
988368
Fri, May 3, 2024

Volume 15, Issue 2 (June 2017)
Iranian Rehabilitation Journal 2017, 15(2): 125-134 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zeynalzadeh Ghoochani B, Derakhshanrad S A, Hosseini S A, Talebian S, Biglarian A, Zeinalzadeh A et al . Investigating the Impact of Dual Task Condition and Visual Manipulation on Healthy Young Old During Non-Dominant Leg Stance. Iranian Rehabilitation Journal 2017; 15 (2) :125-134
URL: http://irj.uswr.ac.ir/article-1-688-en.html
URL: http://irj.uswr.ac.ir/article-1-688-en.html
Bahareh Zeynalzadeh Ghoochani1 
 , Seyed Alireza Derakhshanrad * 1, Seyed Ali Hosseini2 , Saeed Talebian3 , Akbar Biglarian4 , Afsaneh Zeinalzadeh5 , Salman Nazary Moghadam5
, Seyed Alireza Derakhshanrad * 1, Seyed Ali Hosseini2 , Saeed Talebian3 , Akbar Biglarian4 , Afsaneh Zeinalzadeh5 , Salman Nazary Moghadam5
, Seyed Alireza Derakhshanrad * 1, Seyed Ali Hosseini2 , Saeed Talebian3 , Akbar Biglarian4 , Afsaneh Zeinalzadeh5 , Salman Nazary Moghadam5
1- Department of Occupational Therapy, School of Rehabilitation Sciences, Shiraz University of Medical Sciences, Shiraz, Iran.
2- Department of Occupational Therapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Physiotherapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
4- Department of Biostatistics, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
5- Department of Physiotherapy, School of Paramedical, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Department of Occupational Therapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Physiotherapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
4- Department of Biostatistics, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
5- Department of Physiotherapy, School of Paramedical, Mashhad University of Medical Sciences, Mashhad, Iran.
Full-Text [PDF 641 kb]
(1374 Downloads)
| Abstract (HTML) (5556 Views)



Full-Text: (1317 Views)
1. Introduction
Human beings are highly dependent on both of their legs for performing work, during leisure and while accomplishing daily activities. However, the importance of the non-dominant leg is usually neglected in practice and research. Comprehensive understanding of balance mechanism is a prerequisite for any future prevention plan in first, second or third level. This research study is thus aimed to contribute to the persisting knowledge base on the above-mentioned topic. The idea proposed in here is in accordance with Horak‘s opinion, according to which obtaining thoughtful fundamental information may lead to the development of more effective balance rehabilitation and fall prevention plans [1]. For postural analyses, force plate is the most conventionally used method that studies the Center of Pressure (COP) sways in balance studies [2, 3]. It has also been proposed that exploring the underlying nature of COP sways can offer clues towards developing better means of managing displacement.
Although most studies in the field of balance inquiry have been focused on double foot standing [2, 4], the results obtained from them does not quite help in estimating the individual roles of the right and left foot characteristics and their contributions and capabilities in different circumstances. Hence, in this study we focused on the roles of the non-dominant foot, so as to monitor, document, and understand its importance in performing balance functions.
The study employed the dual task paradigm to analyze the balance pattern. In dual task conditions, the person encounters an extra task along with the postural task. Cognitive dual task also conveys the concept of cognitive-postural interaction. According to Raymakers, the impact of cognition on posture deserves to be studied more [5]. Additionally, to change the level of upcoming challenge to balance system, visual input can also be manipulated [6, 7]. Visual input in combination with the focus of attention is known to have an added value in making the situation more complicated just like the circumstances that people encounter in their real life. In the light of the above-mentioned points, this study aimed to explore balance strategy of healthy elderly individuals under cognitive dual task which is complemented with altered visual input during the decreased somatosensory input of standing on the non-dominant leg.
2. Methods
Participants
A sample of twenty active young old with non-dominant left leg from Tehran was conscripted into a cross-sectional study, which was aimed to examine one-legged standing balance pattern on a force plate at Motor Control Laboratory in University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. Based on previous medical history, twenty healthy participants including 14 males and 6 females were recruited in the study. Descriptive information was the mean age of 61.15±1.95 years, 166.9±7.07 centimeters height, weight of 73.9±8.89 kg, and BMI average factor of 26.6±2.8 with MMSE mean scores of 28.25±1.97. They were selected conveniently according to the inclusion criteria followed by four health house centers that function under the supervision of municipality and University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. The equation of:
was used in this cross-sectional research to identify convenient participant’s number for the conduct of the study. The exclusion criteria included the presence of an abnormality, fracture or contracture in spine or lower extremity, balance and vestibular problems, any neurologic disorders, mental or psychological disorders, taking medicines that may affect awareness, having diabetes or any sensory problem, speech pathology and seizure or epilepsy. Inclusion criteria included having an independent active living, due to which they were assumed to be healthy and normal not being frail, and being able to follow the instructions. Ethical considerations of the study were approved by University of Social Welfare and Rehabilitation Sciences Ethical Committee.
Procedure
Four different conditions that were used to assess one leg standing balance on force plate are as follows: Single left leg standing with open eyes (condition “a”), Single left leg standing with open eyes performing Stroop dual task (condition “b”), Single left leg standing with eyes shut (condition “c”) and Single left leg standing with eyes shut under dual task condition (condition “d”).
These tasks were performed in random order to avoid practice or learning effect. The postural test protocol encompassed standing on the non-dominant leg on the force plate. It is worth mentioning that all the participants’ left legs were their non-dominant leg, so all test procedures took place by standing on left leg for all participants without any exception.
Test commenced with describing the cognitive auditory Stroop dual task and 4 postural assessment conditions after filling out the consent form. Since the participants were unfamiliar with the specifications of the Stroop task, three preliminary sample trials were executed by playing Stroop sounds through wireless earphone (LEM-NP10, Taiwan) while the participants were in sitting position. The Stroop test, which was applied as cognitive dual task for condition ‘b’ and ‘d’ consisted of ‘high’ and ‘low’ words which were played in either high or low tone pitch [8].
The correct response to the test would be disregarding the played word itself repeating the tone pitch rapidly. For example, if the word low was produced in high tone pitch, the right response would be “high” and vice versa. Randomized congruency existed between word and its tone. The microphone (LEM-NP10, Taiwan) also recorded the participants’ answers to the stimuli. The error ratio (deduction of error numbers by total), and average reaction time (latency in reacting to the stimulus) of their responses were later analyzed and calculated from these recorded answers [9].
Beginning of stimuli was in 500 ms, the time gap between two following stimuli was randomly calculated to be either 2000 ms or 3000 ms so that anticipatory replies can be eliminated from the study [10]. The participants were required to stand on the force plate (Kistler- sensitivity: 10, sampling rate: 400 Hz) without shoes, eyeing forward, arms on their sides for 20 seconds in 4 distinct conditions that involved different levels of difficulty (adding and removing visual inputs and Stroop task). They were asked to undergo eight conditions that were performed on a random basis so as to inhibit learning effect.
One minute seated rest interval was provided to the participants so that the errors caused due to fatigue can be avoided. For the sake of force plate precision, calibration was done prior to every trial. One of the most important precautions that was taken care of was that the raised leg (non-supporting one) should not have any kind of contact with the force plate surface. In addition, the participants were not allowed to perform small jumps to balance their stance as many people do while standing on one leg (i.e. the participants were asked to stay on one leg but the primary place of foot would be changed after jumps). In the above described two circumstances or in the case of stepping, the rule was violated and in that case the acquired data was not considered void and was not subjected to further analyses. The experiment was performed at the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Data analysis
The postural dependent variables that were considered in the present investigation were categorized into two groups: (1) linear variables, including mean velocity, area, displacement in X axis (Range Side Way), and range of anterior posterior sway in Y axis (Range Fore After); and (2) nonlinear variables, including Entropy X and Entropy Y. In addition, independent variables of visual input and Stroop task during standing on one leg were also considered in the study. Auditory Stroop task (cognitive dual task) performance was measured by error ratio and reaction time.
