
988368
Wed, Jun 17, 2026

Volume 24, Issue 1 (March 2026)
Iranian Rehabilitation Journal 2026, 24(1): 79-98 |
Back to browse issues page



Ethics code: IR.SSRC.REC.1402.109
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abdolhosseini L, Fatahi A, Yousefian Molla R. Corrective Exercise and Orthotic Implementation in Females With Hallux Valgus: A Comparative Kinetics-based Study. Iranian Rehabilitation Journal 2026; 24 (1) :79-98
URL: http://irj.uswr.ac.ir/article-1-2627-en.html
URL: http://irj.uswr.ac.ir/article-1-2627-en.html



1- Department of Physical Education and Sport Sciences, CT.C., Islamic Azad University, Tehran, Iran.
Full-Text [PDF 1719 kb]
(115 Downloads)
| Abstract (HTML) (1403 Views)



Full-Text: (6 Views)
Introduction
Hallux valgus (HV) is a prevalent tri-planar deformity of the first ray, biomechanically characterized by lateral deviation of the hallux greater than 15°, medial deviation of the first metatarsal, and external rotation of the great toe [1]. These malalignments result in impaired range of motion at the first metatarsophalangeal (MTP) joint, lateral subluxation of the flexor hallucis tendons, and reduced load-bearing capacity during the stance phase [2]. From a kinetic perspective, the deformity is associated with excessive adduction at the tarsometatarsal joint, leading to lateral displacement and instability at the MTP joint, commonly presenting as a b:union: [3]. These biomechanical disruptions alter normal plantar pressure distribution and negatively affect gait mechanics [1].
Research indicates that HV prevalence is considerably higher in women: 30% to 58% in women compared to 12–25% in men [4, 5]. This higher percentage might have sophisticated implications for middle-aged individuals, as HV is linked to functional limitations and reduced quality of life [6]. While fall risk is often emphasized in older populations, emerging studies suggest that gait instability and postural control deficits may begin earlier in the presence of HV [4]. These impairments are likely mediated by compromised joint alignment, asymmetrical loading patterns, and hallux dysfunction during gait [7]. Since midlife represents a transitional stage in neuromuscular health, early recognition of these biomechanical alterations is crucial for implementing preventive strategies aimed at maintaining mobility.
Treatment options for this condition span both surgical and non-surgical modalities, with clinical decision-making influenced by factors, such as the severity of the deformity, patient age, physical activity level, overall health status, and individual preferences [8]. Surgical interventions, such as osteotomies, implant-based corrections, or joint replacements are typically reserved for severe cases [9]. Despite their potential effectiveness, these procedures are often costly, may involve complications, and are not always permanent solutions [9]. On the other hand, non-surgical approaches are primarily indicated in mild to moderate cases and aim to reduce pain, improve function, and correct deformity progression through conservative means [8]. These include the use of wide-toe footwear, kinesiology taping, protective pads, b:union: cushions, as well as pharmacologic agents like anti-inflammatory drugs and analgesics [8, 10, 11].
In recent years, non-invasive interventions, such as corrective exercises and orthotic devices have attracted considerable attention for their potential to alleviate symptoms and improve foot biomechanics in patients with HV [8, 11]. Despite the growing interest in conservative management strategies, the evidence regarding the efficacy of these interventions remains inconsistent and inconclusive. Some studies, including those by Bischof [12] and Kim et al. [13], have reported limited therapeutic benefits from non-invasive treatments. On the contrary, other investigations, such as Hum [14], Farzadi [15], and Kim [1] have demonstrated positive outcomes when orthoses are combined with targeted corrective exercises, notably in pain reduction and enhancement of functional capacity. Moreover, several studies emphasize the effectiveness of corrective exercises alone, particularly in decreasing pain and improving gait mechanics [8, 16]. However, these encouraging results are not universally confirmed; for example, Menz et al. [17] found no significant advantage in combining corrective.
Collectively, the body of evidence suggests that non-invasive interventions predominantly function to alleviate symptoms, improve foot biomechanics, and slow the progression of HV deformity rather than fully correct the anatomical malalignment of the hallux [14]. While individual studies have shown promising results for both corrective exercise programs and orthotic devices—especially in the early stages of the condition through biomechanical stabilization and functional improvement—a definitive consensus on the most effective conservative approach remains elusive. Moreover, a critical gap persists in understanding the comparative and combined effects of these interventions on foot kinetics and plantar pressure distribution during gait. Despite evidence supporting each modality independently, no comprehensive research has systematically evaluated how corrective exercises, orthotic use, and their combination influence plantar pressure variables in patients with HV. Accordingly, the present study is designed to compare the effects of two intervention strategies—corrective exercise and orthotic application—on kinetic foot variables and plantar pressure distribution in middle-aged women diagnosed with HV. By implementing intervention periods of eight and twelve weeks, this study aims to elucidate whether these treatment modalities can induce significant biomechanical changes during gait. Addressing this knowledge gap is pivotal for refining conservative management protocols and optimizing functional outcomes in individuals with early to moderate HV.
Materials and Methods
Study design
This study was designed as a randomized controlled trial with 3 parallel groups to investigate and compare the effects of corrective exercise band orthotic implementation on kinetic parameters in females diagnosed with HV. Participants were randomly allocated into one of three groups: Corrective exercise group (CEG), orthotic implement group (OG), and control group (CG), with an equal allocation ratio of 1:1:1. Randomization was performed using a table of random numbers by an independent individual who was not involved in the assessment or delivery of the interventions. Allocation concealment was ensured through the use of sequentially numbered, opaque sealed envelopes. These envelopes were prepared by an independent researcher not involved in participant recruitment or assessment, and were opened sequentially only after the participant’s enrollment. This process minimized the risk of selection bias. Participants were blinded to the study hypothesis and group comparisons. The visibly different interventions (corrective exercises vs orthotics) were presented as standard variations in conservative care, with no disclosure of comparative outcomes.
Outcome assessors remained unaware of group assignments by conducting measurements in a separate facility without exposure to intervention materials. Moreover, the study employed a double-blind design: participant blinding was maintained by informing all participants that they would receive one of several commonly used conservative treatments for HV, without disclosing the specific aim or group comparisons of the study. The trial was conducted at the Andaman Kar Clinic in Tehran City, Iran. The total duration of the study was 12 weeks, with data collection performed at 3 time points: baseline (pre-test), mid-intervention (week 8), and post-test (week 12). To ensure data reliability, high-precision and validated biomechanical equipment was utilized for kinetic assessments. All measurements were repeated three times, and the average was used for analysis. The assessments were conducted by a highly experienced and qualified biomechanical specialist, ensuring the collection of consistent and accurate data.
Study participants
The sample size was calculated using statistical formulas and G*Power software, version 3.1.9.7, informed by previous similar studies. With a confidence level of 95%, a statistical power of 0.8, a significance level of 0.05, and an estimated effect size of 0.45, a total of 45 participants were determined to be the required sample size. Initially, 100 individuals were screened for eligibility, and after applying the inclusion and exclusion criteria, 45 participants were enrolled and equally allocated across three parallel groups: CEG, OG, and CG, with 15 individuals in each group.
A total of 100 female patients with HV who visited Andaman Kar Clinic in Tehran were initially screened between January and June 2024. Based on inclusion and exclusion criteria, which were considered ….., 45 individuals were deemed eligible and enrolled in the study. Randomization was performed using block randomization via a random number table by an independent individual not involved in assessment or intervention delivery, with block sizes of 3 to ensure balanced group sizes. Participants with similar pre-test scores were randomly distributed across the three groups to reduce baseline variability. No participant declined participation or dropped out during the study.
The inclusion criteria were as follows: female gender, age range of 40–50 years, with physical and mental health, clinical diagnosis of mild to moderate HV (defined as an angle between 18° and 29°, mean 23.4±3.1°), not currently pregnant, no engagement in regular physical activity or other clinical trials, no history of major orthopedic or neurological conditions, and ability to follow the study protocol. Foot dominance was assessed during screening, with 42 participants identified as right-foot D and 18 as left-foot D. All participants provided informed written consent after being briefed about the study procedures. The exclusion criteria included presence of cardiovascular diseases, visual or auditory impairments, sensorimotor dysfunctions, musculoskeletal disorders, other foot deformities that could affect gait, past dislocations or fractures in the spine, lower limbs, or great toe (verified by medical records), severe HV (defined as an angle >30°) [11], joint stiffness, or inability to perform the prescribed exercises. Participants were also excluded if they failed to comply with the protocol or voluntarily withdrew during the intervention period. However, none of the participants met these exclusion conditions during the trial. The exclusion criteria were evaluated through clinical examination, personal health questionnaires, and medical records.
Body mass index (BMI) was calculated using the standard formula: weight (kg)/height (m²) [18]. HV angle and joint flexibility were measured by a trained physician using a standardized goniometer [19]. Weekly follow-up calls were made to monitor compliance with both the corrective exercise and orthotic interventions. At baseline, there were no statistically significant differences between the CEG, OG, and CG in terms of age, BMI, or kinetic parameters, confirming the success of the randomization process. All data were collected confidentially and stored securely, accessible only to the lead investigator and evaluator.
Study intervention
Three groups participated in this randomized controlled trial: the CEG, the OG, and the CG. The interventions for each group are detailed below.
Orthotic group (OG)
Participants in the OG used HV splints (Andam Kar Company®) [20], which are small dynamic braces attached to the great toe and foot. These splints were designed to align the great toe joint neutrally, support joint movement during gait, protect the bony prominence from friction, and reduce active bursitis. The splint consisted of an internal bar applying outward pressure on the first metatarsal, a strap pulling the great toe inward, and a second strap securing the metatarsals. Additionally, a hinge supported the great toe joint during walking. The splints were custom-fitted for each participant without requiring specialized adjustments and were suitable for home use Figure 1 represents the HV orthotic splint.
Hallux valgus (HV) is a prevalent tri-planar deformity of the first ray, biomechanically characterized by lateral deviation of the hallux greater than 15°, medial deviation of the first metatarsal, and external rotation of the great toe [1]. These malalignments result in impaired range of motion at the first metatarsophalangeal (MTP) joint, lateral subluxation of the flexor hallucis tendons, and reduced load-bearing capacity during the stance phase [2]. From a kinetic perspective, the deformity is associated with excessive adduction at the tarsometatarsal joint, leading to lateral displacement and instability at the MTP joint, commonly presenting as a b:union: [3]. These biomechanical disruptions alter normal plantar pressure distribution and negatively affect gait mechanics [1].
Research indicates that HV prevalence is considerably higher in women: 30% to 58% in women compared to 12–25% in men [4, 5]. This higher percentage might have sophisticated implications for middle-aged individuals, as HV is linked to functional limitations and reduced quality of life [6]. While fall risk is often emphasized in older populations, emerging studies suggest that gait instability and postural control deficits may begin earlier in the presence of HV [4]. These impairments are likely mediated by compromised joint alignment, asymmetrical loading patterns, and hallux dysfunction during gait [7]. Since midlife represents a transitional stage in neuromuscular health, early recognition of these biomechanical alterations is crucial for implementing preventive strategies aimed at maintaining mobility.
Treatment options for this condition span both surgical and non-surgical modalities, with clinical decision-making influenced by factors, such as the severity of the deformity, patient age, physical activity level, overall health status, and individual preferences [8]. Surgical interventions, such as osteotomies, implant-based corrections, or joint replacements are typically reserved for severe cases [9]. Despite their potential effectiveness, these procedures are often costly, may involve complications, and are not always permanent solutions [9]. On the other hand, non-surgical approaches are primarily indicated in mild to moderate cases and aim to reduce pain, improve function, and correct deformity progression through conservative means [8]. These include the use of wide-toe footwear, kinesiology taping, protective pads, b:union: cushions, as well as pharmacologic agents like anti-inflammatory drugs and analgesics [8, 10, 11].
In recent years, non-invasive interventions, such as corrective exercises and orthotic devices have attracted considerable attention for their potential to alleviate symptoms and improve foot biomechanics in patients with HV [8, 11]. Despite the growing interest in conservative management strategies, the evidence regarding the efficacy of these interventions remains inconsistent and inconclusive. Some studies, including those by Bischof [12] and Kim et al. [13], have reported limited therapeutic benefits from non-invasive treatments. On the contrary, other investigations, such as Hum [14], Farzadi [15], and Kim [1] have demonstrated positive outcomes when orthoses are combined with targeted corrective exercises, notably in pain reduction and enhancement of functional capacity. Moreover, several studies emphasize the effectiveness of corrective exercises alone, particularly in decreasing pain and improving gait mechanics [8, 16]. However, these encouraging results are not universally confirmed; for example, Menz et al. [17] found no significant advantage in combining corrective.
