
988368
Fri, Jun 19, 2026

Volume 24, Issue 1 (March 2026)
Iranian Rehabilitation Journal 2026, 24(1): 113-122 |
Back to browse issues page



Ethics code: IR.USWR.REC.1401.002
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Kamali M, Arabkari Z, Esmaeil M J. Navigating Sexual Life After Spinal Cord Injury: A Qualitative Exploration of Challenges, Spousal Dynamics, and Societal Barriers. Iranian Rehabilitation Journal 2026; 24 (1) :113-122
URL: http://irj.uswr.ac.ir/article-1-2565-en.html
URL: http://irj.uswr.ac.ir/article-1-2565-en.html



1- Department of Rehabilitation Management, Rehabilitation Research Center, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Mental Health, School of Behavioral Sciences and Mental Health, Tehran Institute of Psychiatry, Iran University of Medical Sciences, Tehran, Iran.
3- Institute for Sciences and Technology Studies, Shahid Beheshti University, Tehran, Iran.
2- Department of Mental Health, School of Behavioral Sciences and Mental Health, Tehran Institute of Psychiatry, Iran University of Medical Sciences, Tehran, Iran.
3- Institute for Sciences and Technology Studies, Shahid Beheshti University, Tehran, Iran.
Keywords: Spinal cord injury (SCI), Sexuality, Qualitative study, Partner relationships, Cultural barriers
Full-Text [PDF 567 kb]
(111 Downloads)
| Abstract (HTML) (1317 Views)
Full-Text: (11 Views)
Introduction
Spinal cord injury (SCI) is a life-altering condition that brings significant changes to physiological, psychological, and social dimensions of life. Among the most impacted areas is sexual function, which is often overlooked in clinical and rehabilitation contexts despite being vital to quality of life (QoL) [1]. Individuals with SCI frequently experience disturbances in their personal relationships, body image, self-esteem, and sexual identity [2, 3]. Common sexual problems include decreased libido, anorgasmia, genital numbness, erectile and ejaculatory dysfunction in men, and inadequate vaginal lubrication and pain during intercourse in women [4, 5]. These challenges are further complicated by social and emotional consequences, such as a perceived loss of masculinity or femininity, fear of rejection, and dissatisfaction in partner relationships [6]. As a result, emotional intimacy often replaces physical intercourse as the primary form of connection in post-SCI relationships [7].
A widespread misconception persists that individuals with physical disabilities are asexual or uninterested in intimate relationships [8, 9]. This stereotyped belief reduces opportunities for romantic connection and hinders social reintegration [10, 11]. In Iran, discussions about sexuality remain highly restricted by cultural taboos and religious conservatism, especially following the Islamic Revolution [12, 13]. Social expectations discourage individuals, particularly women and those with disabilities, from openly discussing or seeking help for sexual issues [14, 15]. Consequently, many people with SCI are deprived of essential sexual health education, psychological support, and therapeutic options [16, 17].
While some studies have examined the life challenges of individuals with SCI, including emotional adjustment, financial stress, and reintegration [18, 19], few have focused directly on sexual health. Even fewer studies have addressed these challenges from both the patient and spousal perspectives in Middle Eastern societies [20]. Given the deeply personal and socially sensitive nature of sexual health—combined with a lack of attention in current rehabilitation programs—this study aims to explore the sexual life challenges of individuals with SCI and their spouses through a qualitative lens [21]. The research intends to inform culturally sensitive interventions, policy development, and inclusive rehabilitation strategies that can improve sexual well-being and overall QoL for this population [17, 22]. Each conducted study has examined a specific aspect of life challenges or sexual intercourse challenges experienced by individuals with SCI following the injury. However, no study has specifically focused on the sex life of individuals with SCI and their spouses. The current study, using a qualitative approach, aims to investigate the sex life challenges of individuals with SCI and their spouses.
Materials and Methods
Study design
This qualitative study conducted a conventional content analysis approach to explore the sexual life challenges of individuals with SCI and their spouses in Tehran City, Iran. The study was conducted from June 2022 to May 2024, focusing on understanding experiences within a cultural context where discussions around sexuality are often taboo.
Setting, samples, and recruitments
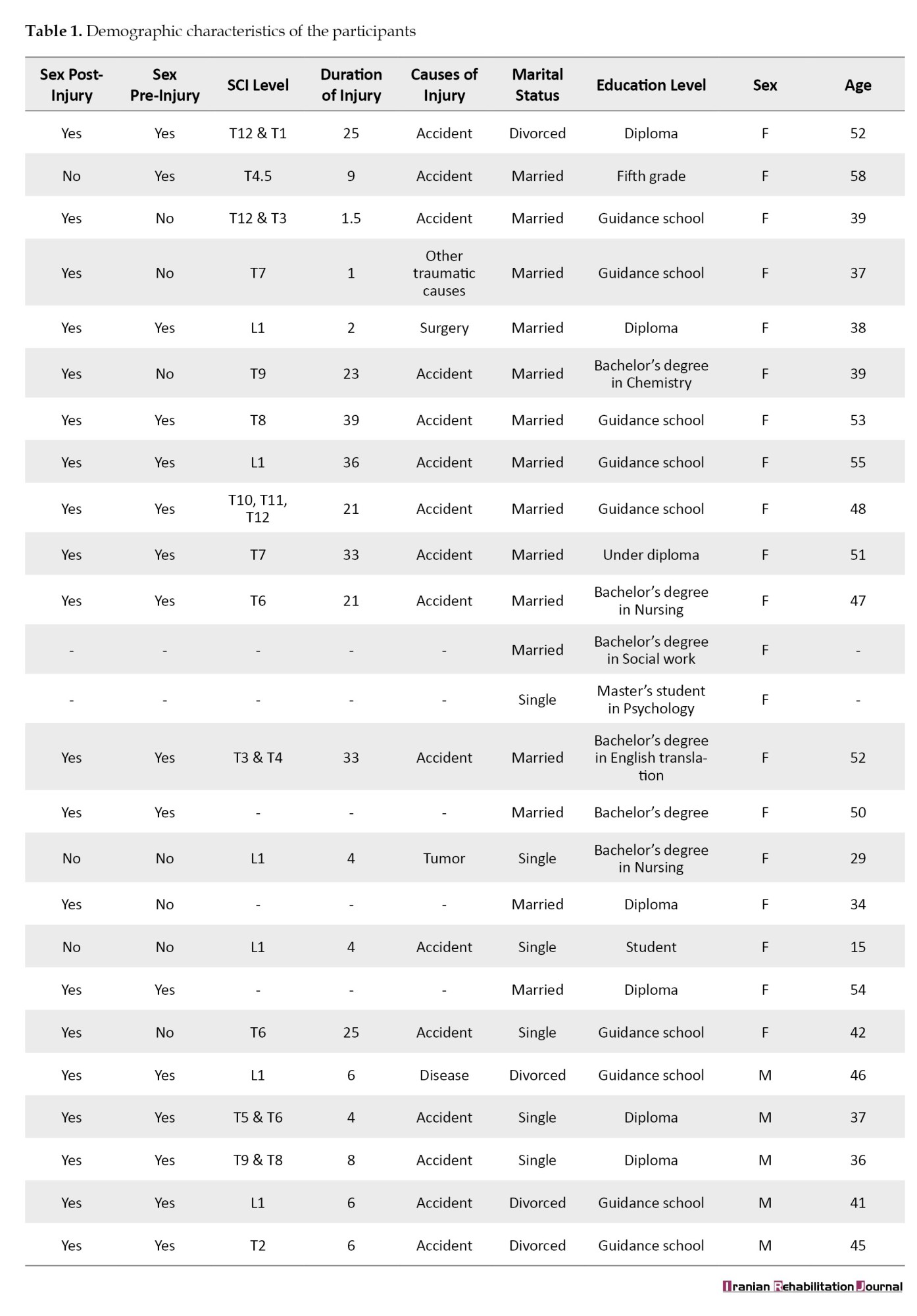
The study recruited 25 participants, including 15 women and 5 men with SCI, 3 spouses without disabilities, and 2 social workers. Participants were selected using purposive and snowball sampling, with an emphasis on maximum variation in gender, age, education, marital status, socioeconomic background, and level of SCI. The inclusion criteria required participants to be willing to share personal experiences related to sexual life after SCI, be married or single with experience in sexual activity or sexual relationships, and have physical-motor disabilities. The exclusion criteria included having other disabilities or unwillingness to participate. Participants’ information is shown in Table 1.
