They proceeded to extract meaning units, defined as segments of participants’ statements that conveyed specific insights. These meaning units were then summarized and categorized based on their similarities and differences. Subsequently, subcategories and main categories were identified and labeled (Table 3).
Two members of the research team compiled the final list of subcategories and categories. This list was then reviewed and discussed by the entire research team. Ultimately, both researchers reached a consensus on the finalized categories and subcategories, which were subsequently documented. Throughout this process, the original data and earlier versions were referenced multiple times, and the categories were regularly revisited to ensure that the results accurately reflected the content of the data. The categories were organized using Microsoft OneNote software, version 2007. Although OneNote software, version 2007 is not specifically tailored for qualitative analysis, it provided adequate functionality, such as data organization, coding, categorization, and retrieval, to meet the requirements of this study. The emphasis of the analysis was on the systematic approach of the researchers rather than on the software itself. Therefore, the use of OneNote was entirely suitable for the purposes of this research.
Trustworthiness
There are 3 primary perspectives for evaluating data in qualitative studies, with the most recognized being articulated by Guba and Lincoln (1994) [35]. Instead of using the terms validity and reliability, they introduce the concept of trustworthiness or credibility to assess the quality of qualitative research. Trustworthiness reflects the degree to which the results of qualitative research can be trusted. They identify four key criteria: Credibility, dependability, confirmability, and transferability.
Credibility refers to whether the findings accurately capture the intended messages of the participants. Dependability relates to the consistency of findings over time, akin to the concept of reliability in quantitative research. Employing a uniform methodology from the beginning to the end of the coding process and meticulously documenting each step can aid other researchers in replicating the study, even if they do not arrive at identical results [36]. Confirmability assesses the degree to which the findings genuinely represent the data characteristics, as opposed to the researchers’ biases. Finally, transferability pertains to the extent to which the findings can be generalized to other settings or contexts [36].
In this study, the rigor of dependability was reinforced through multiple measures. Two researchers conducted independent reviews of the interview transcripts, deriving categories and subcategories on their own. The results of their analyses were then compared and discussed, with similar categories being retained and differing ones undergoing further examination. Necessary adjustments were made based on this discussion. Additionally, interviewees were invited to review their transcripts to confirm their accuracy, which further bolstered the credibility of the data. Peer checking and member checking were also implemented, with both participants and an audit affirming the findings’ reliability. The “Participants and Methods” section provided a detailed description of the study setting and participant characteristics to enhance transferability.
Results
Based on the data analysis, several barriers and facilitators to providing speech therapy services for PWA were identified. These factors often overlapped and were organized into 5 categories and 13 subcategories. Table 4 provides a comprehensive overview of all categories and subcategories.
The facilitators are detailed below, with the absence of these factors indicating a barrier to the provision of speech therapy services for PWAs. Participant quotations are included to illustrate the findings, with de-identified participant codes following each quote to maintain anonymity (i.e. speech therapists are labelled as ‘P’ followed by a number, such as P. 2).
Category 1: Factors related to the speech therapist
All of the speech therapists described the facilitators within this category. Their expertise in treating PWA, along with their patience, high motivation, and familiarity with the PWAs’ language, facilitates treatment.
“There are not many updated treatments, webinars, and workshops for people with stroke in our universities (P. 3).”
“I liked it. I was interested in aphasia since my undergraduate studies. My general tendency was more toward neurology and working with adults. I thought it was fascinating. I felt that I could communicate well with older people, and I enjoyed studying their cases much more. In my mind, it was all very well organized compared to other disorders. That’s why I was interested from the beginning. It was always interesting to me (P. 20).”
Category 2: Factors related to the client and family
All participants mentioned facilitators related to the client and family. The willingness of the family and the PWA to engage in treatment and their patience, along with the low severity of the disorder, were identified as important facilitators. A higher level of family education, appropriate communication with PWAs, and familiarity with speech therapy services also facilitated the initiation of speech therapy services.