Collectively, the body of evidence suggests that non-invasive interventions predominantly function to alleviate symptoms, improve foot biomechanics, and slow the progression of HV deformity rather than fully correct the anatomical malalignment of the hallux [14]. While individual studies have shown promising results for both corrective exercise programs and orthotic devices—especially in the early stages of the condition through biomechanical stabilization and functional improvement—a definitive consensus on the most effective conservative approach remains elusive. Moreover, a critical gap persists in understanding the comparative and combined effects of these interventions on foot kinetics and plantar pressure distribution during gait. Despite evidence supporting each modality independently, no comprehensive research has systematically evaluated how corrective exercises, orthotic use, and their combination influence plantar pressure variables in patients with HV. Accordingly, the present study is designed to compare the effects of two intervention strategies—corrective exercise and orthotic application—on kinetic foot variables and plantar pressure distribution in middle-aged women diagnosed with HV. By implementing intervention periods of eight and twelve weeks, this study aims to elucidate whether these treatment modalities can induce significant biomechanical changes during gait. Addressing this knowledge gap is pivotal for refining conservative management protocols and optimizing functional outcomes in individuals with early to moderate HV.
Materials and Methods
Study design
This study was designed as a randomized controlled trial with 3 parallel groups to investigate and compare the effects of corrective exercise band orthotic implementation on kinetic parameters in females diagnosed with HV. Participants were randomly allocated into one of three groups: Corrective exercise group (CEG), orthotic implement group (OG), and control group (CG), with an equal allocation ratio of 1:1:1. Randomization was performed using a table of random numbers by an independent individual who was not involved in the assessment or delivery of the interventions. Allocation concealment was ensured through the use of sequentially numbered, opaque sealed envelopes. These envelopes were prepared by an independent researcher not involved in participant recruitment or assessment, and were opened sequentially only after the participant’s enrollment. This process minimized the risk of selection bias. Participants were blinded to the study hypothesis and group comparisons. The visibly different interventions (corrective exercises vs orthotics) were presented as standard variations in conservative care, with no disclosure of comparative outcomes.
Outcome assessors remained unaware of group assignments by conducting measurements in a separate facility without exposure to intervention materials. Moreover, the study employed a double-blind design: participant blinding was maintained by informing all participants that they would receive one of several commonly used conservative treatments for HV, without disclosing the specific aim or group comparisons of the study. The trial was conducted at the Andaman Kar Clinic in Tehran City, Iran. The total duration of the study was 12 weeks, with data collection performed at 3 time points: baseline (pre-test), mid-intervention (week 8), and post-test (week 12). To ensure data reliability, high-precision and validated biomechanical equipment was utilized for kinetic assessments. All measurements were repeated three times, and the average was used for analysis. The assessments were conducted by a highly experienced and qualified biomechanical specialist, ensuring the collection of consistent and accurate data.
Study participants
The sample size was calculated using statistical formulas and G*Power software, version 3.1.9.7, informed by previous similar studies. With a confidence level of 95%, a statistical power of 0.8, a significance level of 0.05, and an estimated effect size of 0.45, a total of 45 participants were determined to be the required sample size. Initially, 100 individuals were screened for eligibility, and after applying the inclusion and exclusion criteria, 45 participants were enrolled and equally allocated across three parallel groups: CEG, OG, and CG, with 15 individuals in each group.
A total of 100 female patients with HV who visited Andaman Kar Clinic in Tehran were initially screened between January and June 2024. Based on inclusion and exclusion criteria, which were considered ….., 45 individuals were deemed eligible and enrolled in the study. Randomization was performed using block randomization via a random number table by an independent individual not involved in assessment or intervention delivery, with block sizes of 3 to ensure balanced group sizes. Participants with similar pre-test scores were randomly distributed across the three groups to reduce baseline variability. No participant declined participation or dropped out during the study.
The inclusion criteria were as follows: female gender, age range of 40–50 years, with physical and mental health, clinical diagnosis of mild to moderate HV (defined as an angle between 18° and 29°, mean 23.4±3.1°), not currently pregnant, no engagement in regular physical activity or other clinical trials, no history of major orthopedic or neurological conditions, and ability to follow the study protocol. Foot dominance was assessed during screening, with 42 participants identified as right-foot D and 18 as left-foot D. All participants provided informed written consent after being briefed about the study procedures. The exclusion criteria included presence of cardiovascular diseases, visual or auditory impairments, sensorimotor dysfunctions, musculoskeletal disorders, other foot deformities that could affect gait, past dislocations or fractures in the spine, lower limbs, or great toe (verified by medical records), severe HV (defined as an angle >30°) [11], joint stiffness, or inability to perform the prescribed exercises. Participants were also excluded if they failed to comply with the protocol or voluntarily withdrew during the intervention period. However, none of the participants met these exclusion conditions during the trial. The exclusion criteria were evaluated through clinical examination, personal health questionnaires, and medical records.
Body mass index (BMI) was calculated using the standard formula: weight (kg)/height (m²) [18]. HV angle and joint flexibility were measured by a trained physician using a standardized goniometer [19]. Weekly follow-up calls were made to monitor compliance with both the corrective exercise and orthotic interventions. At baseline, there were no statistically significant differences between the CEG, OG, and CG in terms of age, BMI, or kinetic parameters, confirming the success of the randomization process. All data were collected confidentially and stored securely, accessible only to the lead investigator and evaluator.
Study intervention
Three groups participated in this randomized controlled trial: the CEG, the OG, and the CG. The interventions for each group are detailed below.
Orthotic group (OG)
Participants in the OG used HV splints (Andam Kar Company®) [20], which are small dynamic braces attached to the great toe and foot. These splints were designed to align the great toe joint neutrally, support joint movement during gait, protect the bony prominence from friction, and reduce active bursitis. The splint consisted of an internal bar applying outward pressure on the first metatarsal, a strap pulling the great toe inward, and a second strap securing the metatarsals. Additionally, a hinge supported the great toe joint during walking. The splints were custom-fitted for each participant without requiring specialized adjustments and were suitable for home use Figure 1 represents the HV orthotic splint.
Participants were instructed to wear the splints for 6 hours overnight and an additional 2 to 4 hours during the day, either inside shoes while walking or wearing socks at home, amounting to approximately 8 to 10 hours daily. During the first 10 days, usage was gradually increased, starting from 1 hour per day and incrementally reaching the full daily duration. Compliance was monitored weekly through telephone calls. The splint efficacy and comfort were not pre-tested or validated in pilot users for this study, but were supported by prior meta-analytic evidence on similar orthotic designs [20]. Adherence was monitored through self-reported weekly telephone follow-ups, which may introduce reporting bias.
CEG
Participants in the CEG followed a 12-week home-based corrective exercise program, aimed at addressing muscle imbalances and movement compensations related to HV. Previous studies have shown that structured neuromuscular training can significantly enhance balance and coordination in individuals with foot and ankle dysfunction [21]. The program focused on stretching the adductor hallucis, strengthening the abductor hallucis, increasing the range of motion of the great toe, and reinforcing intrinsic foot muscles. The exercise protocol consisted of 9 specific exercises [21]. Figure 2 represents the corrective exercise program, performed 5 days per week over 12 weeks.
CEG
Participants in the CEG followed a 12-week home-based corrective exercise program, aimed at addressing muscle imbalances and movement compensations related to HV. Previous studies have shown that structured neuromuscular training can significantly enhance balance and coordination in individuals with foot and ankle dysfunction [21]. The program focused on stretching the adductor hallucis, strengthening the abductor hallucis, increasing the range of motion of the great toe, and reinforcing intrinsic foot muscles. The exercise protocol consisted of 9 specific exercises [21]. Figure 2 represents the corrective exercise program, performed 5 days per week over 12 weeks.
The exercises were as follows: toe stretch, where participants lifted their toes upward for 5 seconds and then curled them downward for 5 seconds, repeated 10 times; toe flexion/extension, performed in a kneeling position by pressing the toes against a hard surface for 10 seconds, repeated 4 times; followed by flexing the toes in the opposite direction for 10 seconds, repeated 4 times; great toe stretch, which involved pulling the great toe outward using the fingers and holding for 10 seconds, repeated 4 times; towel gathering, in which participants gathered a towel placed on the floor using their toes, repeated 5 times; resisted toe exercise, performed by wrapping a resistance band or towel around the toes and pulling outward against resistance, repeated 5 times; ball rolling, rolling a golf ball-sized object under the foot for 2 minutes to reduce muscle tension; marble pickup, where participants picked up 20 marbles with their toes and placed them into a bowl; heel lift, performed while seated by lifting the heels and shifting weight to the toes for 5 seconds, repeated 10 times per foot; and seated toe stretch, in which participants sat while lifting one leg and pulled the toes back with the opposite hand for 20 repetitions, performed in 2–3 sets.
The exercises were initially demonstrated and supervised by a specialized rehabilitation and corrective exercise expert at Andaman Kar Clinic to ensure proper technique and understanding. Each session lasted approximately 16 minutes and was performed 5 days per week. Exercise intensity and resistance were not progressively adjusted during the program to maintain consistency and accessibility for home-based implementation. Participants performed the exercises independently at home, with compliance monitored weekly via telephone follow-ups.
CG
Participants in the CG did not receive any specific intervention and were instructed to continue their usual daily activities throughout the study period.
Instruments and equipment
The HV angle was measured using a specialized goniometer (Brand Tavangostar, Model 360) with a measurement accuracy of ±1 degrees. The reliability and validity of this goniometer have been confirmed in previous studies [19]. Participants stood in a natural position while the goniometer’s center was placed on the medial prominence of the great toe. The device’s arms were aligned along the first metatarsal and proximal phalanx, and the angle was read from the indicator. Figure 3 presents the specialized goniometer for HV assessment.
The exercises were initially demonstrated and supervised by a specialized rehabilitation and corrective exercise expert at Andaman Kar Clinic to ensure proper technique and understanding. Each session lasted approximately 16 minutes and was performed 5 days per week. Exercise intensity and resistance were not progressively adjusted during the program to maintain consistency and accessibility for home-based implementation. Participants performed the exercises independently at home, with compliance monitored weekly via telephone follow-ups.
CG
Participants in the CG did not receive any specific intervention and were instructed to continue their usual daily activities throughout the study period.
Instruments and equipment
The HV angle was measured using a specialized goniometer (Brand Tavangostar, Model 360) with a measurement accuracy of ±1 degrees. The reliability and validity of this goniometer have been confirmed in previous studies [19]. Participants stood in a natural position while the goniometer’s center was placed on the medial prominence of the great toe. The device’s arms were aligned along the first metatarsal and proximal phalanx, and the angle was read from the indicator. Figure 3 presents the specialized goniometer for HV assessment.
Dynamic plantar pressure variables were assessed using a foot scan device (RS Scan, Belgium; dimensions 0.5×0.5×0.02 m; equipped with 4363 sensors and operating at 300 Hz). The device was installed flush with the ground surface in the orthotics clinic (Andaman Kar Clinic), where environmental factors such as temperature (<19 °C), humidity (<19% humidity), and lighting were controlled to minimize their effect on data accuracy. The RS Scan system was calibrated according to the protocol described by Koller et al. [22], ensuring precise and reliable pressure measurement. During the assessment, participants walked barefoot across a 10-m walkway with the foot scan device located at the midpoint. Each foot was scanned separately: one foot stepped on the device while the other remained off it, and then the process was repeated in the opposite direction. Before formal data collection, participants were familiarized with the walking procedure through 3 practice trials. If balance or gait irregularities were observed, the trial was repeated to ensure data quality. Three valid walking trials were recorded per participant, with a one-minute rest interval between trials. The stance phase (heel strike to toe-off) was analyzed to extract plantar pressure parameters in ten defined regions: Great toe (T1), toes 2–5 (T2–5), first to fifth metatarsals (M1–M5), midfoot (MF), medial heel (MH), and lateral heel (LH) [22]. Data were transmitted to a processor and visualized via color-coded pressure maps (black indicating no pressure, red indicating the highest pressure, and blue indicating the lowest pressure).
Data collection was conducted by a highly skilled operator specialized in biomechanics and rehabilitation, ensuring precise and reliable measurements. Invalid or noisy data were excluded following thorough quality checks. Each measurement was repeated three times, and the best value was selected for analysis to enhance reliability. Test-retest reliability for plantar pressure measurements with the RS Scan system has been reported as high in previous research [23].
