
988368
Sat, Jun 20, 2026

Volume 24, Issue 1 (March 2026)
Iranian Rehabilitation Journal 2026, 24(1): 123-132 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ali Z A S, AL-Obeidi A H, Mohammed A A. Multimodal Rehabilitation With Ozone and Ultrasound for Partial ACL Tears in Basketball Players. Iranian Rehabilitation Journal 2026; 24 (1) :123-132
URL: http://irj.uswr.ac.ir/article-1-2639-en.html
URL: http://irj.uswr.ac.ir/article-1-2639-en.html



1- College of Health & Medical Techniques, Kufa ALFurat AL-Awsat Technical University, Najaf, Iraq.
Keywords: Anterior cruciate ligament (ACL), Partial ACL tear, Ozone (O₃) therapy, Ultrasound, Rehabilitation, Knee range of motion (ROM)
Full-Text [PDF 562 kb]
(107 Downloads)
| Abstract (HTML) (1535 Views)
References
Full-Text: (13 Views)
Introduction
Among athletes, knee and ankle joints are the most susceptible parts of the body to get injured [1-3]. Anterior cruciate ligament (ACL) injury is one of the most common and functionally important knee pathologies in sports medicine, mainly among the athletes who twist and jump [4]. Complete ACL tears usually require surgical reconstruction, but partial tears of the ACL, defined as a macroscopic disruption of less than 50% of the ligament fibers, present a completely different situation for the clinician where nonsurgical management may be both possible and even more preferable, especially when significant instability or a concurrent meniscal injury is absent [5]. The decision to undertake non-surgical treatment depends on the accomplishment of dynamic knee stability through the improvement of neuromuscular control, strength, and proprioception; these are the objectives that are best attained through structured progressive rehabilitation [6].
Basketball is a very demanding sport that requires frequent high-velocity cutting, pivoting, landing from jumps, and rapid stopping, thus putting the knee joint under a lot of pressure biomechanically. Statistical data from epidemiological studies show that basketball is among the sports with the highest incidence of ACL injuries, mainly among young adults and elite athletes. Often, non-contact mechanisms that lead to valgus collapse with internal tibial rotation cause partial tears, with the ACL being affected disproportionately, and may lead to chronic instability or early-onset osteoarthritis if not treated properly [7].
The primary non-surgical approach for partial ACL tear management continues to be exercise-based rehabilitation, and protocols do indeed emphasize quadriceps and hamstring strengthening, neuromuscular re-education [8, 9], and functional progression [10]. However, there remains considerable heterogeneity with respect to rehabilitation design and length, along with the utilization of adjunctive modalities, yielding variable timelines and disparate outcomes related to return-to-sport status [11]. Growing interest thus exists in interventions that utilize multidisciplinary methods to accelerate tissue healing, modulate pain, and enhance functional gains beyond exercise alone [12].
Among these adjuncts, therapeutic US remains one of the most popular modalities in musculoskeletal physiotherapy [13]. At appropriate intensities (usually 1-3 W/cm² in pulsed mode), US produces thermal and non-thermal bioeffects that include increased collagen synthesis, improved local blood flow, and diminished inflammatory mediators [14]. Recent systematic reviews indicate that US, if combined into extensive rehabilitation programs, results in modest but statistically significant pain and functional gains in knee disorders, although evidence related to ligamentous injuries is limited [15].
Ozone (O₃) therapy has also emerged as a promising bioregulatory intervention in sports medicine [16]. O₃ therapy is delivered through the percutaneous route or by superficial bagging and exhibits strong anti-inflammatory, antioxidant, and pain-relieving properties by modulating cytokine pathways (for instance, tumor necrosis factor [TNF]-α and interleukin [IL]-6), activating antioxidant enzymes, and increasing oxygen supply to the tissues [17]. The earliest clinical studies indicated knee osteoarthritis and tendon diseases as good candidates for the therapy, however, the treatment of acute ligament injuries in sports has not yet resulted in strong proof and the issues of the best dosage, the method of administration, and the safety profile have not been adequately addressed [18].
Critically, no studies to date have examined the synergistic effects of combining O₃ therapy, therapeutic ultrasound, and a supervised, progressive exercise program in athletes with partial ACL tears [19]. Such an approach constitutes a major knowledge gap, considering that these complementary mechanisms are plausibly synergistic, since exercise restores mechanical function, while O₃ and ultrasound might concomitantly reduce inflammation, decrease pain sensitization, and enhance the repair of soft tissues [20].
The present quasi-experimental, 1-group pre-test-post-test study investigates the effectiveness of a 12-week multimodal rehabilitation program that includes O₃ bagging, pulsed therapeutic ultrasound, and progressive resistance training in male basketball players with magnetic resonance imaging (MRI) -confirmed partial ACL tears. This investigation aims at determining whether there is any within-subject change in quadriceps muscle strength, active ROM, and mechanical pain sensitivity. This study will attempt to ensure preliminary evidence for a nonsurgical protocol that can optimize recovery trajectories and inform timely, safe return-to-play decisions in a high-risk athletic population through the rigorous quantification of outcomes with validated instruments and the control of temporal and environmental confounders.
Materials and Methods
Trial design and setting
The research utilized a single-group, quasi-experimental pre-test-post-test design to assess the impact of a 12-week multimodal rehabilitation program. The study took place at the Physical Therapy and Rehabilitation Center in Babylon Governorate, Iraq, from June 24 to October 28, 2024. All evaluations and therapy sessions took place in a controlled clinical environment, under the monitoring of licensed physical therapists, and with the participation of orthopedic specialists from the same center.
Study participants
Participants were male basketball players referred to the Physical Therapy and Rehabilitation Center in the Babylon Governorate, Iraq between December 10, 2024 and April 1, 2025, who fulfilled the following criteria for inclusion in this study [21]. The inclusion criteria were as follows. They must be male basketball players aged 20-30 years and actively playing in regional or national leagues. They must present a diagnosis of an isolated partial tear of ACL, which means in the present study that the disruption of the ligament fibers is less than 50%; this was diagnosed by 1.5 Tesla MRI. The injury regarding the knee under study was sustained within 4 to 8 weeks before the start of the study-subacute phase of the injury. No clinical or radiological signs of other knee pathologies were present, such as meniscal tears-grade ≥II on MRI, collateral ligament injury, osteochondral lesions, or relevant joint effusion requiring removal. Participants had not received surgery for the knee or intra-articular corticosteroid injections or administration of O₃ or application of therapeutic ultrasound to the injured knee for the last 3 months. Participants should be willing not to perform any type of physiotherapy, pharmacological or alternative treatment during the 12-week duration of the study. Written informed consent was obtained; moreover, commitment to adhere to the intervention schedule with an expected minimum attendance rate of 90%.
In case the participants had any of the subsequent conditions [22], they would be eliminated from the study: total ACL tear or multi-ligament knee injury; x-ray signs of knee osteoarthritis (Kellgren–Lawrence grade ≥2); systemic inflammatory or autoimmune diseases like rheumatoid arthritis or gout affecting the entire body; conditions that impair the functioning of the nervous system, balance or muscles which may lead to impaired balance, gait, or motor control; and receiving anticoagulant therapy or O₃ therapy.