Due to the sensitivity of the topic, snowball sampling was encouraged, allowing participants to refer others who might be interested and eligible. Participants’ demographic data were recorded, and the principle of data saturation was used to determine the final sample size.
Data collection
Data were collected through semi-structured, in-depth interviews, each lasting 40–60 minutes. Interviews were conducted face-to-face in private settings to ensure confidentiality and comfort. Open-ended questions were designed to elicit detailed narratives, such as:
“Describe your sex life after SCI.”
“What are your main difficulties before, during, and after sexual intercourse?”
“How do you define sexual health after SCI?”
Initial interviews began with general questions to build trust, followed by more personal topics once rapport was established. Ethical protocols were strictly observed, including informed written consent, anonymity, the right to withdraw at any stage, and the use of codes instead of names. Audio recordings were deleted after transcription and data analysis.
Data analysis
All interviews were audio recorded, transcribed verbatim, and analyzed using the Lundman and Graneheim (2004) method. The analysis involved identifying meaning units, coding them, grouping similar codes into subcategories, and then organizing them into broader categories. Ultimately, a main theme was identified that encapsulated the participants’ experiences.
Rigor and trustworthiness
To ensure analytical rigor, coding was conducted manually by the first author and peer-reviewed by co-researchers. Discussions were held regularly to resolve discrepancies and refine categories. The credibility, dependability, confirmability, and transferability of the findings were ensured through various strategies as follows:
Credibility: Prolonged engagement, member checking, repeated reading of transcripts, and peer debriefing, dependability: verification of interpretations with participants after each interview, confirmability: Maintaining an audit trail of coding steps and analysis, and transferability: Review of findings with individuals who met inclusion criteria but did not participate in interviews.
A neutral researcher with expertise in qualitative research reviewed the coding and offered feedback to validate findings.
Results
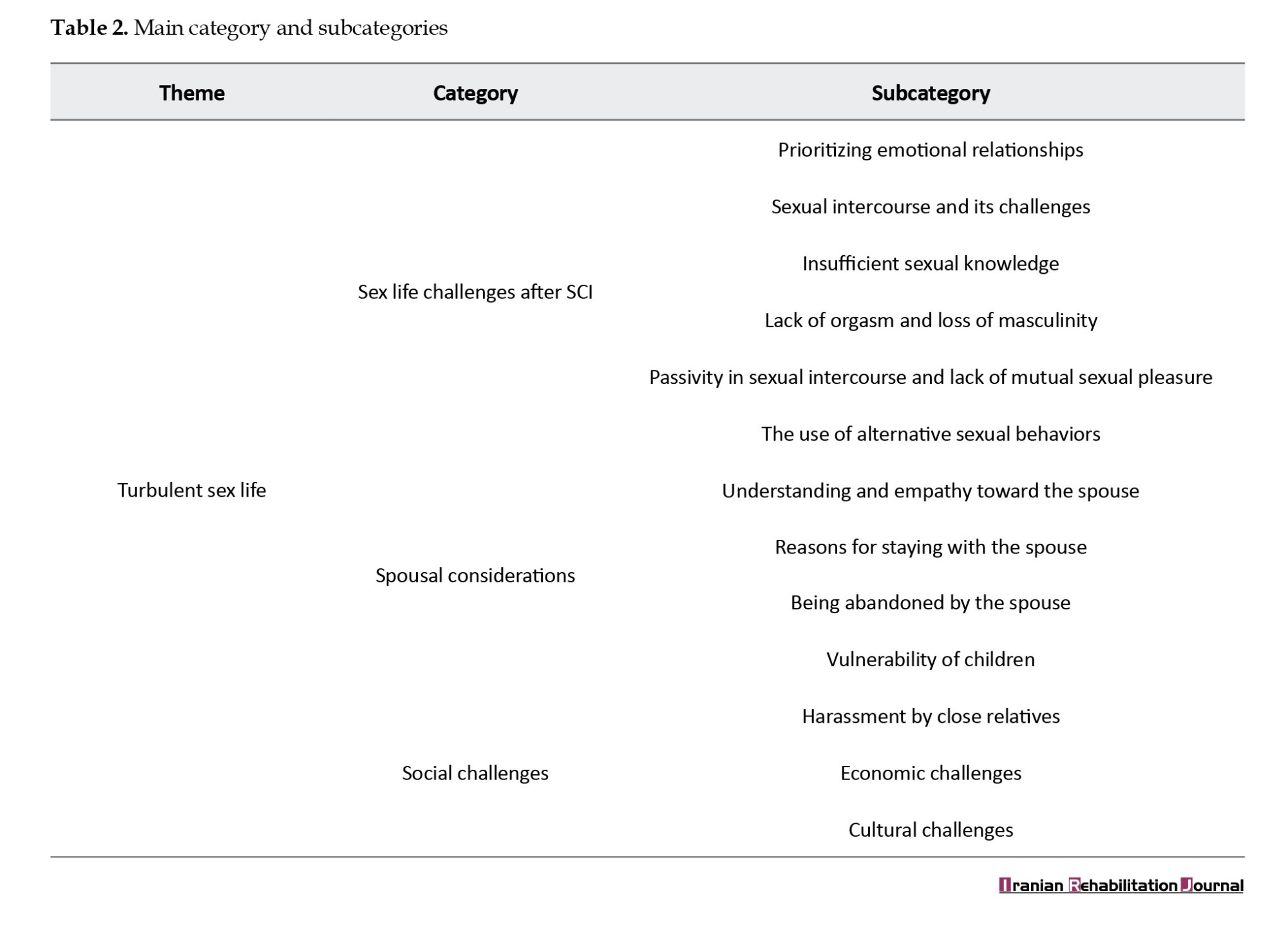
This study explored the sexual life challenges experienced by individuals with SCI and their spouses. Analysis of 25 interviews yielded one overarching theme— “turbulent sex life”—composed of 3 main categories and 13 subcategories. The analysis of participants’ views and opinions culminated in the identification of 1379 primary codes. The main category and subcategories are presented in Table 2.