All procedures were conducted following ethical approval and with participants’ informed consent, adhering to the principles of the Declaration of Helsinki.
Variables and outcome measures
The independent variable in this randomized controlled trial was the intervention group, consisting of three groups: CEG, OG, and CG. The inclusion of the CG group was essential to serve as a baseline, allowing comparison of the effects of CEG and OG interventions against the natural progression without treatment.
The dependent variables comprised biomechanical kinetic parameters of plantar pressure, measured dynamically during the stance phase of gait—a critical period for foot loading and force transmission [22]. These variables included:
Maximum plantar pressure (Pmax)
Defined as the highest-pressure value recorded in Newtons per square centimeter (N/cm²) by any sensor within the designated foot regions during stance, reflecting peak load areas relevant in HV pathology [24]. Calculated by Equation 1:
1. Pmax=max(P1, P2, ..., Pn)
Loading rate (R):
The rate of force application upon foot-ground contact, indicative of mechanical stress and potential injury risk. It is calculated as the ratio of ground reaction force (F) to the contact area (A) [24] (Equation 2):
Impulse (J):
The integral of force throughout application during stance, representing total momentum transfer [24] (Equation 3):
Measurements were obtained using the RS scan foot pressure system (RS scan international, Belgium) at a sampling frequency of 300 Hz during walking trials along a 10-m walkway. The plantar surface was segmented into ten anatomical regions—great toe (T1), toes 2–5 (T2–5), first through fifth metatarsals (M1–M5), MF, MH, and LH—to enable detailed regional pressure analysis [25].
Statistical analysis
Descriptive statistics, including means and standard deviations, were calculated to summarize participant demographics and outcome variables. The Shapiro-Wilk test was used to assess data normality, and Levene’s test evaluated homogeneity of variances. For variables with normal distribution, inferential analysis was performed using a repeated measures general linear model (GLM) to examine the effects of study groups (CEG, OG, and CG), time (baseline, week 8, and week 12), and their interaction on the dependent variables. Post-hoc pairwise comparisons with Bonferroni correction were conducted to identify significant differences between groups and time points. All analyses were performed using SPSS software, version 26 (IBM Corp., New York, USA), with a significance level set at P<0.05. Missing data were not present, as all participants completed the study.
Results
Participant flow and baseline characteristics
All 45 participants (15 per group) completed the study without dropping out. Baseline demographic and kinetic parameters were comparable across groups (P>0.05), confirming successful randomization. Baseline demographic and clinical characteristics of participants are presented in Table 1.
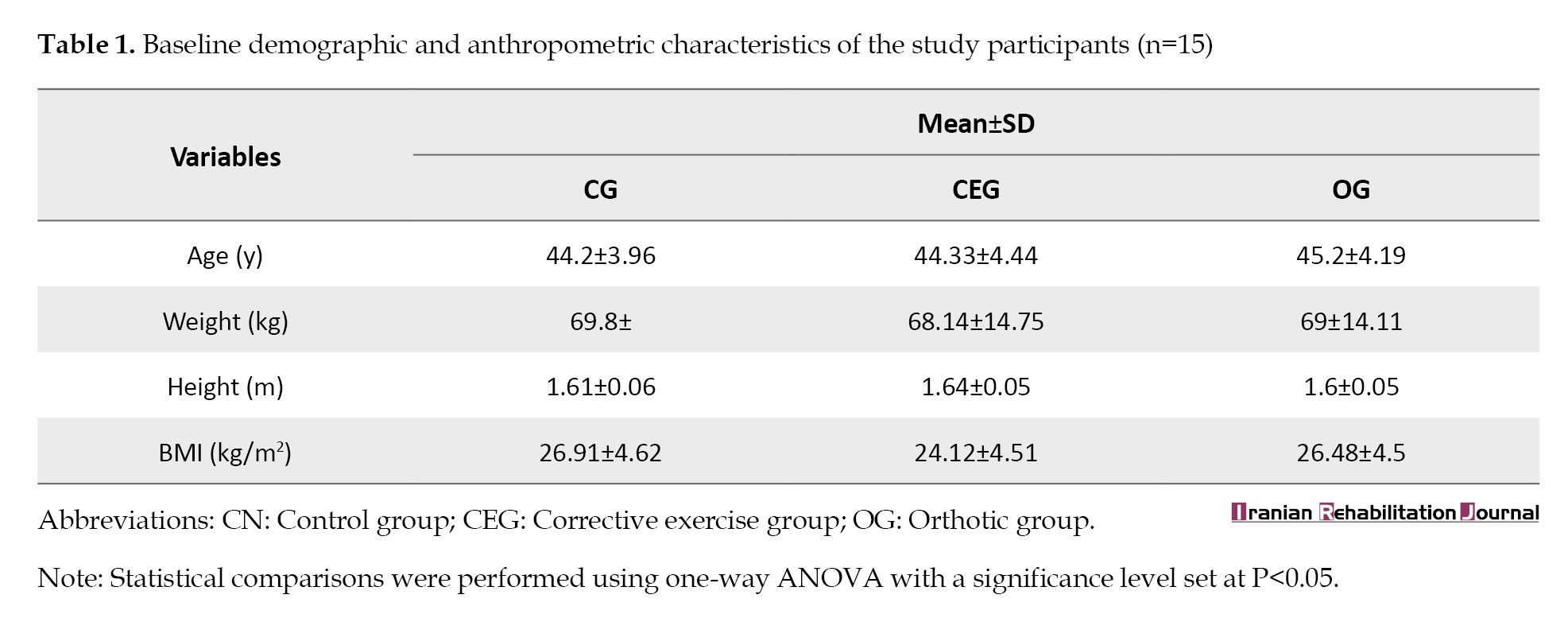
No statistically significant differences were found among the CG, CEG, and OG regarding age, weight, height, and BMI at baseline (all P>0.05). This finding indicates that randomization successfully achieved comparable groups before the intervention.
Inferential statistics
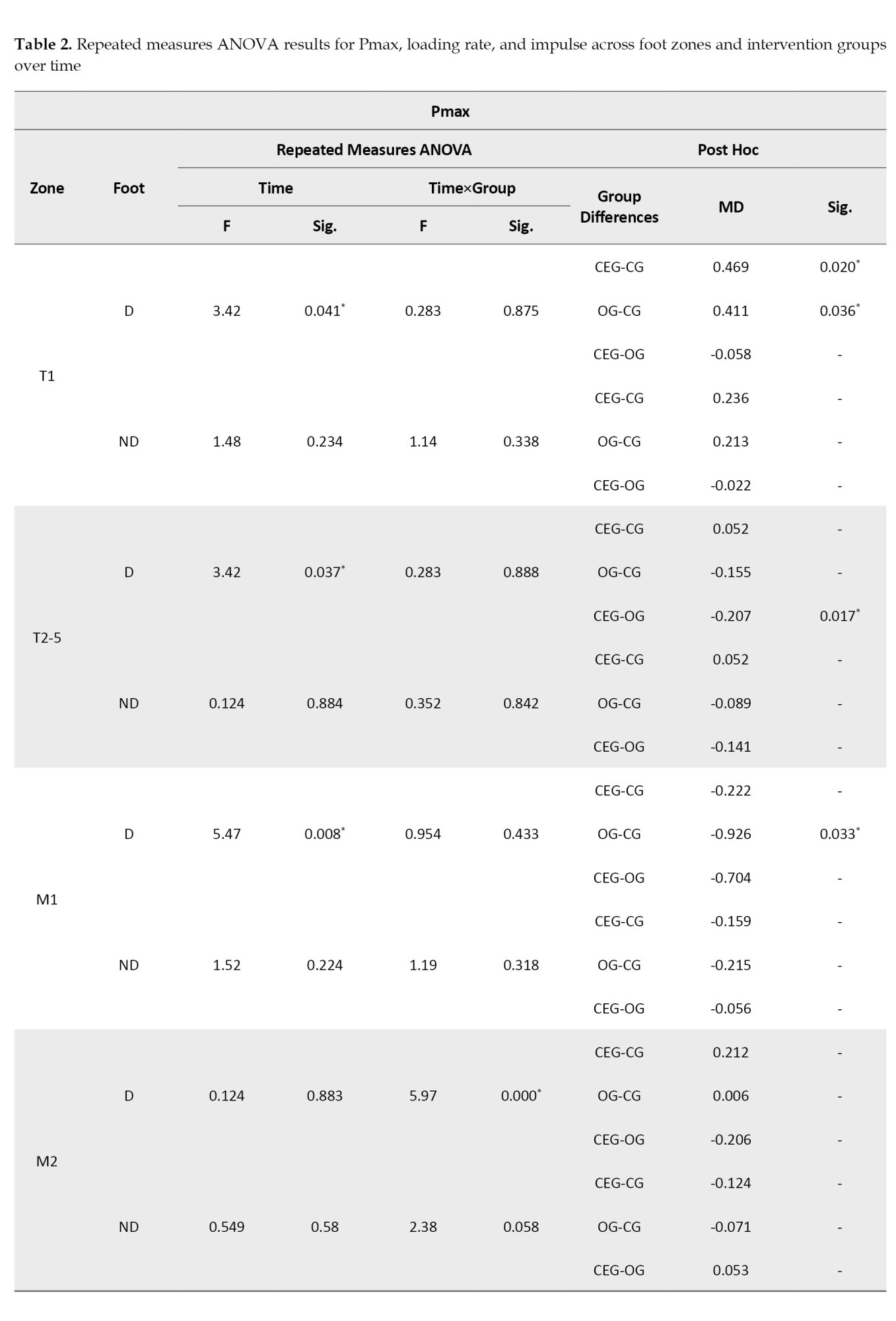
To examine the effects of corrective exercises and orthotic interventions on kinetic parameters, a repeated measures ANOVA was conducted for each dependent variable—Pmax, loading rate, and impulse—across different foot zones and time points (baseline, week 8, and week 12). Analyses were performed for both the dominant (D) and non-dominant (ND) limbs. Where significant main or interaction effects were observed, Bonferroni-adjusted post hoc comparisons were used to identify specific intergroup differences. A detailed summary of these results is presented in Table 2.