Study intervention
All the individuals involved in the study were subject to a rehabilitation treatment, consisting of a combination of O₃ therapy, ultrasound, and physical therapy for a period of 12 weeks. The treatment was administered three times a week (36 sessions in total) from the 26th of June to the 26th of October 2024. The duration of each session was around 45 to 50 minutes and it took place under the continuous supervision of certified physiotherapists who had a minimum of 3 years of clinical experience in the area of sports rehabilitation. The treatment began with the use of the mentioned physical modalities: first, O₃ therapy was given using a method of O₃ bagging in which a polyethylene bag that was airtight was used to enclose the lower limb that was affected and then O₃ gas, which is medical-grade was injected at a concentration of 30 µg/mL for 15 min using a calibrated O₃ generator [23]. Immediately afterward, pulsed therapeutic ultrasound was applied over the anteromedial and anterolateral aspects of the knee by using a 1-MHz device at an intensity of 1.5 W/cm² in pulsed mode (1:4 duty cycle) for 5 min, while the transducer is moved in slow circular motions in order to avoid thermal buildup [24].
Participants performed a structured, progressive exercise program divided into four 3-week phases. The initial phase focused on pain-free neuromuscular activation and restoration of basic ROM through exercises, such as straight-leg raises, heel slides, and quad sets using light elastic resistance bands. The second phase introduced closed kinetic chain exercises-mini-squats, step-ups, and leg press-with progressive external resistance ranging from 0.5 kg to 5 kg, together with static balance training on stable surfaces. Dynamic strengthening tasks, such as lunges and single-leg squats with resistance up to 10 kg, proprioceptive challenges on foam pads, and initiation of stationary cycling for 10-15 min at 60 rpm were added in the third phase. Emphasis on sport-specific functional retraining, including controlled lateral shuffles, pivoting drills, and jump-landing mechanics, with resistance loads increasing up to 20 kg and gradual reintroduction of treadmill walking and running based on the individual’s tolerance, was given in the final phase [25]. All exercises were performed below the participant’s pain threshold (≤2/10 on a visual analog scale) and advancement to the next phase was permitted only in the absence of pain exacerbation or joint swelling. Attendance was monitored, and adherence was defined as completion of at least 33 of the 36 scheduled sessions (≥90%). No additional pharmacological, manual, or alternative therapies were allowed during the study period. Treatment logs were kept for each participant to record session details and exercise progression throughout the study and note any deviation from the protocol.
Outcomes
The research investigated the efficacy of a 12-week multimodal rehabilitation program through a variety of primary and secondary outcome measures. The main outcomes incorporated knee muscle strength, active ROM of the knee joint (flexion, extension, internal, and external rotation), and mechanical pain sensitivity quantified via pressure pain threshold (PPT). Secondary outcomes included changes in knee swelling as measured using the aforementioned method of circumferential measurement at the joint line. Each of the above-mentioned measurements was obtained on two different occasions: one before the intervention and the other after the intervention, in standardized conditions (at the same time of the day, with the same assessor and identical environmental settings) to minimize diurnal and contextual variability.
Muscle strength
Calibrated handheld dynamometer (MicroFET2™, Hoggan Health Industries, USA) was used to assess the quadriceps muscle strength, which has shown excellent test-re-test reliability (ICC>0.90) in athletic populations with knee pathology [26]. Participants were positioned in a supine lying position on a plinth with their hips in neutral alignment and their knees flexed at 60 degrees; this position was chosen so as to maximize the mechanical advantage and isolate the quadriceps contraction while at the same time minimizing compensatory movements. The pad of the dynamometer was placed on the anterior part of the distal tibia, about 5 cm above the medial malleolus, and held firmly in position by the assessor. The participant was asked to do a maximal isometric knee extension against the dynamometer’s resistance for 5 seconds, and strong verbal encouragement was given to ensure that the effort was indeed maximal. A total of 3 trials were conducted; between each repetition a 30-s rest was given to prevent fatigue. The assessor kept the same hand placement and stabilization throughout the trials and made sure no trunk or pelvic movement took place during the testing. The highest value (in kilograms) recorded in the three trials was taken for statistical analysis [26].
Knee ROM
The ROM in the active knee was evaluated by a single physiotherapist who was trained, to use a standard plastic goniometer of 360 degrees (Baseline®) and also guarantee accuracy. The participant was placed in supine lying on a plinth position with the hip and the contralateral limb in a neutral alignment with the knee extension positioning. The participant was first asked to bend the knee and then straighten it while being supported by the physiotherapist to stabilize the pelvis. The goniometer’s axis was positioned appropriately over the femur’s lateral epicondyle. The stationary arm was adjusted parallel to the femur’s longitudinal axis with the greater trochanter as the proximal reference point while the moving arm was aligned with the fibula’s lateral malleolus. Flexion was captured as the angle of full extension (0°) and maximum active bend, and extension was measured as the degree of hyperextension past the neutral 0° position.
The knee was first bent at 90 degrees for internal and external rotation, and the hip was controlled by the examiner in neutral rotation to hinder pelvic compensatory movement. Then, the subject was asked to rotate the tibia medially (internal rotation) and laterally (external rotation) as far as possible without experiencing pain. During this process, the goniometer’s axis was still at the femur’s lateral epicondyle, the stationary arm stayed in line with the femur (towards the greater trochanter), and the moving arm tracked the fibula (towards the lateral malleolus). Each motion was tested three times, and the maximum value (in degrees) was taken for the purpose of analysis. The assessor gave standardized verbal instructions and visual demonstrations prior to each measurement and assured that movements were per.
Pain sensitivity
Pain sensitivity was determined by applying PPT algometry with the Wagner FPX25 digital algometer (Wagner Instruments, USA). This is a handheld device with a 1 cm² circular rubber probe. It was calibrated to show the force in Newton (N). The participant was seated comfortably on a plinth with the affected knee in slight flexion (~20°) and the leg completely relaxed. Before the test, the physiotherapist who, in this case, was the assessor, found the most tender point along the knee joint line by systematic palpation with moderate pressure. The physiotherapist had one year of clinical experience and 30 min of supervised practical training on a patient with a similar knee injury. The pressure of the algometer was applied with the rubber probe positioned perpendicularly to the skin spot which had been over the tender point. The participant was asked to say “now” as soon as the pressure feeling turned into pain. At this verbal signal, the assessor immediately released the pressure and noted down the peak force value shown on the device. The same procedure was done three times at the same place with a 20-s interval in between each trial to allow the nociceptors to recover and not to get sensitized. For the analysis, the mean of the three readings (in Newtons) was used. All the measurements were done in one session under specified environmental conditions. This protocol is in accordance with established guidelines for PPT assessment in musculoskeletal pain research and is also backed by evidence that shows acceptable intra-rater reliability (ICC=0.78-0.89) for the Wagner FPX series when administered by trained clinicians in knee injury populations [28].
Knee swelling
Swelling of the knee was measured through a non-elastic but flexible tape that was placed around the knee at the level of the joint line, and this area was identified as the midpoint between the medial and lateral joint margins with the knee in full extension. The participant was lying down on a plinth with the affected leg relaxed and fully stretched out. Two measurements were taken successively to the nearest 0.1 cm and their mean value was used for the analysis to improve the reliability [29].
Sample size
A total of 10 participants constituted the sample size which was determined by taking into account the feasibility factors, such as the recruitment window at the single recruitment site that had qualified basketball players with MRI-confirmed partial ACL tears. This sample size is in agreement with the recommendations for pilot studies in homogeneous clinical populations that evaluate novel rehabilitation protocols [30].