Theme: Turbulent sex life
SCI was found to significantly disrupt the sexual lives of participants, both physically and emotionally. The findings indicated that sexuality after SCI is influenced by physiological limitations, psychological vulnerability, spousal dynamics, cultural expectations, and social stigma. Many participants had shifted their focus from physical intercourse to emotional intimacy, often due to functional impairments or fear of rejection. The theme encompasses 3 major categories: 1) sex life challenges after SCI, 2) spousal considerations, and 3) social challenges.
Category 1: Sex life challenges after SCI
Physical disability following SCI causes anxiety, stress, fear of abandonment, inability to perform daily and personal activities, dependence on a spouse, and decreased self-esteem. This category included 6 subcategories that revealed the personal and relational difficulties participants faced in their post-injury sex lives.
Subcategory 1: Prioritizing emotional relationships
Due to erectile dysfunction, genital numbness, or lack of orgasm, many individuals with SCI derived sexual satisfaction from emotional connections, such as affectionate words, caresses, and non-penetrative touch. While this shift provided psychological relief, it often created a disconnect with spouses who still prioritized intercourse. Participant 10 stated, “I do not have that sense of orgasm, but when my spouse kisses me and gives me love, I am satisfied inside.”
Subcategory 2: Sexual intercourse and its challenges
Participants identified a range of obstacles before, during, and after sex. These included preparing for hygiene (e.g. bowel evacuation, catheterization), stress and anxiety about urinary or fecal incontinence during intercourse, difficulty in changing sexual positions due to paralysis or pain, erectile dysfunction or lack of ejaculation in men, lack of vaginal lubrication and genital sensation in women, shame and embarrassment. These physical and logistical hurdles contributed to avoidance of sex, diminished frequency, and a sense of frustration.
Subcategory 3: Insufficient sexual knowledge
Many participants lacked knowledge about sexual alternatives, adaptive techniques, and assistive devices (e.g. sex toys, lubricants, medications). They also noted an absence of educational resources provided by hospitals or rehabilitation centers. This lack of information contributed to misconceptions, performance anxiety, and miscommunication between partners. Participant No. 11 expressed, “I had no intercourse with my spouse for one year, not in the hospital, not at home. I could not displace. I used to cooperate with my spouse, but now most of the activities during intercourse are on my spouse’s shoulder.”
Subcategory 4: Lack of orgasm and loss of masculinity
Men often associated their inability to perform sexually with a loss of masculinity. In women, loss of genital sensation led to concealment of sexual dysfunction. One participant explained pretending to have an orgasm so as not to disappoint her husband. Another noted, “My husband left me after realizing I couldn’t feel anything during intercourse.”
Subcategory 5: Passivity in sexual intercourse and lack of mutual sexual pleasure
Due to physical limitations, individuals with SCI reported passivity during intercourse. Spouses, often taking on a more active role, described this imbalance as physically demanding and emotionally dissatisfying. Participant No. 17 mentioned, “Our intercourse has reversed, and I do most of the work. This means that I have to be on top, and as a result, I experience less satisfaction. Because my husband is heavy and I have to move him, it annoys me very much, and I have got a backache. Because of these difficulties, I prefer not to have sex.”
Subcategory 6: The use of alternative sexual behaviors
To cope with sexual dysfunction, participants reported using non-penetrative methods, such as kissing, caressing, oral sex, and stimulation of sensitive areas (e.g. breasts, ears, neck). Some men also used viagra, although side effects were commonly reported. A few participants mentioned resorting to temporary or paid sexual relationships, often in secrecy due to social judgment. Participant No. 20 stated, “Kissing and touching different parts of the body are very pleasurable. When my boyfriend touches my breasts, it feels great; that is the sensitive spot. When he touches my neck or nibbles my ear, I also feel good and enjoy it very much”.
Category 2: spousal considerations
Individuals with SCI strive to maintain their lives and their spouse’s commitment to the relationship. They pay attention to their appearance, body image, physical fitness, and a positive response to their spouse’s request for sexual intercourse. This category explored the role of spouses and the impact of SCI on marital dynamics and family relationships.
Subcategory 1: Understanding and empathy toward the spouse
Individuals with SCI expressed a desire to compensate for their physical limitations by pleasing their spouses emotionally, dressing attractively, and maintaining a positive demeanor. Some even relieved their spouses from caregiving tasks (e.g. changing diapers) to preserve dignity. This mutual empathy was key in sustaining intimacy. Participant No. 7 said, “I think we have to compensate for this psychologically. We have to do many things for them, psychologically and mentally; jokes, laughter, and revealing clothes often. To be honest, I myself put on one outfit in the morning, put on another at noon, and another in the afternoon, and I change my clothes.”
Subcategory 2: Reasons for staying with the spouse
Commitment, emotional attachment, religious beliefs, and shared history were commonly cited reasons for spouses choosing to stay. For some, fulfilling marital duties and spiritual vows were powerful motivators. Participant No. 17 stated, “We got married when I was 19. We grew up together, we know each other’s temperament, and we were always together. I tell him to go and live his life, but he says, ‘This is not in my character.’ I made a deal with Imam Hussein; also, his religiosity has greatly influenced his commitment to our life and staying in this situation.”
