
988368
Wed, May 27, 2026

Volume 15, Issue 4 (December 2017)
Iranian Rehabilitation Journal 2017, 15(4): 377-388 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Desai S, Mantha S, Phalle V. Comprehensive Needs Assessment Study and Deployment of QFD Targeted at New Wheelchair Design. Iranian Rehabilitation Journal 2017; 15 (4) :377-388
URL: http://irj.uswr.ac.ir/article-1-769-en.html
URL: http://irj.uswr.ac.ir/article-1-769-en.html


1- Department of Mechanical Engineering, Veermata Jijabai Technological Institute, Mumbai, India.
Full-Text [PDF 808 kb]
(2819 Downloads)
| Abstract (HTML) (9035 Views)
Full-Text: (3989 Views)
1. Introduction
Disability is a physical or mental condition (consequence of impairment) that restricts normal human activities [1]. Orthopedic and neurological causes are the two primary reasons of physical disabilities limiting mobility [2]. Orthopedic disabilities involve the disfigurement of the skeletal framework, which can be the consequence of sickness (e.g. arthritis) or injury or mishap (e.g. amputation). Neurological disabilities result from the incapacity to control certain parts of the body, which can be due to inborn abnormality (e.g. cerebral palsy) or due to mishap (e.g. spinal cord injury) [2].
People with disabilities in developing countries such as India tackle different social, medicinal, educational, and political difficulties [1]. Disability is a significant public health issue in India. India contributes to 17.86% of the entire world’s population. National Sample Survey Organization (NSSO) reported the population of people with disability in India as 18.5 million in 2001, which is 2.13% of the entire population of the country. The population of people with disability in India has increased by 22.4% from 2001 to 2011 [1], and large lives in rural areas with low family income. Furthermore, World Health Organization (WHO) has reported that any country has at least 10% of the population that accounts for people with disability, and among them, only 10% have access to wheelchair [3–5].
As per WHO, there are around 10 million potential wheelchair users in India, which can be validated by latest nationwide census of India [1]. There is an enormous requirement for assistive technologies (ATs) for people with disability in India; however, they are either imported (i.e., designed for developed countries) or very expensive(i.e., not suitable for people with low income). Accessibility of rehabilitation interventions and their delivery is exceptionally constrained. In many cases, use of such devices is restricted to the urban communities [2].
A wheelchair is a highest utilized assistive device used by people with different levels of disability. In most cases, the user requires aid to move a wheelchair, to use a toilet, to help in lifting from bed, and so on. Extensive use of existing wheelchairs increases caregiver dependency, risk of bedsores, risk of injury during transfer, and so on, which severely decreases quality of life, safety, and comfort of people with disability. Therefore, improving the designs of wheelchairs is highly essential in order to promote quality of life and level of participation among people with disability. Previously, wheelchair makers just focused on the manufacturing efficiency and cost of the wheelchair and rarely performed assessment of users’ needs. Investigating the needs and expectations of wheelchair users and caregivers is one of the initial moves toward providing a design alternative which will resolve various difficulties.
The primary goal in developing a new assistive product is to comprehensively assess the users’ needs. By assessing the users’ needs at the start might help to enhance and filter out the problems that create inconveniences and imperfections in the design. It is the necessary to understand the necessities of people with disabilities prior to designing rehabilitation interventions like a wheelchair. The design of wheelchair for users of a developed country might be inadequate in comparison to a developing country such as India because the users’ needs are completely different. A number of studies have been performed to understand the technological needs and desires of users of wheelchair [6–13].
No wheelchair has been intended to address the issues of users from the rural areas. Till date, no study has been performed to depict the nature of wheelchair users’ challenges from the Indian users’ perspectives. Indian ergonomic preferences, the performance objectives of wheelchair, and the wheelchair features are essential to study in order to accomplish a user-centric wheelchair design. Thus, a clear understanding of the difficulties of wheelchair users in India is highly essential in order to build a systematic, evidence-based design. The motivation behind this study was to depict the wheelchair users’ challenges from Indian users’ perspectives. Results of this study are quite useful to design a systematic, evidence-based wheelchair design that matches the Indian users’ necessities.