Barriers to effective speech therapy included limited family time and the negative personality traits of PWAs or their family members. The involvement of family members in therapy sessions can be beneficial, providing motivation and financial support, or it can be disruptive by causing distractions. The occupational demands and past communication needs of PWAs influenced their motivation and the outcomes of their therapy. Additionally, the value that families placed on speech ability significantly impacted both access to and continuity of treatment. For instance, if a PWA previously held a job that required strong verbal communication skills, this could enhance their motivation to engage in speech therapy sessions.
“It is very important how the family communicates with the client; they should not talk too loudly, be patient, be kind, ...(P. 8)”.
“We know that, in terms of prognostic indicators, one of the most important factors is the severity of language impairment during the acute phase. The more severe the damage, the less likely it is that the patient will return to their original condition (P. 7).”
Category 3: Factors related to the treatment place
Nineteen participants discussed this category. Designating special days for adults, using technology in speech therapy for aphasia, and the possibility of delivering group therapy sessions when needed were considered facilitators in the treatment process. “I had group sessions with PWA, it was very effective, and they were much more motivated in group sessions (P. 3).”
“People who are not familiar with devices often say that having a device is great. But for the past few years, I have been working without one. Of course, I have a physiotherapy device, and I use it for speech therapy. It depends on the therapist’s creativity; for example, with a simple physiotherapy device, a wire stimulator, one can, through creativity, perform a series of manipulations and use it similarly to Vital Stim. I am using it, and it has had a great impact on my work. I mean, having a device is necessary. You can’t rely only on books, pictures, or writing for therapy (P. 12).”
Category 4: Factors related to the presence of the client in the treatment place
Thirteen speech therapists noted that several factors, including the affordability of speech therapy services, financial support for clients, convenient transportation options, and the proximity of the clinics to the homes of PWAs, acted as facilitators in this regard. Participants observed that financial challenges hindered access to services for PWAs, while favorable financial conditions promoted service utilization.
“If there were insurance for PWA, more clients would come to us (P. 8).”
“The patient who comes to the clinic works well. We also don’t have patients on call. It doesn’t matter whether it’s 5 days a week (P. 5).”
Category 5: Factors related to community
Five of the participants discussed facilitators related to this category. A positive attitude among clinic personnel and support from the community for PWAs and their families were identified as key facilitators. Additionally, the medical team, comprising physicians and nurses, served as facilitators by referring PWAs to speech therapy services.
“PWA should be important to the government and even rehabilitation services should be mandatory for them (P. 17).”
“Look, we are doing good work now. As far as I know, many universities are involved, for example, through seminars, webinars, teamwork initiatives, and conferences. At present, doctors, nurses, and other professionals such as occupational therapists and physiotherapists, as well as our own colleagues, are engaged in these efforts. I also see that associations in every province and city are carrying out activities to raise awareness, emphasizing that teamwork is truly needed (P. 20) (Table 4).”
Discussion
This study aimed to explore the experiences of Iranian speech therapists regarding the barriers and facilitators in delivering speech therapy services for PWA. From the insights shared by the speech therapists, 5 main categories and 13 subcategories were identified. The findings not only align with the ICF framework but also contributed to the international literature by contextualizing aphasia service delivery within a sociocultural and financial landscape that has been underexplored in current research.
arriers and facilitators to providing speech therapy services to PWA
First category: Factors related to the speech therapist
According to the ICF, this category is classified as environmental factors. All participants emphasized the importance of the speech therapist’s skills, aligning with previous research indicating that the satisfaction of PWAs often correlates with their therapist’s expertise [23]. However, the present findings expose a notable gap between academic training and clinical requirements in Iran. Similar discrepancies have been observed globally. A 2018 review from Australia highlighted that despite counselling being a vital aspect of speech therapy services, many speech therapists receive inadequate training in this area, resulting in limited knowledge, skills, and confidence in counselling practices [22]. This issue appears particularly prominent in environments where opportunities for professional training are scarce and post-graduation workshops are not routinely available. Therefore, enhancing clinical training and providing structured exposure to PWA during undergraduate programs may be crucial in Iran. Several factors contribute to this expertise. For example, in the present study, speech therapists noted that their own assessments of PWA act as a facilitator in the therapeutic process. Similarly, a study focused on goal setting [37] highlights that ongoing evaluation is a crucial element of therapy. It enables speech therapists to recognize small changes in PWA and make necessary adjustments to the direction of therapy. Providing appropriate educational programs and opportunities for speech therapy students to work directly with individuals who communicate without speech (e.g. PWA) can stimulate a deeper interest in this field. As a result, students are likely to engage in more intensive study, gain practical experience, and develop their expertise. These experiences ultimately lead to the cultivation of more skilled speech therapists and improved treatment outcomes for PWA. Additionally, post-graduation training workshops can further enhance speech therapists’ knowledge and skills in this area. Another notable contribution is that, despite the linguistic diversity in Iran, language differences were seldom perceived as barriers. This finding contrasts with Singapore, where multilingualism and multiculturalism were reported to undermine speech therapists’ confidence [20]. This disparity may be indicative of Iranian therapists’ propensity to operate within their own local linguistic communities, which lessens, though does not entirely eliminate, communication challenges.