Subcategory 3: Being abandoned by the spouse
Some individuals reported abandonment shortly after their injury. Reasons included the lack of sexual satisfaction, the spouse’s physical exhaustion, economic burdens, and altered physical appearance. Spouses who remained often struggled with unmet needs and the guilt of contemplating divorce. Participant No. 23 stated, “Fifty percent of marriage is sexual pleasure, but when you tell someone ‘I cannot have an erection, or I cannot satisfy you normally,’ well, she may be annoyed, and she will not accept it. For this reason, my wife filed for divorce six months after the injury.”
Subcategory 4: Vulnerability of children
Participants with children described the emotional and social toll on their offspring. Some children faced stigma from peers or rejection by suitors due to having a parent with SCI. Others were exposed to family conflicts or parental infidelity, which affected their psychological health. Participant No. 12 stated, “My children know their father is involved with other women, but what can they do? They are upset.”
Category 3: Social challenges
The final category revealed how societal norms, financial limitations, and familial interference further complicated the sexual and relational lives of individuals with SCI. This category consisted of 3 subcategories.
Subcategory 1: Harassment by close relatives
Several participants, particularly women, reported receiving inappropriate sexual propositions from friends, acquaintances, or even in-laws after their partner’s injury. These intrusions were deeply unsettling and often exacerbated feelings of vulnerability. In some cases, family members encouraged divorce or questioned the viability of the marriage. Participant No. 17 stated, “I love my life. This is what happened to my husband, and I do not want to leave my life. As soon as friends and relatives in the hospital environment, even strangers, see my life and find out about my husband’s problem, they offer me sexual intercourse. They say, ‘Why did you stay? Leave him and go to your life. He may not improve anymore.”
Subcategory 2: Economic challenges
The high cost of medications, personal hygiene supplies, and caregiving imposed severe financial burdens on families. Many participants were renters or relied on external support. As financial stress increased, couples found themselves deprioritizing sexual intimacy. Participant No. 19 said, “I have cervical SCI, and my husband is healthy. We should pay a large amount of costs for care and hygiene equipment; I also have a kid, and we are renters. My husband is confused here. When he has no money to take care of me, he has to take care of me; he must go to work or not to go to work; he has to hire someone to take care of me, but he has no money. I mean, life is messy and turbulent. How can he be interested in sexual intercourse!”
Subcategory 3: Cultural challenges
Participants consistently mentioned that Iranian cultural norms viewed individuals with disabilities as asexual or unworthy of romantic relationships. Temporary marriages or relationships outside marriage were often hidden due to fear of judgment. This cultural taboo led to social isolation, particularly for single women with SCI. Participant No. 12 stated, “I have had several clients, both male and female, who were worried about being judged. Some were forced to live together, while others were financially well-off, and each lived in a separate house. The healthy spouses were involved in sexual intercourse with their boyfriends or girlfriends.”
Discussion
This study aimed to explore the sexual life challenges experienced by individuals with SCI and their spouses within a culturally conservative Iranian context. The findings revealed that SCI has far-reaching consequences on individuals’ physical, emotional, relational, and social well-being—particularly their sexual and intimate lives. These results align with previous research highlighting that sexual health is one of the most significantly disrupted domains after SCI and yet remains one of the most neglected in rehabilitation planning [1, 3].
One of the main findings was that emotional intimacy often replaced physical intercourse in individuals with SCI. Due to genital insensitivity, erectile and ejaculatory dysfunction, or pain, both men and women with SCI reported shifting their focus toward emotional satisfaction and affectionate behaviors such as touching, hugging, and kissing [9]. This echoes findings from Soler et al., who noted that men with SCI often found deeper sexual satisfaction in emotional closeness rather than penetration-based intimacy [23]. Similarly, women prioritized affection over orgasm, using emotional connection to compensate for physical limitations [24].
However, this shift was not always mutually fulfilling. Many spouses—especially healthy partners—continued to value traditional intercourse, which led to frustration, emotional fatigue, and sometimes relationship breakdowns [5]. Female spouses often experienced physical strain during intercourse due to their partner’s passivity, while male partners struggled with sexual dissatisfaction caused by their wives’ limited engagement [25]. Participants also reported concealing their sexual dysfunction, particularly women pretending to have orgasms to preserve partner satisfaction [26]. This behavior reflects patterns documented by Previnaire et al. and Khazaeipour et al., in which individuals with SCI often “perform” sexual responses to avoid rejection or marital conflict [27].
A significant barrier was the lack of sexual education and professional support. Many participants expressed minimal knowledge of alternative techniques, sexual aids, or available medications. They had not received guidance from health professionals in hospitals or rehabilitation centers [8, 9]. This finding is consistent with international studies that show inadequate training among healthcare providers negatively affects sexual rehabilitation [8, 28]. The study also revealed the impact of cultural and religious norms. In Iran, sexual matters—especially for women or people with disabilities—are surrounded by taboo, limiting access to information or support [12, 15]. Some participants entered secret temporary marriages or concealed intimate relationships due to societal judgment, leading to stress and isolation [9, 10]. Economic pressures added further complexity. Families faced high costs for medications, hygiene, and care, often leading to neglect of sexual and emotional intimacy [22, 29]. These results align with research showing that financial strain lowers life satisfaction and disrupts sexual well-being [30].
The limitations of this research included extremely difficult access to participants, their reluctance to cooperate and discuss sexual intercourse and problems, and the weak cooperation of center officials due to the sensitivity of the topic. It can assist policymakers and legislators in the fields of rehabilitation and health, as well as sexual health professionals, in developing practical and educational strategies for this target group. By conducting workshops and culture building among officials and individuals with SCI, steps can be taken to improve their sex life and QoL. Additionally, by developing family-centered programs aimed at enhancing interpersonal relationships and reducing children’s vulnerability, policymakers can contribute to the stability and understanding of individuals with SCI. It is recommended that studies be conducted on the vulnerability of children of individuals with SCI, as well as the sexual challenges faced by spouses of these individuals.
Conclusion
Collectively, the findings reveal that sexual life after SCI is not merely a private issue but a complex interplay of physical, emotional, relational, and social factors. The need for culturally sensitive counseling, sexual education, and inclusive rehabilitation policies is urgent. Furthermore, attention must be paid to the emotional health of spouses and children who also bear the psychological weight of injury-related changes. These insights can guide interventions aimed at enhancing QoL and preserving intimacy for individuals with SCI and their families.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1401.002). Participants were fully informed of the study’s objectives, and their privacy and confidentiality were protected throughout the process.