Statistical methods
The entire statistical analysis was performed using the IBM SPSS Statistics software, version 26.0. Because of the very small sample size (n=10) and the non-normal distribution of all outcome variables, as proven by Shapiro-Wilk tests (P<0.05 for all measures), it was compulsory to use non-parametric statistical methods all through. All the outcomes of the research were compared by the differences between pre- and post-intervention, including primary outcomes (quadriceps strength in kg through active knee ROM in degrees for flexion, extension, and internal and external rotation, and PPT in Newtons) and secondary outcomes (knee circumference in cm as an indicator of swelling). The Wilcoxon signed-rank test was used to determine the statistical significance of the changes from baseline to week 12. The effect size was calculated using the Equation 1:
1. r=Z/√N
Where Z is the test statistic, and N is the total number of observations; then, r values of ≥0.10, ≥0.30, and ≥0.50 were defined as small, medium, and large effects, correspondingly. The Mean±SD (descriptive statistics) were given for all variables at the two time points to assist clinical interpretation. The significance level was determined beforehand at α=0.05, with two-tailed tests for all the tests performed.
Results
Participants’ characteristics
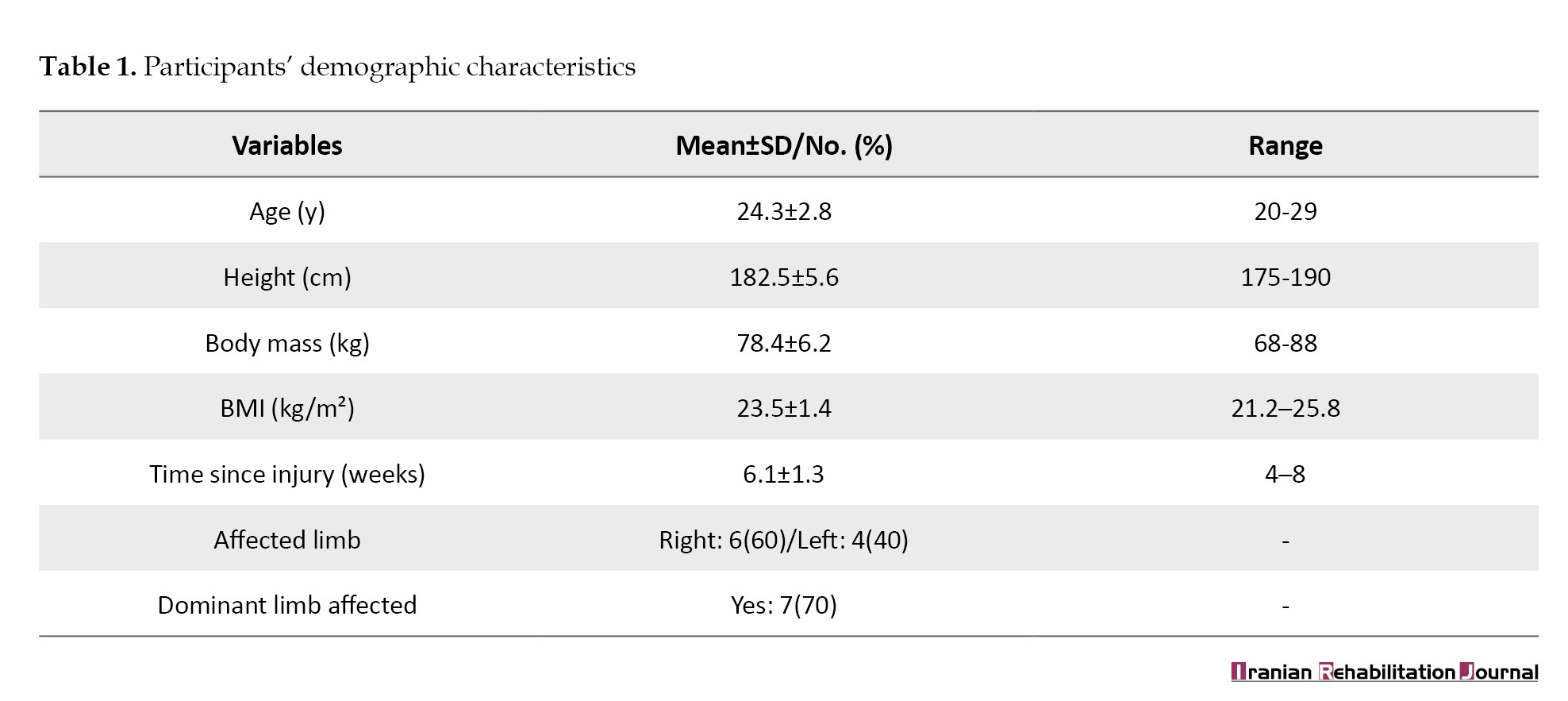
Ten male basketball players with MRI-confirmed partial ACL tears participated in the study. All participants were actively competing in regional or national leagues and sustained their injury during sport-specific activities (e.g. landing from a jump or rapid deceleration). The primary demographic and injury-related traits are collectively presented in Table 1.
Within-group changes in outcome measures
Significant improvements were observed across all primary and secondary outcome measures following the 12-week multimodal rehabilitation program (Table 2).
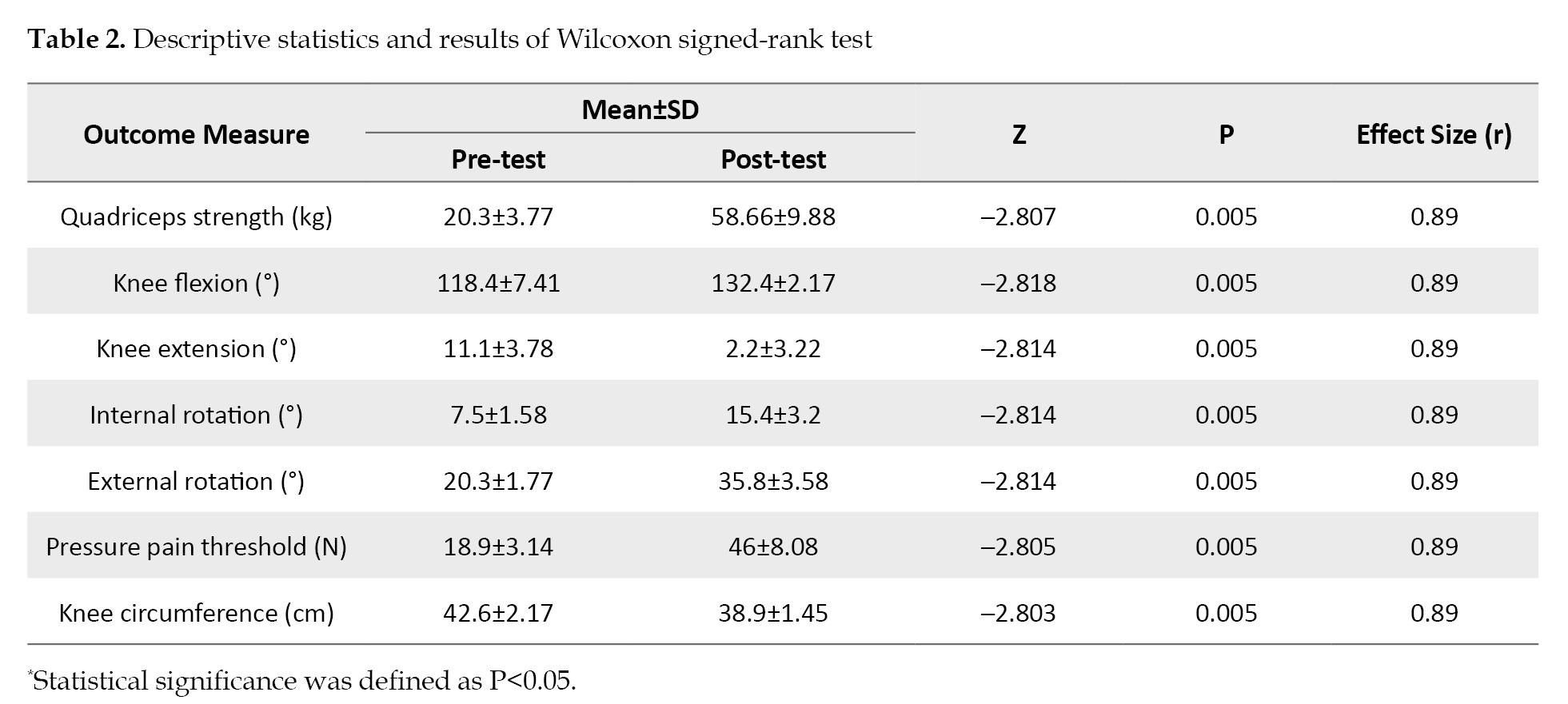
The Wilcoxon signed-rank test revealed statistically significant differences (P=0.005) for all variables, with large effect sizes (r=0.89).
