
988368
Sat, Jun 20, 2026

Volume 24, Issue 1 (March 2026)
Iranian Rehabilitation Journal 2026, 24(1): 51-64 |
Back to browse issues page



Ethics code: IR.USWR.REC.1400.039
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Haidarian M, Pourmohamadreza-Tajrishi M. Improving Response Inhibition and Social Skills in Children With Attention-deficit/hyperactivity Disorder: Cognitive Rehabilitation Exercises. Iranian Rehabilitation Journal 2026; 24 (1) :51-64
URL: http://irj.uswr.ac.ir/article-1-2612-en.html
URL: http://irj.uswr.ac.ir/article-1-2612-en.html



1- Department of Psychology and Education of Exceptional Children, Faculty of Psychology and Education Sciences, University of Isfahan, Isfahan- Iran.
2- Department of Psychology and Education of Exceptional Children, Faculty of Behavioral Sciences and Mental Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Psychology and Education of Exceptional Children, Faculty of Behavioral Sciences and Mental Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Keywords: Attention-deficit/hyperactivity disorder (ADHD), Cognitive rehabilitation, Response inhibition, Social skills
Full-Text [PDF 591 kb]
(106 Downloads)
| Abstract (HTML) (1316 Views)
References
Full-Text: (14 Views)
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental disorder of childhood, defined by core symptoms of hyperactivity, impulsivity, and inattention. Children with ADHD exhibit difficulties across cognitive and attentional domains, including problem-solving, planning, orientation, cognitive flexibility, sustained attention, response inhibition, and working memory. Additional challenges often emerge as delays in motivation and mood regulation, which are closely linked to difficulties acquiring social skills and related learning opportunities [1].
According to the criteria of the DSM-5-TR (the latest revision of the diagnostic and statistical manual of mental disorders), ADHD can be subtyped into 3 presentations: Predominantly inattentive type, predominantly hyperactive-impulsive type, and the combined type, which features both hyperactive/impulsive and inattentive symptoms [2].
Globally, the prevalence of ADHD ranges from 3% to 7%, with boys diagnosed roughly 3 to 5 times more often than girls [3]. In Iran, prevalence among primary school-aged children is reported at 8.7%, with a male-to-female ratio of approximately 4:1 [4]. The etiologies of ADHD are not fully understood and encompass genetic, environmental, and psychosocial factors. Family studies indicate a high heritability with no clear gender differences. Genetic contributions also appear to influence the persistence of ADHD into adulthood. Environmental risk factors include parental exposure to substances, exposure to toxins such as chemicals and heavy metals, nutritional factors, lifestyle factors, and broader psychosocial contexts [5].
According to Barkley, the principal deficit in ADHD lies in response inhibition, a core factor that influences cognitive functioning in children. Response inhibition is the capacity to suppress thoughts, behaviors, and emotions, enabling a child to respond to stimuli without undue delay. Impairments in response inhibition give rise to impulsive behaviors that can adversely affect other cognitive and social domains [6]. Response inhibition supports rapid, timely responding through 3 interconnected neural processes: 1) Inhibition of the dominant response; 2) halting the current response and delaying the decision to respond or continue responding; and 3) sustaining the delay period with self-directed control (interference control). Children with ADHD typically show difficulties across all 3 inhibitory processes, with the dominant response inhibition often being the most affected [7].
Response inhibition deficits in children with ADHD markedly affect social functioning. These children frequently exhibit impulsive behaviors, such as interrupting others or speaking out of turn, which can foster misunderstandings and peer conflicts. They may also have difficulty recognizing and regulating inadequate responses in social contexts [8]. Poor management of socially appropriate responses can result in negative social feedback, hindering the development and maintenance of peer relationships. Prior research indicates that children with ADHD show lower inhibitory control and longer reaction times, reflecting difficulties in regulating responses in everyday emotional and sensory environments. Impulsivity and problems sustaining social interactions can delay social learning, narrowing opportunities to acquire essential social skills. This situation can create a cycle in which social challenges undermine self-esteem, thereby impairing learning from social experiences and the acquisition of social competencies [9].
Social skills encompass the abilities involved in processing information, engaging with peers, and sustaining appropriate social interactions [10]. Children with ADHD frequently exhibit deficits in communication, social interaction, social relationship processing, and social cognition compared with typically developing peers. Because many children with ADHD may lack awareness of their social skill deficiencies, they can struggle to maintain peer and classroom relationships [11].
Response inhibition profoundly shapes how children with ADHD engage in social interactions, often creating obstacles to forming and sustaining friendships and to enjoying positive social experiences. Enhancing response inhibition alongside social skills requires a comprehensive, multifaceted strategy that emphasizes awareness, practice, and support [12]. Nonpharmacological approaches, such as neurofeedback [13], social skills training [14], response inhibition training, parent training, positive reinforcement, behavioral interventions, structured games, and the use of technology, have been proposed as integrated, multimodal treatments to address social and behavioral challenges in children [15], especially with ADHD.
Technology-based approaches are a common avenue for supporting children with ADHD. Several programs and gaming platforms aim to strengthen cognitive functions by pairing technology with structured games, making training in response inhibition and social interaction engaging [12]. Cognitive rehabilitation is one example: it uses interactive, computer-based exercises to target specific cognitive abilities, notably attention and response inhibition, through repeated practice and immediate feedback. To maintain engagement, these exercises are often game-like and incorporate educational content delivered via music, images, text, video, and animation on a computer screen. This presentation style enhances interactivity, accessibility, and measurement accuracy [16]. Grounded in neuroplasticity, cognitive rehabilitation can be viewed as a corrective and restorative approach that enables the acquisition of new skills through frequent practice and supports recall through neural reorganization [17].
Attentive rehabilitation of attention and memory (ARAM) is an applied software system developed at the Center for Cognitive Behavioral Neuroscience, Shahid Beheshti University, designed as a cognitive intervention [16]. A growing body of evidence supports ARAM’s effectiveness in executive functions [18-20], working memory, and problem-solving [21], as well as inhibitory control [22]. The cognitive rehabilitation exercises used within ARAM offer advantages over traditional interventions in several respects: 1) They employ game-like materials to capture attention, sustain engagement, and motivate children; 2) children participate actively over time, fostering continued involvement; 3) the exercises provide repeated practice opportunities, with flexible access that supports skill development; 4) content can be adjusted and individualized based on each child’s progress; 5) immediate, appropriate feedback is provided after each task, addressing the child’s needs during practice; 6) clinicians can monitor progress and support ongoing participation; and 7) the program supports ongoing exercise and periodic review, with potential for longer-term effectiveness. These features collectively distinguish cognitive rehabilitation via ARAM from conventional treatment approaches by emphasizing engagement, personalization, feedback, and sustained practice to promote skill acquisition and maintenance.
Given the advantages of cognitive rehabilitation over conventional approaches, technology-enabled interventions could enable tailored ADHD treatments in home- or school-based settings. This technology enables personalization to each child’s potential and may improve access to early intervention, thereby potentially expanding individualized treatments and benefiting community health [23]. Nevertheless, a major challenge remains: there is a lack of high-quality clinical trials providing robust evidence for the effectiveness of cognitive rehabilitation approaches. Consequently, more rigorous studies are needed to determine whether technological advances and early-access interventions can reduce or eliminate ADHD-related problems. A combined approach that integrates technological interventions with individualized treatment appears feasible and promising. Accordingly, the present study aims to evaluate the impact of cognitive rehabilitation exercises on response inhibition and social skills in children with ADHD.
Materials and Methods
This quasi-experimental study employed a pre-test–post-test and a 2-month follow-up design with a control group. From the population of boys aged 8–10 years diagnosed with ADHD in Tehran City, Iran, 30 children meeting criteria for ADHD of the combined type, as determined by a psychiatric interview, were recruited from a rehabilitation center in Tehran. The sample size was set at 30 participants (15 in the experimental group and 15 in the control group) based on a Type I error rate of 0.05, a study power of 0.84, and an anticipated attrition rate of 20%. A sample of 30 participants is relatively modest and could limit statistical power and the extent to which the findings apply to other populations. Nevertheless, the use of a control group with both a pre-test and a post-test provides a solid framework for assessing the impact of interventions. A 2-month follow-up also strengthens the study’s credibility by allowing sufficient exposure to the interventions and observation of any changes. After obtaining written informed consent, parents completed the Connors’ parent rating scale (CPRS). Each child was then individually assessed for intellectual ability using Raven’s progressive matrices (RPM). Following IQ assessment and matching on disorder severity, participants were randomly assigned to the experimental or control group. Data collection instruments included the CPRS, RPM, the stroop color–word test (SCWT), and the social skills rating scale (SSRS). The sequence of administration was as follows: CPRS (parent report), RPM (cognitive ability), SCWT, and SSRS (behavioral and social skills assessments), with randomization occurring after IQ and severity matching. The inclusion criteria were as follows: An intelligence quotient (IQ) of at least 90 on RPM, a Connors’ score of at least 60, and the absence of sensory impairments (e.g. vision or hearing loss) and comorbid disorders. Children were excluded if they were participating in a similar intervention at the same time or within the past 6 months.
CPRS is the most commonly used tool for assessing ADHD. Developed by Connors in 1997, it comprises 27 items, each rated on a 4-point scale: 0=not at all, 1=just a little, 2=quite a lot, 3=very much. Through factor analysis, 5 domains emerge: Conduct problems, learning problems, psychosomatic problems, impulsivity/hyperactivity, and anxiety. The inter-domain correlations range from 0.52 to 0.80, which supports the scale’s construct validity. The CPRS also demonstrates good discriminant validity, effectively distinguishing ADHD from non-ADHD individuals. In the Iranian population, reliability has been reported as a total-scale Cronbach α of 0.73 and a test-re-test reliability of 0.58. A t score above 60 indicates ADHD [24].
RPM is a culture-free, nonverbal measure of general intelligence that does not rely on language or literacy and comes in 2 formats to accommodate different age groups and needs. Form A, the original black-and-white version published in England in 1938, contains 60 items in which a portion of each image is missing; test-takers infer the underlying pattern and choose the correct missing piece from 6 or 8 options, with scoring the same as Form B. Form B, the colored version introduced in 1947, targets children aged 5 to 9 and adults with intellectual disabilities, consisting of 36 colored geometric images that follow the same response procedure and scoring as Form A. Raw scores are converted to IQ scores with a mean of 100 and a standard deviation of 15. Validity evidence indicates strong general-factor (g) validity, with correlations with established measures such as the Stanford–Binet and Wechsler scales ranging from roughly 0.40 to 0.76, and reliability indices across age groups ranging from about 0.40 to 0.92 [25]. The RPM demonstrated acceptable reliability and validity among Iranian school children in Tehran [26]. In the present study, RPM was administered individually.