Quality Function Deployment (QFD) is one of the methodical strategies that are intended at fulfilling the users’ needs with better integration of multidisciplinary teams [14, 15]. Numerous researchers agree that QFD enhances the competitiveness of products thereby reducing the period of product development [16, 17]. Nowadays, QFD is utilized effectively by manufacturers of electronics, appliances, automobiles, and construction equipments (e.g. IBM and General Motors) [18, 19]. Thus, a comprehensive, user-centered, QFD-based approach is essential to address various issues encountered by Indian wheelchair users in order to enhance quality of life, comfort, and safety. The primary goal of this study was to explore the needs of wheelchair users with needs assessment study and to recognize design considerations for a new design.
Needs and expectation assessment is executed early in the study to understand difficulties confronted by Indian wheelchair users. The secondary goal of this study was to apply QFD-based method to understand and explore users’ needs
Disability is a physical or mental condition (consequence of impairment) that restricts normal human activities [1]. Orthopedic and neurological causes are the two primary reasons of physical disabilities limiting mobility [2]. Orthopedic disabilities involve the disfigurement of the skeletal framework, which can be the consequence of sickness (e.g. arthritis) or injury or mishap (e.g. amputation). Neurological disabilities result from the incapacity to control certain parts of the body, which can be due to inborn abnormality (e.g. cerebral palsy) or due to mishap (e.g. spinal cord injury) [2].
People with disabilities in developing countries such as India tackle different social, medicinal, educational, and political difficulties [1]. Disability is a significant public health issue in India. India contributes to 17.86% of the entire world’s population. National Sample Survey Organization (NSSO) reported the population of people with disability in India as 18.5 million in 2001, which is 2.13% of the entire population of the country. The population of people with disability in India has increased by 22.4% from 2001 to 2011 [1], and large lives in rural areas with low family income. Furthermore, World Health Organization (WHO) has reported that any country has at least 10% of the population that accounts for people with disability, and among them, only 10% have access to wheelchair [3–5].
As per WHO, there are around 10 million potential wheelchair users in India, which can be validated by latest nationwide census of India [1]. There is an enormous requirement for assistive technologies (ATs) for people with disability in India; however, they are either imported (i.e., designed for developed countries) or very expensive(i.e., not suitable for people with low income). Accessibility of rehabilitation interventions and their delivery is exceptionally constrained. In many cases, use of such devices is restricted to the urban communities [2].
A wheelchair is a highest utilized assistive device used by people with different levels of disability. In most cases, the user requires aid to move a wheelchair, to use a toilet, to help in lifting from bed, and so on. Extensive use of existing wheelchairs increases caregiver dependency, risk of bedsores, risk of injury during transfer, and so on, which severely decreases quality of life, safety, and comfort of people with disability. Therefore, improving the designs of wheelchairs is highly essential in order to promote quality of life and level of participation among people with disability. Previously, wheelchair makers just focused on the manufacturing efficiency and cost of the wheelchair and rarely performed assessment of users’ needs. Investigating the needs and expectations of wheelchair users and caregivers is one of the initial moves toward providing a design alternative which will resolve various difficulties.
The primary goal in developing a new assistive product is to comprehensively assess the users’ needs. By assessing the users’ needs at the start might help to enhance and filter out the problems that create inconveniences and imperfections in the design. It is the necessary to understand the necessities of people with disabilities prior to designing rehabilitation interventions like a wheelchair. The design of wheelchair for users of a developed country might be inadequate in comparison to a developing country such as India because the users’ needs are completely different. A number of studies have been performed to understand the technological needs and desires of users of wheelchair [6–13].
No wheelchair has been intended to address the issues of users from the rural areas. Till date, no study has been performed to depict the nature of wheelchair users’ challenges from the Indian users’ perspectives. Indian ergonomic preferences, the performance objectives of wheelchair, and the wheelchair features are essential to study in order to accomplish a user-centric wheelchair design. Thus, a clear understanding of the difficulties of wheelchair users in India is highly essential in order to build a systematic, evidence-based design. The motivation behind this study was to depict the wheelchair users’ challenges from Indian users’ perspectives. Results of this study are quite useful to design a systematic, evidence-based wheelchair design that matches the Indian users’ necessities.