Strength of the quadriceps improved remarkably by 189%, of which the biggest part was reflected in the range from 20.30 kg to 58.66 kg. Also, active knee flexion rose 14° almost to the normal range (132.4°), and also extension deficit was reduced from 11.1° to 2.2°, and this is already a sign of great reduction of joint stiffness. Meanwhile, the ROM in rotation doubled as well, with the internal rotation rising from 7.5° to 15.4° and external rotation from 20.3° to 35.8°. Pain threshold measured with PPT improved 143% meaning it increased from 18.9 N to 46.0 N, thus reflecting the substantial reduction of mechanical hyperalgesia. Knee swelling determined by the circumferential method decreased by 3.7 cm on average, from 42.6 cm to 38.9 cm.
Discussion
This quasi-experimental research indicates a notable and statistically valid 12-week rehabilitation program and O₃ bagging along with other modalities like pulsed therapeutic ultrasound and progressive resistance training, which results in a substantial increase in strength, knee ROM, mechanical pain sensitivity, and joint swelling in male basketball players with MRI-confirmed partial ACL tears. All of the primary and secondary outcomes showed large effect sizes (r=0.89) with P<0.005, which not only confirms the hypothesis that biophysical adjuncts can enhance the efficacy of exercise-based rehabilitation in this high-risk athletic population but also allows to conclusively assert that their contribution is indeed substantial.
The 189% strength increase (from 20.3 to 58.7 kg) of the quadriceps is especially remarkable because one of the features of the ACL disease, even in partial tears, is the quadriceps’ inhibition, which also serves as a major barrier to attaining functional restoration. This hearty gain in strength is probably the outcome of the progressive neuromuscular loading and the anti-inflammatory and oxygenation-enhancing effects of O₃ therapy working together. O₃ has been proven to activate antioxidant enzymes (e.g. superoxide dismutase [SOD]) and make mitochondrial respiration more efficient, thus minimizing exercise-induced oxidative stress and muscle fatigue [31]. At the same time, pulsed ultrasound might have enabled the healing ligament to be more mechanically stable by facilitating collagen realignment and fibroblast proliferation within it, thus allowing higher training intensities with no pain exacerbation [32]. The current results are in accordance with those reported by Saghaeinooshabadi et al., who observed increased muscle performance after elastic resistance training in ACL-injured individuals and contributed to their findings by showing that pairing such exercises with O₃ and ultrasound multiplies functional outcomes [6].
In a similar vein, the recovery of almost natural knee ROM-flexion attaining 132.4° (in the usual range of 130-135°) and the decline of the extension deficit from 11.1° to 2.2°, point out the successful elimination of arthrogenic muscle inhibition and capsular stiffness. The increase in rotational mobility (internal and external rotation) by twice signifies better dynamic joint control, which is probably due to the neuromuscular re-education part of the program that went from static stabilization to sport-specific agility drills [33]. These improvements in ROM agree with the biomechanical principles set by evidence and support clinical observations that early mobilization along with anti-edema strategies speeds up recovery in subacute ligament injuries [33, 34].
The 143% rise in PPT (from 18.9 to 46.0 N) indicates a significant drop in mechanical hyperalgesia, which is a common result of ligamentous trauma leading to peripheral and central sensitization. The analgesic effect may be due to the O₃’s ability to modulate the pro-inflammatory cytokines (e.g. TNF-α, IL-6) and the ultrasound’s non-thermal bioeffects on the nociceptor’s activity. Also, the 3.7 cm shrinkage in knee circumference observed provides a clear sign of the reduction of synovitis and soft tissue edema that facilitates the pain-free movement and strength development [35].
Although these remarkable outcomes have been reported, it is still necessary to recognize a number of limitations. To begin with, the lack of a control group inhibits the outcome attribution to the intervention alone and the possibility of the natural history or placebo effects has not been ruled out. Next, the small number of participants (n=10) affects the extent to which the findings can apply to broader populations and the statistical power, but the consistency and size of effects indicate their strength. Moreover, no blinding of participants and therapists was done, which brought in the possibility of performance and detection bias. To add, long-term follow-up was not performed; thus, it is not known whether the gains will last and whether there is a chance of re-injury or not.
It is imperative that future studies will throw light on these shortcomings with randomized controlled trials that will compare this multimodal protocol with an exercise-only or standard care, involving larger samples, concealed allocation, and assessor blinding. Also, research that involves biomarkers like serum IL-6, COMP, or imaging biomarkers like T2 mapping on MRI could be helpful in understanding the biological mechanisms that are responsible for the clinical improvements. Moreover, the longitudinal tracking of return-to-sport rates and re-injury incidence would be a strong validation of the clinical utility of this approach.
Conclusion
The output of this 12-week quasi-experimental study indicates that a multimodal rehabilitation plan combining O₃ bagging, pulsed therapeutic ultrasound, and progressive resistance training resulted in improvements in quadriceps strength, knee ROM, mechanical pain sensitivity, and joint swelling, not only statistically but also in a way that could be observed clinically, in male basketball players who had already undergone MRI and were diagnosed with partial ACL tears. The large effect sizes along with the restoration of almost normal knee function, which was shown by flexion reaching 132.4°, extension deficit being reduced to 2.2°, and PPT more than doubling, all contribute to restoring the biological and clinical plausibility of combining biophysical adjuncts with exercise-based rehabilitation during the subacute phase of partial ligament injury.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Al-Furat Al-Awsat Technical University, Najaf, Iraq (Code: FA-3).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to this work. Each author participated in the conceptualization, design, data collection, data analysis, interpretation of results, and drafting of the manuscript. All authors read and approved the final version of the manuscript.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely appreciate the basketball players who volunteered their time and effort to participate in this study.
Among athletes, knee and ankle joints are the most susceptible parts of the body to get injured [1-3]. Anterior cruciate ligament (ACL) injury is one of the most common and functionally important knee pathologies in sports medicine, mainly among the athletes who twist and jump [4]. Complete ACL tears usually require surgical reconstruction, but partial tears of the ACL, defined as a macroscopic disruption of less than 50% of the ligament fibers, present a completely different situation for the clinician where nonsurgical management may be both possible and even more preferable, especially when significant instability or a concurrent meniscal injury is absent [5]. The decision to undertake non-surgical treatment depends on the accomplishment of dynamic knee stability through the improvement of neuromuscular control, strength, and proprioception; these are the objectives that are best attained through structured progressive rehabilitation [6].