Data analyses were performed by two statistical tests; the repeated measurement analyses of variance for force plate variables and the paired t-test for dual task data. The statistical assumption of P<0.05 was the reference criteria to accept the significant differences. The R2015a Matlab program, Microsoft Office Excel 2013 and IBM SPSS statistics 20 software were also used for data analyses.
3. Results
Repeated measurement analysis of variance revealed that all postural variables were significantly different except Entropy X (Table 1). Although the test conditions were performed with random order, the differences between them were maintained the symbol code of a- b- c and d were ascribed to them without repeating the full description of each condition every time it was performed. The symbol ‘a’ denoted the single task eyes open condition, ‘b’ referred to eyes open with dual task condition, ‘c’ symbolized eyes shut single task condition and ‘d’ meant dual task with closed eyes condition. Further Post hoc multiple comparisons for each postural variable were performed:
Linear variables: Bonferroni method was used for the detection of the exact conditions in which the differences existed between them.
Variable “Area”: Bonferroni test helped in the identification of the differences between conditions a-c
Human beings are highly dependent on both of their legs for performing work, during leisure and while accomplishing daily activities. However, the importance of the non-dominant leg is usually neglected in practice and research. Comprehensive understanding of balance mechanism is a prerequisite for any future prevention plan in first, second or third level. This research study is thus aimed to contribute to the persisting knowledge base on the above-mentioned topic. The idea proposed in here is in accordance with Horak‘s opinion, according to which obtaining thoughtful fundamental information may lead to the development of more effective balance rehabilitation and fall prevention plans [1]. For postural analyses, force plate is the most conventionally used method that studies the Center of Pressure (COP) sways in balance studies [2, 3]. It has also been proposed that exploring the underlying nature of COP sways can offer clues towards developing better means of managing displacement.
Although most studies in the field of balance inquiry have been focused on double foot standing [2, 4], the results obtained from them does not quite help in estimating the individual roles of the right and left foot characteristics and their contributions and capabilities in different circumstances. Hence, in this study we focused on the roles of the non-dominant foot, so as to monitor, document, and understand its importance in performing balance functions.
The study employed the dual task paradigm to analyze the balance pattern. In dual task conditions, the person encounters an extra task along with the postural task. Cognitive dual task also conveys the concept of cognitive-postural interaction. According to Raymakers, the impact of cognition on posture deserves to be studied more [5]. Additionally, to change the level of upcoming challenge to balance system, visual input can also be manipulated [6, 7]. Visual input in combination with the focus of attention is known to have an added value in making the situation more complicated just like the circumstances that people encounter in their real life. In the light of the above-mentioned points, this study aimed to explore balance strategy of healthy elderly individuals under cognitive dual task which is complemented with altered visual input during the decreased somatosensory input of standing on the non-dominant leg.
2. Methods
Participants
A sample of twenty active young old with non-dominant left leg from Tehran was conscripted into a cross-sectional study, which was aimed to examine one-legged standing balance pattern on a force plate at Motor Control Laboratory in University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. Based on previous medical history, twenty healthy participants including 14 males and 6 females were recruited in the study. Descriptive information was the mean age of 61.15±1.95 years, 166.9±7.07 centimeters height, weight of 73.9±8.89 kg, and BMI average factor of 26.6±2.8 with MMSE mean scores of 28.25±1.97. They were selected conveniently according to the inclusion criteria followed by four health house centers that function under the supervision of municipality and University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. The equation of:
was used in this cross-sectional research to identify convenient participant’s number for the conduct of the study. The exclusion criteria included the presence of an abnormality, fracture or contracture in spine or lower extremity, balance and vestibular problems, any neurologic disorders, mental or psychological disorders, taking medicines that may affect awareness, having diabetes or any sensory problem, speech pathology and seizure or epilepsy. Inclusion criteria included having an independent active living, due to which they were assumed to be healthy and normal not being frail, and being able to follow the instructions. Ethical considerations of the study were approved by University of Social Welfare and Rehabilitation Sciences Ethical Committee.
Procedure
Four different conditions that were used to assess one leg standing balance on force plate are as follows: Single left leg standing with open eyes (condition “a”), Single left leg standing with open eyes performing Stroop dual task (condition “b”), Single left leg standing with eyes shut (condition “c”) and Single left leg standing with eyes shut under dual task condition (condition “d”).
These tasks were performed in random order to avoid practice or learning effect. The postural test protocol encompassed standing on the non-dominant leg on the force plate. It is worth mentioning that all the participants’ left legs were their non-dominant leg, so all test procedures took place by standing on left leg for all participants without any exception.
Test commenced with describing the cognitive auditory Stroop dual task and 4 postural assessment conditions after filling out the consent form. Since the participants were unfamiliar with the specifications of the Stroop task, three preliminary sample trials were executed by playing Stroop sounds through wireless earphone (LEM-NP10, Taiwan) while the participants were in sitting position. The Stroop test, which was applied as cognitive dual task for condition ‘b’ and ‘d’ consisted of ‘high’ and ‘low’ words which were played in either high or low tone pitch [8].
The correct response to the test would be disregarding the played word itself repeating the tone pitch rapidly. For example, if the word low was produced in high tone pitch, the right response would be “high” and vice versa. Randomized congruency existed between word and its tone. The microphone (LEM-NP10, Taiwan) also recorded the participants’ answers to the stimuli. The error ratio (deduction of error numbers by total), and average reaction time (latency in reacting to the stimulus) of their responses were later analyzed and calculated from these recorded answers [9].
Beginning of stimuli was in 500 ms, the time gap between two following stimuli was randomly calculated to be either 2000 ms or 3000 ms so that anticipatory replies can be eliminated from the study [10]. The participants were required to stand on the force plate (Kistler- sensitivity: 10, sampling rate: 400 Hz) without shoes, eyeing forward, arms on their sides for 20 seconds in 4 distinct conditions that involved different levels of difficulty (adding and removing visual inputs and Stroop task). They were asked to undergo eight conditions that were performed on a random basis so as to inhibit learning effect.
One minute seated rest interval was provided to the participants so that the errors caused due to fatigue can be avoided. For the sake of force plate precision, calibration was done prior to every trial. One of the most important precautions that was taken care of was that the raised leg (non-supporting one) should not have any kind of contact with the force plate surface. In addition, the participants were not allowed to perform small jumps to balance their stance as many people do while standing on one leg (i.e. the participants were asked to stay on one leg but the primary place of foot would be changed after jumps). In the above described two circumstances or in the case of stepping, the rule was violated and in that case the acquired data was not considered void and was not subjected to further analyses. The experiment was performed at the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Data analysis
The postural dependent variables that were considered in the present investigation were categorized into two groups: (1) linear variables, including mean velocity, area, displacement in X axis (Range Side Way), and range of anterior posterior sway in Y axis (Range Fore After); and (2) nonlinear variables, including Entropy X and Entropy Y. In addition, independent variables of visual input and Stroop task during standing on one leg were also considered in the study. Auditory Stroop task (cognitive dual task) performance was measured by error ratio and reaction time.
Data analyses were performed by two statistical tests; the repeated measurement analyses of variance for force plate variables and the paired t-test for dual task data. The statistical assumption of P<0.05 was the reference criteria to accept the significant differences. The R2015a Matlab program, Microsoft Office Excel 2013 and IBM SPSS statistics 20 software were also used for data analyses.