Quality Function Deployment (QFD) is one of the methodical strategies that are intended at fulfilling the users’ needs with better integration of multidisciplinary teams [14, 15]. Numerous researchers agree that QFD enhances the competitiveness of products thereby reducing the period of product development [16, 17]. Nowadays, QFD is utilized effectively by manufacturers of electronics, appliances, automobiles, and construction equipments (e.g. IBM and General Motors) [18, 19]. Thus, a comprehensive, user-centered, QFD-based approach is essential to address various issues encountered by Indian wheelchair users in order to enhance quality of life, comfort, and safety. The primary goal of this study was to explore the needs of wheelchair users with needs assessment study and to recognize design considerations for a new design.
Needs and expectation assessment is executed early in the study to understand difficulties confronted by Indian wheelchair users. The secondary goal of this study was to apply QFD-based method to understand and explore users’ needs

to identify design parameters for higher user satisfaction. The results of this study will contribute to the development of a wheelchair and improvement in the quality of life of people with disability.
2. Methods
Preliminary analysis
A preliminary analysis was conducted through direct surveillance of wheelchairs and deliberations with the medical professionals from various urban and rural settings. It was conducted to understand the reactions of users toward their existing wheelchair and the expectations of the users toward the desired wheelchair. Results of the preliminary analysis were used as a guideline for designing the research questionnaire and interview guide. It was used to get an underlying picture of users’ perspective.
Participants
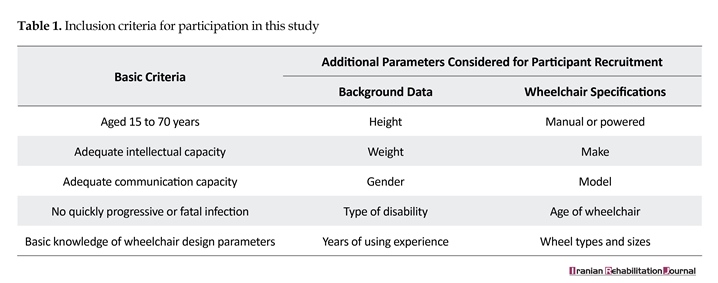
Participants who were in the age group of 15–70 years with adequate intellectual and communicational capacity, not having quickly progressive or fatal infection, and with basic knowledge of wheelchair design parameters participated in this study. Additional inclusion parameters for the study were users’ background data and wheelchair specifications. Table 1 shows the inclusion criteria of participants.
Medical professionals from various healthcare facilities informed potential participants about the study. To obtain comprehensive data as possible, the sample was chosen to provide variation according to the diagnosis, duration of wheelchair use, age, marital status, educational level, type of wheelchair, geographical location, and sex. To accommodate regional variation of India, participants were selected from metropolitan cities, urban areas, and small villages.
2. Methods
Preliminary analysis
A preliminary analysis was conducted through direct surveillance of wheelchairs and deliberations with the medical professionals from various urban and rural settings. It was conducted to understand the reactions of users toward their existing wheelchair and the expectations of the users toward the desired wheelchair. Results of the preliminary analysis were used as a guideline for designing the research questionnaire and interview guide. It was used to get an underlying picture of users’ perspective.
Participants
Participants who were in the age group of 15–70 years with adequate intellectual and communicational capacity, not having quickly progressive or fatal infection, and with basic knowledge of wheelchair design parameters participated in this study. Additional inclusion parameters for the study were users’ background data and wheelchair specifications. Table 1 shows the inclusion criteria of participants.
Medical professionals from various healthcare facilities informed potential participants about the study. To obtain comprehensive data as possible, the sample was chosen to provide variation according to the diagnosis, duration of wheelchair use, age, marital status, educational level, type of wheelchair, geographical location, and sex. To accommodate regional variation of India, participants were selected from metropolitan cities, urban areas, and small villages.