Funding
The project was financially supported by the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Authors' contributions
Conceptualization and methodology: Zoleikha Arabkari and Mohammad Kamali; Data collection, analysis and interpretation: Zoleikha Arabkari; Writing the original draft: Zoleikha Arabkaril and Mohammad Javad Esmaili; Review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Iranian Disabled Association, the Spinal Injury Association, and all participants who collaborated in this research.
Spinal cord injury (SCI) is a life-altering condition that brings significant changes to physiological, psychological, and social dimensions of life. Among the most impacted areas is sexual function, which is often overlooked in clinical and rehabilitation contexts despite being vital to quality of life (QoL) [1]. Individuals with SCI frequently experience disturbances in their personal relationships, body image, self-esteem, and sexual identity [2, 3]. Common sexual problems include decreased libido, anorgasmia, genital numbness, erectile and ejaculatory dysfunction in men, and inadequate vaginal lubrication and pain during intercourse in women [4, 5]. These challenges are further complicated by social and emotional consequences, such as a perceived loss of masculinity or femininity, fear of rejection, and dissatisfaction in partner relationships [6]. As a result, emotional intimacy often replaces physical intercourse as the primary form of connection in post-SCI relationships [7].
A widespread misconception persists that individuals with physical disabilities are asexual or uninterested in intimate relationships [8, 9]. This stereotyped belief reduces opportunities for romantic connection and hinders social reintegration [10, 11]. In Iran, discussions about sexuality remain highly restricted by cultural taboos and religious conservatism, especially following the Islamic Revolution [12, 13]. Social expectations discourage individuals, particularly women and those with disabilities, from openly discussing or seeking help for sexual issues [14, 15]. Consequently, many people with SCI are deprived of essential sexual health education, psychological support, and therapeutic options [16, 17].
While some studies have examined the life challenges of individuals with SCI, including emotional adjustment, financial stress, and reintegration [18, 19], few have focused directly on sexual health. Even fewer studies have addressed these challenges from both the patient and spousal perspectives in Middle Eastern societies [20]. Given the deeply personal and socially sensitive nature of sexual health—combined with a lack of attention in current rehabilitation programs—this study aims to explore the sexual life challenges of individuals with SCI and their spouses through a qualitative lens [21]. The research intends to inform culturally sensitive interventions, policy development, and inclusive rehabilitation strategies that can improve sexual well-being and overall QoL for this population [17, 22]. Each conducted study has examined a specific aspect of life challenges or sexual intercourse challenges experienced by individuals with SCI following the injury. However, no study has specifically focused on the sex life of individuals with SCI and their spouses. The current study, using a qualitative approach, aims to investigate the sex life challenges of individuals with SCI and their spouses.
Materials and Methods
Study design
This qualitative study conducted a conventional content analysis approach to explore the sexual life challenges of individuals with SCI and their spouses in Tehran City, Iran. The study was conducted from June 2022 to May 2024, focusing on understanding experiences within a cultural context where discussions around sexuality are often taboo.
Setting, samples, and recruitments
The study recruited 25 participants, including 15 women and 5 men with SCI, 3 spouses without disabilities, and 2 social workers. Participants were selected using purposive and snowball sampling, with an emphasis on maximum variation in gender, age, education, marital status, socioeconomic background, and level of SCI. The inclusion criteria required participants to be willing to share personal experiences related to sexual life after SCI, be married or single with experience in sexual activity or sexual relationships, and have physical-motor disabilities. The exclusion criteria included having other disabilities or unwillingness to participate. Participants’ information is shown in Table 1.
Due to the sensitivity of the topic, snowball sampling was encouraged, allowing participants to refer others who might be interested and eligible. Participants’ demographic data were recorded, and the principle of data saturation was used to determine the final sample size.
Data collection
Data were collected through semi-structured, in-depth interviews, each lasting 40–60 minutes. Interviews were conducted face-to-face in private settings to ensure confidentiality and comfort. Open-ended questions were designed to elicit detailed narratives, such as:
“Describe your sex life after SCI.”
“What are your main difficulties before, during, and after sexual intercourse?”
“How do you define sexual health after SCI?”
Initial interviews began with general questions to build trust, followed by more personal topics once rapport was established. Ethical protocols were strictly observed, including informed written consent, anonymity, the right to withdraw at any stage, and the use of codes instead of names. Audio recordings were deleted after transcription and data analysis.
Data analysis
All interviews were audio recorded, transcribed verbatim, and analyzed using the Lundman and Graneheim (2004) method. The analysis involved identifying meaning units, coding them, grouping similar codes into subcategories, and then organizing them into broader categories. Ultimately, a main theme was identified that encapsulated the participants’ experiences.
Rigor and trustworthiness
To ensure analytical rigor, coding was conducted manually by the first author and peer-reviewed by co-researchers. Discussions were held regularly to resolve discrepancies and refine categories. The credibility, dependability, confirmability, and transferability of the findings were ensured through various strategies as follows:
Credibility: Prolonged engagement, member checking, repeated reading of transcripts, and peer debriefing, dependability: verification of interpretations with participants after each interview, confirmability: Maintaining an audit trail of coding steps and analysis, and transferability: Review of findings with individuals who met inclusion criteria but did not participate in interviews.
A neutral researcher with expertise in qualitative research reviewed the coding and offered feedback to validate findings.
Results
This study explored the sexual life challenges experienced by individuals with SCI and their spouses. Analysis of 25 interviews yielded one overarching theme— “turbulent sex life”—composed of 3 main categories and 13 subcategories. The analysis of participants’ views and opinions culminated in the identification of 1379 primary codes. The main category and subcategories are presented in Table 2.
Theme: Turbulent sex life
SCI was found to significantly disrupt the sexual lives of participants, both physically and emotionally. The findings indicated that sexuality after SCI is influenced by physiological limitations, psychological vulnerability, spousal dynamics, cultural expectations, and social stigma. Many participants had shifted their focus from physical intercourse to emotional intimacy, often due to functional impairments or fear of rejection. The theme encompasses 3 major categories: 1) sex life challenges after SCI, 2) spousal considerations, and 3) social challenges.
Category 1: Sex life challenges after SCI
Physical disability following SCI causes anxiety, stress, fear of abandonment, inability to perform daily and personal activities, dependence on a spouse, and decreased self-esteem. This category included 6 subcategories that revealed the personal and relational difficulties participants faced in their post-injury sex lives.
Subcategory 1: Prioritizing emotional relationships
Due to erectile dysfunction, genital numbness, or lack of orgasm, many individuals with SCI derived sexual satisfaction from emotional connections, such as affectionate words, caresses, and non-penetrative touch. While this shift provided psychological relief, it often created a disconnect with spouses who still prioritized intercourse. Participant 10 stated, “I do not have that sense of orgasm, but when my spouse kisses me and gives me love, I am satisfied inside.”