3. Results
Repeated measurement analysis of variance revealed that all postural variables were significantly different except Entropy X (Table 1). Although the test conditions were performed with random order, the differences between them were maintained the symbol code of a- b- c and d were ascribed to them without repeating the full description of each condition every time it was performed. The symbol ‘a’ denoted the single task eyes open condition, ‘b’ referred to eyes open with dual task condition, ‘c’ symbolized eyes shut single task condition and ‘d’ meant dual task with closed eyes condition. Further Post hoc multiple comparisons for each postural variable were performed:
Linear variables: Bonferroni method was used for the detection of the exact conditions in which the differences existed between them.
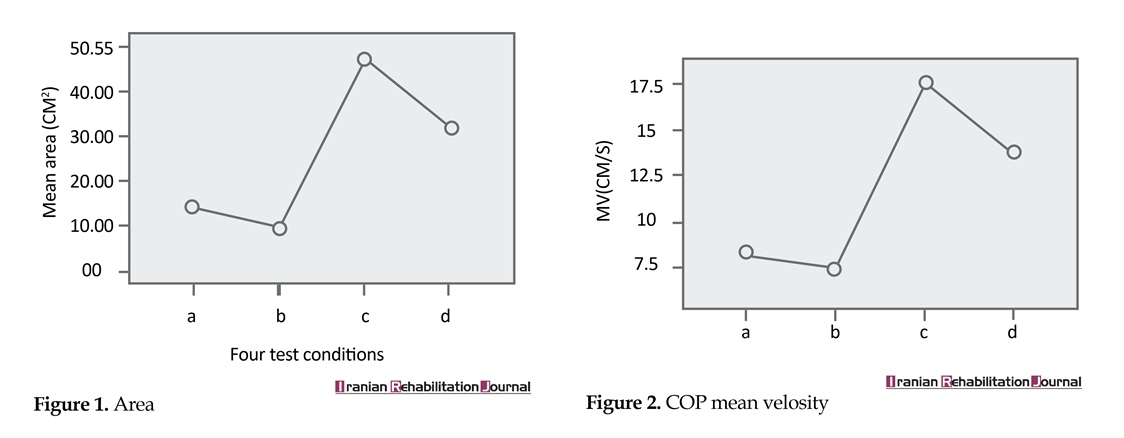
Variable “Area”: Bonferroni test helped in the identification of the differences between conditions a-c

(P<0.0001), a-d (P=0.02), b-c (P=0.0001) and b-d (P<0.0001). Figure 1 represents mean area related to each test condition.
Variable “mean velocity”: Bonferroni test helped in the recognition of the differences between condition a-c (P=0.01), a-d (P=0.002), b-c (P=0.01) and b-d (P=0.0003). Figure 2 depicts mean velocity means related to each test condition.
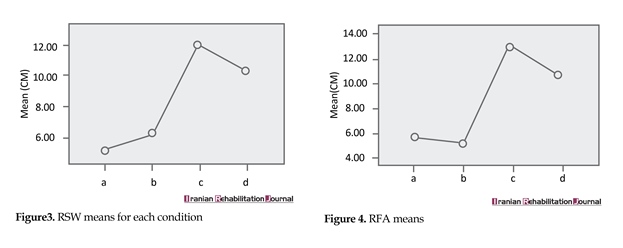
Variable “RSW”: Bonferroni test helped in the calculation of the differences between condition a-c (P<0.0001), a-d (P=0.002), b-c (P=0.01) and b-d (P=0.0004). Figure 3 shows RSW means related to each test condition.
Variable “RFA”: Bonferroni test spotted the differences between condition a-c (P=0.001), a-d (P=0.01), b-c (P=0.0005) and b-d (P=0.004). Figure 4 demonstrates RFA means related to each test condition.
Nonlinear variables
Variable “Entropy X”: Repeated measurement showed no significant differences between different test conditions. Figure 5 signifies Entropy X means related to each test condition. Variable “Entropy Y”: Bonferroni test helped in the identification of the differences between condition a-c (P=0.008). Figure 6 denotes Entropy Y means related to each test condition.
Stroop performance results
According to the results obtained from paired t-test there were no significant differences between cognitive auditory dual task performances during standing on left limb in open eye condition ‘b’ with the closed eyes condition ‘d’. The exact results obtained are described follow; Reaction time during eyes open condition ‘b’ [1.0790±0.06163] and eyes shut condition ‘d’ [0.9919±0.06978], t(13)=1.7, P=0.113, error ratio for eyes open conditionv
Variable “mean velocity”: Bonferroni test helped in the recognition of the differences between condition a-c (P=0.01), a-d (P=0.002), b-c (P=0.01) and b-d (P=0.0003). Figure 2 depicts mean velocity means related to each test condition.
Variable “RSW”: Bonferroni test helped in the calculation of the differences between condition a-c (P<0.0001), a-d (P=0.002), b-c (P=0.01) and b-d (P=0.0004). Figure 3 shows RSW means related to each test condition.
Variable “RFA”: Bonferroni test spotted the differences between condition a-c (P=0.001), a-d (P=0.01), b-c (P=0.0005) and b-d (P=0.004). Figure 4 demonstrates RFA means related to each test condition.
Nonlinear variables
Variable “Entropy X”: Repeated measurement showed no significant differences between different test conditions. Figure 5 signifies Entropy X means related to each test condition. Variable “Entropy Y”: Bonferroni test helped in the identification of the differences between condition a-c (P=0.008). Figure 6 denotes Entropy Y means related to each test condition.
Stroop performance results
According to the results obtained from paired t-test there were no significant differences between cognitive auditory dual task performances during standing on left limb in open eye condition ‘b’ with the closed eyes condition ‘d’. The exact results obtained are described follow; Reaction time during eyes open condition ‘b’ [1.0790±0.06163] and eyes shut condition ‘d’ [0.9919±0.06978], t(13)=1.7, P=0.113, error ratio for eyes open conditionv

(b) [0.1976±0.07479] and closed eyes condition (d) [0.2252±0.06266], t(13)=-0.374, P=0.715.
All participants were found to stand on one leg for 20 seconds, but when it came to dual task conditions or closed eye conditions, these timings could not be maintained. Four participants were not able to do the task with one feet-in-place response during some of these conditions, while many others used stepping strategy instead of being able to maintain balance through the ankle strategy. These four elderly could not concentrate to stay on force plate without putting the raised leg on the floor either in dual task conditions or during eyes closed conditions.
4. Discussion
The linear postural variable change trend during all four conditions indicated that all four linear variables in this study showed significant difference between the conditions: (‘a’ and ‘c’), (‘a’ and ‘d’), (‘b’ and ‘c’) and (‘b’ and ‘d’).
Each two different conditions were scrutinized as follows. The existing differences between condition ‘a’ and ‘c’ were studied by recording the effects of visual input. While condition ‘a’ allowed access to one major sensory input thus contributing to the balance system, the condition ‘c’ eliminated access to this orienting source. Balance system is known to be dependent on three main sources of visual, vestibular and somatosensory inputs [1, 6, 11]. Standing on one leg by itself is challenging due to decreased somatosensory input. Hence, during condition ‘a’ the participants were faced with the challenge of relying on the two other sources of vestibular and visual inputs.
During condition ‘c’ the participants were deprived of more than one source, due to which the load most likely shifts towards the vestibular system. Three individuals’ balance system failed to endure the extra challenges of condition ‘c’ and they could not accomplish the task. These participants were not insisted on accomplishing these tasks due to ethical concerns. Furthermore, their failure was considered as an indicator of the level of difficulty of one leg standing even for healthy elderly individuals. This information can be used as an informative test procedure for clinical and research methods to assess and intervene in the balance system of the elderly population.