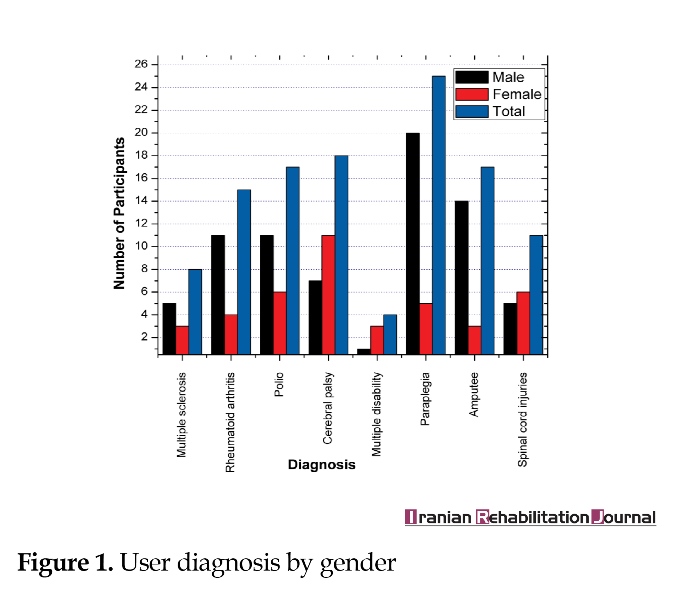
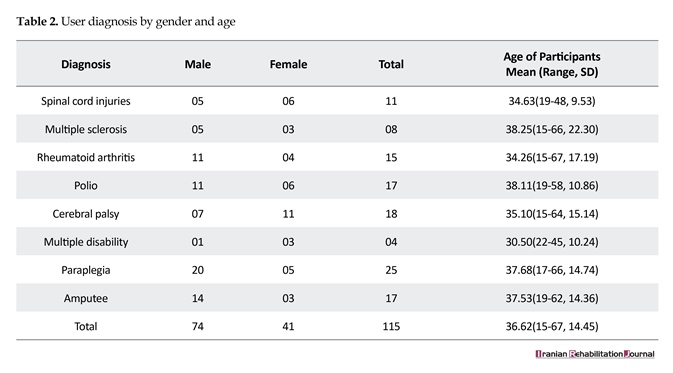
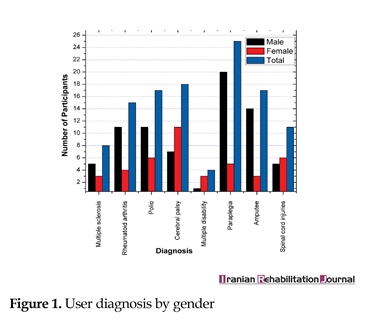
Altogether, participants (n=115) in the age range of 15–70 (mean=36.62) years were chosen for participation. User diagnosis by age and gender is given in Table 2 and Figure 1.
Data collection
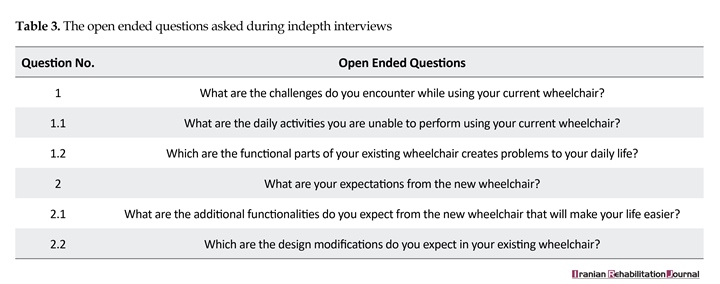
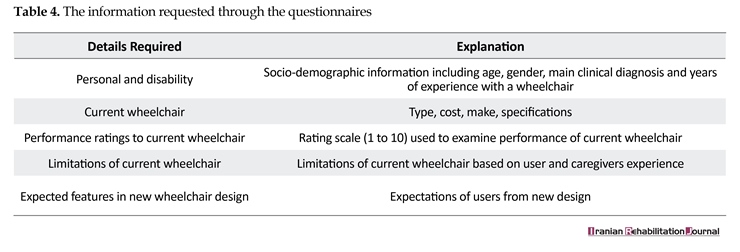
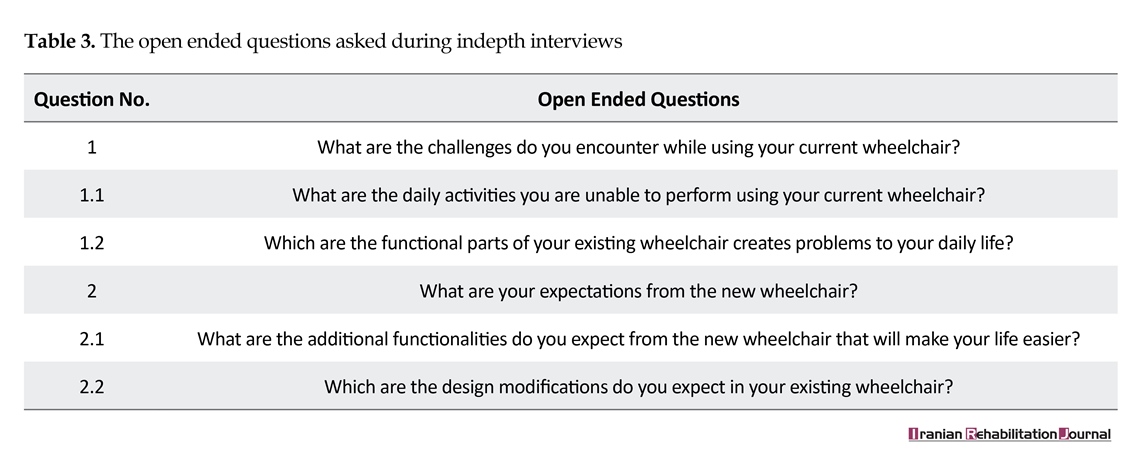
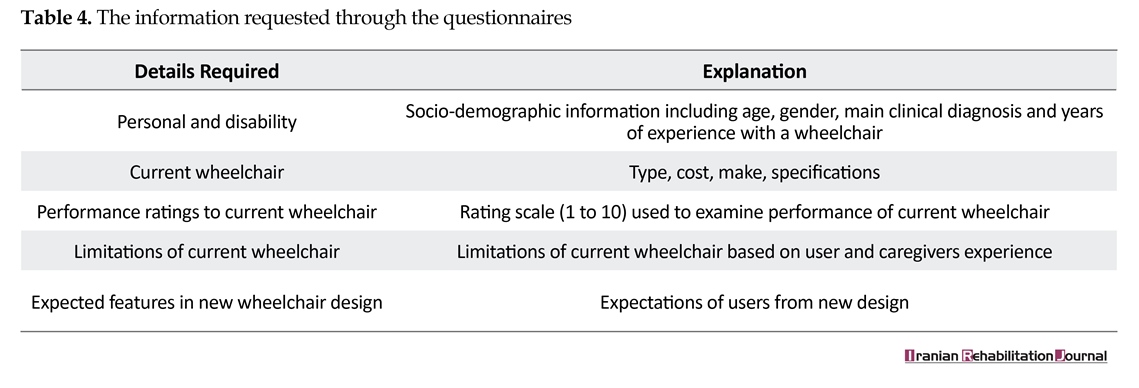
Individual in-depth interview was conducted with wheelchair users and their caregivers. The interview guide was customized as the interviews progressed to collect data in relation to emerging themes. Interview guide (including 12 questions) were used for data collection. It consisted of two open-ended questions (Table 3) with explicit investigations concerning experiences and expectations of wheelchair users. Interviews were conducted in presence of medical professionals skilled in the area of rehabilitation science. Furthermore, structured questionnaire comprising 22 questions was used to collect data. Socio-demographic and user experience information was also collected using questionnaire. Participants were asked about their past and current wheelchair in order to record positive and challenging points. A total of 225 questionnaires were distributed. The information as per the questionnaire is detailed in Table 4.
Data analysis
The framework method provides a systematic model to support thematic analysis [20, 21]. It is used to recognize themes related to difficulties faced by users and understanding their perspectives of a desired wheelchair. The investigation of needs and expectations of wheelchair user yielded both quantitative and qualitative data. All interviews were recorded and checked against notes taken during each interview to confirm the accuracy of the collected content. Framework approach was used to analyze the collected data [20, 21].