The SCWT is a staple neuropsychological tool, first developed by Stroop in 1935, that probes selective attention and response inhibition. It is frequently applied to measures of processing speed, cognitive flexibility, and working memory. In this study, a software rendition of the task was used, comprising 3 stages in which children completed 3 distinct tables as rapidly as possible. Two tables depict congruent trials: reading color names printed in black ink and naming colored stimuli. However, the third table presents an incongruent trial where participants must name the color of the printed word rather than the word itself. This arrangement requires performing a less automatic action (color naming) while inhibiting a more automatic one (word reading), a phenomenon known as the Stroop effect. The task contains 24 items across 4 colors in 4 columns of 6. In the initial two stages, the color words and their ink colors are congruent. In the final stage, they are incongruent, demanding color-based responses while suppressing word-reading tendencies.
Participants are instructed to name the word’s ink color within a 12-s window, with scoring based on the number of correct color identifications. The total score ranges from 0 to 24, with higher scores indicating weaker inhibitory control. Reliability data show test re-test correlations of 0.86, 0.83, and 0.90 for the 3 stages [27]. The primary performance metrics are speed (mean reaction time for correct responses) and accuracy (number of correct responses). For the Persian version, test re-test reliability across the three stages was 0.84, 0.83, and 0.97, respectively, indicating favorable validity for this adaptation [28].
SSRS, created by Gresham and Elliott (1990), measures social skills and is available in parent, teacher, and student forms [29]. Each form may be used alone or in combination; higher scores denote stronger social skills. This study used the parent form, which contains 39 items across 4 subscales: cooperation (10 items), assertiveness (10 items), self-control (10 items), and responsibility (9 items). Scoring uses a 3-point scale (0=never, 1=sometimes, 2=always), yielding a possible total of 0–78. Reliability of the scale has been reported to range from 0.87 to 0.93 [30]. The Persian adaptation, validated in Shiraz City, Iran, with 304 children, showed reliability ranging from 0.77 to 0.99 in a sample including youths with intellectual disabilities and from 0.49 to 0.96 for the student and parent forms among typically developing children [31].
ARAM is a software-based program adapted from a neurological and pleasure-based attention rehabilitation intervention. It comprises 10 exercises organized hierarchically from easy to hard. Each exercise begins at a level accessible to the child, with rewards based on performance. As the child progresses, more challenging tasks are introduced. Exercises are paired with engaging stimuli to capture attention and bolster intrinsic motivation to participate.
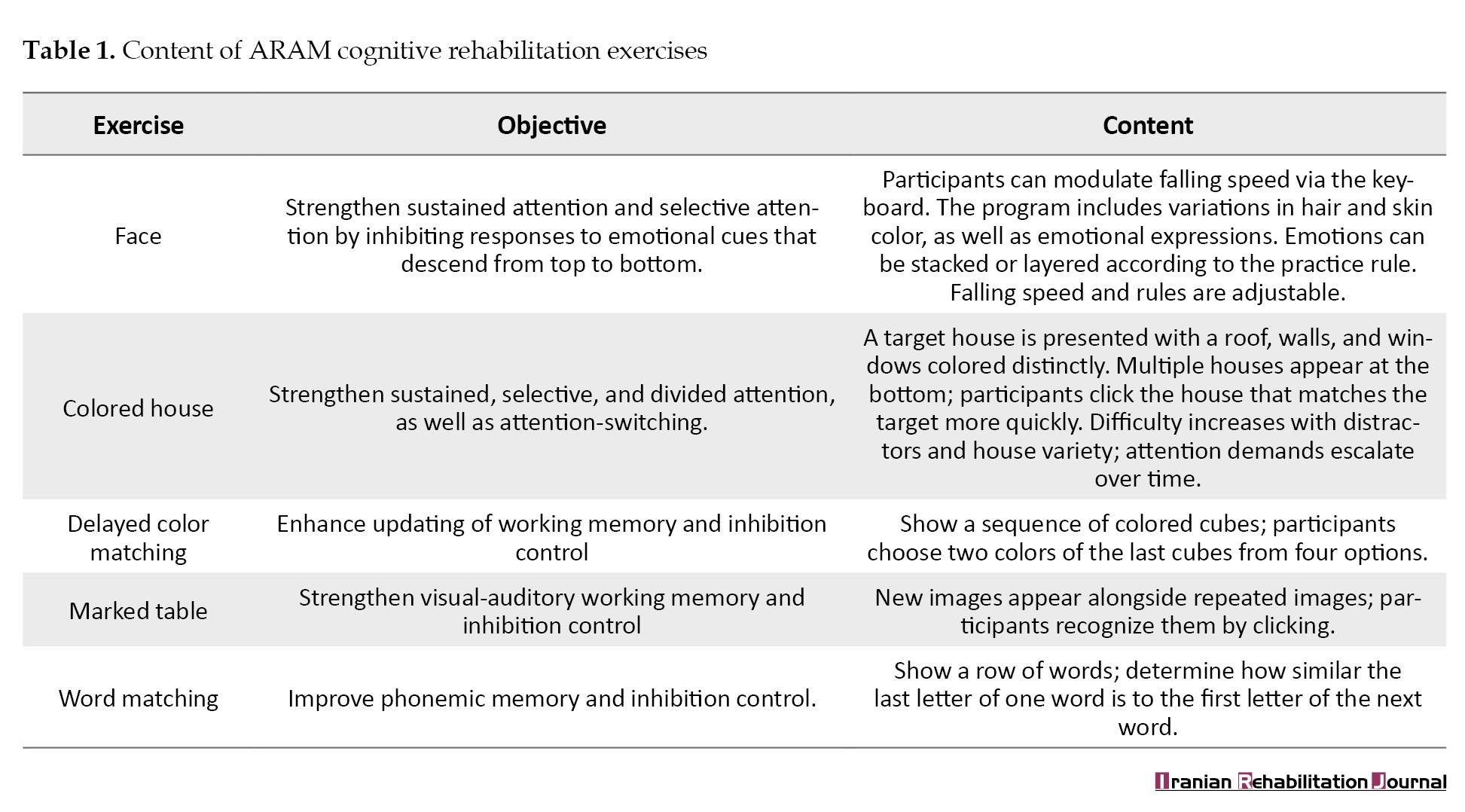
A therapist is required to supervise and ensure correct, sequential task completion. If a child fails to achieve at least 80% accuracy in a single session, the related exercises are repeated in subsequent sessions until the target performance is reached, after which progress resumes. The program design draws on the Sohlberg and Mateer attention model and incorporates aspects of working memory through a vicarious memory framework. ARAM features 5 cores, game-like activities: 1) face, shifting attention from irrelevant to relevant stimuli; 2) colored house, enhancing sustained and selective attention, 3) delayed color matching: improving inhibitory control, 4) marked table: expanding working memory span; and 5) word matching, exercising inhibitory control. An example is the face exercise, where children sort faces into categories based on a rule and 3 features: emotional expression (sad, angry, and neutral), hair color (green, white, and blue), and skin color (yellow, white, and black). Each face possesses one feature from each category, and the child must place it into the single category that matches the rule. In every set, the child must inhibit 2 features and respond to the feature specified by the rule. In short, these tasks train the ability to ignore irrelevant stimulus features and selectively attend to task-relevant features. Exercises are ranked from easy to difficult according to: a) the number of stimuli, b) the speed of stimulus presentation, c) the number of target stimuli, and d) shifts in game rules and roles (Table 1).
Research procedure
After obtaining Ethics Committee approval and securing the necessary referrals and permissions to enter the rehabilitation center, a conveniently accessible clinic in District 6 of Tehran was selected. Providing the center administrators with the information required about the study aim and securing their consent, 30 children were chosen from those who, based on a psychiatric interview, had been diagnosed with ADHD (combined type). Parents completed written consent forms and the Conners’ rating scale. The children willing to participate were individually assessed using the RPM. Based on the eligibility criteria, all 30 children were assigned to one of two groups—experimental and control—in a balanced, random manner, with IQ and symptom severity taken into account. The children in the experimental group participated in a cognitive rehabilitation program across 10 individual sessions (three times per week; each session 60 minutes). To provide an active control, the comparison group used a computer-based brain-training program that matched the experimental condition in total time, engagement, and cognitive effort, but did not target the same core constructs as the rehabilitation intervention exercises. The control program comprises an adaptive suite of tasks that challenge sustained attention, working memory, cognitive flexibility, and problem-solving. Tasks are delivered in short blocks with immediate feedback and adapt in difficulty based on performance to maintain an optimal level of challenge. Sessions were 40 minutes long, twice weekly (80 minutes per week), aligning with the same overall exposure as the ARAM program. The program includes motivational cues, progress indicators, and rewards to mimic typical cognitive-training engagement. This design helps control for nonspecific factors, such as expectancy and practice effects, allowing us to isolate ARAM-specific mechanisms. Although both groups engage in cognitively demanding activities, only ARAM targets the intended core constructs, such as attention allocation strategies and meta-cognitive tactics, facilitating a clearer assessment of ARAM-related gains beyond general cognitive stimulation. The study followed a single-blind design: Neither the children nor their parents knew whether a child had been assigned to the experimental or the control condition. To safeguard objectivity, blinded evaluators conducted outcome assessment, and the data analyst remained unaware of participants’ group allocation (experimental vs control). Data from the pre-test, post-test, and follow-up were analyzed using repeated-measures ANOVA and independent-samples t-tests in SPSS software, version 25.
Results
Across both the experimental and control groups, the most common maternal education level was 16 years (57%), with the smallest shares at 6 years of schooling (6% in one group and 3% in the other). The independent-samples t-test found no significant difference in education level between groups (P=0.396). Regarding mothers’ employment, the experimental group most often reported being employees or homemakers (33.3%), while the control group most commonly listed employee (46.7%), with no significant difference between groups on employment status (P=0.235). For the time since marriage, the majority in both groups had been married more than 10 years (about 72–73% in the experimental group and 53%–54% in the control group), with no significant between-group difference (P=0.271). Regarding maternal economic status, the experimental group most frequently fell into the middle class (40%). In contrast, the control group most frequently fell into the upper class (46.7%), again without a significant difference (P=0.263). Children’s age distributions showed the experimental group had the largest shares in the 8–9 and 9–10-year ranges (each about 46.7%), while the control group most commonly fell in the 8–9 year range (53.3%), with no significant age difference between groups (P=0.766). The chi-square test indicated no significant differences between groups for age category (χ²=33.3, P=0.504), and the Mann–Whitney U test showed no significant difference in IQ between groups (U=105, P=0.754). Conners’ rating scale scores did not differ significantly between groups on any of the factors (t=0.48; P=0.25). The Mean±SD age for the experimental and control groups were 8.47±1.5 and 8.2±1.14, respectively. Descriptive statistics for the variables of response inhibition and social skills across 3 time points (pre-test, post-test, and follow-up) for both the experimental and control groups are presented in Table 2.