The second important point that needs to be discussed is the significant differences between conditions ‘a’ and
All participants were found to stand on one leg for 20 seconds, but when it came to dual task conditions or closed eye conditions, these timings could not be maintained. Four participants were not able to do the task with one feet-in-place response during some of these conditions, while many others used stepping strategy instead of being able to maintain balance through the ankle strategy. These four elderly could not concentrate to stay on force plate without putting the raised leg on the floor either in dual task conditions or during eyes closed conditions.
4. Discussion
The linear postural variable change trend during all four conditions indicated that all four linear variables in this study showed significant difference between the conditions: (‘a’ and ‘c’), (‘a’ and ‘d’), (‘b’ and ‘c’) and (‘b’ and ‘d’).
Each two different conditions were scrutinized as follows. The existing differences between condition ‘a’ and ‘c’ were studied by recording the effects of visual input. While condition ‘a’ allowed access to one major sensory input thus contributing to the balance system, the condition ‘c’ eliminated access to this orienting source. Balance system is known to be dependent on three main sources of visual, vestibular and somatosensory inputs [1, 6, 11]. Standing on one leg by itself is challenging due to decreased somatosensory input. Hence, during condition ‘a’ the participants were faced with the challenge of relying on the two other sources of vestibular and visual inputs.
During condition ‘c’ the participants were deprived of more than one source, due to which the load most likely shifts towards the vestibular system. Three individuals’ balance system failed to endure the extra challenges of condition ‘c’ and they could not accomplish the task. These participants were not insisted on accomplishing these tasks due to ethical concerns. Furthermore, their failure was considered as an indicator of the level of difficulty of one leg standing even for healthy elderly individuals. This information can be used as an informative test procedure for clinical and research methods to assess and intervene in the balance system of the elderly population.
The second important point that needs to be discussed is the significant differences between conditions ‘a’ and

‘c’ from the perspective of increased means in all four linear variables (as depicted in Figures 1, 2, 3 and 4). There is an obvious upward trend for Area, RFA, RSW, MV from condition ‘a’ to ‘c’. Based on traditional assumptions, increased sway can be ascribed to poor balance. Since, condition ‘c’ was the only one that could not be accomplished by all the participants, it was logical to assume it to be the most difficult condition. In addition, the increased sway recorded in participants who did accomplish the condition ‘c’ was indicative of poor balance. According to new theoretical perspective of optimal variability [12-14], this increased amount may still be at the optimal range of variability for those elderly who were able to perform the test.
However, this concept does not represent eyes closed condition as an easy test condition, but it only implies that this increased sway may have happened in the neutral possible range of variability. Thus, this should not be assumed as any pathological or abnormal pattern. Although it is not atypical but it is prone to create risky circumstances in which balance change occurs. In other words, this condition can be the Achilles Heel of balance system of elderly individuals in real life conditions in which they are in a dark room bearing weight on one leg. Based on the obtained results and the significant increase in swaying behavior, standing on a non-dominant leg with eyes shut is susceptible to the risk of falling. Hence, this should be taken into consideration as an important aspect of elderly balance, even those who are healthy and active.
Early detection is an important issue in promoting balance in elderly individuals. This can be made possible only by applying special test conditions to instigate balance system to reveal its efficacy and inefficiency. One of these mentioned conditions is non-dominant leg stance with eyes closed. During condition ‘a’ participants showed acceptable stability in their balance and it was not easy to distinguish those whose balance may encounter difficulties in future. When harder tasks were presented in condition ‘c,’ hidden and invisible problems in balance systems became apparent.
This condition can be used to detect and categorize those who may be at higher risk of falling in their life so that appropriate preventive measures can be adopted to avoid probable falls in the future. Without these interventions, the time when these balance problems become apparent and recognizable; it is already too late to use preventive measures. Hence, preventive measures should be immediately initiated as soon as balance problems are detected. Consequently, non-dominant stance with eyes shut should receive extra attention in conventional balance assessment procedures among the elderly.
If ignored or neglected, this may further increase the risk of fall as the person ages. Therefore, condition ‘c’ is suggested to be considered as an integral part of routine clinical and professional balance assessment programs. Furthermore, its application in community sports can be studied in future studies to identify and imply it on a larger scale. It is also questionable whether elderly could conquer this challenge if they were used to performing postural task with eyes shut during their youth. The found differences between condition ‘a’ and ‘c’ are in agreement with the findings reported by Teasdale [7] and Eikma [15].
The findings of the present study are also in line with the opinion of Brocklehurst et al. [16], Black et al. [17] and Diener et al. [18], according to which normal individuals’ COP increases when they close their eyes. The current study result shows increased sway in the eyes shut condition which corresponds with earlier findings of Blaszczyk [19]. Based on the findings in existing articles and the current study, eyes shut stance should become a high priority condition in fall prevention agenda.
Regarding the differences between condition ‘b’ and ‘c’, there are two issues of dual task performance in condition ‘b’ as compared with the eyes shut condition ‘c’. According to the analysis of changes in the four linear variables, swaying was considerably less in dual task condition with open eyes. One possible explanation for such behavior is the availability of visual source in condition ‘b’. It is supposed that the dual task diverts the individual’s attention from postural task, due to which postural task becomes automatic [20].
This phenomenon was also observed in the present study and is quite evident from the results presented in Figure 1, 2, 3, and 4. Another decline from condition ‘c’ to ‘d’ due to dual task effect was also recorded. However, this decrease was not statistically significant, but it was worth mentioning to support the difference between conditions ‘b’ and ‘c’, and thereby showcasing the effects of dual task performance.
Effects of dual task represented in Figures 1, 2, 3 and 4 demonstrate reducer effect. The decreased amount of sway refers to dual task effect. When eyes were closed during conditions ‘c’ and ‘d’, dual task reduced the sway to a lower amount. Therefore, dual task is accompanied by a decrease in the amount of sway that creates its own special pattern. Investigators can also consider this new concept of synergistic association between postural and cognitive tasks, especially because it seems to negate the pre-assumed notion of competition for attentional sources between them [21].
The clinical implication of such dual tasks involves its prescription during hard and challenging postural conditions so as to control swaying due to increased automaticity. These findings are in line with Swan’s [22] point of view about balance enhancement by performing a secondary cognitive dual task. During dual task performance, individuals would experience a major contraction in all body muscles so that swaying can be controlled and the participants are available for answering the stimuli while maintaining balance. As a result the participants swayed less during dual task conditions and they survived the difficult situation.
However, there is a flip side to this coin, decreased sway induced by freezing or damping effect may decrease the degree of freedom of the balance system of the participants. Hence, this interpretation of decreased sway by dual task is complicated. The persisting ambiguity of its implication left the question of whether dual tasks help in improving balance of elderly individuals still unanswered. In fact, decreased sway in patients suffering from Parkinson’s disease [23, 24] has created a new domain for debate against the traditional interpretation of decreased sway as an indicator of good balance.
Differences between conditions ‘a’ and ‘d’ and conditions ‘b’ and ‘d’ was mainly due to eyes shut effect during condition ‘d’. Closing the eyes increased the sway of the participants in the conditions ‘a’ and ‘b’. One of the participants could not complete the condition ‘b, while condition ‘d’ could not be completed by four participants. The failure of participants to accomplish the tasks is in agreement with Woollacott’s [11] propositions, according to which elderly individuals may lose their balance when somatosensory and visual inputs are manipulated. Another explanation for this is based on special terms and instruction of standing, including non-weight bearing leg not touching the force plate or not making small leaps while standing on one leg.