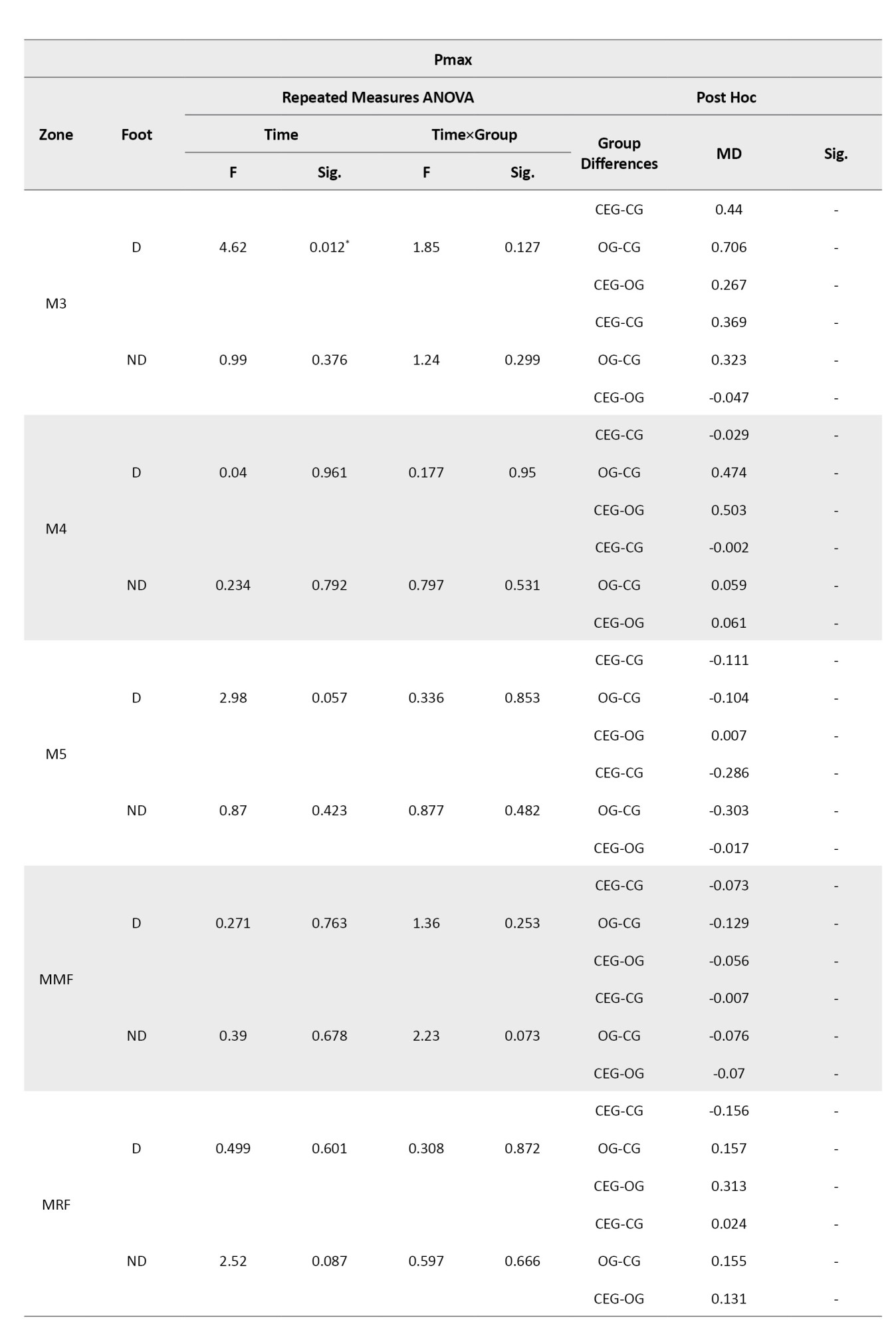
Pmax
A significant main effect of time was found in several foot zones, including the great toe (T1), toes 2–5 (T2–5), first metatarsal (M1), and third metatarsal (M3) on the D limb (all P < 0.05). Notably, CEG and OG showed significant reductions in maximum pressure at T1 compared to CG (P=0.020 and P=0.036, respectively). However, no significant time×group interaction was observed for T1, indicating a general temporal improvement. At zone T2–5, a significant time×group interaction was observed (F=42.57, P<0.001), and Bonferroni post hoc tests showed that CEG significantly differed from both OG and CG (P=0.017 and P<0.001, respectively). Similar patterns were detected in the M3 and M5 regions, where CEG demonstrated more pronounced reductions over time compared to the control group. No significant effects were observed in MF and heel regions (MH, LH), suggesting that intervention effects were localized primarily in the forefoot areas related to HV deformity.
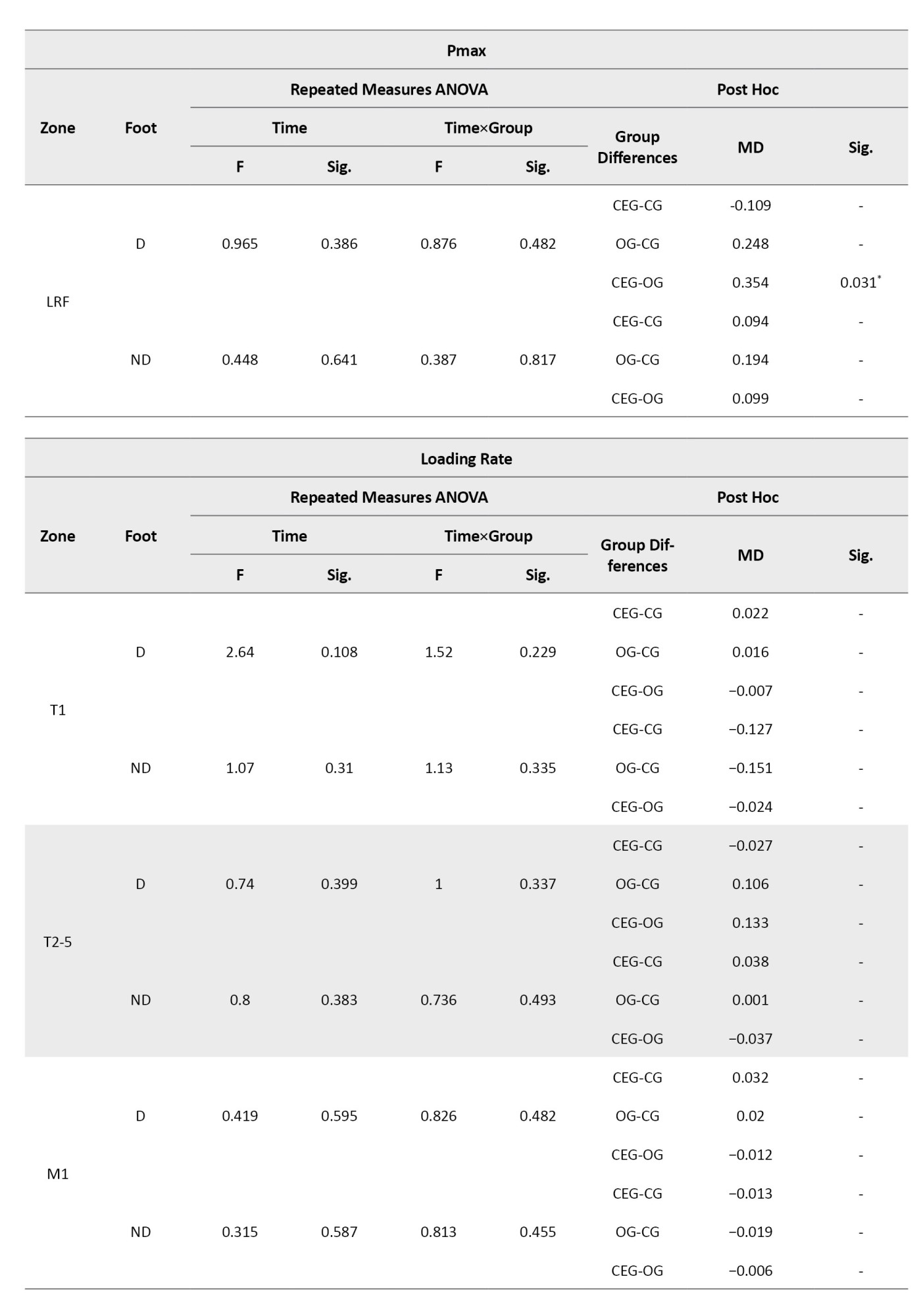
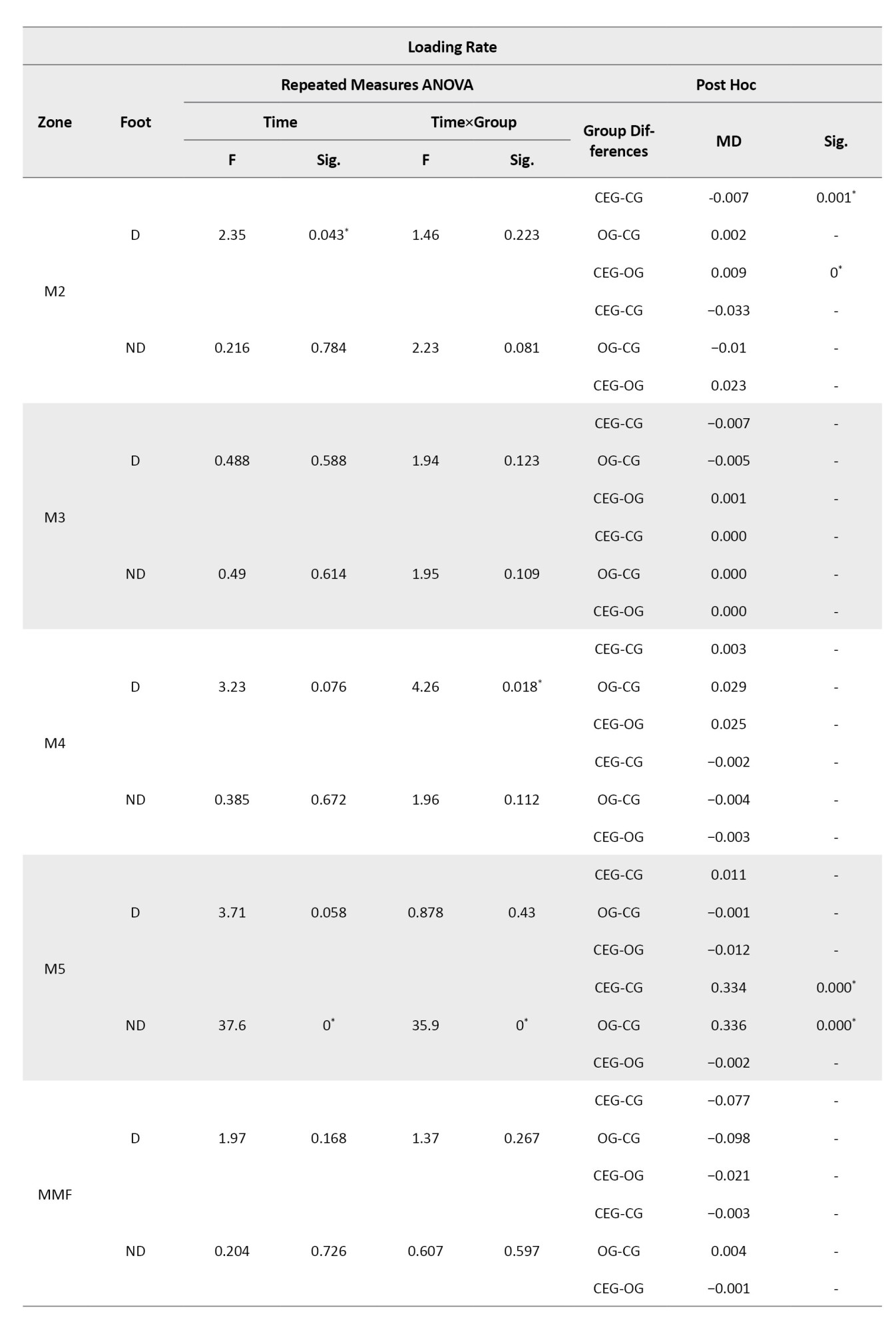
Loading rate
For loading rate, a significant main effect of time was found in zones such as M2 (D), M4 (D), and LRF (D and ND). A particularly strong time×group interaction was found in the lateral rearfoot of the D limb (LRF-D) (F=12.09, P<0.001). Bonferroni post hoc tests revealed that CEG significantly differed from CG (P<0.001) and also from OG (P=0.031), indicating the corrective exercise program had a greater impact in reducing loading rate in this zone. Additionally, significant intergroup differences were detected in the ND limb at zones M5 and LRF, with the CEG outperforming both OG and CG in reducing loading rate values (P<0.001).