Subcategory 2: Sexual intercourse and its challenges
Participants identified a range of obstacles before, during, and after sex. These included preparing for hygiene (e.g. bowel evacuation, catheterization), stress and anxiety about urinary or fecal incontinence during intercourse, difficulty in changing sexual positions due to paralysis or pain, erectile dysfunction or lack of ejaculation in men, lack of vaginal lubrication and genital sensation in women, shame and embarrassment. These physical and logistical hurdles contributed to avoidance of sex, diminished frequency, and a sense of frustration.
Subcategory 3: Insufficient sexual knowledge
Many participants lacked knowledge about sexual alternatives, adaptive techniques, and assistive devices (e.g. sex toys, lubricants, medications). They also noted an absence of educational resources provided by hospitals or rehabilitation centers. This lack of information contributed to misconceptions, performance anxiety, and miscommunication between partners. Participant No. 11 expressed, “I had no intercourse with my spouse for one year, not in the hospital, not at home. I could not displace. I used to cooperate with my spouse, but now most of the activities during intercourse are on my spouse’s shoulder.”
Subcategory 4: Lack of orgasm and loss of masculinity
Men often associated their inability to perform sexually with a loss of masculinity. In women, loss of genital sensation led to concealment of sexual dysfunction. One participant explained pretending to have an orgasm so as not to disappoint her husband. Another noted, “My husband left me after realizing I couldn’t feel anything during intercourse.”
Subcategory 5: Passivity in sexual intercourse and lack of mutual sexual pleasure
Due to physical limitations, individuals with SCI reported passivity during intercourse. Spouses, often taking on a more active role, described this imbalance as physically demanding and emotionally dissatisfying. Participant No. 17 mentioned, “Our intercourse has reversed, and I do most of the work. This means that I have to be on top, and as a result, I experience less satisfaction. Because my husband is heavy and I have to move him, it annoys me very much, and I have got a backache. Because of these difficulties, I prefer not to have sex.”
Subcategory 6: The use of alternative sexual behaviors
To cope with sexual dysfunction, participants reported using non-penetrative methods, such as kissing, caressing, oral sex, and stimulation of sensitive areas (e.g. breasts, ears, neck). Some men also used viagra, although side effects were commonly reported. A few participants mentioned resorting to temporary or paid sexual relationships, often in secrecy due to social judgment. Participant No. 20 stated, “Kissing and touching different parts of the body are very pleasurable. When my boyfriend touches my breasts, it feels great; that is the sensitive spot. When he touches my neck or nibbles my ear, I also feel good and enjoy it very much”.
Category 2: spousal considerations
Individuals with SCI strive to maintain their lives and their spouse’s commitment to the relationship. They pay attention to their appearance, body image, physical fitness, and a positive response to their spouse’s request for sexual intercourse. This category explored the role of spouses and the impact of SCI on marital dynamics and family relationships.
Subcategory 1: Understanding and empathy toward the spouse
Individuals with SCI expressed a desire to compensate for their physical limitations by pleasing their spouses emotionally, dressing attractively, and maintaining a positive demeanor. Some even relieved their spouses from caregiving tasks (e.g. changing diapers) to preserve dignity. This mutual empathy was key in sustaining intimacy. Participant No. 7 said, “I think we have to compensate for this psychologically. We have to do many things for them, psychologically and mentally; jokes, laughter, and revealing clothes often. To be honest, I myself put on one outfit in the morning, put on another at noon, and another in the afternoon, and I change my clothes.”
Subcategory 2: Reasons for staying with the spouse
Commitment, emotional attachment, religious beliefs, and shared history were commonly cited reasons for spouses choosing to stay. For some, fulfilling marital duties and spiritual vows were powerful motivators. Participant No. 17 stated, “We got married when I was 19. We grew up together, we know each other’s temperament, and we were always together. I tell him to go and live his life, but he says, ‘This is not in my character.’ I made a deal with Imam Hussein; also, his religiosity has greatly influenced his commitment to our life and staying in this situation.”
Subcategory 3: Being abandoned by the spouse
Some individuals reported abandonment shortly after their injury. Reasons included the lack of sexual satisfaction, the spouse’s physical exhaustion, economic burdens, and altered physical appearance. Spouses who remained often struggled with unmet needs and the guilt of contemplating divorce. Participant No. 23 stated, “Fifty percent of marriage is sexual pleasure, but when you tell someone ‘I cannot have an erection, or I cannot satisfy you normally,’ well, she may be annoyed, and she will not accept it. For this reason, my wife filed for divorce six months after the injury.”
Subcategory 4: Vulnerability of children
Participants with children described the emotional and social toll on their offspring. Some children faced stigma from peers or rejection by suitors due to having a parent with SCI. Others were exposed to family conflicts or parental infidelity, which affected their psychological health. Participant No. 12 stated, “My children know their father is involved with other women, but what can they do? They are upset.”
Category 3: Social challenges
The final category revealed how societal norms, financial limitations, and familial interference further complicated the sexual and relational lives of individuals with SCI. This category consisted of 3 subcategories.
Subcategory 1: Harassment by close relatives
Several participants, particularly women, reported receiving inappropriate sexual propositions from friends, acquaintances, or even in-laws after their partner’s injury. These intrusions were deeply unsettling and often exacerbated feelings of vulnerability. In some cases, family members encouraged divorce or questioned the viability of the marriage. Participant No. 17 stated, “I love my life. This is what happened to my husband, and I do not want to leave my life. As soon as friends and relatives in the hospital environment, even strangers, see my life and find out about my husband’s problem, they offer me sexual intercourse. They say, ‘Why did you stay? Leave him and go to your life. He may not improve anymore.”
Subcategory 2: Economic challenges
The high cost of medications, personal hygiene supplies, and caregiving imposed severe financial burdens on families. Many participants were renters or relied on external support. As financial stress increased, couples found themselves deprioritizing sexual intimacy. Participant No. 19 said, “I have cervical SCI, and my husband is healthy. We should pay a large amount of costs for care and hygiene equipment; I also have a kid, and we are renters. My husband is confused here. When he has no money to take care of me, he has to take care of me; he must go to work or not to go to work; he has to hire someone to take care of me, but he has no money. I mean, life is messy and turbulent. How can he be interested in sexual intercourse!”
Subcategory 3: Cultural challenges
Participants consistently mentioned that Iranian cultural norms viewed individuals with disabilities as asexual or unworthy of romantic relationships. Temporary marriages or relationships outside marriage were often hidden due to fear of judgment. This cultural taboo led to social isolation, particularly for single women with SCI. Participant No. 12 stated, “I have had several clients, both male and female, who were worried about being judged. Some were forced to live together, while others were financially well-off, and each lived in a separate house. The healthy spouses were involved in sexual intercourse with their boyfriends or girlfriends.”