Interpersonal aspects of therapy, such as establishing trust and building rapport, were identified as key facilitators. This finding aligns with the findings of Hersh et al. who emphasized the centrality of relational communication in therapy [37]. However, in collectivist cultures like Iran, where family and community ties are deeply valued, these relational skills may play an even stronger role in therapy engagement compared to more individualistic societies.
Second category: Factors related to client and family
According to the ICF, this category falls under the body structure and function and environmental factors construct. PWA characteristics, such as their personality traits, are considered personal factors, while families are categorized as environmental factors.
Families can act as facilitators in communication when they engage appropriately with the PWAs. Other studies have also emphasized the role of family communication. Effective facilitating behaviors include paying attention to the PWA while speaking, allowing sufficient time for responses, focusing on the content of speech rather than how it is articulated, and demonstrating patience during communication. In Howe’s study, families of PWA expressed a need for training on the best strategies for communicating with them. This finding indicates that the concept of effective communication is not sufficiently addressed in treatment sessions [23, 38-40]. Therefore, even if families understand that PWA require different communication methods, they still need training to implement these strategies effectively.
The presence of family members in treatment sessions was seen as a facilitator, encouraging PWA to perform better. Similar findings have been documented in other studies. Having family members present during speech therapy can enhance the PWA’s performance by helping them articulate their needs and facilitating interactions with the speech therapist [22, 39]. Consequently, speech therapists should provide training for families on how to participate in therapy sessions to support the treatment process actively.
High injury severity and the presence of comorbidities were identified as barriers to providing speech therapy services to PWA. Consistent with this study, other research has shown that impairments in expressive and receptive abilities, cognitive challenges, emotional control difficulties, and general issues like fatigue reduce PWA’s participation in the community [38]. Additionally, a lack of motivation among clients in Singapore has been associated with a decline in intervention [20].
Twelve speech therapists discussed family challenges, some of which arose as a result of stroke. One significant issue was financial difficulties. Families of PWA, as noted in the 2011 study by Howe and colleagues, reported new financial burdens and increased responsibilities compared to their situation prior to the stroke [8]. This finding suggests that financial concerns are a common issue. However, in contexts where insurance or state support alleviates some of the costs, Iranian families often bear the full financial responsibility for treatment. This situation exacerbates economic stress and may directly reduce access to and participation in therapy. The lack of comprehensive health insurance in Iran presents a significant barrier.
Therefore, it is essential for families of PWA to receive support from both the government and workplaces to continue treatment. Such support can alleviate financial difficulties and help families manage the additional responsibilities that come with caring for a PWA. Financial assistance, such as loans or insurance coverage, can mitigate economic stress. Additionally, allowing family members to take time off work to care for PWA and raising awareness about managing new responsibilities can further encourage families to stay engaged in the speech therapy process.
Third category: Factors related to the treatment place
All factors in this category fall under the environmental domain of the ICF. The possibility of determining the duration and frequency of the sessions according to the PWAs’ condition facilitated continuation of treatment. Research indicate that intensive therapy is particularly effective for PWA, even in chronic cases. Additionally, PWA who undergo long-term treatment tend to exhibit greater improvement [22, 41]. In the present study, the majority of participants similarly recognized high treatment frequency as a key facilitator.