Qualitative data were analyzed by developing categories to determine data tendency, data resemblance, and emerging
Data collection
Individual in-depth interview was conducted with wheelchair users and their caregivers. The interview guide was customized as the interviews progressed to collect data in relation to emerging themes. Interview guide (including 12 questions) were used for data collection. It consisted of two open-ended questions (Table 3) with explicit investigations concerning experiences and expectations of wheelchair users. Interviews were conducted in presence of medical professionals skilled in the area of rehabilitation science. Furthermore, structured questionnaire comprising 22 questions was used to collect data. Socio-demographic and user experience information was also collected using questionnaire. Participants were asked about their past and current wheelchair in order to record positive and challenging points. A total of 225 questionnaires were distributed. The information as per the questionnaire is detailed in Table 4.
Data analysis
The framework method provides a systematic model to support thematic analysis [20, 21]. It is used to recognize themes related to difficulties faced by users and understanding their perspectives of a desired wheelchair. The investigation of needs and expectations of wheelchair user yielded both quantitative and qualitative data. All interviews were recorded and checked against notes taken during each interview to confirm the accuracy of the collected content. Framework approach was used to analyze the collected data [20, 21].
Qualitative data were analyzed by developing categories to determine data tendency, data resemblance, and emerging
themes. At first, the raw information was examined to recognize relevant expressions and sentences. These were selected and further scrutinized to recognize evolving themes related to the topic. The data were composed with respect to developing themes and re-examined to further refine the growing themes. Data were then set into figures and charts by compressing individual responses and evolving themes. The investigation then concentrated on seeking patterns of themes and the data poised into the classifications [20, 21].
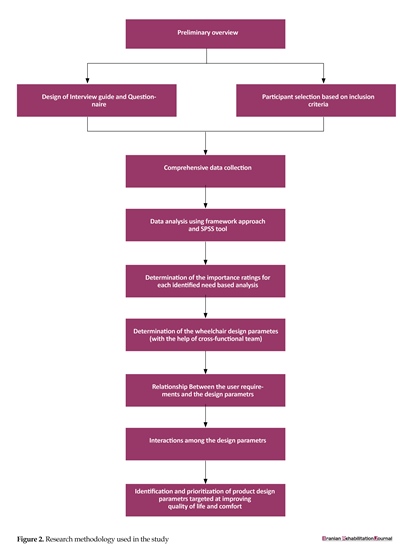
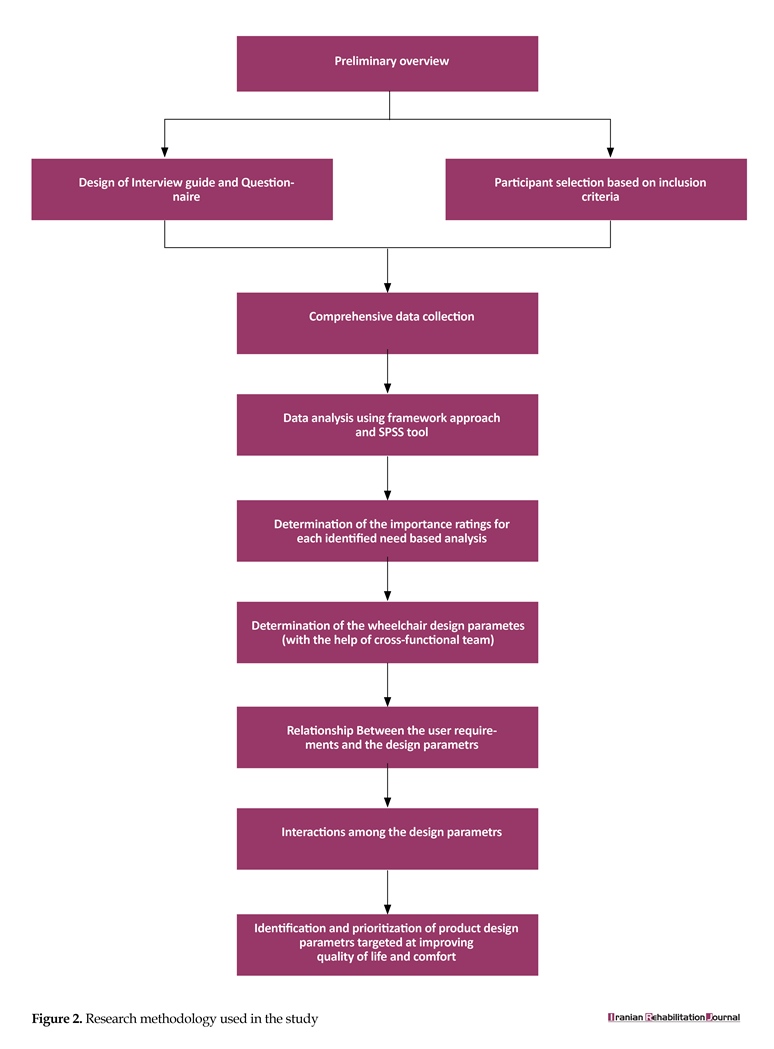
Next, investigation of the categories was performed. An interpretative analysis was used to provide explanations for the outcome. Furthermore, quantitative data was managed using excel spread sheet and analyzed using SPSS tool. Then, the analyzed information was processed using QFD design by means of House of Quality (HoQ) matrix. Using HoQ matrix, user requirements were converted in terms of design requirements. QFD investigation was supported by various matrices and tables. It was implemented to convert user requirements into the product design parameters in order to improve quality of life of people with disability [22–24]. The research methodology employed in this study is shown in Figure 2.