Basketball is a very demanding sport that requires frequent high-velocity cutting, pivoting, landing from jumps, and rapid stopping, thus putting the knee joint under a lot of pressure biomechanically. Statistical data from epidemiological studies show that basketball is among the sports with the highest incidence of ACL injuries, mainly among young adults and elite athletes. Often, non-contact mechanisms that lead to valgus collapse with internal tibial rotation cause partial tears, with the ACL being affected disproportionately, and may lead to chronic instability or early-onset osteoarthritis if not treated properly [7].
The primary non-surgical approach for partial ACL tear management continues to be exercise-based rehabilitation, and protocols do indeed emphasize quadriceps and hamstring strengthening, neuromuscular re-education [8, 9], and functional progression [10]. However, there remains considerable heterogeneity with respect to rehabilitation design and length, along with the utilization of adjunctive modalities, yielding variable timelines and disparate outcomes related to return-to-sport status [11]. Growing interest thus exists in interventions that utilize multidisciplinary methods to accelerate tissue healing, modulate pain, and enhance functional gains beyond exercise alone [12].
Among these adjuncts, therapeutic US remains one of the most popular modalities in musculoskeletal physiotherapy [13]. At appropriate intensities (usually 1-3 W/cm² in pulsed mode), US produces thermal and non-thermal bioeffects that include increased collagen synthesis, improved local blood flow, and diminished inflammatory mediators [14]. Recent systematic reviews indicate that US, if combined into extensive rehabilitation programs, results in modest but statistically significant pain and functional gains in knee disorders, although evidence related to ligamentous injuries is limited [15].
Ozone (O₃) therapy has also emerged as a promising bioregulatory intervention in sports medicine [16]. O₃ therapy is delivered through the percutaneous route or by superficial bagging and exhibits strong anti-inflammatory, antioxidant, and pain-relieving properties by modulating cytokine pathways (for instance, tumor necrosis factor [TNF]-α and interleukin [IL]-6), activating antioxidant enzymes, and increasing oxygen supply to the tissues [17]. The earliest clinical studies indicated knee osteoarthritis and tendon diseases as good candidates for the therapy, however, the treatment of acute ligament injuries in sports has not yet resulted in strong proof and the issues of the best dosage, the method of administration, and the safety profile have not been adequately addressed [18].
Critically, no studies to date have examined the synergistic effects of combining O₃ therapy, therapeutic ultrasound, and a supervised, progressive exercise program in athletes with partial ACL tears [19]. Such an approach constitutes a major knowledge gap, considering that these complementary mechanisms are plausibly synergistic, since exercise restores mechanical function, while O₃ and ultrasound might concomitantly reduce inflammation, decrease pain sensitization, and enhance the repair of soft tissues [20].
The present quasi-experimental, 1-group pre-test-post-test study investigates the effectiveness of a 12-week multimodal rehabilitation program that includes O₃ bagging, pulsed therapeutic ultrasound, and progressive resistance training in male basketball players with magnetic resonance imaging (MRI) -confirmed partial ACL tears. This investigation aims at determining whether there is any within-subject change in quadriceps muscle strength, active ROM, and mechanical pain sensitivity. This study will attempt to ensure preliminary evidence for a nonsurgical protocol that can optimize recovery trajectories and inform timely, safe return-to-play decisions in a high-risk athletic population through the rigorous quantification of outcomes with validated instruments and the control of temporal and environmental confounders.
Materials and Methods
Trial design and setting
The research utilized a single-group, quasi-experimental pre-test-post-test design to assess the impact of a 12-week multimodal rehabilitation program. The study took place at the Physical Therapy and Rehabilitation Center in Babylon Governorate, Iraq, from June 24 to October 28, 2024. All evaluations and therapy sessions took place in a controlled clinical environment, under the monitoring of licensed physical therapists, and with the participation of orthopedic specialists from the same center.
Study participants
Participants were male basketball players referred to the Physical Therapy and Rehabilitation Center in the Babylon Governorate, Iraq between December 10, 2024 and April 1, 2025, who fulfilled the following criteria for inclusion in this study [21]. The inclusion criteria were as follows. They must be male basketball players aged 20-30 years and actively playing in regional or national leagues. They must present a diagnosis of an isolated partial tear of ACL, which means in the present study that the disruption of the ligament fibers is less than 50%; this was diagnosed by 1.5 Tesla MRI. The injury regarding the knee under study was sustained within 4 to 8 weeks before the start of the study-subacute phase of the injury. No clinical or radiological signs of other knee pathologies were present, such as meniscal tears-grade ≥II on MRI, collateral ligament injury, osteochondral lesions, or relevant joint effusion requiring removal. Participants had not received surgery for the knee or intra-articular corticosteroid injections or administration of O₃ or application of therapeutic ultrasound to the injured knee for the last 3 months. Participants should be willing not to perform any type of physiotherapy, pharmacological or alternative treatment during the 12-week duration of the study. Written informed consent was obtained; moreover, commitment to adhere to the intervention schedule with an expected minimum attendance rate of 90%.
In case the participants had any of the subsequent conditions [22], they would be eliminated from the study: total ACL tear or multi-ligament knee injury; x-ray signs of knee osteoarthritis (Kellgren–Lawrence grade ≥2); systemic inflammatory or autoimmune diseases like rheumatoid arthritis or gout affecting the entire body; conditions that impair the functioning of the nervous system, balance or muscles which may lead to impaired balance, gait, or motor control; and receiving anticoagulant therapy or O₃ therapy.
Study intervention
All the individuals involved in the study were subject to a rehabilitation treatment, consisting of a combination of O₃ therapy, ultrasound, and physical therapy for a period of 12 weeks. The treatment was administered three times a week (36 sessions in total) from the 26th of June to the 26th of October 2024. The duration of each session was around 45 to 50 minutes and it took place under the continuous supervision of certified physiotherapists who had a minimum of 3 years of clinical experience in the area of sports rehabilitation. The treatment began with the use of the mentioned physical modalities: first, O₃ therapy was given using a method of O₃ bagging in which a polyethylene bag that was airtight was used to enclose the lower limb that was affected and then O₃ gas, which is medical-grade was injected at a concentration of 30 µg/mL for 15 min using a calibrated O₃ generator [23]. Immediately afterward, pulsed therapeutic ultrasound was applied over the anteromedial and anterolateral aspects of the knee by using a 1-MHz device at an intensity of 1.5 W/cm² in pulsed mode (1:4 duty cycle) for 5 min, while the transducer is moved in slow circular motions in order to avoid thermal buildup [24].
Participants performed a structured, progressive exercise program divided into four 3-week phases. The initial phase focused on pain-free neuromuscular activation and restoration of basic ROM through exercises, such as straight-leg raises, heel slides, and quad sets using light elastic resistance bands. The second phase introduced closed kinetic chain exercises-mini-squats, step-ups, and leg press-with progressive external resistance ranging from 0.5 kg to 5 kg, together with static balance training on stable surfaces. Dynamic strengthening tasks, such as lunges and single-leg squats with resistance up to 10 kg, proprioceptive challenges on foam pads, and initiation of stationary cycling for 10-15 min at 60 rpm were added in the third phase. Emphasis on sport-specific functional retraining, including controlled lateral shuffles, pivoting drills, and jump-landing mechanics, with resistance loads increasing up to 20 kg and gradual reintroduction of treadmill walking and running based on the individual’s tolerance, was given in the final phase [25]. All exercises were performed below the participant’s pain threshold (≤2/10 on a visual analog scale) and advancement to the next phase was permitted only in the absence of pain exacerbation or joint swelling. Attendance was monitored, and adherence was defined as completion of at least 33 of the 36 scheduled sessions (≥90%). No additional pharmacological, manual, or alternative therapies were allowed during the study period. Treatment logs were kept for each participant to record session details and exercise progression throughout the study and note any deviation from the protocol.