According to Jonsson, changes in force and muscular parts were also found to contribute to loss of balance during one leg stance. Furthermore, it was also proposed that the first 5 seconds of one leg standing are the most precarious and perilous phase during which the difficulty of maintaining balance and one leg standing is at its highest [25]. This dynamic phase of transition from double leg to one leg standing is one of the most determinative challenges to the functional maintenance of the balance system. This very reason was considered as the major contributing factor behind the inability of healthy participants to start and hold their one leg stand. These propositions are also in agreement with that of Bohannon and Briggs et al., who found that single limb stance is difficult for the elderly [26, 27].
These findings were also congruent with the results obtained by Bryant, according to which over half of the study participants were at the time of retirement failed to finish all three one leg stance tests [28]. Another explanation to this could be the increasing levels of difficulty of conditions ‘b’, ‘c’ and ‘d’ as compared to condition ‘a’. Zeynalzadeh et al. found that double leg stance of healthy elderly is susceptible to changes only in the presence of two simultaneous challenges - visual deprivation and dual task. As opposed to the double leg stance, one leg stance was found to be more prone to internal and external inputs and manipulations [29].
Another crucial aspect that influences one leg standing is the ankle strategy [30]. Mediolateral and anterior-posterior sway highlights the importance of evertor/invertor and dorsi/plantar flexor muscle activity. In fact, the reason behind the inability of the participants to accomplish the one leg stance was the failure of ankle strategy and failure to show feet-in-place response. These participants mainly used the stepping strategy, were unable to manage sway by concentrated muscle activity in the ankle region or could not follow the pendulum model. One specific point that needs to be considered while planning any balance program is to devise suitable methods for training or strengthening ankle muscles. New insight into mediolateral and anterior-posterior characters may help in increasing the levels of awareness on development of evidence based and science driven health promotion perspective and plans.
As far as studies on the nonlinear aspects of balance are concerned, the balance pattern is fascinatingly different from linear variable change patterns. Firstly, the recorded values of Entropy X were not significantly different. It showed that although participant’s sways were different during four conditions, but the hidden nature of sway regularity was not significantly different in the frontal plane. Secondly, the only significant difference between conditions ‘a’ and ‘c’ was for Entropy Y. Different levels of predictability and degree of freedom for these two conditions were shown.
5. Conclusion
The major reason behind the differences of pattern between linear and nonlinear variables was that the balance characteristics and dynamics were beyond the sway displacement dependent amounts (linear variable). Furthermore, it was also influenced by the regularity of sway movements and its predictability (non-linear variable) thereby disclosing subtle substrate mechanisms. In other words, linear variables filter the sway displacement in a quantitative manner, while nonlinear variables regardless of the sway amount represent the sway regularity pattern changes concerning the complexity of pattern and underlying random features. Hence, it is recommended to study these linear and non-linear postural variables together in a balance study to reveal the explicit and implicit underlying patterns of the same.
The last point is related to cognitive dual task performance of Stroop test. There were no significant differences between cognitive performance of auditory Stroop between conditions ‘b’ and ‘d’. It was also found that the participants’ reaction time was less during eyes shut condition ‘d’ as compared to the open eyes condition ‘b’. However, error ratio was higher during closed eyes condition “d’ than that of ‘b’. Since the result about the reaction time and error ratio were not significantly different, it would be better to avoid deducing any rigid or absolute interpretation from them. It can only be supposed that concurrent cognitive auditory Stroop task performance was not significantly different between condition ‘b’ and ‘d’, and in fact, it was not influenced by visual input being present or absent.
One leg standing is a very challenging condition with the primary challenge of decreased somatosensory input of one leg. It is suggested as one of the most informative test condition by adding extra challenges such as; dual task or visual deprivation. Increased level of difficulty during one leg stance would increase responsiveness of one leg standing to screen balancing problems when elderly do not show balance problem during merely one leg standing.
Non-dominant leg did not show constant and stable balance pattern during dual task conditions concurrent with visual manipulation. Since the most vulnerable condition was eyes shut condition, it is seriously recommended to be monitored. Its vulnerability and susceptibility among the elderly may turn it into an Achilles heel of balance system. It is recommended that fall prevention strategies should concentrate on such conditions, it is highly recommended that non-dominant leg standing with closed eyes be included in enablement programs and empowerment protocols of a capable balance system. Furthermore, dual task was proved to be a sway modulator which can be used during performing difficult postural tasks to make balance more automatic and less dependent on conscious cognitive sources which may sometimes deviate the attention of the individual towards the second task.
The most important limitation of the study was restricted access to the force plate due to limited and scheduled time assigned to use it. Though the present study helped in the identification of specific dual task conditions that may pose a risk on the balance of elderly individuals, even in real life, it is important to note that all the participants had left leg as the non-dominant leg. Hence, it is highly recommended that similar studies in which participants with right non-dominant leg are also included, be conducted. Increased level of difficulty is also suggested to be an integral part of assessment procedures as shown to be effective in this study, but their applicability as clinical intervention methods needs to be investigated in future studies. Comparative analysis of the underlying factors and risks associated right and left non-dominant legs should also be explored in future studies.
Acknowledgments
Special thanks go to Pezhman Lali, Nabavi, Talimkhani and Argasi for their contribution in the conduct of the study. This study was not funded but ethically approved by ethical committee of University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Conflicts of Interest
All authors certify that this manuscript has neither been published in whole nor in part nor being considered for publication elsewhere. The authors have no conflicts of interest to declare.