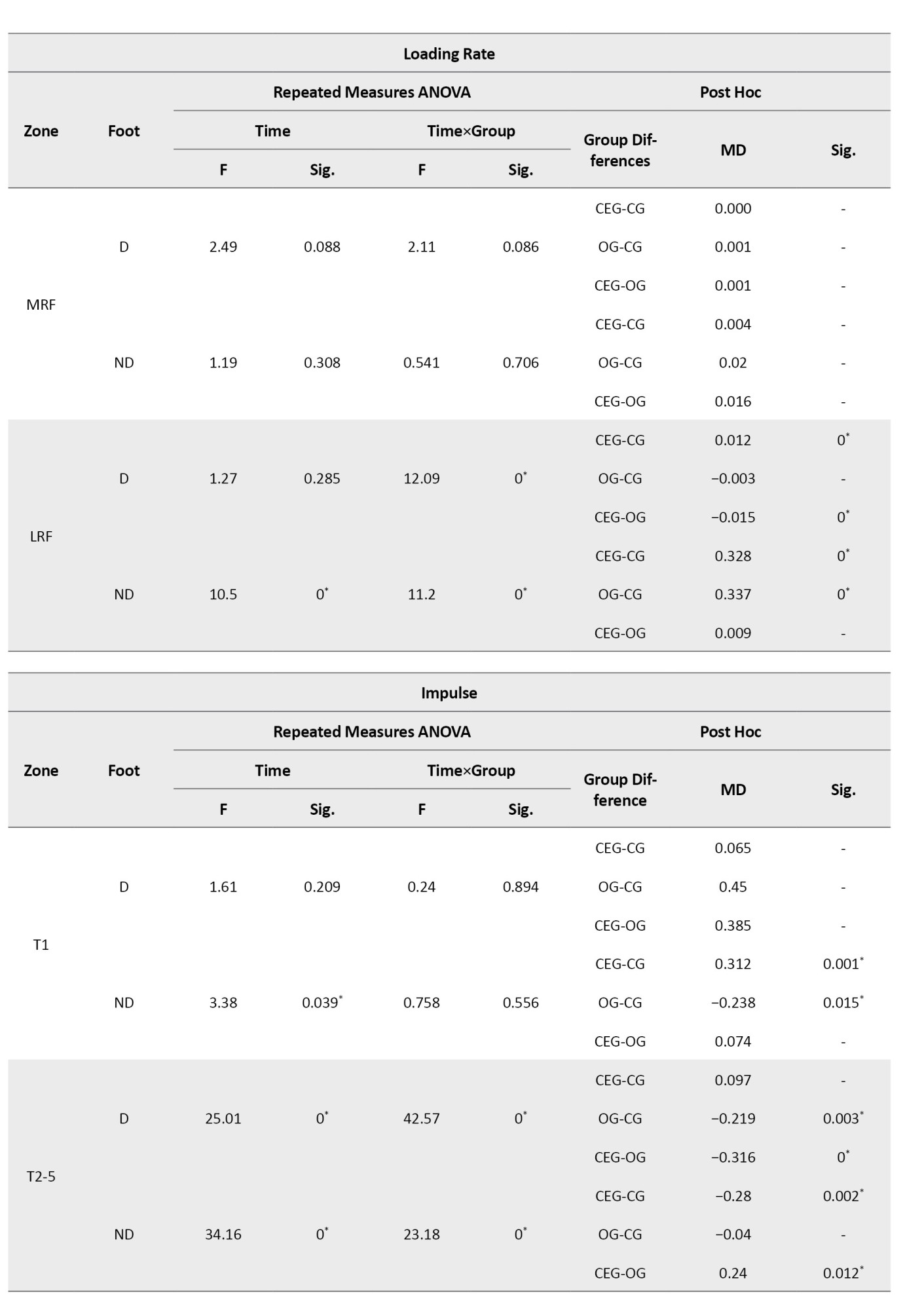
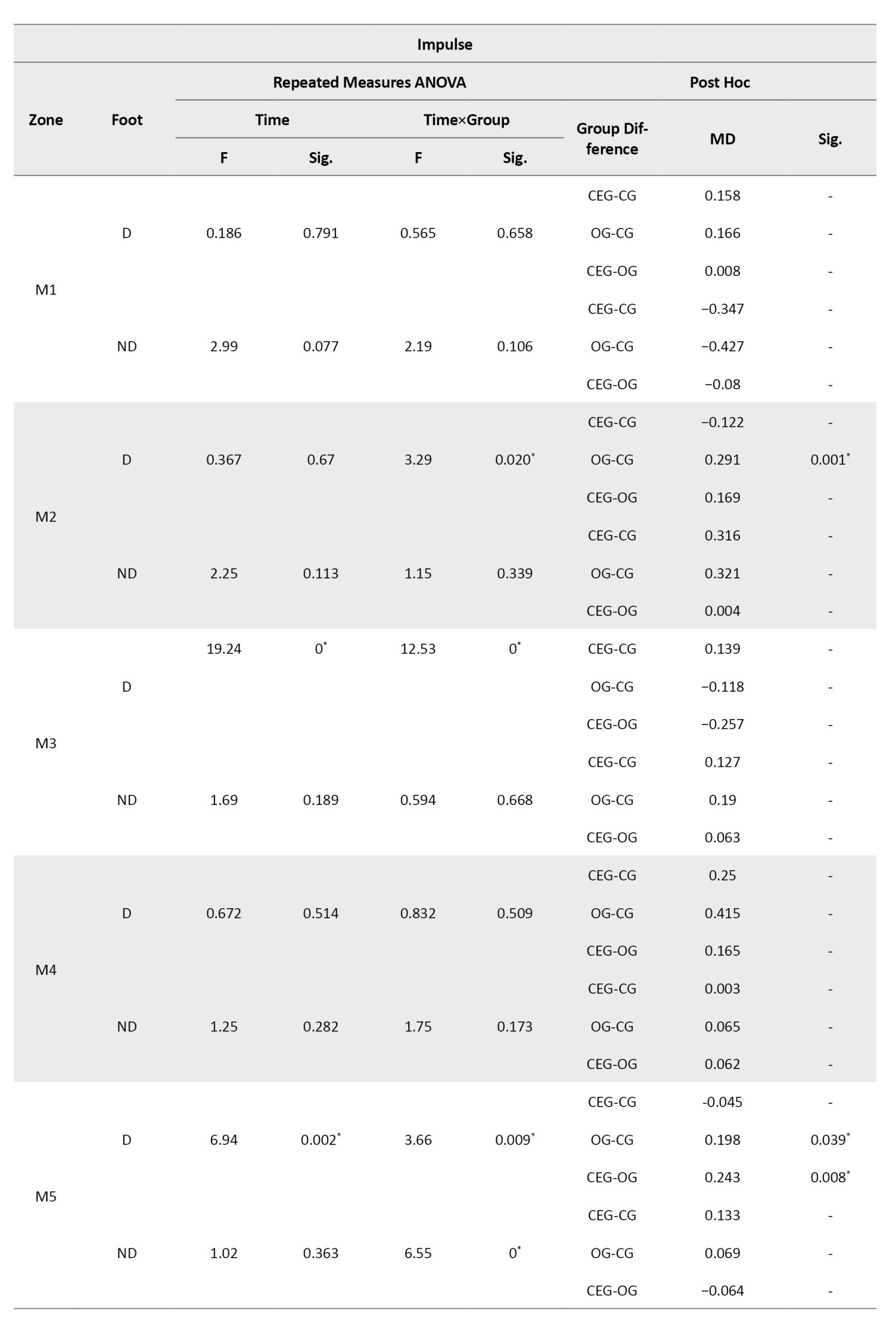
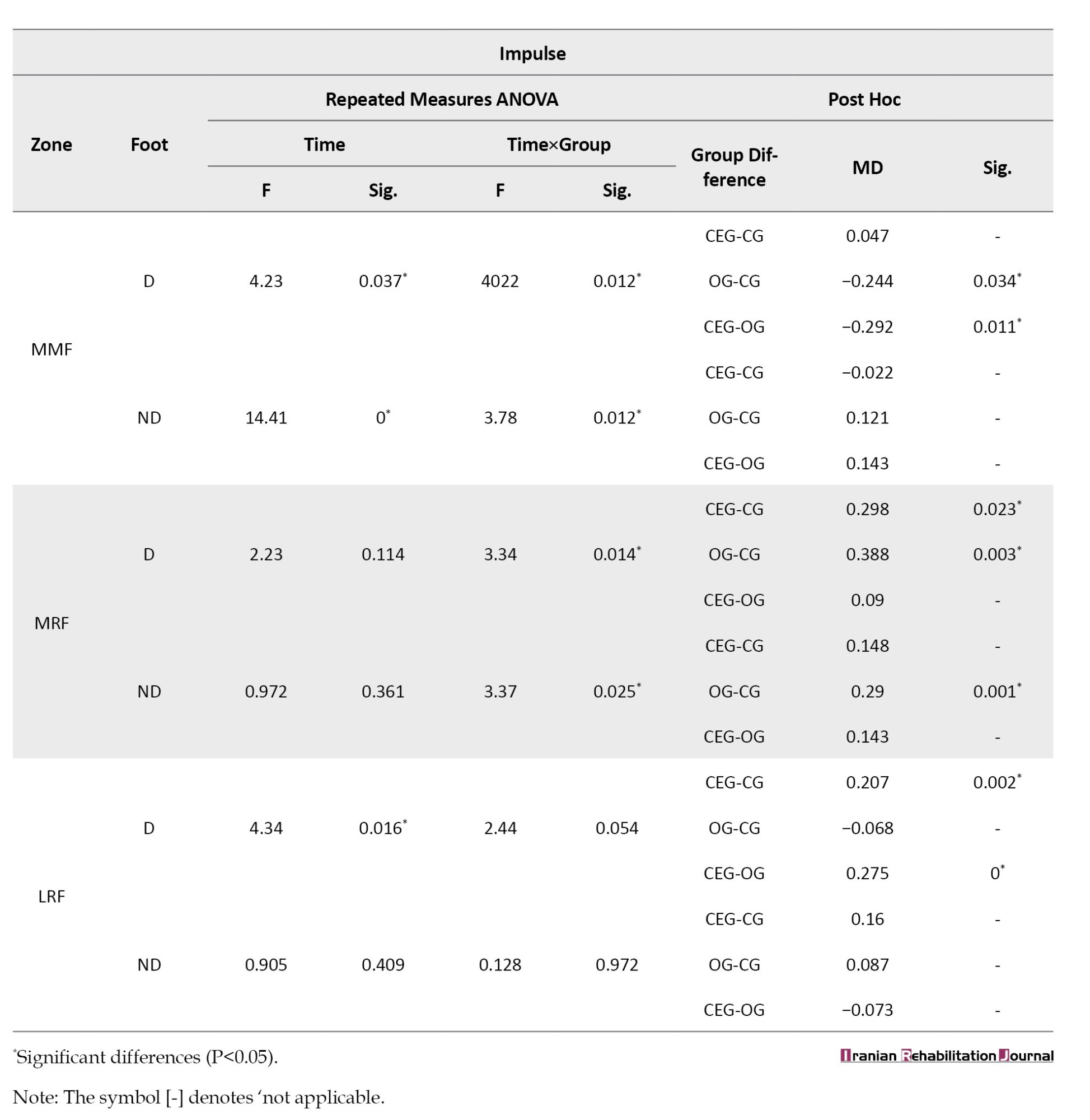
Impulse
Regarding impulse, a significant time effect was found in several forefoot and MF regions, especially T2–5, M3, M5, MMF, and MRF, with interaction effects also being statistically significant (all P<0.05). Bonferroni-adjusted comparisons revealed significant reductions in impulse in the CEG group compared to both OG and CG in zones T2–5 and M3 on both D and ND limbs. For example, at T2–5 (ND), CEG showed significantly lower impulse values compared to CG (P=0.002) and OG (P=0.012). In contrast, no significant changes were observed in MH and MF regions for impulse, highlighting that the interventions primarily affected the anterior plantar region.
Data are presented as F and P derived from repeated measures ANOVA. Post hoc comparisons were conducted using Bonferroni correction. Abbreviations: D, D foot; ND foot; CG, control group; CEG; OG, orthotic group; LRF, lateral rearfoot; MRF, medial rearfoot; MMF, medial forefoot. Bold P values indicate statistically significant differences (P<0.05).
Discussion
This study aimed to evaluate the comparative effectiveness of a 12-week corrective exercise program and orthotic intervention in altering plantar pressure-related kinetic parameters in individuals with HV. Results indicated significant time and time × group interaction effects, particularly in forefoot regions. Specifically, the CEG showed significant reductions in Pmax at the great toe, toes 2–5, and third metatarsal of the D foot compared to both the orthotic group and control group. Similarly, loading rate in the LRF-D decreased more substantially in CEG than in OG and CG. Impulse values also significantly declined in CEG across key forefoot zones in both limbs, while MF and heel regions remained largely unaffected. These results highlight the regional specificity and biomechanical impact of the corrective exercise protocol, suggesting that such targeted interventions may provide greater functional improvements in load distribution than passive orthotic support. The findings of the present study showed that both corrective exercises and orthotic interventions led to significant changes in Pmax in women with HV; however, the pattern and affected regions differed between groups. Corrective exercises resulted in pressure reductions in the hallux, second metatarsal, and LH areas, consistent with previous studies on plantar load redistribution [10, 16, 26]. In contrast, the orthotic group exhibited increased pressure at the hallux of the ND foot and decreased pressure in some metatarsal regions, indicating a redistribution of load within the foot [10, 20]. Between-group comparisons also revealed that both interventions reduced pressure at the hallux compared to the control group, but orthotics shifted load to lateral and MF areas, which may help compensate for excessive pressure but can cause increased loading in certain regions. Overall, corrective exercises were more effective in targeted reduction of forefoot pressures, whereas orthotics produced a broader but less focused pattern of load redistribution. These findings emphasize the importance of dynamic muscle training and motor relearning in improving foot biomechanics in HV.