Outcomes
The research investigated the efficacy of a 12-week multimodal rehabilitation program through a variety of primary and secondary outcome measures. The main outcomes incorporated knee muscle strength, active ROM of the knee joint (flexion, extension, internal, and external rotation), and mechanical pain sensitivity quantified via pressure pain threshold (PPT). Secondary outcomes included changes in knee swelling as measured using the aforementioned method of circumferential measurement at the joint line. Each of the above-mentioned measurements was obtained on two different occasions: one before the intervention and the other after the intervention, in standardized conditions (at the same time of the day, with the same assessor and identical environmental settings) to minimize diurnal and contextual variability.
Muscle strength
Calibrated handheld dynamometer (MicroFET2™, Hoggan Health Industries, USA) was used to assess the quadriceps muscle strength, which has shown excellent test-re-test reliability (ICC>0.90) in athletic populations with knee pathology [26]. Participants were positioned in a supine lying position on a plinth with their hips in neutral alignment and their knees flexed at 60 degrees; this position was chosen so as to maximize the mechanical advantage and isolate the quadriceps contraction while at the same time minimizing compensatory movements. The pad of the dynamometer was placed on the anterior part of the distal tibia, about 5 cm above the medial malleolus, and held firmly in position by the assessor. The participant was asked to do a maximal isometric knee extension against the dynamometer’s resistance for 5 seconds, and strong verbal encouragement was given to ensure that the effort was indeed maximal. A total of 3 trials were conducted; between each repetition a 30-s rest was given to prevent fatigue. The assessor kept the same hand placement and stabilization throughout the trials and made sure no trunk or pelvic movement took place during the testing. The highest value (in kilograms) recorded in the three trials was taken for statistical analysis [26].
Knee ROM
The ROM in the active knee was evaluated by a single physiotherapist who was trained, to use a standard plastic goniometer of 360 degrees (Baseline®) and also guarantee accuracy. The participant was placed in supine lying on a plinth position with the hip and the contralateral limb in a neutral alignment with the knee extension positioning. The participant was first asked to bend the knee and then straighten it while being supported by the physiotherapist to stabilize the pelvis. The goniometer’s axis was positioned appropriately over the femur’s lateral epicondyle. The stationary arm was adjusted parallel to the femur’s longitudinal axis with the greater trochanter as the proximal reference point while the moving arm was aligned with the fibula’s lateral malleolus. Flexion was captured as the angle of full extension (0°) and maximum active bend, and extension was measured as the degree of hyperextension past the neutral 0° position.
The knee was first bent at 90 degrees for internal and external rotation, and the hip was controlled by the examiner in neutral rotation to hinder pelvic compensatory movement. Then, the subject was asked to rotate the tibia medially (internal rotation) and laterally (external rotation) as far as possible without experiencing pain. During this process, the goniometer’s axis was still at the femur’s lateral epicondyle, the stationary arm stayed in line with the femur (towards the greater trochanter), and the moving arm tracked the fibula (towards the lateral malleolus). Each motion was tested three times, and the maximum value (in degrees) was taken for the purpose of analysis. The assessor gave standardized verbal instructions and visual demonstrations prior to each measurement and assured that movements were per.
Pain sensitivity
Pain sensitivity was determined by applying PPT algometry with the Wagner FPX25 digital algometer (Wagner Instruments, USA). This is a handheld device with a 1 cm² circular rubber probe. It was calibrated to show the force in Newton (N). The participant was seated comfortably on a plinth with the affected knee in slight flexion (~20°) and the leg completely relaxed. Before the test, the physiotherapist who, in this case, was the assessor, found the most tender point along the knee joint line by systematic palpation with moderate pressure. The physiotherapist had one year of clinical experience and 30 min of supervised practical training on a patient with a similar knee injury. The pressure of the algometer was applied with the rubber probe positioned perpendicularly to the skin spot which had been over the tender point. The participant was asked to say “now” as soon as the pressure feeling turned into pain. At this verbal signal, the assessor immediately released the pressure and noted down the peak force value shown on the device. The same procedure was done three times at the same place with a 20-s interval in between each trial to allow the nociceptors to recover and not to get sensitized. For the analysis, the mean of the three readings (in Newtons) was used. All the measurements were done in one session under specified environmental conditions. This protocol is in accordance with established guidelines for PPT assessment in musculoskeletal pain research and is also backed by evidence that shows acceptable intra-rater reliability (ICC=0.78-0.89) for the Wagner FPX series when administered by trained clinicians in knee injury populations [28].
Knee swelling
Swelling of the knee was measured through a non-elastic but flexible tape that was placed around the knee at the level of the joint line, and this area was identified as the midpoint between the medial and lateral joint margins with the knee in full extension. The participant was lying down on a plinth with the affected leg relaxed and fully stretched out. Two measurements were taken successively to the nearest 0.1 cm and their mean value was used for the analysis to improve the reliability [29].
Sample size
A total of 10 participants constituted the sample size which was determined by taking into account the feasibility factors, such as the recruitment window at the single recruitment site that had qualified basketball players with MRI-confirmed partial ACL tears. This sample size is in agreement with the recommendations for pilot studies in homogeneous clinical populations that evaluate novel rehabilitation protocols [30].
Statistical methods
The entire statistical analysis was performed using the IBM SPSS Statistics software, version 26.0. Because of the very small sample size (n=10) and the non-normal distribution of all outcome variables, as proven by Shapiro-Wilk tests (P<0.05 for all measures), it was compulsory to use non-parametric statistical methods all through. All the outcomes of the research were compared by the differences between pre- and post-intervention, including primary outcomes (quadriceps strength in kg through active knee ROM in degrees for flexion, extension, and internal and external rotation, and PPT in Newtons) and secondary outcomes (knee circumference in cm as an indicator of swelling). The Wilcoxon signed-rank test was used to determine the statistical significance of the changes from baseline to week 12. The effect size was calculated using the Equation 1:
1. r=Z/√N
Where Z is the test statistic, and N is the total number of observations; then, r values of ≥0.10, ≥0.30, and ≥0.50 were defined as small, medium, and large effects, correspondingly. The Mean±SD (descriptive statistics) were given for all variables at the two time points to assist clinical interpretation. The significance level was determined beforehand at α=0.05, with two-tailed tests for all the tests performed.
Results
Participants’ characteristics
Ten male basketball players with MRI-confirmed partial ACL tears participated in the study. All participants were actively competing in regional or national leagues and sustained their injury during sport-specific activities (e.g. landing from a jump or rapid deceleration). The primary demographic and injury-related traits are collectively presented in Table 1.
Within-group changes in outcome measures
Significant improvements were observed across all primary and secondary outcome measures following the 12-week multimodal rehabilitation program (Table 2).
The Wilcoxon signed-rank test revealed statistically significant differences (P=0.005) for all variables, with large effect sizes (r=0.89).
Strength of the quadriceps improved remarkably by 189%, of which the biggest part was reflected in the range from 20.30 kg to 58.66 kg. Also, active knee flexion rose 14° almost to the normal range (132.4°), and also extension deficit was reduced from 11.1° to 2.2°, and this is already a sign of great reduction of joint stiffness. Meanwhile, the ROM in rotation doubled as well, with the internal rotation rising from 7.5° to 15.4° and external rotation from 20.3° to 35.8°. Pain threshold measured with PPT improved 143% meaning it increased from 18.9 N to 46.0 N, thus reflecting the substantial reduction of mechanical hyperalgesia. Knee swelling determined by the circumferential method decreased by 3.7 cm on average, from 42.6 cm to 38.9 cm.