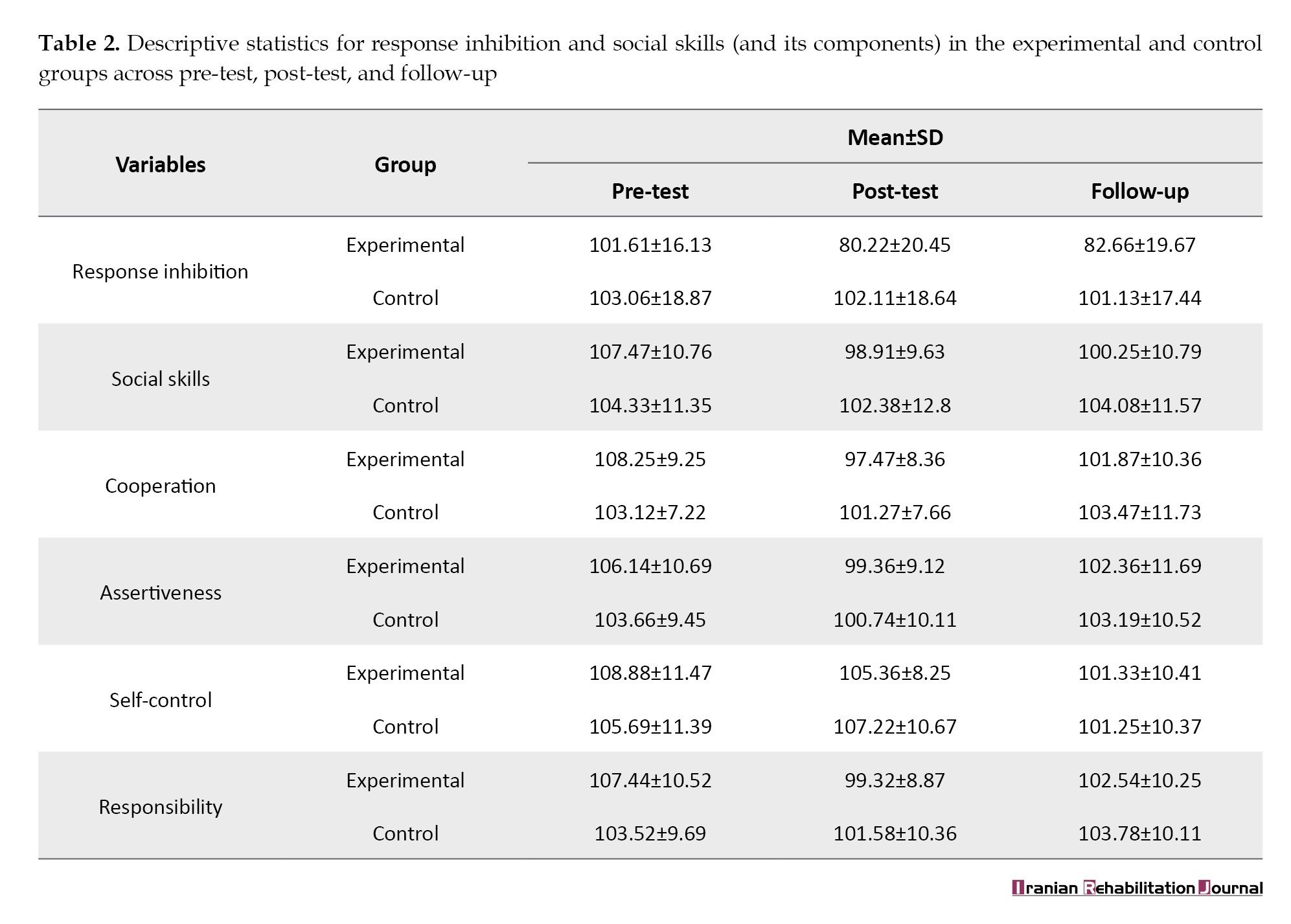
Table 2 reports descriptive statistics for two core constructs, including response inhibition and social skills (and their components: Cooperation, assertiveness, self-control, and responsibility), which were organized by time point (pre-test, post-test, follow-up) and group (experimental and control). Higher scores reflect greater social skills, while lower scores for response inhibition indicate better functioning. Across time points, the experimental group shows pronounced changes from pre-test to post-test, especially in response inhibition and several social-skills components, followed by partial reversion at follow-up. The control group, in contrast, exhibits more modest and stable patterns. This pattern—greater short-term changes with partial retention at follow-up—repeats across the global social skills measure and its components. In summary, the descriptive data suggest a more notable immediate improvement in the experimental group after the intervention, with partial maintenance at follow-up, relative to the control group; however, interpretations of significance and direction should rely on the planned inferential analyses and the scoring of each subscale.
To test the hypothesis that cognitive rehabilitation exercises improve both response inhibition and social skills in children with ADHD, a repeated-measures analysis of variance (ANOVA) was employed. Assessments of the ANOVA assumptions for repeated measures indicated that the normality assumption for the dependent variables across all three time points was met. Data inspection revealed no outliers. To examine skewness and kurtosis, the Shapiro-Wilk test was used. Since the absolute values of skewness and kurtosis for both response inhibition and social skills across the three time points in the experimental group were less than 2, the data were considered approximately normal (P>0.05). The multivariate normality assumption (Mauchly’s test) was 0.967, which, being greater than the critical value, indicated that sphericity was satisfied. Therefore, Greenhouse-Geisser correction was not necessary (epsilon=0.413/0.574, depending on the test). Given that all assumptions were met, repeated-measures ANOVA was used to compare response inhibition and social skills (and their components) between the experimental and control groups across the pre-test, post-test, and follow-up (Table 3).
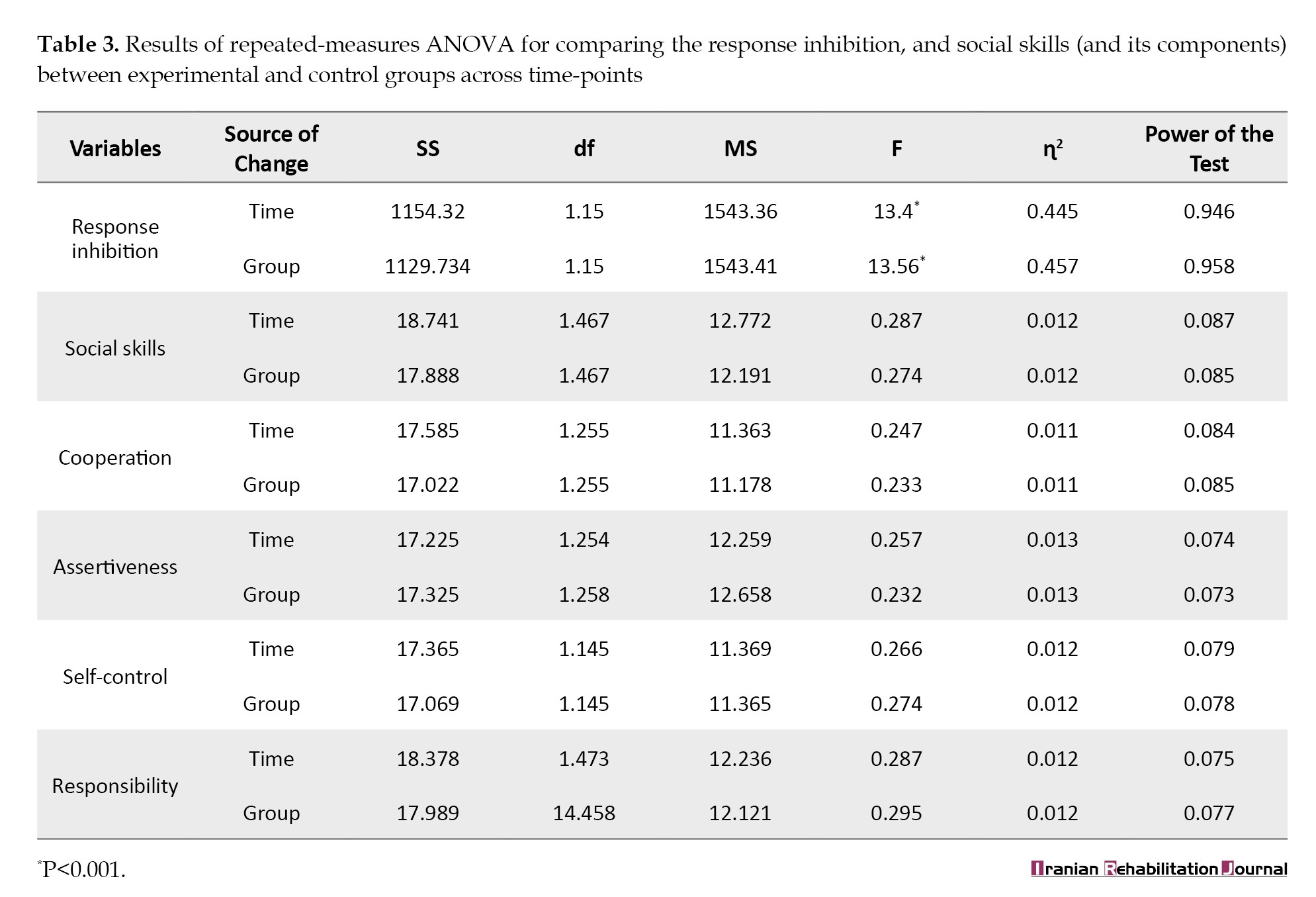
Based on the results summarized in Table 3, the mean difference in response inhibition between the experimental and control groups is statistically significant across pre-test, post-test, and follow-up, suggesting a noteworthy association with participation in cognitive rehabilitation. However, the magnitude of this association - as indicated by eta squared (η2) – suggests a substantial portion of the observed variance within the experimental group is related to the intervention. In contrast, the comparative effect size across groups remains more modest when using the same metric. Regarding social skills and their components (as shown in Table 3), there are no statistically significant between-group differences at any time point (P>0.05). η2 estimates indicate only a very small portion of variance in social skills attributable to group membership, and this modest effect does not reach significance when contrasted with the control groups’ changes. In short, the cognitive rehabilitation program appears to have a meaningful impact on response inhibition. Still, the evidence does not support a between-group difference in social skills within the study period. To assess the group effect over time, an independent-samples t-test was used at each time point (Table 4).