Moreover, high internet speed was identified as a critical requirement for conducting telerehabilitation sessions. Correspondingly, Caughlin noted that simple, user-friendly technology customized to meet the needs and abilities of PWA enhances the telerehabilitation process and improves outcomes [42].
Fourteen speech therapists expressed concerns over barriers related to the treatment environment and the clinic’s location within the city. Likewise, other studies have identified a high noise level in treatment rooms as a significant barrier [22]. In conclusion, speech therapists should not focus solely on the scientific aspects of therapy; they must also ensure a suitable environment and provide the necessary facilities for PWA.
Fourth category: Factors related to the presence of the client in the treatment place
These factors fall within the environmental domain of ICF. In this study, the low cost of speech therapy services and financial support for PWA were identified as facilitators. Similarly, another study highlighted that having various speech therapy fees aligned with clients’ income levels also served as a facilitator [39]. The findings from these studies can help enhance the role of facilitators in practice in Iran. Additionally, in a study conducted by Howe and colleagues in 2008, 25 PWAs were interviewed regarding environmental factors that affect their social participation. The participants indicated that financial disadvantages associated with aphasia presented a significant barrier [39]. Correspondingly, a study in Singapore noted that the cost of healthcare services emerged as a crucial factor discouraging treatment for both families and PWA [20]. The findings from Iran offer an essential perspective: without widespread insurance coverage, even modest service fees can become unaffordable, especially when factoring in indirect costs like travel and lost wages. This finding puts financial strain not just as an individual obstacle, but as a systemic issue that affects overall participation. As discussed in previous sections, providing financial support for PWA and their families can help them continue speech therapy. Currently, it is crucial to develop such services in Iran.
In the subcategory of challenging commutes, speech therapists noted that transportation issues hindered PWA from accessing treatment. Likewise, many participants in Parr’s study expressed that transportation difficulties often outweighed the advantages of receiving care [43]. Comparisons with earlier data indicate that although financial and transportation barriers are commonly experienced, their impact is exacerbated in countries with limited social support systems.
Fifth category: Factors related to community
Rising awareness through speech therapists and influential institutions, along with referrals of PWA to speech therapy by medical professionals, has been reported to enhance family understanding of the condition. Governments should leverage media and other credible resources to disseminate information about aphasia and its treatments. A study identified increased awareness of aphasia as a key facilitator [23]. Similarly, in Hinckley’s study, both PWA and their caregivers noted that physicians often have limited knowledge regarding aphasia and its treatment options [44]. A significant barrier in this area is the community’s lack of support for PWA and their families. Another study revealed that families of PWA express the need for both financial and emotional assistance [8]. Moreover, a small number of participants in Hersh’s study indicated that government policies addressing the needs of PWA were insufficient [45].
From an ICF perspective, this finding underscores how environmental and personal factors intersect, with community-level deficiencies imposing additional pressure on therapists and families, thereby influencing the social participation of PWA.
Conclusion
This study examined the barriers and facilitators to providing speech therapy services for PWA from the viewpoints of Iranian speech therapists. Several factors were consistently identified across the participants’ interviews. Although the frequency of these barriers and facilitators was not the primary focus of this research, the identification of common factors underscores their significant impact on treatment outcomes. All participants noted the expertise of the speech therapist as a key facilitator. Other facilitators highlighted by nearly all participants included the involvement of the PWA, their family, and the characteristics of the treatment environment. The most frequently cited barriers involved the attributes of the PWA and their family, as well as the communication partners. In conclusion, the success of speech therapy relies heavily on the active engagement of speech therapists, PWA, families, and the broader community. As there have been no studies on the quality of speech therapy services provided to PWA in Iran, the findings of this study can assist in investigating the factors that influence these services. By analyzing the factors identified from participants’ interviews, we can develop strategies to mitigate barriers and enhance facilitators, with the support of stakeholders in this field. This approach aims to improve the quality of life for PWA and their families, while ensuring that the time and efforts of speech therapists, as well as the resources and time of PWA, are utilized more effectively.