Pmax
The findings of the present study indicate that both corrective exercise and orthotic interventions led to significant changes in Pmax in women with HV. However, the nature and location of these changes varied across groups and time points. In the CEG, significant reductions in Pmax were observed at the hallux (T1), second metatarsal (M2), and LRF of the D foot. Post hoc analyses revealed a significant reduction of 0.443 in pressure under the hallux and an increase of 0.918 under M2 after 8 weeks compared to baseline. Furthermore, an increase of 0.321 in the LH was detected between weeks 8 and 12. These results align with findings by Menz [8], who emphasized the efficacy of targeted exercise interventions in redistributing plantar loads, and Yoo [16], who found elevated pressures under the second and third metatarsals among HV patients. In contrast, the orthotic group demonstrated significant changes in different plantar regions. Maximum pressure increased at the hallux of the ND foot by 0.427 after 12 weeks and significantly decreased at M1 and M3 in the D foot (by 0.67 and 1.02, respectively). These findings are consistent with studies by Bryant [25] and Kelly [27], which reported orthoses to be effective in offloading pressure from central metatarsal heads. Galica [28] also noted reduced load beneath the hallux with orthotic use, though in the current study, an increase was observed in the ND foot, potentially due to altered gait compensation patterns. However, the present results contrast with Hsien-Yu Chen’s findings, which indicated reductions in heel pressure following orthotic intervention—an effect not replicated here. Inter-group comparisons further revealed that both CEG and OG achieved significant reductions in maximum pressure at the hallux compared to the CG (reductions of 0.469 and 0.411, respectively). Notably, orthotic intervention led to an increase in pressure under T2–5 by 0.207 compared to CEG, and also caused a notable increase at M1 (0.926) and the LRF (0.357), suggesting that the passive support offered by orthoses may redistribute load toward other plantar zones rather than reduce it overall. This redistribution effect may explain the increased pressure in non-targeted regions, supporting prior conclusions by Menz et al. [10], who observed orthoses to significantly affect MTP load in women with HV. Overall, the corrective exercise protocol appeared to achieve more consistent and targeted reductions in forefoot plantar pressure—especially under the hallux and metatarsals—while orthotic devices demonstrated a mixed pattern of load redistribution, with some increases observed in lateral and mid-forefoot zones. These outcomes underscore the biomechanical benefits of dynamic muscular re-education in mitigating the excessive forefoot load commonly seen in HV pathology.
Loading rate
The results of the present study demonstrate that both corrective exercise and orthotic interventions have significant yet distinct effects on the loading rate across specific plantar regions in women with HV. In the CEG, significant reductions in loading rate were observed in the ND foot at the second metatarsal (M2) and MF, and in the lateral rear foot of both feet. Post hoc analysis revealed a reduction of 0.018 at M2 in the ND foot both compared to pre-intervention and to week 8, indicating a progressive adaptation over time. The MF showed a smaller but significant decrease of 0.003 after 12 weeks. Interestingly, the LH in the D foot exhibited a significant increase of 0.004 from pre-intervention to week 8, and the same trend persisted between weeks 8 and 12. In contrast, the LH of the ND foot showed a significant reduction (0.016) at week 8 compared to baseline. These findings partially align with those of Hutton [29], who reported that in HV patients, mechanical load tends to shift laterally, and corrective exercise may assist in restoring a more balanced plantar load distribution. In the current study, this lateral load shift appears to have been reversed in the ND foot but not in the D one—suggesting possible asymmetry in neuromuscular adaptation or functional dominance effects. In the OG, loading rate reductions were observed at M2 and M4 of the D foot and at the LH in both feet. Specifically, post-intervention analysis showed that the loading rate at M2 and M4 reduced by 0.007 and 0.065, respectively, after 12 weeks. Furthermore, the LRF loading rate decreased by 0.019 in both feet after both 8 and 12 weeks. These findings are consistent with the results of Hutton [29], which reported abnormal forefoot and MF loading in HV patients, and suggested that orthotic use may effectively mitigate these abnormal pressures by redistributing loads across the plantar surface. Between-group comparisons provided further insights. The CEG showed a significant reduction in loading rate at M2 in the D foot compared to both the CG (by 0.007) and the orthotic group (where loading increased by 0.009 relative to CEG). For the fifth metatarsal in the ND foot (M5), both interventions unexpectedly resulted in increased loading rates—0.334 for CEG and 0.336 for OG—suggesting a compensatory shift in load toward the lateral forefoot. Additionally, corrective exercise led to a significant reduction in LH loading rate (by 0.012 in the D and 0.328 in the ND foot), while orthotics showed a slightly greater reduction in the ND foot (0.337), but an increase of 0.015 in the D foot compared to CEG. These findings suggest that corrective exercises are more effective in reducing localized loading rates, particularly in the medial and MF regions, while orthotic devices may offer broader but less targeted load redistribution, sometimes at the cost of increased loading in other areas (e.g. lateral forefoot). The increase in M5 loading in both groups also raises questions about secondary compensations that may arise from each intervention. Overall, while both interventions demonstrated positive effects on plantar load modulation, corrective exercises showed more specific improvements in targeted regions (M2, MF, and LRF), whereas orthotic interventions were more generalized but may risk compensatory increases elsewhere. These results highlight the importance of individualized intervention strategies in patients with HV, especially when targeting biomechanical risk factors for further deformity progression or discomfort.
Impulse
Repeated measures ANOVA on impulse within the CEG indicated significant effects of the 8- and 12-week interventions on impulse in the second to fifth toes of both feet, the third metatarsal head in the D foot, and the MF region in the ND foot. Post hoc comparisons showed significant decreases in impulse at the second to fifth toes of the D foot after 8 weeks (0.512 decrease) and 12 weeks (0.505 decrease) compared to pre-intervention. Similarly, in the ND foot, impulse decreased by 0.125 after 8 weeks and further by 0.074 at 12 weeks compared to 8 weeks. A significant reduction of 0.601 was observed in the third metatarsal head of the D foot after 12 weeks. However, impulse increased in the MF region of the ND foot by 0.371 after 8 weeks and 0.386 after 12 weeks. These results partially concur with Collan [30], which reported reductions in impulse in the D foot following corrective exercises. However, the increase in MF impulse in the ND foot was not consistent with previous findings, suggesting complexity in biomechanical adaptations between limbs. In the orthotic group, 8- and 12-week use significantly influenced impulse in the hallux and toes two to five, the third metatarsal head in the D foot, the second metatarsal head in the ND foot, and the MF in both feet. Post hoc analyses revealed a significant decrease in impulse in the hallux of the D foot after 12 weeks (0.034 decrease). However, toes two to five in the D foot showed significant increases at 12 weeks relative to pre-intervention (1.16 increase) and 8 weeks (2.0 increase). The second metatarsal head of the ND foot showed a 0.022 decrease after 8 weeks. Impulse in the third metatarsal head of the D foot decreased by 0.36 after 12 weeks. MF impulse increased significantly in both feet after intervention, with larger increases after 12 weeks (up to 0.407 in the D foot and 0.292 in the ND foot). These findings align with Galica [28] and Wen [31], who documented decreases in impulse in the hallux and MF regions following orthotic use. However, they conflict with Aiyer [24], who reported increased impulse in the MH and decreased impulse in the LH and forefoot. Between-group comparisons demonstrated significant differences in impulse across multiple foot regions, including the hallux of the ND foot, toes two to five in both feet, the second and third metatarsal heads of the D foot, the fifth metatarsal head of both feet, the MF, and the medial and LH regions. Corrective exercises significantly reduced impulse in the hallux of the ND foot by 0.312, while orthotics increased it by 0.238. Orthotic intervention increased impulse in toes two to five of the D foot by 0.219 compared to controls and by 0.316 compared to corrective exercises. Conversely, corrective exercises increased impulse in toes two to five of the ND foot by 0.28 compared to controls, while orthotics decreased it by 0.24 compared to corrective exercises. Both interventions reduced impulse in the MH of the D foot (corrective exercises by 0.298 and orthotics by 0.388) and LH (corrective exercises by 0.207). Orthotics also increased impulse in the MH of the ND foot by 0.29. Overall, both corrective exercises and orthotics effectively reduced impulse in medial and LH regions of the D foot, with greater effect seen from exercises. Orthotics exerted stronger effects in MF impulse reduction, while exercises more substantially decreased impulse in toes two to five of the ND foot and the hallux of the ND foot compared to controls.
Conclusion
In summary, both corrective exercise and orthotic interventions significantly modulate plantar pressure parameters in women with HV. However, corrective exercises provide more focused and consistent reductions in forefoot loading, particularly in the hallux and metatarsal heads, thereby offering superior biomechanical benefits. Orthotic devices contribute to broader load redistribution but may induce compensatory pressure increases in adjacent foot regions. Clinicians should consider prioritizing dynamic, muscle-based rehabilitation approaches to address the multifactorial nature of HV, while orthotic use should be tailored individually to avoid unintended biomechanical consequences. Further longitudinal research is warranted to assess the long-term clinical impacts of these interventions.
Study limitations and future directions
Despite the promising findings, this study has several limitations that should be acknowledged. First, the sample comprised solely of female participants, which limits the generalizability of results to males or mixed-gender populations. Second, the relatively short intervention duration of 12 weeks may not be sufficient to capture long-term biomechanical adaptations, symptom relief, or functional improvements associated with HV treatment. Third, the study did not assess clinical outcomes such as pain intensity, quality of life, or gait kinematics, which are important for evaluating the overall effectiveness of interventions. Additionally, the lack of follow-up evaluations limits the understanding of the sustainability of the observed biomechanical changes. Future research should aim to include larger, more diverse cohorts, longer follow-up periods, and comprehensive clinical outcome measures to better elucidate the therapeutic benefits and potential drawbacks of corrective exercise and orthotic interventions in HV management.
Study implications
The findings suggest that corrective exercise programs should be considered a primary conservative treatment option for HV to specifically address abnormal plantar loading patterns and improve foot function. Orthotic devices can serve as adjuncts to redistribute plantar loads, but clinicians should monitor for potential compensatory load increases in non-target areas. Rehabilitation strategies combining dynamic muscle training with orthotic support may optimize clinical outcomes.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Research Ethics Committee of the Sport Sciences Research Institute, Tehran, Iran (Code: IR.SSRC.REC.1402.109). and adhered to the principles outlined in the Declaration of Helsinki.
Funding
This study did not receive any financial support from funding organizations in the public, private, or non-profit domains.
Authors' contributions
Study design: Ali Fatahi; Data collection: Laya Abdolhosseini; and Razieh Yousefian Molla; Writing: Ali Fatahi and Razieh Yousefian Molla.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The Authors would like to express their best thanks to all the participants of the research.
Data collection was conducted by a highly skilled operator specialized in biomechanics and rehabilitation, ensuring precise and reliable measurements. Invalid or noisy data were excluded following thorough quality checks. Each measurement was repeated three times, and the best value was selected for analysis to enhance reliability. Test-retest reliability for plantar pressure measurements with the RS Scan system has been reported as high in previous research [23].
All procedures were conducted following ethical approval and with participants’ informed consent, adhering to the principles of the Declaration of Helsinki.
Variables and outcome measures
The independent variable in this randomized controlled trial was the intervention group, consisting of three groups: CEG, OG, and CG. The inclusion of the CG group was essential to serve as a baseline, allowing comparison of the effects of CEG and OG interventions against the natural progression without treatment.
The dependent variables comprised biomechanical kinetic parameters of plantar pressure, measured dynamically during the stance phase of gait—a critical period for foot loading and force transmission [22]. These variables included:
Maximum plantar pressure (Pmax)
Defined as the highest-pressure value recorded in Newtons per square centimeter (N/cm²) by any sensor within the designated foot regions during stance, reflecting peak load areas relevant in HV pathology [24]. Calculated by Equation 1:
1. Pmax=max(P1, P2, ..., Pn)
Loading rate (R):
The rate of force application upon foot-ground contact, indicative of mechanical stress and potential injury risk. It is calculated as the ratio of ground reaction force (F) to the contact area (A) [24] (Equation 2):
Impulse (J):
The integral of force throughout application during stance, representing total momentum transfer [24] (Equation 3):
Measurements were obtained using the RS scan foot pressure system (RS scan international, Belgium) at a sampling frequency of 300 Hz during walking trials along a 10-m walkway. The plantar surface was segmented into ten anatomical regions—great toe (T1), toes 2–5 (T2–5), first through fifth metatarsals (M1–M5), MF, MH, and LH—to enable detailed regional pressure analysis [25].
Statistical analysis
Descriptive statistics, including means and standard deviations, were calculated to summarize participant demographics and outcome variables. The Shapiro-Wilk test was used to assess data normality, and Levene’s test evaluated homogeneity of variances. For variables with normal distribution, inferential analysis was performed using a repeated measures general linear model (GLM) to examine the effects of study groups (CEG, OG, and CG), time (baseline, week 8, and week 12), and their interaction on the dependent variables. Post-hoc pairwise comparisons with Bonferroni correction were conducted to identify significant differences between groups and time points. All analyses were performed using SPSS software, version 26 (IBM Corp., New York, USA), with a significance level set at P<0.05. Missing data were not present, as all participants completed the study.