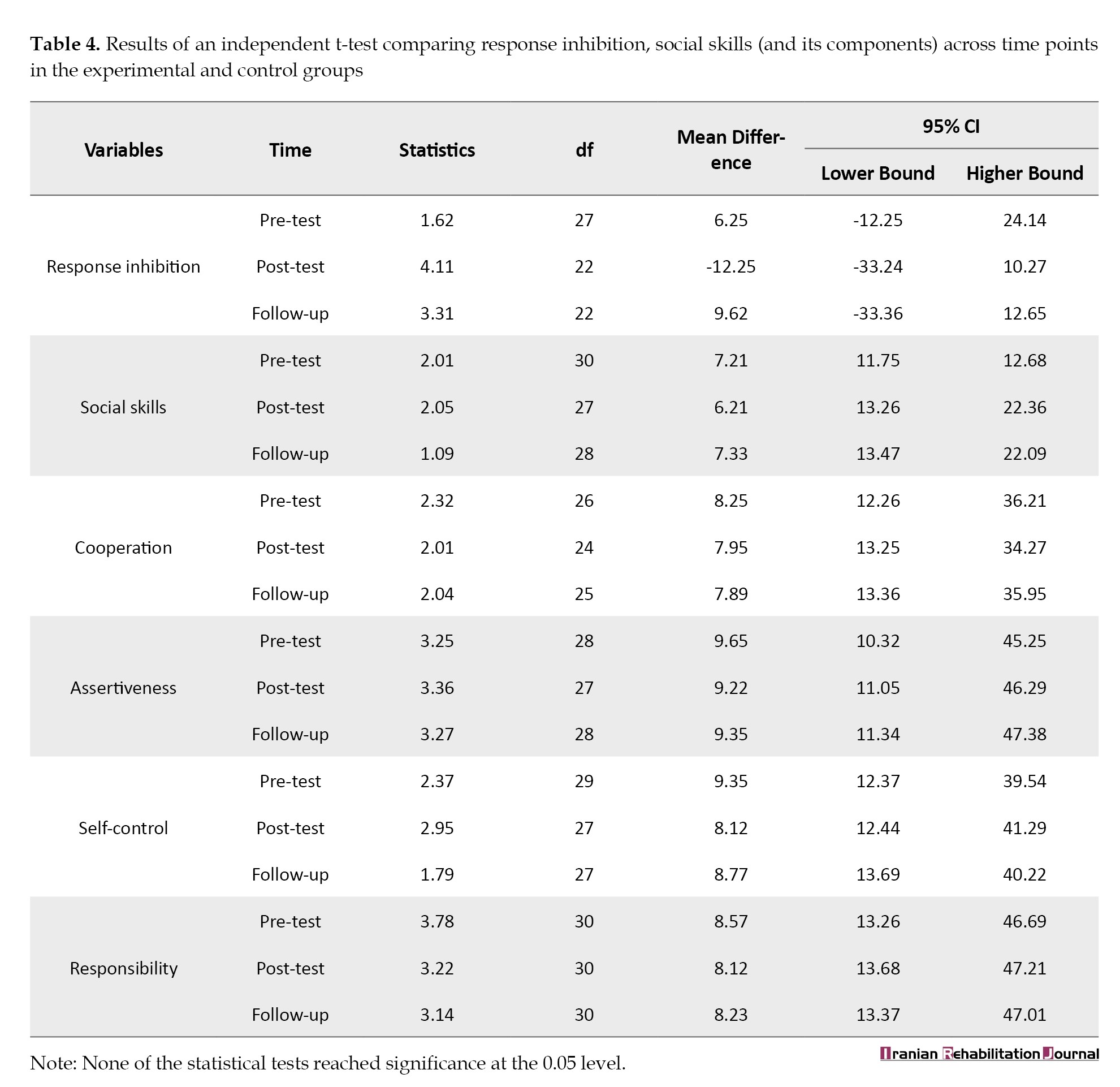
Based on Table 4, there is no evidence of a statistically significant between-group difference (experimental vs control) for response inhibition or for social skills and their components at any time point (pre-test, post-test, or follow-up). Across all measures, the P exceed 0.05, and the 95% confidence intervals for the mean differences consistently include zero, indicating substantial uncertainty about any true group effect. Although some time points show apparent mean gaps between groups, these differences are not statistically reliable within this sample. In short, the cognitive rehabilitation program did not demonstrate a detectable between-group advantage in either response inhibition or social skills, including at the 2-month follow-up. This finding emphasizes uncertainty, avoids overclaiming group effects, and clarifies that follow-up changes did not reflect a durable between-group advantage.
Discussion
The present study aimed to determine the effect of cognitive rehabilitation exercises on improving response inhibition and social skills in 8- to 10-year-old boys with combined-type ADHD. The initial findings indicate that cognitive rehabilitation exercises enhanced response inhibition in the experimental group, consistent with prior research [32, 33]. One interpretation is that advances in technology have broadened the range of therapeutic approaches for ADHD, and computer-based cognitive rehabilitation not only provides a safe, engaging environment for children but also increases their motivation to perform the exercises, with fewer negative outcomes. Because such interventions can individualize treatment and focus on each child’s unique abilities and interests, delivering positive feedback and reinforcement in each session can help the child attend to relevant cues, follow game rules, and resist distractions. All of this can be achieved through positive reinforcement and feedback during cognitive rehabilitation tasks [23].
Drawing on evidence from a prior study [32], it appears that when children with ADHD are exposed to emotionally charged stimuli during a task, their response inhibition may decline because they struggle to identify the emotions present in the stimuli. In the current study, the exercises were emotionally neutral, suggesting that children perform better and make fewer errors when processing tasks that do not involve emotional expressions, allowing them to shift their responses between stimuli more effectively and to resist interference. Consequently, response inhibition may improve. Moreover, cognitive rehabilitation exercises teach children to wait and delay a response until the appropriate moment by practicing patience and perseverance, delivering the target stimulus precisely, and ignoring or withholding responses to irrelevant stimuli until the appropriate time [23].
The second finding of the study showed that cognitive rehabilitation exercises did not improve social skills in children with combined-type ADHD. This result aligns with some prior findings [14, 34, 35] and contrasts with others [36]. One plausible explanation, supported by a prior review [34], is that the effectiveness of social-skills training interventions varies with program length and the number of sessions. The review examined 25 randomized clinical trials involving 2690 children aged 5–13 years, with intervention durations ranging from five weeks to 24 months. Most trials were conducted in outpatient clinics across the United States, Asia, and Europe. The absence of parental involvement likely constrained the transfer of social skills to the real world. The intervention did not include structured parent training, which may limit reinforcement of social skills outside the clinic and reduce opportunities for at-home practice. Notably, social-skills outcomes were more consistently reported by parents than by teachers, suggesting potential informant bias and highlighting the importance of multi-informant assessment. Many trials emphasize parent training components to ensure comprehension of the intervention and to enable parents to supervise and support at-home application of learned skills [35]. Therefore, it is plausible that the lack of combined social-skills improvement in the present study stems from the failure to implement an integrated program that jointly targets social skills and cognitive rehabilitation. The absence of structured parental training within the cognitive rehabilitation protocol may have further contributed to the minimal changes observed in children’s social skills in the experimental group. Future work should include formal parent-focused modules alongside child-focused cognitive rehabilitation and social skills training to enhance ecological validity and foster durable improvements in social functioning.
On the other hand, when interpreting the findings of the present study in light of conflicting prior results [36], it is worth noting that one study [19] reported a positive correlation between engaging in physical exercise and improvements in cognitive symptoms and social skills among children with ADHD. However, the divergence between the current study and another study [36], which reported changes in social behavior in children with ADHD after participating in a social skills intervention, suggests that the present study did not observe a meaningful change in the social skills profile of the experimental group relative to the control group following cognitive rehabilitation exercises. Indeed, some research indicates that deficits in cognitive processes (e.g. working memory) may negatively affect social understanding and reduce a child’s ability to engage in and sustain social interactions. The absence of observed social-skills improvements may reflect a tension between overt self-regulatory deficits and a child’s motivation or willingness to engage in cognitive rehabilitation exercises. In addition, parental reports of children’s social skills can be biased, and detectable gains in social functioning may require a longer or broader intervention window than the present protocol provides. Taken together, the cognitive rehabilitation training implemented in this study did not directly or indirectly elevate social skills in children with ADHD. A realistic appraisal of social functioning may therefore benefit from a more ecologically valid simulation of social interactions—elements that were not captured by the cognitive rehabilitation exercises used here. These findings suggest that explicit social-skills training, integrated with cognitive rehabilitation and practice in real-world settings, may be necessary to translate improvements in self-regulation into tangible gains in social functioning.
Improving response inhibition has wide practical implications because it may help children with ADHD recall details from past interactions, engage in discussions about current topics, and respond appropriately to social cues—a skill central to forming and maintaining social relationships at school. The results show no meaningful improvements in social skill components (including cooperation, self-control, assertiveness, and responsibility) among children with ADHD. This finding underscores the importance of incorporating parent perspectives when evaluating the real-world impact of cognitive rehabilitation interventions, as adult perceptions of children’s social abilities can influence how outcomes are interpreted.
Overall, the study suggests there are potential strategies for enhancing social skills in children with ADHD that were not captured by the cognitive rehabilitation protocol employed here. Notably, several key social competencies appear to have been under-targeted: active listening, attention to nonverbal cues (e.g. facial expressions and posture), understanding and respecting social boundaries and norms, and emotion regulation skills. While direct assessment of social situations poses challenges for children with ADHD, a deeper understanding of the link between ADHD and social cognition could inform the development of novel interventions. Such approaches might incorporate patience-building and self-awareness training to foster more meaningful and enduring social connections.
The major limitations of the present study include its cross-sectional design, non-random sampling, small sample size, reliance on parent-reported measures, absence of a combined parent-training and cognitive-rehabilitation program, and a relatively brief intervention duration. Specifically, the study enrolled 30 children (15 per group), which constrains statistical power and the generalizability of findings to broader ADHD populations. Social skills were assessed primarily through parent-report scales, which may be susceptible to informant bias and may not fully reflect real-world functioning, as parental perspectives can be influenced by expectations or daily stress. The study also relied on a single cognitive control task (the Stroop test) and a parent-rated social skills scale, which may not capture the multifaceted nature of response inhibition and social functioning in everyday contexts. This outcome underscores the need for multi-informant assessments (e.g. teacher and peer reports, direct behavioral observations) to obtain a more comprehensive picture of social skills development. The intervention consisted of 10 sessions with a 2-month follow-up. At the same time, it provides an initial assessment of effects, which may be insufficient to yield lasting, transferable changes, particularly in social skills. Although a control group with pre-test and post-test strengthens the design, the short duration may have limited the opportunity to observe sustained improvements.