Study limitations
This study, like other research projects, faced several limitations. First, the time constraints experienced by some speech therapists prevented them from participating in the study. Second, there is a potential for bias in the information provided by the interviewees. Third, while online interviews offered convenience, they may have inadvertently excluded therapists with limited internet access, thereby limiting participant diversity. Fourth, the self-selection of participants could have introduced bias, as those with greater interest or confidence in the topic may have been more inclined to take part. Finally, it is essential to acknowledge the limited generalizability of the findings, considering the qualitative nature of the research and the small sample size.
Key recommendations
Clinical educators should provide students with sufficient training and practical opportunities in aphasia therapy during their education. Policy makers should offer financial and structural support for PWA and their families to facilitate continuity of speech therapy. Clinic administrators should provide a suitable environment and the necessary facilities for speech therapists, as well as create opportunities for their ongoing professional development and learning. Public health authorities and professionals should raise awareness about aphasia and its treatment among both the public and healthcare providers.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences, Isfahan, Iran (Code: IR.MUI.RESEARCH.REC.1399.503). Informed consent was obtained from each participant in two copies to enter the study. We de-identified the participants by assigning a unique number to each, rather than using their names. After the analysis was completed, each individual was informed of the study’s results.
Funding
This article was extracted from the master’s thesis of Zahra Poursaeid, approved by Isfahan University of Medical Sciences, Isfahan, Iran (Code: 399531) and financially supported by Isfahan University of Medical Sciences, Isfahan, Iran.
Authors' contributions
Conceptualization, supervision, investigation, data analysis and writing: All authors; Data collection: Zahra Poursaeid and Leila Ghasisin; Funding acquisition and resources: Leila Ghasisin.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Authors are grateful to all speech therapists who cooperated in this project.
References
- Croquelois A, Bogousslavsky J. Stroke aphasia: 1,500 consecutive cases. Cerebrovascular Diseases. 2011; 31(4):392-399. [DOI:10.1159/000323217] [PMID]
- Aghamohammadi S, Kazemi E, Khosravi A, Kazemeini H. The trend of ten leading causes of death in the Islamic Republic of Iran, 2006-2011. Iranian Journal of Epidemiology. 2017; 12(4):1-11. [Link]
- Kelly-Hayes M. Influence of age and health behaviors on stroke risk: Lessons from longitudinal studies. Journal of the American Geriatrics Society. 2010; 58:S325-S8. [DOI:10.1111/j.1532-5415.2010.02915.x] [PMID]
- Le Dorze G, Signori FH. Needs, barriers and facilitators experienced by spouses of people with aphasia. Disability and Rehabilitation. 2010; 32(13):1073-87. [DOI:10.3109/09638280903374121] [PMID]
- Berg K, Isaksen J, Wallace SJ, Cruice M, Simmons-Mackie N, Worrall L. Establishing consensus on a definition of aphasia: an e-Delphi study of international aphasia researchers. Aphasiology. 2022; 36(4):385-400. [DOI:10.1080/02687038.2020.1852003]
- Simmons-Mackie N, Kagan A. Application of the ICF in aphasia. Seminars in Speech and Language. 2007; 28(4):244-53. [DOI:10.1055/s-2007-986521] [PMID]
- Brown K, Worrall L, Davidson B, Howe T. Snapshots of success: An insider perspective on living successfully with aphasia. Aphasiology. 2010; 24(10):1267-95. [DOI:10.1080/02687031003755429]
- Howe T, Davidson B, Worrall L, Hersh D, Ferguson A, Sherratt S, et al. ‘You needed to rehab… families as well’: Family members’ own goals for aphasia rehabilitation.International Journal of Language & Communication Disorders. 2012; 47(5):511-21. [DOI:10.1111/j.1460-6984.2012.00159.x] [PMID]