References
[1]Horak FB. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls. Age and Ageing. 2006; 35(Supplement 2):7–11. doi: 10.1093/ageing/afl077
[2]Blaszczyk JW, Prince F, Raiche M, Hébert R. Effect of ageing and vision on limb load asymmetry during quiet stance. Journal of Biomechanics. 2000; 33(10):1243–8. doi: 10.1016/s0021-9290(00)00097-x
[3]Era P, Heikkinen E, Gause-Nilsson I, Schroll M. Postural balance in elderly people: Changes over a five-year follow-up and its predictive value for survival. Aging clinical and experimental research. 2002; 14(3 Suppl):37-46. PMID: 12475132
[4]Redfern MS, Jennings JR, Martin C, Furman JM. Attention influences sensory integration for postural control in older adults. Gait & Posture. 2001; 14(3):211–6. doi: 10.1016/s0966-6362(01)00144-8
[5]Raymakers JA, Samson MM, Verhaar HJJ. The assessment of body sway and the choice of the stability parameter(s). Gait & Posture. 2005; 21(1):48–58. doi: 10.1016/j.gaitpost.2003.11.006
[6]Manchester D, Woollacott M, Zederbauer-Hylton N, Marin O. Visual, vestibular and somatosensory contributions to balance control in the older adult. Journal of Gerontology. 1989; 44(4):118–27. doi: 10.1093/geronj/44.4.m118
[7]Teasdale N, Stelmach GE, Breunig A, Meeuwsen HJ. Age differences in visual sensory integration. Experimental Brain Research. 1991; 85(3). doi: 10.1007/bf00231755
[8]Siu KC, Lugade V, Chou LS, van Donkelaar P, Woollacott MH. Dual-task interference during obstacle clearance in healthy and balance-impaired older adults. Aging Clinical and Experimental Research. 2008; 20(4):349–54. doi: 10.1007/bf03324867
[9]Green EJ, Barber PJ. Interference effects in an auditory stroop task: Congruence and correspondence. Acta Psychologica. 1983; 53(3):183–94. doi: 10.1016/0001-6918(83)90001-x
[10]Mohammadirad S, Salavati M, Takamjani IE, Akhbari B, Sherafat S, Mazaheri M, et al. Intra and intersession reliability of a postural control protocol in athletes with and without anterior cruciate ligament reconstruction: A dual-task paradigm. International Journal of Sports Physical Therapy. 2012; 7(6):627-36. PMCID: PMC3537456
[11]Woollacott MH, Shumway-Cook A. Changes in posture control across the life span—a systems approach. Physical Therapy. 1990; 70(12):799–807. doi: 10.1093/ptj/70.12.799
[12]Stergiou N, Harbourne RT, Cavanaugh JT. Optimal movement variability. Journal of Neurologic Physical Therapy. 2006; 30(3):120–9. doi: 10.1097/01.npt.0000281949.48193.d9
[13]Harbourne RT, Stergiou N. Movement variability and the use of nonlinear tools: Principles to guide physical therapist practice. Physical Therapy. 2009; 89(3):267–82. doi: 10.2522/ptj.20080130
[14]Stergiou N, Decker LM. Human movement variability, nonlinear dynamics, and pathology: Is there a connection. Human Movement Science. 2011; 30(5):869–88. doi: 10.1016/j.humov.2011.06.002
[15]Eikema DJA, Hatzitaki V, Tzovaras D, Papaxanthis C. Age-dependent modulation of sensory reweighting for controlling posture in a dynamic virtual environment. AGE. 2011; 34(6):1381–92. doi: 10.1007/s11357-011-9310-9
[16]Brocklehurst JC, Robertson D, James-Groom P. Clinical correlates of sway in old age—sensory modalities. Age and Ageing. 1982; 11(1):1–10. doi: 10.1093/ageing/11.1.1
[17]Black FO, Wall C, Rockette HE, Kitch R. Normal subject postural sway during the romberg test. American Journal of Otolaryngology. 1982; 3(5):309–18. doi: 10.1016/s0196-0709(82)80002-1
[18]Diener H., Dichgans J, Bacher M, Gompf B. Quantification of postural sway in normals and patients with cerebellar diseases. Electroencephalography and Clinical Neurophysiology. 1984; 57(2):134–42. doi: 10.1016/0013-4694(84)90172-x
[19]Blaszczyk JW, Klonowski W. Postural stability and fractal dynamics. Acta Neurobiol. 2001; 61:105-12.
[20]Ruffieux J, Keller M, Lauber B, Taube W. Changes in standing and walking performance under dual-task conditions across the life span. Sports Medicine. 2015; 45(12):1739–58. doi: 10.1007/s40279-015-0369-9
[21]Bonnet CT, Baudry S. Active vision task and postural control in healthy, young adults: Synergy and probably not duality. Gait & Posture. 2016; 48:57–63. doi: 10.1016/j.gaitpost.2016.04.016
[22]Swan L, Otani H, Loubert PV, Sheffert SM, Dunbar GL. Improving balance by performing a secondary cognitive task. British Journal of Psychology. 2004; 95(1):31–40. doi: 10.1348/000712604322779442
[23]Horak FB, Nutt JG, Nashner LM. Postural inflexibility in parkinsonian subjects. Journal of the Neurological Sciences. 1992; 111(1):46–58. doi: 10.1016/0022-510x(92)90111-w
[24]Van Emmerik REA, Van Wegen EEH. On the functional aspects of variability in postural control. Exercise and Sport Sciences Reviews . 2002; 30(4):177–83. doi: 10.1097/00003677-200210000-00007
[25]Jonsson E, Seiger Å, Hirschfeld H. One-leg stance in healthy young and elderly adults: A measure of postural steadiness. Clinical Biomechanics. 2004; 19(7):688–94. doi: 10.1016/j.clinbiomech.2004.04.002
[26]Bohannon RW. One-legged balance test times. Perceptual and Motor Skills. 1994; 78(3):801–2. doi: 10.1177/003151259407800322
[27]Briggs RC, Gossman MR, Birch R, Drews JE, Shaddeau SA. Balance performance among non institutionalized elderly women. Physical Therapy. 1989; 69(9):748–56. doi: 10.1093/ptj/69.9.748
[28]Bryant EC, Trew ME, Bruce AM, Kuisma RME, Smith AW. Gender differences in balance performance at the time of retirement. Clinical Biomechanics. 2005; 20(3):330–5. doi: 10.1016/j.clinbiomech.2004.11.006
[29]Zeynalzadeh Ghoochani B, Hosseini SA, Talebian S, Biglarian A, Zeinalzadeh A, Nazary-Moghadam S, et al. Healthy older adults balance pattern under dual task conditions: Exploring the strategy and trend. Health Promotion Perspectives. 2016; 6(4):207–12. doi: 10.15171/hpp.2016.34
[30]Clifford AM, Holder-Powell H. Postural control in healthy individuals. Clinical Biomechanics. 2010; 25(6):546–51. doi: 10.1016/j.clinbiomech.2010.03.005
However, this concept does not represent eyes closed condition as an easy test condition, but it only implies that this increased sway may have happened in the neutral possible range of variability. Thus, this should not be assumed as any pathological or abnormal pattern. Although it is not atypical but it is prone to create risky circumstances in which balance change occurs. In other words, this condition can be the Achilles Heel of balance system of elderly individuals in real life conditions in which they are in a dark room bearing weight on one leg. Based on the obtained results and the significant increase in swaying behavior, standing on a non-dominant leg with eyes shut is susceptible to the risk of falling. Hence, this should be taken into consideration as an important aspect of elderly balance, even those who are healthy and active.
Early detection is an important issue in promoting balance in elderly individuals. This can be made possible only by applying special test conditions to instigate balance system to reveal its efficacy and inefficiency. One of these mentioned conditions is non-dominant leg stance with eyes closed. During condition ‘a’ participants showed acceptable stability in their balance and it was not easy to distinguish those whose balance may encounter difficulties in future. When harder tasks were presented in condition ‘c,’ hidden and invisible problems in balance systems became apparent.
This condition can be used to detect and categorize those who may be at higher risk of falling in their life so that appropriate preventive measures can be adopted to avoid probable falls in the future. Without these interventions, the time when these balance problems become apparent and recognizable; it is already too late to use preventive measures. Hence, preventive measures should be immediately initiated as soon as balance problems are detected. Consequently, non-dominant stance with eyes shut should receive extra attention in conventional balance assessment procedures among the elderly.
If ignored or neglected, this may further increase the risk of fall as the person ages. Therefore, condition ‘c’ is suggested to be considered as an integral part of routine clinical and professional balance assessment programs. Furthermore, its application in community sports can be studied in future studies to identify and imply it on a larger scale. It is also questionable whether elderly could conquer this challenge if they were used to performing postural task with eyes shut during their youth. The found differences between condition ‘a’ and ‘c’ are in agreement with the findings reported by Teasdale [7] and Eikma [15].
The findings of the present study are also in line with the opinion of Brocklehurst et al. [16], Black et al. [17] and Diener et al. [18], according to which normal individuals’ COP increases when they close their eyes. The current study result shows increased sway in the eyes shut condition which corresponds with earlier findings of Blaszczyk [19]. Based on the findings in existing articles and the current study, eyes shut stance should become a high priority condition in fall prevention agenda.
Regarding the differences between condition ‘b’ and ‘c’, there are two issues of dual task performance in condition ‘b’ as compared with the eyes shut condition ‘c’. According to the analysis of changes in the four linear variables, swaying was considerably less in dual task condition with open eyes. One possible explanation for such behavior is the availability of visual source in condition ‘b’. It is supposed that the dual task diverts the individual’s attention from postural task, due to which postural task becomes automatic [20].