To address these limitations, future work should pursue larger, randomly sampled cohorts to improve representativeness and statistical power. Longitudinal designs and randomized controlled trials would strengthen causal inferences. Extending both cognitive rehabilitation and social-skills training duration and implementing integrated, family-inclusive programs in which both parents and children receive targeted social-skills instruction could enhance ecological validity and real-world applicability. By addressing larger samples, randomization, longer interventions, and family-focused components, future research can more effectively assess and promote social functioning in children with ADHD. Additionally, future studies should incorporate a broader battery of outcome measures, including multiple cognitive-control tasks (e.g. interference control, working memory updating, and varied contexts of response inhibition) and objective/behavioral indicators of social skills (e.g. teacher ratings, peer sociometric measures, and structured behavioral observations in naturalistic settings), to provide a more nuanced and ecologically valid assessment of change.
Conclusion
Based on the present results, cognitive rehabilitation exercises improve response inhibition in children with ADHD, suggesting potential for clinically significant gains in response control and behavioral regulation. This finding has clear educational relevance, as it underscores the value of training parents and teachers in behavioral and social skills, whose active involvement is central to the effectiveness and durability of treatment outcomes. Engaged adults help children practice and generalize learned skills, potentially enhancing social skills development and quality of life for children with ADHD.
As with many early-stage studies, the generalizability of these results is constrained by sample size, demographic diversity, and design features (for example, cross-sectional elements or limited follow-up). These factors warrant cautious interpretation of the magnitude and durability of effects. If outcomes rely heavily on parent or teacher reports, there is a risk of informant bias. Objective or multi-informant measures (e.g. teacher and peer ratings, direct observation) would strengthen confidence in real-world applicability. While improvements in response inhibition are promising, translating these gains into broad social functioning and classroom behavior remains to be demonstrated across varied contexts and over time. The current approach may benefit from greater integration with broader behavioral and social skills curricula, including mechanisms for sustained practice and reinforcement beyond the intervention period.
Future work should incorporate integrated, multi-informant evaluations, including parent-, teacher-, and peer-reported outcomes, alongside objective behavioral observations, to capture a comprehensive picture of change. It will be important to evaluate long-term outcomes across multiple environments (home, school, community) and to examine differential effects by ADHD presentation, age, and comorbidities. Exploring multi-modal delivery models—computer-based, in-person coaching, and hybrid formats—could optimize engagement, scalability, and accessibility. Finally, developing structured modules that target behavioral self-regulation, classroom behavior, and social interaction skills, with systematic feedback loops, would promote transfer of skills to daily life.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (IR.USWR.REC.1400.039). Informed consent was obtained from both the mothers and the participating children before enrollment.
Funding
This work extracted from master's thesis of Milad Haidarian, approved by Department of Psychology and Education of Exceptional Children, Faculty of Psychology and Education Sciences, University of Isfahan, Isfahan, Iran. This study received partial support from the deputy of Research and Technology at the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Authors' contributions
Methodology, resources, supervision, funding acquisition, formal analysis, data interpretation, and validation: Masoume Pourmohamadreza-Tajrishi; Conceptualization, writing the original draft, data analysis, investigation review, and editing and investigation: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their appreciation to all mothers and their children with attention deficit/hyperactivity disorder for their participation in this study.
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental disorder of childhood, defined by core symptoms of hyperactivity, impulsivity, and inattention. Children with ADHD exhibit difficulties across cognitive and attentional domains, including problem-solving, planning, orientation, cognitive flexibility, sustained attention, response inhibition, and working memory. Additional challenges often emerge as delays in motivation and mood regulation, which are closely linked to difficulties acquiring social skills and related learning opportunities [1].
According to the criteria of the DSM-5-TR (the latest revision of the diagnostic and statistical manual of mental disorders), ADHD can be subtyped into 3 presentations: Predominantly inattentive type, predominantly hyperactive-impulsive type, and the combined type, which features both hyperactive/impulsive and inattentive symptoms [2].
Globally, the prevalence of ADHD ranges from 3% to 7%, with boys diagnosed roughly 3 to 5 times more often than girls [3]. In Iran, prevalence among primary school-aged children is reported at 8.7%, with a male-to-female ratio of approximately 4:1 [4]. The etiologies of ADHD are not fully understood and encompass genetic, environmental, and psychosocial factors. Family studies indicate a high heritability with no clear gender differences. Genetic contributions also appear to influence the persistence of ADHD into adulthood. Environmental risk factors include parental exposure to substances, exposure to toxins such as chemicals and heavy metals, nutritional factors, lifestyle factors, and broader psychosocial contexts [5].
According to Barkley, the principal deficit in ADHD lies in response inhibition, a core factor that influences cognitive functioning in children. Response inhibition is the capacity to suppress thoughts, behaviors, and emotions, enabling a child to respond to stimuli without undue delay. Impairments in response inhibition give rise to impulsive behaviors that can adversely affect other cognitive and social domains [6]. Response inhibition supports rapid, timely responding through 3 interconnected neural processes: 1) Inhibition of the dominant response; 2) halting the current response and delaying the decision to respond or continue responding; and 3) sustaining the delay period with self-directed control (interference control). Children with ADHD typically show difficulties across all 3 inhibitory processes, with the dominant response inhibition often being the most affected [7].
Response inhibition deficits in children with ADHD markedly affect social functioning. These children frequently exhibit impulsive behaviors, such as interrupting others or speaking out of turn, which can foster misunderstandings and peer conflicts. They may also have difficulty recognizing and regulating inadequate responses in social contexts [8]. Poor management of socially appropriate responses can result in negative social feedback, hindering the development and maintenance of peer relationships. Prior research indicates that children with ADHD show lower inhibitory control and longer reaction times, reflecting difficulties in regulating responses in everyday emotional and sensory environments. Impulsivity and problems sustaining social interactions can delay social learning, narrowing opportunities to acquire essential social skills. This situation can create a cycle in which social challenges undermine self-esteem, thereby impairing learning from social experiences and the acquisition of social competencies [9].
Social skills encompass the abilities involved in processing information, engaging with peers, and sustaining appropriate social interactions [10]. Children with ADHD frequently exhibit deficits in communication, social interaction, social relationship processing, and social cognition compared with typically developing peers. Because many children with ADHD may lack awareness of their social skill deficiencies, they can struggle to maintain peer and classroom relationships [11].
Response inhibition profoundly shapes how children with ADHD engage in social interactions, often creating obstacles to forming and sustaining friendships and to enjoying positive social experiences. Enhancing response inhibition alongside social skills requires a comprehensive, multifaceted strategy that emphasizes awareness, practice, and support [12]. Nonpharmacological approaches, such as neurofeedback [13], social skills training [14], response inhibition training, parent training, positive reinforcement, behavioral interventions, structured games, and the use of technology, have been proposed as integrated, multimodal treatments to address social and behavioral challenges in children [15], especially with ADHD.
Technology-based approaches are a common avenue for supporting children with ADHD. Several programs and gaming platforms aim to strengthen cognitive functions by pairing technology with structured games, making training in response inhibition and social interaction engaging [12]. Cognitive rehabilitation is one example: it uses interactive, computer-based exercises to target specific cognitive abilities, notably attention and response inhibition, through repeated practice and immediate feedback. To maintain engagement, these exercises are often game-like and incorporate educational content delivered via music, images, text, video, and animation on a computer screen. This presentation style enhances interactivity, accessibility, and measurement accuracy [16]. Grounded in neuroplasticity, cognitive rehabilitation can be viewed as a corrective and restorative approach that enables the acquisition of new skills through frequent practice and supports recall through neural reorganization [17].
Attentive rehabilitation of attention and memory (ARAM) is an applied software system developed at the Center for Cognitive Behavioral Neuroscience, Shahid Beheshti University, designed as a cognitive intervention [16]. A growing body of evidence supports ARAM’s effectiveness in executive functions [18-20], working memory, and problem-solving [21], as well as inhibitory control [22]. The cognitive rehabilitation exercises used within ARAM offer advantages over traditional interventions in several respects: 1) They employ game-like materials to capture attention, sustain engagement, and motivate children; 2) children participate actively over time, fostering continued involvement; 3) the exercises provide repeated practice opportunities, with flexible access that supports skill development; 4) content can be adjusted and individualized based on each child’s progress; 5) immediate, appropriate feedback is provided after each task, addressing the child’s needs during practice; 6) clinicians can monitor progress and support ongoing participation; and 7) the program supports ongoing exercise and periodic review, with potential for longer-term effectiveness. These features collectively distinguish cognitive rehabilitation via ARAM from conventional treatment approaches by emphasizing engagement, personalization, feedback, and sustained practice to promote skill acquisition and maintenance.
Given the advantages of cognitive rehabilitation over conventional approaches, technology-enabled interventions could enable tailored ADHD treatments in home- or school-based settings. This technology enables personalization to each child’s potential and may improve access to early intervention, thereby potentially expanding individualized treatments and benefiting community health [23]. Nevertheless, a major challenge remains: there is a lack of high-quality clinical trials providing robust evidence for the effectiveness of cognitive rehabilitation approaches. Consequently, more rigorous studies are needed to determine whether technological advances and early-access interventions can reduce or eliminate ADHD-related problems. A combined approach that integrates technological interventions with individualized treatment appears feasible and promising. Accordingly, the present study aims to evaluate the impact of cognitive rehabilitation exercises on response inhibition and social skills in children with ADHD.
Materials and Methods
This quasi-experimental study employed a pre-test–post-test and a 2-month follow-up design with a control group. From the population of boys aged 8–10 years diagnosed with ADHD in Tehran City, Iran, 30 children meeting criteria for ADHD of the combined type, as determined by a psychiatric interview, were recruited from a rehabilitation center in Tehran. The sample size was set at 30 participants (15 in the experimental group and 15 in the control group) based on a Type I error rate of 0.05, a study power of 0.84, and an anticipated attrition rate of 20%. A sample of 30 participants is relatively modest and could limit statistical power and the extent to which the findings apply to other populations. Nevertheless, the use of a control group with both a pre-test and a post-test provides a solid framework for assessing the impact of interventions. A 2-month follow-up also strengthens the study’s credibility by allowing sufficient exposure to the interventions and observation of any changes. After obtaining written informed consent, parents completed the Connors’ parent rating scale (CPRS). Each child was then individually assessed for intellectual ability using Raven’s progressive matrices (RPM). Following IQ assessment and matching on disorder severity, participants were randomly assigned to the experimental or control group. Data collection instruments included the CPRS, RPM, the stroop color–word test (SCWT), and the social skills rating scale (SSRS). The sequence of administration was as follows: CPRS (parent report), RPM (cognitive ability), SCWT, and SSRS (behavioral and social skills assessments), with randomization occurring after IQ and severity matching. The inclusion criteria were as follows: An intelligence quotient (IQ) of at least 90 on RPM, a Connors’ score of at least 60, and the absence of sensory impairments (e.g. vision or hearing loss) and comorbid disorders. Children were excluded if they were participating in a similar intervention at the same time or within the past 6 months.