Discussion
This quasi-experimental research indicates a notable and statistically valid 12-week rehabilitation program and O₃ bagging along with other modalities like pulsed therapeutic ultrasound and progressive resistance training, which results in a substantial increase in strength, knee ROM, mechanical pain sensitivity, and joint swelling in male basketball players with MRI-confirmed partial ACL tears. All of the primary and secondary outcomes showed large effect sizes (r=0.89) with P<0.005, which not only confirms the hypothesis that biophysical adjuncts can enhance the efficacy of exercise-based rehabilitation in this high-risk athletic population but also allows to conclusively assert that their contribution is indeed substantial.
The 189% strength increase (from 20.3 to 58.7 kg) of the quadriceps is especially remarkable because one of the features of the ACL disease, even in partial tears, is the quadriceps’ inhibition, which also serves as a major barrier to attaining functional restoration. This hearty gain in strength is probably the outcome of the progressive neuromuscular loading and the anti-inflammatory and oxygenation-enhancing effects of O₃ therapy working together. O₃ has been proven to activate antioxidant enzymes (e.g. superoxide dismutase [SOD]) and make mitochondrial respiration more efficient, thus minimizing exercise-induced oxidative stress and muscle fatigue [31]. At the same time, pulsed ultrasound might have enabled the healing ligament to be more mechanically stable by facilitating collagen realignment and fibroblast proliferation within it, thus allowing higher training intensities with no pain exacerbation [32]. The current results are in accordance with those reported by Saghaeinooshabadi et al., who observed increased muscle performance after elastic resistance training in ACL-injured individuals and contributed to their findings by showing that pairing such exercises with O₃ and ultrasound multiplies functional outcomes [6].
In a similar vein, the recovery of almost natural knee ROM-flexion attaining 132.4° (in the usual range of 130-135°) and the decline of the extension deficit from 11.1° to 2.2°, point out the successful elimination of arthrogenic muscle inhibition and capsular stiffness. The increase in rotational mobility (internal and external rotation) by twice signifies better dynamic joint control, which is probably due to the neuromuscular re-education part of the program that went from static stabilization to sport-specific agility drills [33]. These improvements in ROM agree with the biomechanical principles set by evidence and support clinical observations that early mobilization along with anti-edema strategies speeds up recovery in subacute ligament injuries [33, 34].
The 143% rise in PPT (from 18.9 to 46.0 N) indicates a significant drop in mechanical hyperalgesia, which is a common result of ligamentous trauma leading to peripheral and central sensitization. The analgesic effect may be due to the O₃’s ability to modulate the pro-inflammatory cytokines (e.g. TNF-α, IL-6) and the ultrasound’s non-thermal bioeffects on the nociceptor’s activity. Also, the 3.7 cm shrinkage in knee circumference observed provides a clear sign of the reduction of synovitis and soft tissue edema that facilitates the pain-free movement and strength development [35].
Although these remarkable outcomes have been reported, it is still necessary to recognize a number of limitations. To begin with, the lack of a control group inhibits the outcome attribution to the intervention alone and the possibility of the natural history or placebo effects has not been ruled out. Next, the small number of participants (n=10) affects the extent to which the findings can apply to broader populations and the statistical power, but the consistency and size of effects indicate their strength. Moreover, no blinding of participants and therapists was done, which brought in the possibility of performance and detection bias. To add, long-term follow-up was not performed; thus, it is not known whether the gains will last and whether there is a chance of re-injury or not.
It is imperative that future studies will throw light on these shortcomings with randomized controlled trials that will compare this multimodal protocol with an exercise-only or standard care, involving larger samples, concealed allocation, and assessor blinding. Also, research that involves biomarkers like serum IL-6, COMP, or imaging biomarkers like T2 mapping on MRI could be helpful in understanding the biological mechanisms that are responsible for the clinical improvements. Moreover, the longitudinal tracking of return-to-sport rates and re-injury incidence would be a strong validation of the clinical utility of this approach.
Conclusion
The output of this 12-week quasi-experimental study indicates that a multimodal rehabilitation plan combining O₃ bagging, pulsed therapeutic ultrasound, and progressive resistance training resulted in improvements in quadriceps strength, knee ROM, mechanical pain sensitivity, and joint swelling, not only statistically but also in a way that could be observed clinically, in male basketball players who had already undergone MRI and were diagnosed with partial ACL tears. The large effect sizes along with the restoration of almost normal knee function, which was shown by flexion reaching 132.4°, extension deficit being reduced to 2.2°, and PPT more than doubling, all contribute to restoring the biological and clinical plausibility of combining biophysical adjuncts with exercise-based rehabilitation during the subacute phase of partial ligament injury.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Al-Furat Al-Awsat Technical University, Najaf, Iraq (Code: FA-3).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to this work. Each author participated in the conceptualization, design, data collection, data analysis, interpretation of results, and drafting of the manuscript. All authors read and approved the final version of the manuscript.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely appreciate the basketball players who volunteered their time and effort to participate in this study.
References
- Khaliliyan H, Sharafatvaziri A, Safaeepour Z, Bahramizadeh M. Gait and muscle activity measures after biomechanical device therapy in subjects with ankle instability: A systematic review. The Foot. 2024; 59:102083. [DOI:10.1016/j.foot.2024.102083] [PMID]
- Khaliliyan H, Bahramizadeh M, Zare A, Khaghani A, Mohajeri S, Ansari M, et al. Efficacy of vibro-medical foot orthoses on gait, postural control, and muscle activity in physically active young adults: A systematic review. Journal of Prosthetics and Orthotics. 2025; 10-97. [DOI:10.32598/irj.22.4.1719.5]
- Karimi MT, Bahramizadeh M, Khaliliyan H, Ansari M, Batra K, Afolabi A, et al. Investigating the effects of knee valgus orthosis on knee joint contact forces among subjects with knee osteoarthritis: A case series study. Journal of Health and Social Sciences. 2024; 9(2):190-200. [Link]
- Bendo A, Brovina F, Bushati S, Sallaku D, Bushati M, Papa E. The effect of high interval intensity training (HIIT) on the performance of basketball players 10-15 years old. Retos. 2025; 62:627-36. [DOI:10.47197/retos.v62.109315]