Results
Participant flow and baseline characteristics
All 45 participants (15 per group) completed the study without dropping out. Baseline demographic and kinetic parameters were comparable across groups (P>0.05), confirming successful randomization. Baseline demographic and clinical characteristics of participants are presented in Table 1.
No statistically significant differences were found among the CG, CEG, and OG regarding age, weight, height, and BMI at baseline (all P>0.05). This finding indicates that randomization successfully achieved comparable groups before the intervention.
Inferential statistics
To examine the effects of corrective exercises and orthotic interventions on kinetic parameters, a repeated measures ANOVA was conducted for each dependent variable—Pmax, loading rate, and impulse—across different foot zones and time points (baseline, week 8, and week 12). Analyses were performed for both the dominant (D) and non-dominant (ND) limbs. Where significant main or interaction effects were observed, Bonferroni-adjusted post hoc comparisons were used to identify specific intergroup differences. A detailed summary of these results is presented in Table 2.
Pmax
A significant main effect of time was found in several foot zones, including the great toe (T1), toes 2–5 (T2–5), first metatarsal (M1), and third metatarsal (M3) on the D limb (all P < 0.05). Notably, CEG and OG showed significant reductions in maximum pressure at T1 compared to CG (P=0.020 and P=0.036, respectively). However, no significant time×group interaction was observed for T1, indicating a general temporal improvement. At zone T2–5, a significant time×group interaction was observed (F=42.57, P<0.001), and Bonferroni post hoc tests showed that CEG significantly differed from both OG and CG (P=0.017 and P<0.001, respectively). Similar patterns were detected in the M3 and M5 regions, where CEG demonstrated more pronounced reductions over time compared to the control group. No significant effects were observed in MF and heel regions (MH, LH), suggesting that intervention effects were localized primarily in the forefoot areas related to HV deformity.
Loading rate
For loading rate, a significant main effect of time was found in zones such as M2 (D), M4 (D), and LRF (D and ND). A particularly strong time×group interaction was found in the lateral rearfoot of the D limb (LRF-D) (F=12.09, P<0.001). Bonferroni post hoc tests revealed that CEG significantly differed from CG (P<0.001) and also from OG (P=0.031), indicating the corrective exercise program had a greater impact in reducing loading rate in this zone. Additionally, significant intergroup differences were detected in the ND limb at zones M5 and LRF, with the CEG outperforming both OG and CG in reducing loading rate values (P<0.001).
Impulse
Regarding impulse, a significant time effect was found in several forefoot and MF regions, especially T2–5, M3, M5, MMF, and MRF, with interaction effects also being statistically significant (all P<0.05). Bonferroni-adjusted comparisons revealed significant reductions in impulse in the CEG group compared to both OG and CG in zones T2–5 and M3 on both D and ND limbs. For example, at T2–5 (ND), CEG showed significantly lower impulse values compared to CG (P=0.002) and OG (P=0.012). In contrast, no significant changes were observed in MH and MF regions for impulse, highlighting that the interventions primarily affected the anterior plantar region.
Data are presented as F and P derived from repeated measures ANOVA. Post hoc comparisons were conducted using Bonferroni correction. Abbreviations: D, D foot; ND foot; CG, control group; CEG; OG, orthotic group; LRF, lateral rearfoot; MRF, medial rearfoot; MMF, medial forefoot. Bold P values indicate statistically significant differences (P<0.05).
Discussion
This study aimed to evaluate the comparative effectiveness of a 12-week corrective exercise program and orthotic intervention in altering plantar pressure-related kinetic parameters in individuals with HV. Results indicated significant time and time × group interaction effects, particularly in forefoot regions. Specifically, the CEG showed significant reductions in Pmax at the great toe, toes 2–5, and third metatarsal of the D foot compared to both the orthotic group and control group. Similarly, loading rate in the LRF-D decreased more substantially in CEG than in OG and CG. Impulse values also significantly declined in CEG across key forefoot zones in both limbs, while MF and heel regions remained largely unaffected. These results highlight the regional specificity and biomechanical impact of the corrective exercise protocol, suggesting that such targeted interventions may provide greater functional improvements in load distribution than passive orthotic support. The findings of the present study showed that both corrective exercises and orthotic interventions led to significant changes in Pmax in women with HV; however, the pattern and affected regions differed between groups. Corrective exercises resulted in pressure reductions in the hallux, second metatarsal, and LH areas, consistent with previous studies on plantar load redistribution [10, 16, 26]. In contrast, the orthotic group exhibited increased pressure at the hallux of the ND foot and decreased pressure in some metatarsal regions, indicating a redistribution of load within the foot [10, 20]. Between-group comparisons also revealed that both interventions reduced pressure at the hallux compared to the control group, but orthotics shifted load to lateral and MF areas, which may help compensate for excessive pressure but can cause increased loading in certain regions. Overall, corrective exercises were more effective in targeted reduction of forefoot pressures, whereas orthotics produced a broader but less focused pattern of load redistribution. These findings emphasize the importance of dynamic muscle training and motor relearning in improving foot biomechanics in HV.
Pmax
The findings of the present study indicate that both corrective exercise and orthotic interventions led to significant changes in Pmax in women with HV. However, the nature and location of these changes varied across groups and time points. In the CEG, significant reductions in Pmax were observed at the hallux (T1), second metatarsal (M2), and LRF of the D foot. Post hoc analyses revealed a significant reduction of 0.443 in pressure under the hallux and an increase of 0.918 under M2 after 8 weeks compared to baseline. Furthermore, an increase of 0.321 in the LH was detected between weeks 8 and 12. These results align with findings by Menz [8], who emphasized the efficacy of targeted exercise interventions in redistributing plantar loads, and Yoo [16], who found elevated pressures under the second and third metatarsals among HV patients. In contrast, the orthotic group demonstrated significant changes in different plantar regions. Maximum pressure increased at the hallux of the ND foot by 0.427 after 12 weeks and significantly decreased at M1 and M3 in the D foot (by 0.67 and 1.02, respectively). These findings are consistent with studies by Bryant [25] and Kelly [27], which reported orthoses to be effective in offloading pressure from central metatarsal heads. Galica [28] also noted reduced load beneath the hallux with orthotic use, though in the current study, an increase was observed in the ND foot, potentially due to altered gait compensation patterns. However, the present results contrast with Hsien-Yu Chen’s findings, which indicated reductions in heel pressure following orthotic intervention—an effect not replicated here. Inter-group comparisons further revealed that both CEG and OG achieved significant reductions in maximum pressure at the hallux compared to the CG (reductions of 0.469 and 0.411, respectively). Notably, orthotic intervention led to an increase in pressure under T2–5 by 0.207 compared to CEG, and also caused a notable increase at M1 (0.926) and the LRF (0.357), suggesting that the passive support offered by orthoses may redistribute load toward other plantar zones rather than reduce it overall. This redistribution effect may explain the increased pressure in non-targeted regions, supporting prior conclusions by Menz et al. [10], who observed orthoses to significantly affect MTP load in women with HV. Overall, the corrective exercise protocol appeared to achieve more consistent and targeted reductions in forefoot plantar pressure—especially under the hallux and metatarsals—while orthotic devices demonstrated a mixed pattern of load redistribution, with some increases observed in lateral and mid-forefoot zones. These outcomes underscore the biomechanical benefits of dynamic muscular re-education in mitigating the excessive forefoot load commonly seen in HV pathology.
Loading rate
The results of the present study demonstrate that both corrective exercise and orthotic interventions have significant yet distinct effects on the loading rate across specific plantar regions in women with HV. In the CEG, significant reductions in loading rate were observed in the ND foot at the second metatarsal (M2) and MF, and in the lateral rear foot of both feet. Post hoc analysis revealed a reduction of 0.018 at M2 in the ND foot both compared to pre-intervention and to week 8, indicating a progressive adaptation over time. The MF showed a smaller but significant decrease of 0.003 after 12 weeks. Interestingly, the LH in the D foot exhibited a significant increase of 0.004 from pre-intervention to week 8, and the same trend persisted between weeks 8 and 12. In contrast, the LH of the ND foot showed a significant reduction (0.016) at week 8 compared to baseline. These findings partially align with those of Hutton [29], who reported that in HV patients, mechanical load tends to shift laterally, and corrective exercise may assist in restoring a more balanced plantar load distribution. In the current study, this lateral load shift appears to have been reversed in the ND foot but not in the D one—suggesting possible asymmetry in neuromuscular adaptation or functional dominance effects. In the OG, loading rate reductions were observed at M2 and M4 of the D foot and at the LH in both feet. Specifically, post-intervention analysis showed that the loading rate at M2 and M4 reduced by 0.007 and 0.065, respectively, after 12 weeks. Furthermore, the LRF loading rate decreased by 0.019 in both feet after both 8 and 12 weeks. These findings are consistent with the results of Hutton [29], which reported abnormal forefoot and MF loading in HV patients, and suggested that orthotic use may effectively mitigate these abnormal pressures by redistributing loads across the plantar surface. Between-group comparisons provided further insights. The CEG showed a significant reduction in loading rate at M2 in the D foot compared to both the CG (by 0.007) and the orthotic group (where loading increased by 0.009 relative to CEG). For the fifth metatarsal in the ND foot (M5), both interventions unexpectedly resulted in increased loading rates—0.334 for CEG and 0.336 for OG—suggesting a compensatory shift in load toward the lateral forefoot. Additionally, corrective exercise led to a significant reduction in LH loading rate (by 0.012 in the D and 0.328 in the ND foot), while orthotics showed a slightly greater reduction in the ND foot (0.337), but an increase of 0.015 in the D foot compared to CEG. These findings suggest that corrective exercises are more effective in reducing localized loading rates, particularly in the medial and MF regions, while orthotic devices may offer broader but less targeted load redistribution, sometimes at the cost of increased loading in other areas (e.g. lateral forefoot). The increase in M5 loading in both groups also raises questions about secondary compensations that may arise from each intervention. Overall, while both interventions demonstrated positive effects on plantar load modulation, corrective exercises showed more specific improvements in targeted regions (M2, MF, and LRF), whereas orthotic interventions were more generalized but may risk compensatory increases elsewhere. These results highlight the importance of individualized intervention strategies in patients with HV, especially when targeting biomechanical risk factors for further deformity progression or discomfort.
Impulse
Repeated measures ANOVA on impulse within the CEG indicated significant effects of the 8- and 12-week interventions on impulse in the second to fifth toes of both feet, the third metatarsal head in the D foot, and the MF region in the ND foot. Post hoc comparisons showed significant decreases in impulse at the second to fifth toes of the D foot after 8 weeks (0.512 decrease) and 12 weeks (0.505 decrease) compared to pre-intervention. Similarly, in the ND foot, impulse decreased by 0.125 after 8 weeks and further by 0.074 at 12 weeks compared to 8 weeks. A significant reduction of 0.601 was observed in the third metatarsal head of the D foot after 12 weeks. However, impulse increased in the MF region of the ND foot by 0.371 after 8 weeks and 0.386 after 12 weeks. These results partially concur with Collan [30], which reported reductions in impulse in the D foot following corrective exercises. However, the increase in MF impulse in the ND foot was not consistent with previous findings, suggesting complexity in biomechanical adaptations between limbs. In the orthotic group, 8- and 12-week use significantly influenced impulse in the hallux and toes two to five, the third metatarsal head in the D foot, the second metatarsal head in the ND foot, and the MF in both feet. Post hoc analyses revealed a significant decrease in impulse in the hallux of the D foot after 12 weeks (0.034 decrease). However, toes two to five in the D foot showed significant increases at 12 weeks relative to pre-intervention (1.16 increase) and 8 weeks (2.0 increase). The second metatarsal head of the ND foot showed a 0.022 decrease after 8 weeks. Impulse in the third metatarsal head of the D foot decreased by 0.36 after 12 weeks. MF impulse increased significantly in both feet after intervention, with larger increases after 12 weeks (up to 0.407 in the D foot and 0.292 in the ND foot). These findings align with Galica [28] and Wen [31], who documented decreases in impulse in the hallux and MF regions following orthotic use. However, they conflict with Aiyer [24], who reported increased impulse in the MH and decreased impulse in the LH and forefoot. Between-group comparisons demonstrated significant differences in impulse across multiple foot regions, including the hallux of the ND foot, toes two to five in both feet, the second and third metatarsal heads of the D foot, the fifth metatarsal head of both feet, the MF, and the medial and LH regions. Corrective exercises significantly reduced impulse in the hallux of the ND foot by 0.312, while orthotics increased it by 0.238. Orthotic intervention increased impulse in toes two to five of the D foot by 0.219 compared to controls and by 0.316 compared to corrective exercises. Conversely, corrective exercises increased impulse in toes two to five of the ND foot by 0.28 compared to controls, while orthotics decreased it by 0.24 compared to corrective exercises. Both interventions reduced impulse in the MH of the D foot (corrective exercises by 0.298 and orthotics by 0.388) and LH (corrective exercises by 0.207). Orthotics also increased impulse in the MH of the ND foot by 0.29. Overall, both corrective exercises and orthotics effectively reduced impulse in medial and LH regions of the D foot, with greater effect seen from exercises. Orthotics exerted stronger effects in MF impulse reduction, while exercises more substantially decreased impulse in toes two to five of the ND foot and the hallux of the ND foot compared to controls.