CPRS is the most commonly used tool for assessing ADHD. Developed by Connors in 1997, it comprises 27 items, each rated on a 4-point scale: 0=not at all, 1=just a little, 2=quite a lot, 3=very much. Through factor analysis, 5 domains emerge: Conduct problems, learning problems, psychosomatic problems, impulsivity/hyperactivity, and anxiety. The inter-domain correlations range from 0.52 to 0.80, which supports the scale’s construct validity. The CPRS also demonstrates good discriminant validity, effectively distinguishing ADHD from non-ADHD individuals. In the Iranian population, reliability has been reported as a total-scale Cronbach α of 0.73 and a test-re-test reliability of 0.58. A t score above 60 indicates ADHD [24].
RPM is a culture-free, nonverbal measure of general intelligence that does not rely on language or literacy and comes in 2 formats to accommodate different age groups and needs. Form A, the original black-and-white version published in England in 1938, contains 60 items in which a portion of each image is missing; test-takers infer the underlying pattern and choose the correct missing piece from 6 or 8 options, with scoring the same as Form B. Form B, the colored version introduced in 1947, targets children aged 5 to 9 and adults with intellectual disabilities, consisting of 36 colored geometric images that follow the same response procedure and scoring as Form A. Raw scores are converted to IQ scores with a mean of 100 and a standard deviation of 15. Validity evidence indicates strong general-factor (g) validity, with correlations with established measures such as the Stanford–Binet and Wechsler scales ranging from roughly 0.40 to 0.76, and reliability indices across age groups ranging from about 0.40 to 0.92 [25]. The RPM demonstrated acceptable reliability and validity among Iranian school children in Tehran [26]. In the present study, RPM was administered individually.
The SCWT is a staple neuropsychological tool, first developed by Stroop in 1935, that probes selective attention and response inhibition. It is frequently applied to measures of processing speed, cognitive flexibility, and working memory. In this study, a software rendition of the task was used, comprising 3 stages in which children completed 3 distinct tables as rapidly as possible. Two tables depict congruent trials: reading color names printed in black ink and naming colored stimuli. However, the third table presents an incongruent trial where participants must name the color of the printed word rather than the word itself. This arrangement requires performing a less automatic action (color naming) while inhibiting a more automatic one (word reading), a phenomenon known as the Stroop effect. The task contains 24 items across 4 colors in 4 columns of 6. In the initial two stages, the color words and their ink colors are congruent. In the final stage, they are incongruent, demanding color-based responses while suppressing word-reading tendencies.
Participants are instructed to name the word’s ink color within a 12-s window, with scoring based on the number of correct color identifications. The total score ranges from 0 to 24, with higher scores indicating weaker inhibitory control. Reliability data show test re-test correlations of 0.86, 0.83, and 0.90 for the 3 stages [27]. The primary performance metrics are speed (mean reaction time for correct responses) and accuracy (number of correct responses). For the Persian version, test re-test reliability across the three stages was 0.84, 0.83, and 0.97, respectively, indicating favorable validity for this adaptation [28].
SSRS, created by Gresham and Elliott (1990), measures social skills and is available in parent, teacher, and student forms [29]. Each form may be used alone or in combination; higher scores denote stronger social skills. This study used the parent form, which contains 39 items across 4 subscales: cooperation (10 items), assertiveness (10 items), self-control (10 items), and responsibility (9 items). Scoring uses a 3-point scale (0=never, 1=sometimes, 2=always), yielding a possible total of 0–78. Reliability of the scale has been reported to range from 0.87 to 0.93 [30]. The Persian adaptation, validated in Shiraz City, Iran, with 304 children, showed reliability ranging from 0.77 to 0.99 in a sample including youths with intellectual disabilities and from 0.49 to 0.96 for the student and parent forms among typically developing children [31].
ARAM is a software-based program adapted from a neurological and pleasure-based attention rehabilitation intervention. It comprises 10 exercises organized hierarchically from easy to hard. Each exercise begins at a level accessible to the child, with rewards based on performance. As the child progresses, more challenging tasks are introduced. Exercises are paired with engaging stimuli to capture attention and bolster intrinsic motivation to participate.
A therapist is required to supervise and ensure correct, sequential task completion. If a child fails to achieve at least 80% accuracy in a single session, the related exercises are repeated in subsequent sessions until the target performance is reached, after which progress resumes. The program design draws on the Sohlberg and Mateer attention model and incorporates aspects of working memory through a vicarious memory framework. ARAM features 5 cores, game-like activities: 1) face, shifting attention from irrelevant to relevant stimuli; 2) colored house, enhancing sustained and selective attention, 3) delayed color matching: improving inhibitory control, 4) marked table: expanding working memory span; and 5) word matching, exercising inhibitory control. An example is the face exercise, where children sort faces into categories based on a rule and 3 features: emotional expression (sad, angry, and neutral), hair color (green, white, and blue), and skin color (yellow, white, and black). Each face possesses one feature from each category, and the child must place it into the single category that matches the rule. In every set, the child must inhibit 2 features and respond to the feature specified by the rule. In short, these tasks train the ability to ignore irrelevant stimulus features and selectively attend to task-relevant features. Exercises are ranked from easy to difficult according to: a) the number of stimuli, b) the speed of stimulus presentation, c) the number of target stimuli, and d) shifts in game rules and roles (Table 1).
Research procedure
After obtaining Ethics Committee approval and securing the necessary referrals and permissions to enter the rehabilitation center, a conveniently accessible clinic in District 6 of Tehran was selected. Providing the center administrators with the information required about the study aim and securing their consent, 30 children were chosen from those who, based on a psychiatric interview, had been diagnosed with ADHD (combined type). Parents completed written consent forms and the Conners’ rating scale. The children willing to participate were individually assessed using the RPM. Based on the eligibility criteria, all 30 children were assigned to one of two groups—experimental and control—in a balanced, random manner, with IQ and symptom severity taken into account. The children in the experimental group participated in a cognitive rehabilitation program across 10 individual sessions (three times per week; each session 60 minutes). To provide an active control, the comparison group used a computer-based brain-training program that matched the experimental condition in total time, engagement, and cognitive effort, but did not target the same core constructs as the rehabilitation intervention exercises. The control program comprises an adaptive suite of tasks that challenge sustained attention, working memory, cognitive flexibility, and problem-solving. Tasks are delivered in short blocks with immediate feedback and adapt in difficulty based on performance to maintain an optimal level of challenge. Sessions were 40 minutes long, twice weekly (80 minutes per week), aligning with the same overall exposure as the ARAM program. The program includes motivational cues, progress indicators, and rewards to mimic typical cognitive-training engagement. This design helps control for nonspecific factors, such as expectancy and practice effects, allowing us to isolate ARAM-specific mechanisms. Although both groups engage in cognitively demanding activities, only ARAM targets the intended core constructs, such as attention allocation strategies and meta-cognitive tactics, facilitating a clearer assessment of ARAM-related gains beyond general cognitive stimulation. The study followed a single-blind design: Neither the children nor their parents knew whether a child had been assigned to the experimental or the control condition. To safeguard objectivity, blinded evaluators conducted outcome assessment, and the data analyst remained unaware of participants’ group allocation (experimental vs control). Data from the pre-test, post-test, and follow-up were analyzed using repeated-measures ANOVA and independent-samples t-tests in SPSS software, version 25.
Results
Across both the experimental and control groups, the most common maternal education level was 16 years (57%), with the smallest shares at 6 years of schooling (6% in one group and 3% in the other). The independent-samples t-test found no significant difference in education level between groups (P=0.396). Regarding mothers’ employment, the experimental group most often reported being employees or homemakers (33.3%), while the control group most commonly listed employee (46.7%), with no significant difference between groups on employment status (P=0.235). For the time since marriage, the majority in both groups had been married more than 10 years (about 72–73% in the experimental group and 53%–54% in the control group), with no significant between-group difference (P=0.271). Regarding maternal economic status, the experimental group most frequently fell into the middle class (40%). In contrast, the control group most frequently fell into the upper class (46.7%), again without a significant difference (P=0.263). Children’s age distributions showed the experimental group had the largest shares in the 8–9 and 9–10-year ranges (each about 46.7%), while the control group most commonly fell in the 8–9 year range (53.3%), with no significant age difference between groups (P=0.766). The chi-square test indicated no significant differences between groups for age category (χ²=33.3, P=0.504), and the Mann–Whitney U test showed no significant difference in IQ between groups (U=105, P=0.754). Conners’ rating scale scores did not differ significantly between groups on any of the factors (t=0.48; P=0.25). The Mean±SD age for the experimental and control groups were 8.47±1.5 and 8.2±1.14, respectively. Descriptive statistics for the variables of response inhibition and social skills across 3 time points (pre-test, post-test, and follow-up) for both the experimental and control groups are presented in Table 2.
Table 2 reports descriptive statistics for two core constructs, including response inhibition and social skills (and their components: Cooperation, assertiveness, self-control, and responsibility), which were organized by time point (pre-test, post-test, follow-up) and group (experimental and control). Higher scores reflect greater social skills, while lower scores for response inhibition indicate better functioning. Across time points, the experimental group shows pronounced changes from pre-test to post-test, especially in response inhibition and several social-skills components, followed by partial reversion at follow-up. The control group, in contrast, exhibits more modest and stable patterns. This pattern—greater short-term changes with partial retention at follow-up—repeats across the global social skills measure and its components. In summary, the descriptive data suggest a more notable immediate improvement in the experimental group after the intervention, with partial maintenance at follow-up, relative to the control group; however, interpretations of significance and direction should rely on the planned inferential analyses and the scoring of each subscale.
To test the hypothesis that cognitive rehabilitation exercises improve both response inhibition and social skills in children with ADHD, a repeated-measures analysis of variance (ANOVA) was employed. Assessments of the ANOVA assumptions for repeated measures indicated that the normality assumption for the dependent variables across all three time points was met. Data inspection revealed no outliers. To examine skewness and kurtosis, the Shapiro-Wilk test was used. Since the absolute values of skewness and kurtosis for both response inhibition and social skills across the three time points in the experimental group were less than 2, the data were considered approximately normal (P>0.05). The multivariate normality assumption (Mauchly’s test) was 0.967, which, being greater than the critical value, indicated that sphericity was satisfied. Therefore, Greenhouse-Geisser correction was not necessary (epsilon=0.413/0.574, depending on the test). Given that all assumptions were met, repeated-measures ANOVA was used to compare response inhibition and social skills (and their components) between the experimental and control groups across the pre-test, post-test, and follow-up (Table 3).