This phenomenon was also observed in the present study and is quite evident from the results presented in Figure 1, 2, 3, and 4. Another decline from condition ‘c’ to ‘d’ due to dual task effect was also recorded. However, this decrease was not statistically significant, but it was worth mentioning to support the difference between conditions ‘b’ and ‘c’, and thereby showcasing the effects of dual task performance.
Effects of dual task represented in Figures 1, 2, 3 and 4 demonstrate reducer effect. The decreased amount of sway refers to dual task effect. When eyes were closed during conditions ‘c’ and ‘d’, dual task reduced the sway to a lower amount. Therefore, dual task is accompanied by a decrease in the amount of sway that creates its own special pattern. Investigators can also consider this new concept of synergistic association between postural and cognitive tasks, especially because it seems to negate the pre-assumed notion of competition for attentional sources between them [21].
The clinical implication of such dual tasks involves its prescription during hard and challenging postural conditions so as to control swaying due to increased automaticity. These findings are in line with Swan’s [22] point of view about balance enhancement by performing a secondary cognitive dual task. During dual task performance, individuals would experience a major contraction in all body muscles so that swaying can be controlled and the participants are available for answering the stimuli while maintaining balance. As a result the participants swayed less during dual task conditions and they survived the difficult situation.
However, there is a flip side to this coin, decreased sway induced by freezing or damping effect may decrease the degree of freedom of the balance system of the participants. Hence, this interpretation of decreased sway by dual task is complicated. The persisting ambiguity of its implication left the question of whether dual tasks help in improving balance of elderly individuals still unanswered. In fact, decreased sway in patients suffering from Parkinson’s disease [23, 24] has created a new domain for debate against the traditional interpretation of decreased sway as an indicator of good balance.
Differences between conditions ‘a’ and ‘d’ and conditions ‘b’ and ‘d’ was mainly due to eyes shut effect during condition ‘d’. Closing the eyes increased the sway of the participants in the conditions ‘a’ and ‘b’. One of the participants could not complete the condition ‘b, while condition ‘d’ could not be completed by four participants. The failure of participants to accomplish the tasks is in agreement with Woollacott’s [11] propositions, according to which elderly individuals may lose their balance when somatosensory and visual inputs are manipulated. Another explanation for this is based on special terms and instruction of standing, including non-weight bearing leg not touching the force plate or not making small leaps while standing on one leg.
According to Jonsson, changes in force and muscular parts were also found to contribute to loss of balance during one leg stance. Furthermore, it was also proposed that the first 5 seconds of one leg standing are the most precarious and perilous phase during which the difficulty of maintaining balance and one leg standing is at its highest [25]. This dynamic phase of transition from double leg to one leg standing is one of the most determinative challenges to the functional maintenance of the balance system. This very reason was considered as the major contributing factor behind the inability of healthy participants to start and hold their one leg stand. These propositions are also in agreement with that of Bohannon and Briggs et al., who found that single limb stance is difficult for the elderly [26, 27].
These findings were also congruent with the results obtained by Bryant, according to which over half of the study participants were at the time of retirement failed to finish all three one leg stance tests [28]. Another explanation to this could be the increasing levels of difficulty of conditions ‘b’, ‘c’ and ‘d’ as compared to condition ‘a’. Zeynalzadeh et al. found that double leg stance of healthy elderly is susceptible to changes only in the presence of two simultaneous challenges - visual deprivation and dual task. As opposed to the double leg stance, one leg stance was found to be more prone to internal and external inputs and manipulations [29].
Another crucial aspect that influences one leg standing is the ankle strategy [30]. Mediolateral and anterior-posterior sway highlights the importance of evertor/invertor and dorsi/plantar flexor muscle activity. In fact, the reason behind the inability of the participants to accomplish the one leg stance was the failure of ankle strategy and failure to show feet-in-place response. These participants mainly used the stepping strategy, were unable to manage sway by concentrated muscle activity in the ankle region or could not follow the pendulum model. One specific point that needs to be considered while planning any balance program is to devise suitable methods for training or strengthening ankle muscles. New insight into mediolateral and anterior-posterior characters may help in increasing the levels of awareness on development of evidence based and science driven health promotion perspective and plans.
As far as studies on the nonlinear aspects of balance are concerned, the balance pattern is fascinatingly different from linear variable change patterns. Firstly, the recorded values of Entropy X were not significantly different. It showed that although participant’s sways were different during four conditions, but the hidden nature of sway regularity was not significantly different in the frontal plane. Secondly, the only significant difference between conditions ‘a’ and ‘c’ was for Entropy Y. Different levels of predictability and degree of freedom for these two conditions were shown.
5. Conclusion
The major reason behind the differences of pattern between linear and nonlinear variables was that the balance characteristics and dynamics were beyond the sway displacement dependent amounts (linear variable). Furthermore, it was also influenced by the regularity of sway movements and its predictability (non-linear variable) thereby disclosing subtle substrate mechanisms. In other words, linear variables filter the sway displacement in a quantitative manner, while nonlinear variables regardless of the sway amount represent the sway regularity pattern changes concerning the complexity of pattern and underlying random features. Hence, it is recommended to study these linear and non-linear postural variables together in a balance study to reveal the explicit and implicit underlying patterns of the same.
The last point is related to cognitive dual task performance of Stroop test. There were no significant differences between cognitive performance of auditory Stroop between conditions ‘b’ and ‘d’. It was also found that the participants’ reaction time was less during eyes shut condition ‘d’ as compared to the open eyes condition ‘b’. However, error ratio was higher during closed eyes condition “d’ than that of ‘b’. Since the result about the reaction time and error ratio were not significantly different, it would be better to avoid deducing any rigid or absolute interpretation from them. It can only be supposed that concurrent cognitive auditory Stroop task performance was not significantly different between condition ‘b’ and ‘d’, and in fact, it was not influenced by visual input being present or absent.
One leg standing is a very challenging condition with the primary challenge of decreased somatosensory input of one leg. It is suggested as one of the most informative test condition by adding extra challenges such as; dual task or visual deprivation. Increased level of difficulty during one leg stance would increase responsiveness of one leg standing to screen balancing problems when elderly do not show balance problem during merely one leg standing.
Non-dominant leg did not show constant and stable balance pattern during dual task conditions concurrent with visual manipulation. Since the most vulnerable condition was eyes shut condition, it is seriously recommended to be monitored. Its vulnerability and susceptibility among the elderly may turn it into an Achilles heel of balance system. It is recommended that fall prevention strategies should concentrate on such conditions, it is highly recommended that non-dominant leg standing with closed eyes be included in enablement programs and empowerment protocols of a capable balance system. Furthermore, dual task was proved to be a sway modulator which can be used during performing difficult postural tasks to make balance more automatic and less dependent on conscious cognitive sources which may sometimes deviate the attention of the individual towards the second task.
The most important limitation of the study was restricted access to the force plate due to limited and scheduled time assigned to use it. Though the present study helped in the identification of specific dual task conditions that may pose a risk on the balance of elderly individuals, even in real life, it is important to note that all the participants had left leg as the non-dominant leg. Hence, it is highly recommended that similar studies in which participants with right non-dominant leg are also included, be conducted. Increased level of difficulty is also suggested to be an integral part of assessment procedures as shown to be effective in this study, but their applicability as clinical intervention methods needs to be investigated in future studies. Comparative analysis of the underlying factors and risks associated right and left non-dominant legs should also be explored in future studies.
Acknowledgments
Special thanks go to Pezhman Lali, Nabavi, Talimkhani and Argasi for their contribution in the conduct of the study. This study was not funded but ethically approved by ethical committee of University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Conflicts of Interest
All authors certify that this manuscript has neither been published in whole nor in part nor being considered for publication elsewhere. The authors have no conflicts of interest to declare.