Discussion
This study aimed to explore the sexual life challenges experienced by individuals with SCI and their spouses within a culturally conservative Iranian context. The findings revealed that SCI has far-reaching consequences on individuals’ physical, emotional, relational, and social well-being—particularly their sexual and intimate lives. These results align with previous research highlighting that sexual health is one of the most significantly disrupted domains after SCI and yet remains one of the most neglected in rehabilitation planning [1, 3].
One of the main findings was that emotional intimacy often replaced physical intercourse in individuals with SCI. Due to genital insensitivity, erectile and ejaculatory dysfunction, or pain, both men and women with SCI reported shifting their focus toward emotional satisfaction and affectionate behaviors such as touching, hugging, and kissing [9]. This echoes findings from Soler et al., who noted that men with SCI often found deeper sexual satisfaction in emotional closeness rather than penetration-based intimacy [23]. Similarly, women prioritized affection over orgasm, using emotional connection to compensate for physical limitations [24].
However, this shift was not always mutually fulfilling. Many spouses—especially healthy partners—continued to value traditional intercourse, which led to frustration, emotional fatigue, and sometimes relationship breakdowns [5]. Female spouses often experienced physical strain during intercourse due to their partner’s passivity, while male partners struggled with sexual dissatisfaction caused by their wives’ limited engagement [25]. Participants also reported concealing their sexual dysfunction, particularly women pretending to have orgasms to preserve partner satisfaction [26]. This behavior reflects patterns documented by Previnaire et al. and Khazaeipour et al., in which individuals with SCI often “perform” sexual responses to avoid rejection or marital conflict [27].
A significant barrier was the lack of sexual education and professional support. Many participants expressed minimal knowledge of alternative techniques, sexual aids, or available medications. They had not received guidance from health professionals in hospitals or rehabilitation centers [8, 9]. This finding is consistent with international studies that show inadequate training among healthcare providers negatively affects sexual rehabilitation [8, 28]. The study also revealed the impact of cultural and religious norms. In Iran, sexual matters—especially for women or people with disabilities—are surrounded by taboo, limiting access to information or support [12, 15]. Some participants entered secret temporary marriages or concealed intimate relationships due to societal judgment, leading to stress and isolation [9, 10]. Economic pressures added further complexity. Families faced high costs for medications, hygiene, and care, often leading to neglect of sexual and emotional intimacy [22, 29]. These results align with research showing that financial strain lowers life satisfaction and disrupts sexual well-being [30].
The limitations of this research included extremely difficult access to participants, their reluctance to cooperate and discuss sexual intercourse and problems, and the weak cooperation of center officials due to the sensitivity of the topic. It can assist policymakers and legislators in the fields of rehabilitation and health, as well as sexual health professionals, in developing practical and educational strategies for this target group. By conducting workshops and culture building among officials and individuals with SCI, steps can be taken to improve their sex life and QoL. Additionally, by developing family-centered programs aimed at enhancing interpersonal relationships and reducing children’s vulnerability, policymakers can contribute to the stability and understanding of individuals with SCI. It is recommended that studies be conducted on the vulnerability of children of individuals with SCI, as well as the sexual challenges faced by spouses of these individuals.
Conclusion
Collectively, the findings reveal that sexual life after SCI is not merely a private issue but a complex interplay of physical, emotional, relational, and social factors. The need for culturally sensitive counseling, sexual education, and inclusive rehabilitation policies is urgent. Furthermore, attention must be paid to the emotional health of spouses and children who also bear the psychological weight of injury-related changes. These insights can guide interventions aimed at enhancing QoL and preserving intimacy for individuals with SCI and their families.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1401.002). Participants were fully informed of the study’s objectives, and their privacy and confidentiality were protected throughout the process.
Funding
The project was financially supported by the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Authors' contributions
Conceptualization and methodology: Zoleikha Arabkari and Mohammad Kamali; Data collection, analysis and interpretation: Zoleikha Arabkari; Writing the original draft: Zoleikha Arabkaril and Mohammad Javad Esmaili; Review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Iranian Disabled Association, the Spinal Injury Association, and all participants who collaborated in this research.
References
- Bryant C, Gustafsson L, Aplin T, Setchell J. Supporting sexuality after spinal cord injury: A scoping review of non-medical approaches. Disability and Rehabilitation. 2022; 44(19):5669-82. [DOI:10.1080/09638288.2021.1937339] [PMID]
- Acosta-Santillán PL, Toro-Sashida MF, Rosas-Mendoza AV, Fuentes-Orozco C, Jasso-García K, de León-Flores PG, et al. Quality of sexual life in Mexican men after spinal cord injury. Journal of Rehabilitation Medicine. 2023; 55:11641. [DOI:10.2340/jrm.v55.11641] [PMID]
- Taylan S, Gözüyeşil E, Manav Aİ, Işık Eİ. An evaluation of the factors that affect the sexual satisfaction of people with spinal cord injuries. The Journal of Spinal Cord Medicine. 2021; 44(4):590-7. [DOI:10.1080/10790268.2019.1672955] [PMID]
- Rahmani A, Shahbandi A, Ghashghaie S, Ghodsi Z, Khazaeipour Z, Abbaszadeh M, et al. Factors affecting sexual health in individuals with spinal cord injury: A systematic scoping review. Chinese Journal of Traumatology. 2025; 28(03):193-200. [DOI:10.1016/j.cjtee.2024.05.002] [PMID]