Based on the results summarized in Table 3, the mean difference in response inhibition between the experimental and control groups is statistically significant across pre-test, post-test, and follow-up, suggesting a noteworthy association with participation in cognitive rehabilitation. However, the magnitude of this association - as indicated by eta squared (η2) – suggests a substantial portion of the observed variance within the experimental group is related to the intervention. In contrast, the comparative effect size across groups remains more modest when using the same metric. Regarding social skills and their components (as shown in Table 3), there are no statistically significant between-group differences at any time point (P>0.05). η2 estimates indicate only a very small portion of variance in social skills attributable to group membership, and this modest effect does not reach significance when contrasted with the control groups’ changes. In short, the cognitive rehabilitation program appears to have a meaningful impact on response inhibition. Still, the evidence does not support a between-group difference in social skills within the study period. To assess the group effect over time, an independent-samples t-test was used at each time point (Table 4).
Based on Table 4, there is no evidence of a statistically significant between-group difference (experimental vs control) for response inhibition or for social skills and their components at any time point (pre-test, post-test, or follow-up). Across all measures, the P exceed 0.05, and the 95% confidence intervals for the mean differences consistently include zero, indicating substantial uncertainty about any true group effect. Although some time points show apparent mean gaps between groups, these differences are not statistically reliable within this sample. In short, the cognitive rehabilitation program did not demonstrate a detectable between-group advantage in either response inhibition or social skills, including at the 2-month follow-up. This finding emphasizes uncertainty, avoids overclaiming group effects, and clarifies that follow-up changes did not reflect a durable between-group advantage.
Discussion
The present study aimed to determine the effect of cognitive rehabilitation exercises on improving response inhibition and social skills in 8- to 10-year-old boys with combined-type ADHD. The initial findings indicate that cognitive rehabilitation exercises enhanced response inhibition in the experimental group, consistent with prior research [32, 33]. One interpretation is that advances in technology have broadened the range of therapeutic approaches for ADHD, and computer-based cognitive rehabilitation not only provides a safe, engaging environment for children but also increases their motivation to perform the exercises, with fewer negative outcomes. Because such interventions can individualize treatment and focus on each child’s unique abilities and interests, delivering positive feedback and reinforcement in each session can help the child attend to relevant cues, follow game rules, and resist distractions. All of this can be achieved through positive reinforcement and feedback during cognitive rehabilitation tasks [23].
Drawing on evidence from a prior study [32], it appears that when children with ADHD are exposed to emotionally charged stimuli during a task, their response inhibition may decline because they struggle to identify the emotions present in the stimuli. In the current study, the exercises were emotionally neutral, suggesting that children perform better and make fewer errors when processing tasks that do not involve emotional expressions, allowing them to shift their responses between stimuli more effectively and to resist interference. Consequently, response inhibition may improve. Moreover, cognitive rehabilitation exercises teach children to wait and delay a response until the appropriate moment by practicing patience and perseverance, delivering the target stimulus precisely, and ignoring or withholding responses to irrelevant stimuli until the appropriate time [23].
The second finding of the study showed that cognitive rehabilitation exercises did not improve social skills in children with combined-type ADHD. This result aligns with some prior findings [14, 34, 35] and contrasts with others [36]. One plausible explanation, supported by a prior review [34], is that the effectiveness of social-skills training interventions varies with program length and the number of sessions. The review examined 25 randomized clinical trials involving 2690 children aged 5–13 years, with intervention durations ranging from five weeks to 24 months. Most trials were conducted in outpatient clinics across the United States, Asia, and Europe. The absence of parental involvement likely constrained the transfer of social skills to the real world. The intervention did not include structured parent training, which may limit reinforcement of social skills outside the clinic and reduce opportunities for at-home practice. Notably, social-skills outcomes were more consistently reported by parents than by teachers, suggesting potential informant bias and highlighting the importance of multi-informant assessment. Many trials emphasize parent training components to ensure comprehension of the intervention and to enable parents to supervise and support at-home application of learned skills [35]. Therefore, it is plausible that the lack of combined social-skills improvement in the present study stems from the failure to implement an integrated program that jointly targets social skills and cognitive rehabilitation. The absence of structured parental training within the cognitive rehabilitation protocol may have further contributed to the minimal changes observed in children’s social skills in the experimental group. Future work should include formal parent-focused modules alongside child-focused cognitive rehabilitation and social skills training to enhance ecological validity and foster durable improvements in social functioning.
On the other hand, when interpreting the findings of the present study in light of conflicting prior results [36], it is worth noting that one study [19] reported a positive correlation between engaging in physical exercise and improvements in cognitive symptoms and social skills among children with ADHD. However, the divergence between the current study and another study [36], which reported changes in social behavior in children with ADHD after participating in a social skills intervention, suggests that the present study did not observe a meaningful change in the social skills profile of the experimental group relative to the control group following cognitive rehabilitation exercises. Indeed, some research indicates that deficits in cognitive processes (e.g. working memory) may negatively affect social understanding and reduce a child’s ability to engage in and sustain social interactions. The absence of observed social-skills improvements may reflect a tension between overt self-regulatory deficits and a child’s motivation or willingness to engage in cognitive rehabilitation exercises. In addition, parental reports of children’s social skills can be biased, and detectable gains in social functioning may require a longer or broader intervention window than the present protocol provides. Taken together, the cognitive rehabilitation training implemented in this study did not directly or indirectly elevate social skills in children with ADHD. A realistic appraisal of social functioning may therefore benefit from a more ecologically valid simulation of social interactions—elements that were not captured by the cognitive rehabilitation exercises used here. These findings suggest that explicit social-skills training, integrated with cognitive rehabilitation and practice in real-world settings, may be necessary to translate improvements in self-regulation into tangible gains in social functioning.
Improving response inhibition has wide practical implications because it may help children with ADHD recall details from past interactions, engage in discussions about current topics, and respond appropriately to social cues—a skill central to forming and maintaining social relationships at school. The results show no meaningful improvements in social skill components (including cooperation, self-control, assertiveness, and responsibility) among children with ADHD. This finding underscores the importance of incorporating parent perspectives when evaluating the real-world impact of cognitive rehabilitation interventions, as adult perceptions of children’s social abilities can influence how outcomes are interpreted.
Overall, the study suggests there are potential strategies for enhancing social skills in children with ADHD that were not captured by the cognitive rehabilitation protocol employed here. Notably, several key social competencies appear to have been under-targeted: active listening, attention to nonverbal cues (e.g. facial expressions and posture), understanding and respecting social boundaries and norms, and emotion regulation skills. While direct assessment of social situations poses challenges for children with ADHD, a deeper understanding of the link between ADHD and social cognition could inform the development of novel interventions. Such approaches might incorporate patience-building and self-awareness training to foster more meaningful and enduring social connections.
The major limitations of the present study include its cross-sectional design, non-random sampling, small sample size, reliance on parent-reported measures, absence of a combined parent-training and cognitive-rehabilitation program, and a relatively brief intervention duration. Specifically, the study enrolled 30 children (15 per group), which constrains statistical power and the generalizability of findings to broader ADHD populations. Social skills were assessed primarily through parent-report scales, which may be susceptible to informant bias and may not fully reflect real-world functioning, as parental perspectives can be influenced by expectations or daily stress. The study also relied on a single cognitive control task (the Stroop test) and a parent-rated social skills scale, which may not capture the multifaceted nature of response inhibition and social functioning in everyday contexts. This outcome underscores the need for multi-informant assessments (e.g. teacher and peer reports, direct behavioral observations) to obtain a more comprehensive picture of social skills development. The intervention consisted of 10 sessions with a 2-month follow-up. At the same time, it provides an initial assessment of effects, which may be insufficient to yield lasting, transferable changes, particularly in social skills. Although a control group with pre-test and post-test strengthens the design, the short duration may have limited the opportunity to observe sustained improvements.
To address these limitations, future work should pursue larger, randomly sampled cohorts to improve representativeness and statistical power. Longitudinal designs and randomized controlled trials would strengthen causal inferences. Extending both cognitive rehabilitation and social-skills training duration and implementing integrated, family-inclusive programs in which both parents and children receive targeted social-skills instruction could enhance ecological validity and real-world applicability. By addressing larger samples, randomization, longer interventions, and family-focused components, future research can more effectively assess and promote social functioning in children with ADHD. Additionally, future studies should incorporate a broader battery of outcome measures, including multiple cognitive-control tasks (e.g. interference control, working memory updating, and varied contexts of response inhibition) and objective/behavioral indicators of social skills (e.g. teacher ratings, peer sociometric measures, and structured behavioral observations in naturalistic settings), to provide a more nuanced and ecologically valid assessment of change.
Conclusion
Based on the present results, cognitive rehabilitation exercises improve response inhibition in children with ADHD, suggesting potential for clinically significant gains in response control and behavioral regulation. This finding has clear educational relevance, as it underscores the value of training parents and teachers in behavioral and social skills, whose active involvement is central to the effectiveness and durability of treatment outcomes. Engaged adults help children practice and generalize learned skills, potentially enhancing social skills development and quality of life for children with ADHD.
As with many early-stage studies, the generalizability of these results is constrained by sample size, demographic diversity, and design features (for example, cross-sectional elements or limited follow-up). These factors warrant cautious interpretation of the magnitude and durability of effects. If outcomes rely heavily on parent or teacher reports, there is a risk of informant bias. Objective or multi-informant measures (e.g. teacher and peer ratings, direct observation) would strengthen confidence in real-world applicability. While improvements in response inhibition are promising, translating these gains into broad social functioning and classroom behavior remains to be demonstrated across varied contexts and over time. The current approach may benefit from greater integration with broader behavioral and social skills curricula, including mechanisms for sustained practice and reinforcement beyond the intervention period.
Future work should incorporate integrated, multi-informant evaluations, including parent-, teacher-, and peer-reported outcomes, alongside objective behavioral observations, to capture a comprehensive picture of change. It will be important to evaluate long-term outcomes across multiple environments (home, school, community) and to examine differential effects by ADHD presentation, age, and comorbidities. Exploring multi-modal delivery models—computer-based, in-person coaching, and hybrid formats—could optimize engagement, scalability, and accessibility. Finally, developing structured modules that target behavioral self-regulation, classroom behavior, and social interaction skills, with systematic feedback loops, would promote transfer of skills to daily life.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (IR.USWR.REC.1400.039). Informed consent was obtained from both the mothers and the participating children before enrollment.