Conclusion
In summary, both corrective exercise and orthotic interventions significantly modulate plantar pressure parameters in women with HV. However, corrective exercises provide more focused and consistent reductions in forefoot loading, particularly in the hallux and metatarsal heads, thereby offering superior biomechanical benefits. Orthotic devices contribute to broader load redistribution but may induce compensatory pressure increases in adjacent foot regions. Clinicians should consider prioritizing dynamic, muscle-based rehabilitation approaches to address the multifactorial nature of HV, while orthotic use should be tailored individually to avoid unintended biomechanical consequences. Further longitudinal research is warranted to assess the long-term clinical impacts of these interventions.
Study limitations and future directions
Despite the promising findings, this study has several limitations that should be acknowledged. First, the sample comprised solely of female participants, which limits the generalizability of results to males or mixed-gender populations. Second, the relatively short intervention duration of 12 weeks may not be sufficient to capture long-term biomechanical adaptations, symptom relief, or functional improvements associated with HV treatment. Third, the study did not assess clinical outcomes such as pain intensity, quality of life, or gait kinematics, which are important for evaluating the overall effectiveness of interventions. Additionally, the lack of follow-up evaluations limits the understanding of the sustainability of the observed biomechanical changes. Future research should aim to include larger, more diverse cohorts, longer follow-up periods, and comprehensive clinical outcome measures to better elucidate the therapeutic benefits and potential drawbacks of corrective exercise and orthotic interventions in HV management.
Study implications
The findings suggest that corrective exercise programs should be considered a primary conservative treatment option for HV to specifically address abnormal plantar loading patterns and improve foot function. Orthotic devices can serve as adjuncts to redistribute plantar loads, but clinicians should monitor for potential compensatory load increases in non-target areas. Rehabilitation strategies combining dynamic muscle training with orthotic support may optimize clinical outcomes.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Research Ethics Committee of the Sport Sciences Research Institute, Tehran, Iran (Code: IR.SSRC.REC.1402.109). and adhered to the principles outlined in the Declaration of Helsinki.
Funding
This study did not receive any financial support from funding organizations in the public, private, or non-profit domains.
Authors' contributions
Study design: Ali Fatahi; Data collection: Laya Abdolhosseini; and Razieh Yousefian Molla; Writing: Ali Fatahi and Razieh Yousefian Molla.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The Authors would like to express their best thanks to all the participants of the research.
References
- Kim EJ, Shin HS, Takatori N, Yoo HJ, Cho YJ, Yoo WJ, et al. Inter-segmental foot kinematics during gait in elderly females according to the severity of hallux valgus. Journal of Orthopaedic Research. 2020; 38(11):2409-18. [DOI:10.1002/jor.24657] [PMID]
- Buddhadev HH, Barbee CE. Redistribution of joint moments and work in older women with and without hallux valgus at two walking speeds. Gait & Posture. 2020; 77:112-7. [DOI:10.1016/j.gaitpost.2020.01.023] [PMID]
- Watanabe K, Ikeda Y, Suzuki D, Teramoto A, Kobayashi T, Suzuki T, et al. Three-dimensional analysis of tarsal bone response to axial loading in patients with hallux valgus and normal feet. Clinical Biomechanics. 2017; 42:65-9. [DOI:10.1016/j.clinbiomech.2017.01.012] [PMID]
- Nix S, Smith M, Vicenzino B. Prevalence of hallux valgus in the general population: A systematic review and meta-analysis. Journal of Foot and Ankle Research. 2010; 3(1):21. [DOI:10.1186/1757-1146-3-21] [PMID]
- Cai Y, Song Y, He M, He W, Zhong X, Wen H, et al. Global prevalence and incidence of hallux valgus: A systematic review and meta-analysis. Journal of Foot and Ankle Research. 2023; 16(1):63. [DOI:10.1186/s13047-023-00661-9] [PMID]
- Menz HB, Roddy E, Thomas E, Croft PR. Impact of hallux valgus severity on general and foot-specific health-related quality of life. Arthritis Care & Research. 2011; 63(3):396-404. [DOI:10.1002/acr.20396] [PMID]
- Nix SE, Vicenzino BT, Collins NJ, Smith MD. Gait parameters associated with hallux valgus: A systematic review. Journal of Foot and Ankle Research. 2013; 6(1):9. [DOI:10.1186/1757-1146-6-9] [PMID]
- Menz HB, Lim PQ, Hurn SE, Mickle KJ, Buldt AK, Cotchett MP, et al. Footwear, foot orthoses and strengthening exercises for the non-surgical management of hallux valgus: Protocol for a randomised pilot and feasibility trial. Journal of Foot and Ankle Research. 2022; 15(1):45. [DOI:10.1186/s13047-022-00553-4] [PMID]
- Seidenstein AH, Torrez TW, Andrews NA, Patch DA, Conklin MJ, Shah A. Pediatric hallux valgus: An overview of history, examination, conservative, and surgical management. Paediatrics & Child Health. 2022; 27(2):75-81. [DOI:10.1093/pch/pxab074] [PMID]
- Menz HB, Lim PQ, Hurn SE, Mickle KJ, Buldt AK, Cotchett MP, et al. Effectiveness of footwear and foot orthoses in reducing medial metatarsophalangeal joint pressure in women with hallux valgus. Gait & Posture. 2024; 111:156-61. [DOI:10.1016/j.gaitpost.2024.04.021] [PMID]
- Tarantino D, Palermi S, Sirico F, Corrado B. Hallux valgus deformity: Treatment options, post-operative management, and return to sport. Journal of Human Sport & Exercise. 2021; 16. [DOI:10.14198/jhse.2021.16.Proc4.14]
- Bischoff A, Logan D. First metatarsophalangeal joint arthrodesis for hallux valgus in a patient with preaxial polydactyly and triphalangeal hallux. Foot & Ankle Surgery: Techniques, Reports & Cases. 2022; 2(1):100158. [DOI:10.1016/j.fastrc.2022.100158]
- Kim MH, Kwon OY, Kim SH, Jung DY. Comparison of muscle activities of abductor hallucis and adductor hallucis between the short foot and toe-spread-out exercises in subjects with mild hallux valgus. Journal of Back and Musculoskeletal Rehabilitation. 2013; 26(2):163-8. [DOI:10.3233/BMR-2012-00363] [PMID]
- Hurn SE, Vicenzino BT, Smith MD. Non-surgical treatment of hallux valgus: A current practice survey of Australian podiatrists. Journal of Foot and Ankle Research. 2016; 9(1):16. [DOI:10.1186/s13047-016-0146-5] [PMID]
- Farzadi M, Safaeepour Z, Mousavi M, Saeeidi H, Farzi M. Effect of arch support insole on plantar pressure distribution in females with mild and moderate hallux valgus. Rehabilitation Journal. 2013; 14(3):107-14. [Link]
- Yoo TG, Cho HS, Lee MG. Effects of a single corrective exercise and taping on gait patterns, plantar pressure, balance, and pain in female moderate hallux valgus patients. Korean Journal of Sport Science. 2020; 31(2):153-68. [DOI:10.24985/kjss.2020.31.2.153]
- Menz H, Lim P, Hurn S, Mickle K, Buldt A, Cotchett MP, et al. Effectiveness of footwear and foot orthoses in reducing medial metatarsophalangeal joint pressure in women with hallux valgus. 2024 [Unpublished]. [DOI:10.2139/ssrn.4601878]
- Ramel A, Halldorsson TI, Tryggvadottir EA, Martinez JA, Kiely M, Bandarra NM, Thorsdottir I. Relationship between BMI and body fatness in three European countries. European Journal of Clinical Nutrition 2013; 67(3):254-8. [DOI: 10.1038/ejcn.2013.6] [PMID]
- Farber DC, DeOrio JK, Steel III MW. Goniometric versus computerized angle measurement in assessing hallux valgus. Foot & Ankle International. 2005; 26(3):234-8. [DOI:10.1177/107110070502600309] [PMID]
- Kwan MY, Yick KL, Yip J, Tse CY. Hallux valgus orthosis characteristics and effectiveness: A systematic review with meta-analysis. BMJ Open. 2021; 11(8):e047273. [DOI:10.1136/bmjopen-2020-047273] [PMID]
- Gumuskaya O, Peterson B, Donnelly H, Unver B, Lafferty D, Tehan P. Preoperative and postoperative physical and mechanical rehabilitation interventions in hallux valgus: A systematic review. Journal of Foot and Ankle Research. 2025;18(3):e70083. [DOI:10.1002/jfa2.70083] [PMID]
- Koller U, Willegger M, Windhager R, Wanivenhaus A, Trnka HJ, Schuh R. Plantar pressure characteristics in hallux valgus feet. Journal of Orthopaedic Research. 2014; 32(12):1688-93. [DOI:10.1002/jor.22707] [PMID]
- Hida T, Okuda R, Yasuda T, Jotoku T, Shima H, Neo M. Comparison of plantar pressure distribution in patients with hallux valgus and healthy matched controls. Journal of Orthopaedic Science. 2017; 22(6):1054-9. [DOI:10.1016/j.jos.2017.08.008] [PMID]
- Aiyer A, Massel DH, Siddiqui N, Acevedo JI. Biomechanical comparison of 2 common techniques of minimally invasive hallux valgus correction. Foot & Ankle International. 2021; 42(3):373-80. [DOI:10.1177/1071100721992051] [PMID]
- Bryant A, Tinley P, Singer K. Plantar pressure distribution in normal, hallux valgus and hallux limitus feet. The Foot. 1999; 9(3):115-9. [DOI:10.1054/foot.1999.0538]
- Yoon YK, Tang ZH, Shim DW, Rhyu HJ, Han SH, Lee JW, et al. Minimally invasive transverse distal metatarsal osteotomy (MITO) for hallux valgus correction: Early outcomes of mild to moderate vs severe deformities. Foot & Ankle International. 2023; 44(10):992-1002. [DOI:10.1177/10711007231185330] [PMID]
- Kelly AR. The effects of a foot-toe orthosis on dynamic balance and hallux valgus angle. Normal: Illinois State University; 2014. [Link]
- Galica AM, Hagedorn TJ, Dufour AB, Riskowski JL, Hillstrom HJ, Casey VA, et al. Hallux valgus and plantar pressure loading: The Framingham foot study. Journal of Foot and Ankle Research. 2013; 6(1):42. [DOI:10.1186/1757-1146-6-42] [PMID]
- Hutton W, Dhanendran M. The mechanics of normal and hallux valgus feet-A quantitative study. Clinical Orthopaedics and Related Research. 1981; 157:7-13. [DOI:10.1097/00003086-198106000-00004]
- Collan L, Kankare JA, Mattila K. The biomechanics of the first metatarsal bone in hallux valgus: A preliminary study utilizing a weight bearing extremity CT. Foot and Ankle Surgery. 2013; 19(3):155-61. [DOI:10.1016/j.fas.2013.01.003] [PMID]
- Wen J, Ding Q, Yu Z, Sun W, Wang Q, Wei K. Adaptive changes of foot pressure in hallux valgus patients. Gait & Posture. 2012; 36(3):344-9. [DOI:10.1016/j.gaitpost.2012.03.030] [PMID]
Article type: Original Research Articles |
Subject:
methodology in rehabilitation
Received: 2025/09/2 | Accepted: 2025/10/25 | Published: 2026/03/1
Received: 2025/09/2 | Accepted: 2025/10/25 | Published: 2026/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