- Sherratt S, Worrall L, Pearson C, Howe T, Hersh D, Davidson B. “Well it has to be language-related”: Speech-language pathologists’ goals for people with aphasia and their families. International Journal of Speech-Language Pathology. 2011; 13(4):317-28. [DOI:10.3109/17549507.2011.584632] [PMID]
- Bethoux F, Calmels P, Gautheron V, Minaire P. Quality of life of the spouses of stroke patients: A preliminary study. The International Journal of Robotics Research. 1996; 19(4):291-300. [DOI:10.1097/00004356-199612000-00001] [PMID]
- Holland AL, Fromm DS, DeRuyter F, Stein M. Treatment efficacy: Aphasia. Journal of Speech, Language, and Hearing Research. 1996; 39(5):S27-36. [DOI:10.1044/jshr.3905.s27] [PMID]
- Godecke E, Armstrong EA, Rai T, Middleton S, Ciccone N, Whitworth A, et al. A randomized controlled trial of very early rehabilitation in speech after stroke. London: SAGE Publications; 2016. [DOI:10.1177/1747493016641116] [PMID]
- Code C, Petheram B. Delivering for aphasia. International Journal of Speech-Language Pathology. 2011; 13(1):3-10 [DOI:10.3109/17549507.2010.520090] [PMID]
- Greener J, Langhorne P. Systematic reviews in rehabilitation for stroke: Issues and approaches to addressing them. Clinical Rehabilitation. 2002; 16(1):69-74. [DOI:10.1191/0269215502cr469oa] [PMID]
- Hinckley JJ. Finding messages in bottles: Living successfully with stroke and aphasia. Topics in Stroke Rehabilitation. 2006; 13(1):25-36. [DOI:10.1310/FLJ3-04DQ-MG8W-89EU] [PMID]
- Shrubsole K, Worrall L, Power E, O’Connor DA. Barriers and facilitators to meeting aphasia guideline recommendations: What factors influence speech pathologists’ practice? Disability and Rehabilitation. 2019; 41(13):1596-607. [DOI:10.1080/09638288.2018.1432706] [PMID]
- Rohde A, Townley-O’Neill K, Trendall K, Worrall L, Cornwell P. A comparison of client and therapist goals for people with aphasia: A qualitative exploratory study. Aphasiology. 2012; 26(10):1298-315. [DOI:10.1080/02687038.2012.706799]
- Worrall L, Sherratt S, Rogers P, Howe T, Hersh D, Ferguson A, et al. What people with aphasia want: Their goals according to the ICF. Aphasiology. 2011; 25(3):309-22. [DOI:10.1080/02687038.2010.508530]
- Alary Gauvreau C, Le Dorze G, Croteau C, Hallé M-C. Understanding practices of speech-language pathologists in aphasia rehabilitation: A grounded theory study. Aphasiology. 2019; 33(7):846-64. [DOI:10.1080/02687038.2019.1602814]
- Guo YE, Togher L, Power E. Speech pathology services for people with aphasia: What is the current practice in Singapore? Disability and Rehabilitation. 2014; 36(8):691-704. [DOI:10.3109/09638288.2013.804597] [PMID]
- Sekhon JK, Oates J, Kneebone I, Rose M. Counselling training for speech-language therapists working with people affected by post-stroke aphasia: A systematic review. International Journal of Language & Communication. 2019; 54(3):321-46. [DOI:10.1111/1460-6984.12455] [PMID]
- Verna A, Davidson B, Rose T. Speech-language pathology services for people with aphasia: A survey of current practice in Australia. International Journal of Speech-Language Pathology. 2009; 11(3):191-205. [DOI:10.1080/17549500902726059]
- Chow C. Barriers and facilitators that affect access to an outpatient speech-language therapy aphasia clinic [master thesis]. Christchurch: University of Canterbury; 2015. [Link]
- Nilipour R. Trends in speech and language rehabilitation in Iran. International Railway Journal. 2003; 1(1):25-8. [Link]
- Azizi-Zeinalhajlou A, Imani A, Dastgiri S. [Population aging and burden of diseases (a review) (Persian)]. Tasvīr-i salāmat. 2015; 6:54-61. [Link]
- Ellis C, Urban S. Age and aphasia: A review of presence, type, recovery and clinical outcomes. Topics in Stroke Rehabilitation. 2016; 23(6):430-9. [DOI:10.1080/10749357.2016.1150412] [PMID]