Funding
This work extracted from master's thesis of Milad Haidarian, approved by Department of Psychology and Education of Exceptional Children, Faculty of Psychology and Education Sciences, University of Isfahan, Isfahan, Iran. This study received partial support from the deputy of Research and Technology at the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Authors' contributions
Methodology, resources, supervision, funding acquisition, formal analysis, data interpretation, and validation: Masoume Pourmohamadreza-Tajrishi; Conceptualization, writing the original draft, data analysis, investigation review, and editing and investigation: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their appreciation to all mothers and their children with attention deficit/hyperactivity disorder for their participation in this study.
References
- Halperin JM, Marks DJ, Chacko A, Bedard AC, O’Neill S, Curchack-Lichtin J, et al. Training executive, attention, and motor skills (TEAMS): A preliminary randomized clinical trial of preschool youth with ADHD. Research on Child and Adolescent Psychopathology. 2020; 48(3):375-89. [DOI:10.1007/s10802-019-00610-w] [PMID]
- APA. DSM-5-text revision 5th Ed. Diagnostic and statistical manual of mental disorders. Arlington: American Psychiatric A; 2022. [Link]
- Mohr-Jensen C, Steen-Jensen T, Bang-Schnack M. What do primary and secondary school teachers know about ADHD in children? Findings from a systematic review and a representative, nationwide sample of Danish teachers. Journal of Attention Disorders. 2019; 23(3):206-19. [DOI:10.1177/1087054715599206] [PMID]
- Hassanzadeh S, Amraei K, Samadzadeh S. A meta-analysis of attention deficit/hyperactivity disorder prevalence in Iran. Empowering Exceptional Children. 2019; 10(2):165-77. [Link]
- Froehlich TE, Anixt JS, Loe IM, Chirdkiatgumchai V, Kuan L, Gilman RC. Update on environmental risk factors for attention-deficit/hyperactivity disorder. Current Psychiatry Reports. 2011; 13(5):333-44. [DOI:10.1007/s11920-011-0221-3] [PMID]
- Dos Santos Afonso Junior A, Machado-Pinheiro W, Osório AAC, Seabra AG, Teixeira M, de Araújo Nascimento J, et al. Association between ADHD symptoms and inhibition-related brain activity using functional near-infrared spectroscopy (fNIRS). Neuroscience Letters. 2023; 792:136962. [DOI:10.1016/j.neulet.2022.136962] [PMID]
- Lee K, Cho IH, Park J, Choi H, Cheon KA. Response inhibition as a critical executive function in differentiating attention-deficit/hyperactivity disorder from autism spectrum disorder: A comprehensive attention test study. Frontiers in Psychiatry. 2024; 15. [DOI:10.3389/fpsyt.2024.1426376] [PMID]
- Barkley RA. Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment. New York: Guilford Publications; 2014. [Link]
- Wehmeier PM, Schacht A, Barkley RA. Social and emotional impairment in children and adolescents with ADHD and the impact on quality of life. Journal of Adolescent Health. 2010; 46(3):209-17. [DOI:10.1016/j.jadohealth.2009.09.009] [PMID]
- Ros R, Graziano PA. Social functioning in children with or at risk for attention deficit/hyperactivity disorder: A meta-analytic review. Journal of Clinical Child & Adolescent Psychology. 2018; 47(2):213-35. [DOI:10.1080/15374416.2016.1266644] [PMID]
- Willis D, Siceloff ER, Morse M, Neger E, Flory K. Stand-alone social skills training for youth with ADHD: A systematic review. Clinical Child and Family Psychology Review. 2019;22(3):348-66. [DOI:10.1007/s10567-019-00291-3] [PMID]
- Wong KP, Qin J, Xie YJ, Zhang B. Effectiveness of technology-based interventions for school-age children with attention-deficit/hyperactivity disorder: Systematic review and meta-analysis of randomized controlled trials. JMIR Mental Health. 2023; 10:e51459. [DOI:10.2196/51459] [PMID]
- Hemmati S, Vameghi R, Sajedi F, Gharib M, Pourmohammadreza-Tajrishi M, Teymori R. The effect of neurofeedback on brain waves in children with autism spectrum disorders. Iranian-Rehabilitation-Journal. 2016; 14(3):133-8. [DOI:10.18869/nrip.irj.14.3.133]
- Storebø OJ, Elmose Andersen M, Skoog M, Joost Hansen S, Simonsen E, Pedersen N, et al. Social skills training for attention deficit hyperactivity disorder (ADHD) in children aged 5 to 18 years. Cochrane Database of Systematic Reviews. 2019; 6(6):Cd008223. [DOI:10.1002/14651858.CD008223.pub3] [PMID]
- Tajik ZPT, Bidhendi-Yarandi R. The effect of computerized cognitive training on the improvement of emotion regulation in children with autism spectrum disorder. Journal of Comprehensive Pediatrics. 2025; 16(3):e161769. [DOI:10.5812/jcp-161769]
- Nejati V. Program for attention rehabilitation and strengthening (PARS) improves executive functions in children with attention deficit- hyperactivity disorder (ADHD). Research in Developmental Disabilities. 2021; 113:103937. [DOI:10.1016/j.ridd.2021.103937] [PMID]
- Kirk H, Gray K, Ellis K, Taffe J, Cornish K. Impact of attention training on academic achievement, executive functioning and behaviour in children with developmental disabilities: A randomised controlled trial. American. Journal on Intellectual and Developmental Disabilities. 2017; 122(2):97-117. [DOI:10.1352/1944-7558-122.2.97] [PMID]
- Alipanah M, Pourmohamadreza-Tajrishi M, Nejati V, Vahedi M. The effectiveness of cognitive rehabilitative program on executive functions in children with dyscalculia. Archieve of Rehabilitation 2022; 23(3):352-71. [DOI:10.32598/RJ.23.3.487.17]
- Haidarian M, Pourmohamadreza-Tajrishi M. Computer game-based task and the promotion of cognitive flexibility and emotion regulation in attention deficit/hyperactivity disorder. Archives of Neuroscience. 2025; 12(3):1. [DOI:10.5812/ans-161967]
- Haidarian M, Pourmohamadreza-Tajrishi M, Nejati V, Vahedi M. Effect of digital-based cognitive rehabilitation on executive functions in children with attention deficit/hyperactivity disorder. Middle East Journal of Rehabilitation and Health Studies. 2025; 12(1):e151447. [DOI:10.5812/mejrh-151447]
- Haqnazari FV Nejati, Pouretemad H. [Effectiveness of computerized working memory training on sustained attention and working memory of male school students (Persian)]. The Scientific Journal of Rehabilitation Medicine. 2022; 11(1):2-13. [DOI: 10.32598/SJRM.11.1.1]
- Martinelli MK, Mostofsky SH, Rosch KS. Investigating the impact of cognitive load and motivation on response control in relation to delay discounting in children with ADHD. Journal of Abnormal Child Psychology. 2017; 45(7):1339-53. [DOI:10.1007/s10802-016-0237-6] [PMID]
- Herrera N, Cibrian FL, Silva LM, Beltran JA, Schuck SEB, Hayes GR, et al. Digital health intervention for children with ADHD to improve mental health intervention, patient experiences, and outcomes: A study protocol. BMC Digital Health. 2024; 2(1):78. [DOI:10.1186/s44247-024-00134-4] [PMID]
- Shahaeian A, Shahim S, Bashash L, Yousefi F. Standardiztion, factor analysis and reliability of the conners’ parent reting scale for 6 to 11 years old children in Shiraz. Journal of Educational Psychology Studies. 2007; 3(3):97-120. [Link]
- Raven J, Raven JC, Court JH. Manual for raven’s progressive matrices and vocabulary scales. London: Springer Nature; 2003. [Link]
- Baraheni MN. Raven’s progressive matrices as applied to Iranian children. Educational and Psychological Measurement. 1974; 34(4):983-8. [DOI:10.1177/001316447403400433]
- Scarpina F, Tagini S. The stroop color and word test. Lausanne: Frontiers in Psychology; 2017. [DOI:10.3389/fpsyg.2017.00557] [PMID]
- Karimi Aliabad T, Kafi M, Farrahi H. Study of executive functions in bipolar disorders patients. Advances in Cognitive Sciences. 2010; 12(2):29-39. [Link]
- Gresham FM, Elliott SN. Social skills rating system. Minneapolis: NCS Pearson; 1990. [Link]
- Crosby JW. Test review: F. M. Gresham & S. N. Elliott social skills improvement system rating scales. Minneapolis, MN: NCS Pearson, 2008. Journal of Psychoeducational Assessment. 2011; 29(3):292-6. [DOI:10.1177/0734282910385806]
- Shahim S. Reliability of the social skills rating system in a group of Iranian children. Psychological Reports. 2001; 89(3):566-70. [DOI:10.2466/PR0.89.7.566-570] [PMID]
- Tenenbaum RB, Musser ED, Morris S, Ward AR, Raiker JS, Coles EK, et al. Response inhibition, response execution, and emotion regulation among children with attention-deficit/hyperactivity disorder. Research on Child and Adolescent Psychopathology. 2019; 47(4):589-603. [DOI:10.1007/s10802-018-0466-y] [PMID]
- Guan Lim C, Lim-Ashworth NSJ, Fung DSS. Updates in technology-based interventions for attention deficit hyperactivity disorder. Current Opinion in Psychiatry. 2020; 33(6):577-85. [DOI:10.1097/YCO.0000000000000643] [PMID]
- Daley D, van der Oord S, Ferrin M, Danckaerts M, Doepfner M, Cortese S, et al. Behavioral interventions in attention-deficit/hyperactivity disorder: A meta-analysis of randomized controlled trials across multiple outcome domains. Journal of the American Academy of Child and Adolescent Psychiatry. 2014; 53(8):835-47. [DOI:10.1016/j.jaac.2014.05.013] [PMID]
- Ragnarsdottir B, Hannesdottir DK, Halldorsson F, Njardvik U. Gender and age differences in social skills among children with ADHD: Peer problems and prosocial behavior. Child & Family Behavior Therapy. 2018; 40(4):263-78. [DOI:10.1080/07317107.2018.1522152]
- García-Castellar R, Sánchez-Chiva D, Roselló-Miranda B, Flor-Arasil P. Exploring the effectiveness of combining social skills training and two parent programs in improving the social competence of children with attention-deficit/hyperactivity disorder. Children. 2025; 12(2):132. [DOI:10.3390/children12020132] [PMID]
Article type: Original Research Articles |
Subject:
Psychology
Received: 2025/08/30 | Accepted: 2025/10/10 | Published: 2026/03/1
Received: 2025/08/30 | Accepted: 2025/10/10 | Published: 2026/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