- Barrett OE, Ho AK, Finlay KA. Sexual function and sexual satisfaction following spinal cord injury: An interpretative phenomenological analysis of partner experiences. Disability and Rehabilitation. 2024; 46(1):86-95. [DOI:10.1080/09638288.2022.2159073] [PMID]
- Sharma S. Sexuality and relationship experiences of women with spinal cord injury: Reflections from an Indian context. Sexual and Reproductive Health Matters. 2022; 29(2):2057652. [DOI:10.1080/26410397.2022.2057652] [PMID]
- Kathnelson J, Kurtz Landy CM, Ditor D, Tamim HH, Gage W. Examining the psychological and emotional experience of sexuality for men after spinal cord injury. Cogent Psychology. 2020; 7(1):1722355. [DOI:10.1080/23311908.2020.1722355]
- Kathnelson JD, Kurtz Landy CM, Ditor DS, Tamim H, Gage WH. Supporting sexual adjustment from the perspective of men living with spinal cord injury. Spinal Cord. 2020; 58(11):1176-82. [DOI:10.1038/s41393-020-0479-6] [PMID]
- Maasoumi R, Zarei F, Emami Razavi SH, Merghati Khoei E. How Iranian women with spinal cord injury understand sexuality. Trauma Monthly. 2017; 22(3):1. [DOI:10.5812/traumamon.33116]
- Esmaeilipour M, Naghavi A. [Untold stories of people living with a disability: The perspective of girls with a physical disability about sex (Persian)]. Research in Cognitive and Behavioral Sciences. 2020; 10(1):47-58. [Doi:10.22108/cbs.2021.126600.1476]
- Kreuter M, Siösteen A, Biering-Sørensen F. Sexuality and sexual life in women with spinal cord injury: A controlled study. Journal of Rehabilitation Medicine. 2008; 40(1):61-9. [DOI:10.2340/16501977-0128] [PMID]
- Farahani FK. Adolescents and young people’s sexual and reproductive health in Iran: A conceptual review. The Journal of Sex Research. 2020; 57(6):743-80. [DOI:10.1080/00224499.2020.1768203] [PMID]
- Janighorban M, Boroumandfar Z, Pourkazemi R, Mostafavi F. Barriers to vulnerable adolescent girls’ access to sexual and reproductive health. BMc Public Health. 2022; 22(1):2212. [DOI:10.1186/s12889-022-14687-4] [PMID]
- Gomes CM, Miranda EP, de Bessa Jr J, Bellucci CHS, Battistella LR, Abdo CHN, et al. Erectile function predicts sexual satisfaction in men with spinal cord injury. Sexual Medicine. 2017; 5(3):e148-e55. [DOI:10.1016/j.esxm.2017.06.002] [PMID]
- Bostani Khalesi Z, Sembor M, Azen SA. An explanation of empowerment-based sexual health education strategies: A qualitative study. Journal of Qualitative Research in Health Sciences. 2017; 6(3):253-65. [Link]
- Gianotten WL, Alley JC, Diamond LM. The health benefits of sexual expression. International Journal of Sexual Health. 2021; 33(4):478-93. [DOI:10.1080/19317611.2021.1966564] [PMID]
- Maasoumi R, Zarei F, Merghati-Khoei E, Lawson T, Emami-Razavi SH. Development of a sexual needs rehabilitation framework in women post-spinal cord injury: A study from Iran. Archives of Physical Medicine and Rehabilitation. 2018; 99(3):548-54. [DOI:10.1016/j.apmr.2017.08.477] [PMID]
- Hall AG, Karabukayeva A, Rainey C, Kelly RJ, Patterson J, Wade J, et al. Perspectives on life following a traumatic spinal cord injury. Disability and Health Journal. 2021; 14(3):101067. [DOI:10.1016/j.dhjo.2021.101067] [PMID]
- Mohammadi F, Oshvandi K, Bijani M, Borzou SR, Khodaveisi M, Masoumi SZ. Perception of facing life’s challenges in patients with spinal cord injury in Iran: A qualitative study. BMC Psychology. 2022; 10(1):202. [DOI:10.1186/s40359-022-00909-2] [PMID]
- Kudo D, Miyakoshi N, Hongo M, Kasukawa Y, Ishikawa Y, Ishikawa N, et al. An epidemiological study of traumatic spinal cord injuries in the fastest aging area in Japan. Spinal Cord. 2019; 57(6):509-15. [DOI:10.1038/s41393-019-0255-7] [PMID]
- Zanini C, Amann J, Brach M, Gemperli A, Rubinelli S. The challenges characterizing the lived experience of caregiving. A qualitative study in the field of spinal cord injury. Spinal Cord. 2021; 59(5):493-503. [DOI:10.1038/s41393-021-00618-4] [PMID]
- Mahooti F, Raheb G, Alipour F, Hatamizadeh N. Psychosocial challenges of social reintegration for people with spinal cord injury: A qualitative study. Spinal Cord. 2020; 58(10):1119-27. [DOI:10.1038/s41393-020-0449-z] [PMID]
- Soler JM, Navaux MA, Previnaire JG. Positive sexuality in men with spinal cord injury. Spinal Cord. 2018; 56(12):1199-206. [DOI:10.1038/s41393-018-0177-9] [PMID]
- Sramkova T, Skrivanova K, Dolan I, Zamecnik L, Sramkova K, Kriz J, et al. Women’s sex life after spinal cord injury. Sexual Medicine. 2017; 5(4):e255-e9. [DOI:10.1016/j.esxm.2017.07.003] [PMID]
- Taylan S, Özkan İ, Küçükakça Çelik G. Experiences of patients and their partners with sexual problems after spinal cord injury: A phenomenological qualitative study. The Journal of Spinal Cord Medicine. 2022; 45(2):245-53. [DOI:10.1080/10790268.2020.1798136] [PMID]
- Khazaeipour Z, Maasoumi R, Zarei F. Exploring Iranian individual’s perception toward divorce after disability related to spinal cord injury. Spinal Cord Series and Cases. 2020; 6(1):45. [DOI:10.1038/s41394-020-0298-1] [PMID]
- Previnaire J, Soler J, Alexander M, Courtois F, Elliott S, McLain A. Prediction of sexual function following spinal cord injury: A case series. Spinal Cord Series and Cases. 2017; 3(1):17096. [DOI:10.1038/s41394-017-0023-x] [PMID]
- Ferreiro-Velasco M, Barca-Buyo A, Salvador de La Barrera S, Montoto-Marqués A, Miguéns Vázquez X, Rodríguez-Sotillo A. Sexual issues in a sample of women with spinal cord injury. Spinal Cord. 2005; 43(1):51-5. [DOI:10.1038/sj.sc.3101657] [PMID]
- de Oliveira Ferro JK, Lemos A, da Silva CP, de Paiva Lima CRO, Raposo MCF, de Aguiar Cavalcanti G, et al. Predictive factors of male sexual dysfunction after traumatic spinal cord injury. Spine. 2019; 44(17):1228-37. [DOI:10.1097/BRS.0000000000003049] [PMID]
- Budd MA, Gater Jr DR, Channell I. Psychosocial consequences of spinal cord injury: A narrative review. Journal of Personalized Medicine. 2022; 12(7):1178. [DOI:10.3390/jpm12071178] [PMID]
Article type: Original Research Articles |
Subject:
Rehabilitation Management
Received: 2025/07/8 | Accepted: 2025/11/15 | Published: 2026/03/1
Received: 2025/07/8 | Accepted: 2025/11/15 | Published: 2026/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