- Code C, Heron C. Services for aphasia, other acquired adult neurogenic communication and swallowing disorders in the United Kingdom, 2000. Disability and Rehabilitation. 2003; 25(21):1231-7. [DOI:10.1080/09638280310001599961] [PMID]
- Kamyabi Azar S, Molanorouzi K, Vakili S, Charbashlu H. Fundamentals of quantitative, qualitative and integrated content analysis methodology: examining approaches, strengths, weaknesses and the role of each in the process of preparing educational content. Journal of Early Childhood Health and Education. 2025; 5(4):243-59. [Link]
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qualitative Health Research. 2005; 15(9):1277-88. [DOI:10.1177/1049732305276687] [PMID]
- Kotronoulas G, Miguel S, Dowling M, Fernández-Ortega P, Colomer-Lahiguera S, Bağçivan G, et al. An overview of the fundamentals of data management, analysis, and interpretation in quantitative research. Seminars in Oncology Nursing Journal. 2023; 39(2):151398. [DOI: 10.1016/j.soncn.2023.151398] [PMID]
- Rambod M. Interviewing: The most common methods of data collection in qualitative studies. Sadra Medical Journal. 2018; 6(4):303-16. [Link]
- Jalali R. Qualitative research sampling. Journal of Qualitative Research in Health Sciences. 2013; 1(4):310-20. [Link]
- Shahbazi Sh, Fathizadeh N, Taleghani F. [The process of illegal abortion: A qualitative study (Persian)]. Payesh. 2011; 10(2):183-95. [Link]
- Burnard P. A method of analysing interview transcripts in qualitative research. Nurse Education Today. 1991; 11(6):461-6. [DOI:10.1016/0260-6917(91)90009-Y] [PMID]
- Guba EG, Lincoln YS. Competing paradigms in qualitative research. Handbook of qualitative research. Thousand Oaks: Sage Publications; 1994.
- Abbaszadeh M. Validity and reliability in qualitative researches. Journal of Applied Sociology. 2012; 23(145):19-34. [Link]
- Hersh D, Worrall L, Howe T, Sherratt S, Davidson B. SMARTER goal setting in aphasia rehabilitation. Aphasiology. 2012; 26(2):220-33. [DOI:10.1080/02687038.2011.640392]
- Le Dorze G, Salois-Bellerose É, Alepins M, Croteau C, Hallé MC. A description of the personal and environmental determinants of participation several years post-stroke according to the views of people who have aphasia. Aphasiology. 2014; 28(4):421-39. [DOI:10.1080/02687038.2013.869305]
- Howe TJ, Worrall LE, Hickson LM. Interviews with people with aphasia: Environmental factors that influence their community participation. Aphasiology. 2008; 22(10):1092-120. [DOI:10.1080/02687030701640941]
- Baylor C, Burns M, Eadie T, Britton D, Yorkston K. A qualitative study of interference with communicative participation across communication disorders in adults. American Journal of Speech-Language Pathology. 2011; 20(4):269-87 [DOI:10.1044/1058-0360(2011/10-0084)] [PMID]
- Kong AP-H. Family members’ report on speech-language pathology and community services for persons with aphasia in Hong Kong. Disability and Rehabilitation. 2011; 33(25-26):2633-45. [DOI:10.3109/09638288.2011.579220] [PMID]
- Caughlin S, Mehta S, Corriveau H, Eng JJ, Eskes G, Kairy D, et al. Implementing telerehabilitation after stroke: Lessons learned from Canadian trials. Telemedicine and e-Health. 2020; 26(6):710-9. [DOI:10.1089/tmj.2019.0097] [PMID]
- Parr S, Byng S, Gilpin S, Ireland C. Talking about aphasia. Buckingham. Walton Hall: Open University Press; 1997. [Link]
- Hinckley JJ, Hasselkus A, Ganzfried E. What people living with aphasia think about the availability of aphasia resources. American Journal of Speech-Language Pathology. 2013. [DOI:10.1044/1058-0360(2013/12-0090)]
- Hersh D. How do people with aphasia view their discharge from therapy? Aphasiology. 2009; 23(3):331-50. [DOI:10.1080/02687030701764220]
Article type: Original Research Articles |
Subject:
Speech therapy
Received: 2025/04/30 | Accepted: 2025/10/1 | Published: 2026/03/1
Received: 2025/04/30 | Accepted: 2025/10/1 | Published: 2026/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