References
[1]Horak FB. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls. Age and Ageing. 2006; 35(Supplement 2):7–11. doi: 10.1093/ageing/afl077
[2]Blaszczyk JW, Prince F, Raiche M, Hébert R. Effect of ageing and vision on limb load asymmetry during quiet stance. Journal of Biomechanics. 2000; 33(10):1243–8. doi: 10.1016/s0021-9290(00)00097-x
[3]Era P, Heikkinen E, Gause-Nilsson I, Schroll M. Postural balance in elderly people: Changes over a five-year follow-up and its predictive value for survival. Aging clinical and experimental research. 2002; 14(3 Suppl):37-46. PMID: 12475132
[4]Redfern MS, Jennings JR, Martin C, Furman JM. Attention influences sensory integration for postural control in older adults. Gait & Posture. 2001; 14(3):211–6. doi: 10.1016/s0966-6362(01)00144-8
[5]Raymakers JA, Samson MM, Verhaar HJJ. The assessment of body sway and the choice of the stability parameter(s). Gait & Posture. 2005; 21(1):48–58. doi: 10.1016/j.gaitpost.2003.11.006
[6]Manchester D, Woollacott M, Zederbauer-Hylton N, Marin O. Visual, vestibular and somatosensory contributions to balance control in the older adult. Journal of Gerontology. 1989; 44(4):118–27. doi: 10.1093/geronj/44.4.m118
[7]Teasdale N, Stelmach GE, Breunig A, Meeuwsen HJ. Age differences in visual sensory integration. Experimental Brain Research. 1991; 85(3). doi: 10.1007/bf00231755
[8]Siu KC, Lugade V, Chou LS, van Donkelaar P, Woollacott MH. Dual-task interference during obstacle clearance in healthy and balance-impaired older adults. Aging Clinical and Experimental Research. 2008; 20(4):349–54. doi: 10.1007/bf03324867
[9]Green EJ, Barber PJ. Interference effects in an auditory stroop task: Congruence and correspondence. Acta Psychologica. 1983; 53(3):183–94. doi: 10.1016/0001-6918(83)90001-x
[10]Mohammadirad S, Salavati M, Takamjani IE, Akhbari B, Sherafat S, Mazaheri M, et al. Intra and intersession reliability of a postural control protocol in athletes with and without anterior cruciate ligament reconstruction: A dual-task paradigm. International Journal of Sports Physical Therapy. 2012; 7(6):627-36. PMCID: PMC3537456
[11]Woollacott MH, Shumway-Cook A. Changes in posture control across the life span—a systems approach. Physical Therapy. 1990; 70(12):799–807. doi: 10.1093/ptj/70.12.799
[12]Stergiou N, Harbourne RT, Cavanaugh JT. Optimal movement variability. Journal of Neurologic Physical Therapy. 2006; 30(3):120–9. doi: 10.1097/01.npt.0000281949.48193.d9
[13]Harbourne RT, Stergiou N. Movement variability and the use of nonlinear tools: Principles to guide physical therapist practice. Physical Therapy. 2009; 89(3):267–82. doi: 10.2522/ptj.20080130
[14]Stergiou N, Decker LM. Human movement variability, nonlinear dynamics, and pathology: Is there a connection. Human Movement Science. 2011; 30(5):869–88. doi: 10.1016/j.humov.2011.06.002
[15]Eikema DJA, Hatzitaki V, Tzovaras D, Papaxanthis C. Age-dependent modulation of sensory reweighting for controlling posture in a dynamic virtual environment. AGE. 2011; 34(6):1381–92. doi: 10.1007/s11357-011-9310-9
[16]Brocklehurst JC, Robertson D, James-Groom P. Clinical correlates of sway in old age—sensory modalities. Age and Ageing. 1982; 11(1):1–10. doi: 10.1093/ageing/11.1.1
[17]Black FO, Wall C, Rockette HE, Kitch R. Normal subject postural sway during the romberg test. American Journal of Otolaryngology. 1982; 3(5):309–18. doi: 10.1016/s0196-0709(82)80002-1
[18]Diener H., Dichgans J, Bacher M, Gompf B. Quantification of postural sway in normals and patients with cerebellar diseases. Electroencephalography and Clinical Neurophysiology. 1984; 57(2):134–42. doi: 10.1016/0013-4694(84)90172-x
[19]Blaszczyk JW, Klonowski W. Postural stability and fractal dynamics. Acta Neurobiol. 2001; 61:105-12.
[20]Ruffieux J, Keller M, Lauber B, Taube W. Changes in standing and walking performance under dual-task conditions across the life span. Sports Medicine. 2015; 45(12):1739–58. doi: 10.1007/s40279-015-0369-9
[21]Bonnet CT, Baudry S. Active vision task and postural control in healthy, young adults: Synergy and probably not duality. Gait & Posture. 2016; 48:57–63. doi: 10.1016/j.gaitpost.2016.04.016
[22]Swan L, Otani H, Loubert PV, Sheffert SM, Dunbar GL. Improving balance by performing a secondary cognitive task. British Journal of Psychology. 2004; 95(1):31–40. doi: 10.1348/000712604322779442
[23]Horak FB, Nutt JG, Nashner LM. Postural inflexibility in parkinsonian subjects. Journal of the Neurological Sciences. 1992; 111(1):46–58. doi: 10.1016/0022-510x(92)90111-w
[24]Van Emmerik REA, Van Wegen EEH. On the functional aspects of variability in postural control. Exercise and Sport Sciences Reviews . 2002; 30(4):177–83. doi: 10.1097/00003677-200210000-00007
[25]Jonsson E, Seiger Å, Hirschfeld H. One-leg stance in healthy young and elderly adults: A measure of postural steadiness. Clinical Biomechanics. 2004; 19(7):688–94. doi: 10.1016/j.clinbiomech.2004.04.002
[26]Bohannon RW. One-legged balance test times. Perceptual and Motor Skills. 1994; 78(3):801–2. doi: 10.1177/003151259407800322
[27]Briggs RC, Gossman MR, Birch R, Drews JE, Shaddeau SA. Balance performance among non institutionalized elderly women. Physical Therapy. 1989; 69(9):748–56. doi: 10.1093/ptj/69.9.748
[28]Bryant EC, Trew ME, Bruce AM, Kuisma RME, Smith AW. Gender differences in balance performance at the time of retirement. Clinical Biomechanics. 2005; 20(3):330–5. doi: 10.1016/j.clinbiomech.2004.11.006
[29]Zeynalzadeh Ghoochani B, Hosseini SA, Talebian S, Biglarian A, Zeinalzadeh A, Nazary-Moghadam S, et al. Healthy older adults balance pattern under dual task conditions: Exploring the strategy and trend. Health Promotion Perspectives. 2016; 6(4):207–12. doi: 10.15171/hpp.2016.34
[30]Clifford AM, Holder-Powell H. Postural control in healthy individuals. Clinical Biomechanics. 2010; 25(6):546–51. doi: 10.1016/j.clinbiomech.2010.03.005
Article type: Original Research Articles |
Subject:
Occupational therapy
Received: 2016/11/14 | Accepted: 2017/04/4 | Published: 2017/08/1
Received: 2016/11/14 | Accepted: 2017/04/4 | Published: 2017/08/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Iranian Rehabilitation Journal (IRJ)
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave., Tehran, Iran
Journal Tel: +9821 71732826
& +9821 22180083-92 (Ext: 2826)
& +9821 22180083-92 (Ext: 2826)
Publisher Tel:+9821 453 55 555;
+9821 453 55 000
+9821 453 55 000
E-mail: irj.uswr@gmail.com, irj@uswr.ac.ir