- Diermeier TA, Rothrauff BB, Engebretsen L, Lynch A, Svantesson E, Senorski EA, et al. Treatment after ACL injury: Panther symposium ACL treatment consensus group. British Journal of Sports Medicine. 2021; 55(1):14-22. [DOI:10.1136/bjsports-2020-102200] [PMID]
- Saghaeinooshabadi Z, Zakerzadeh MR, Nazari MA. The intricate link between anterior cruciate ligament rupture and lower limb muscle fatigue: A case study. European Journal of Orthopaedic Surgery & Traumatology. 2025; 35(1):137. [DOI:10.1007/s00590-025-04256-x] [PMID]
- Cares Barrientos S, Retamal Matus H, Petignari Gonzalez A, Valdebenito Oyarzo L. Neuromuscular control of the lower extremity as a risk factor for ACL injury in basketball players. Retos. 2025; 68:964-976. [DOI:10.47197/retos.v68.112934]
- Naser AA, Dehkordi KJ, Radhi MN, Taghian F, Chitsaz A. The effect of multimodal exercise on the levels of BDNF and GDNF in patients with Parkinson’s disease. International Journal of Preventive Medicine. 2025; 16:35. [DOI:10.4103/ijpvm.ijpvm_353_24] [PMID]
- Radi MN, Obaid SH. The effect of exercises by metabolic conditioning on oxygen consumption and endurance in basketball players. Indian J Forensic Med Toxicol. 2020; 14(1):123-129. [Link]
- Hashem NY, Al Edhary DF, Radhi MN, Hmeid MG. The effect of dynamic lactic exercises in the maximum oxygen consumption and lay-up shot endurance of under-20 basketball players. Sport TK. 2022; 2(2):45-52. [DOI:10.6018/sportk.509311]
- Awad AJ, Ghasemi GA, Sadeghi M, Esmaeili H. The effect of 8 weeks of resistance training on hip and knee flexion angles, proprioception, and muscle performance after ACL reconstruction. Retos. 2025; 69:963-972. [DOI:10.47197/retos.v69.114042]
- Corrigan P, Neogi T, Frey-Law L, et al. Relation of pain sensitization to self-reported and performance-based measures of physical functioning: The MOST study. Osteoarthritis Cartilage. 2023; 31(7):966-975. [DOI:10.1016/j.joca.2023.03.011] [PMID]
- Latini E, Curci ER, Massimiani A, et al. Ultrasonography for oxygen-ozone therapy in musculoskeletal diseases. Medical Gas Research. 2019; 9(1):18-24. [DOI:10.4103/2045-9912.254638] [PMID]
- Porter S. Tidy’s physiotherapy. 15th ed. London: Elsevier; 2009. [Link]
- Stausholm MB, Bjordal JM, Moe-Nilssen R, Naterstad IF. Pain pressure threshold algometry in knee osteoarthritis: Intra- and inter-rater reliability. Physiotherapy Theory and Practice. 2023; 39(3):615-22. [DOI:10.1080/09593985.2021.2023929] [PMID]
- Elvis AM, Ekta JS. Ozone therapy: A clinical review.Journal of Natural Science, Biology and Medicine. 2011; 2(1):66-70. [DOI:10.4103/0976-9668.82319] [PMID]
- Liu Q, Liu J, Cao G, et al. Ozone therapy for knee osteoarthritis: A literature visualization analysis. Medical Gas Research. 2025; 15(2):356-65. [DOI:10.4103/mgr.MEDGASRES-D-24-00099] [PMID]
- Wainstein J, Feldbrin Z, Boaz M, Harman-Boehm I. Efficacy of ozone-oxygen therapy for the treatment of diabetic foot ulcers. Diabetes Technology and Therapeutics. 2011; 13(12):1255-60. [DOI:10.1089/dia.2011.0018] [PMID]
- Andersson ML, Thorén E, Sylwander C, Bergman S. Associations between chronic widespread pain, pressure pain thresholds, leptin, and metabolic factors in individuals with knee pain. BMC Musculoskeletal Disorders. 2023; 24(1):639. [DOI:10.1186/s12891-023-06773-4] [PMID]
- Ekim A, Colak M. Effect of low level laser therapy in rheumatoid arthritis patients with carpal tunnel syndrome. Swiss Medical Weekly. 2007; 137(23-24):347-52. [DOI:10.4414/smw.2007.11581] [PMID]
- Giummarra M, Vocale L, King M. Efficacy of non-surgical management and functional outcomes of partial ACL tears: A systematic review of randomised trials. BMC Musculoskeletal Disorders. 2022; 23:332. [DOI:10.1186/s12891-022-05278-w] [PMID]
- Hashemi J, Chandrashekar N, Gill B, Beynnon BD, Slauterbeck JR, Schutt RC Jr, et al. The geometry of the tibial plateau and its influence on the biomechanics of the tibiofemoral joint. The Journal of Bone and Joint Surgery. 2008; 90(12):2724-34. [DOI:10.2106/JBJS.G.01358] [PMID]
- Jeyaraman M, Jeyaraman N, Ramasubramanian S, Balaji S, Nallakumarasamy A, Patro BP, et al. Ozone therapy in musculoskeletal medicine: A comprehensive review. European Journal of Medical Research. 2024; 29(398):1. [DOI:10.1186/s40001-024-01976-4] [PMID]
- Robertson VJ, Baker KG. A review of therapeutic ultrasound: Effectiveness studies. Physical Therapy. 2001; 81(7):1339-50. [DOI:10.1093/ptj/81.7.1339]
- Adams D, Logerstedt DS, Hunter-Giordano A, Axe MJ, Snyder-Mackler L. Current concepts for anterior cruciate ligament reconstruction: A criterion-based rehabilitation progression. The Journal of Orthopaedic & Sports Physical Therapy. 2012; 42(7):601-14. [DOI:10.2519/jospt.2012.3871] [PMID]
- Mentiplay BF, Perraton LG, Bower KJ, Adair B, Pua YH, Williams GP, et al. Assessment of lower limb muscle strength and power using hand-held and fixed dynamometry: A reliability and validity study. Plos One. 2015; 10(10):e0140822. [DOI:10.1371/journal.pone.0140822] [PMID]
- Hancock GE, Hepworth T, Wembridge K. Accuracy and reliability of knee goniometry methods. Journal of Experimental Orthopaedics. 2018; 5:46. [DOI:10.1186/s40634-018-0161-5] [PMID]
- Nunes A, Leite V. Intra-rater reliability of pressure pain threshold with different algometers in healthy participants. Muscles. 2025; 4(1):5. [DOI:10.3390/muscles4010005] [PMID]
- Sturgill LP, Snyder-Mackler L, Manal TJ, Axe MJ. Interrater reliability of a clinical scale to assess knee joint effusion. The Journal of Orthopaedic & Sports Physical Therapy. 2009; 39(12):845-9. [DOI:10.2519/jospt.2009.3143] [PMID]
- Billingham SA, Whitehead AL, Julious SA. An audit of sample sizes for pilot and feasibility trials being undertaken in the United Kingdom registered in the United Kingdom clinical research network database. BMC Medical Research Methodology. 2013; 13:104. [DOI:10.1186/1471-2288-13-104] [PMID]
- Viebahn-Haensler R, León Fernández OS. Mitochondrial dysfunction, its oxidative stress-induced pathologies and redox bioregulation through low-dose medical ozone: A systematic review. Molecules. 2024; 29(12):2738. [DOI:10.3390/molecules29122738] [PMID]
- Larsen A, Kristensen G, Thorlacius-Ussing O, Oxlund H. The influence of ultrasound on the mechanical properties of healing tendons in rabbits. Acta Orthopaedica. 2005; 76(2):225-30. [DOI:10.1080/00016470510030616] [PMID]
- Calabrò RS, Calderone A, Fiorente N. Neurosciences and sports rehabilitation in ACLR: A narrative review on winning alliance strategies and connecting the dots. Journal of Functional Morphology and Kinesiology. 2025; 10(2):119. [DOI:10.3390/jfmk10020119] [PMID]
- You DZ, Leighton JL, Schneider PS. Current concepts in rehabilitation protocols to optimize patient function following musculoskeletal trauma. Injury. 2020; 51:S5-9. [DOI:10.1016/j.injury.2020.03.047] [PMID]
- Chesterton LS, Sim J, Wright CC, Foster NE. Interrater reliability of algometry in measuring pressure pain thresholds in healthy humans, using multiple raters. The Clinical Journal of Pain. 2007; 23(9):760-6. [DOI:10.1097/AJP.0b013e318154b6ae] [PMID]
Article type: Original Research Articles |
Subject:
Rehabilitation Management
Received: 2025/09/16 | Accepted: 2025/10/20 | Published: 2026/03/26
Received: 2025/09/16 | Accepted: 2025/10/20 | Published: 2026/03/26
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