Ethical approval
Full consent was obtained from each subject prior to the study. Each subject was informed that participation was voluntary and confidential. Adequate level of confidentiality of the personal data of the participants was ensured. Any type of misleading information and representation of primary data findings in a biased way was avoided. Research participants did not subject to harm in any ways whatsoever. All subjects were informed that the lack of participation in the study would not impact on their relationships with the staff.
3. Results
Participants
A total of 115 individuals participated in this study (74 male, 41 females) with a variety of diagnoses comprising spinal cord injuries (n=11), multiple sclerosis (n=08), rheumatoid arthritis (n=15), polio (n=17), cerebral palsy (n=18), multiple disability (n=04), paraplegia (n=25), and amputee (n=17). Forty-six participants were between the ages of 15 and 30 years, 50 participants between 31 and 50 years,
Next, investigation of the categories was performed. An interpretative analysis was used to provide explanations for the outcome. Furthermore, quantitative data was managed using excel spread sheet and analyzed using SPSS tool. Then, the analyzed information was processed using QFD design by means of House of Quality (HoQ) matrix. Using HoQ matrix, user requirements were converted in terms of design requirements. QFD investigation was supported by various matrices and tables. It was implemented to convert user requirements into the product design parameters in order to improve quality of life of people with disability [22–24]. The research methodology employed in this study is shown in Figure 2.
Ethical approval
Full consent was obtained from each subject prior to the study. Each subject was informed that participation was voluntary and confidential. Adequate level of confidentiality of the personal data of the participants was ensured. Any type of misleading information and representation of primary data findings in a biased way was avoided. Research participants did not subject to harm in any ways whatsoever. All subjects were informed that the lack of participation in the study would not impact on their relationships with the staff.
3. Results
Participants
A total of 115 individuals participated in this study (74 male, 41 females) with a variety of diagnoses comprising spinal cord injuries (n=11), multiple sclerosis (n=08), rheumatoid arthritis (n=15), polio (n=17), cerebral palsy (n=18), multiple disability (n=04), paraplegia (n=25), and amputee (n=17). Forty-six participants were between the ages of 15 and 30 years, 50 participants between 31 and 50 years,
and 19 participants between 51 and 67 years. Thirty-nine participants had experience of using wheelchair between 0 and 5 years, 51 had between 5 and 10 years, and 25 had ≥10 years. All the interviews are conducted in Hindi and Marathi language.
Key evolving themes
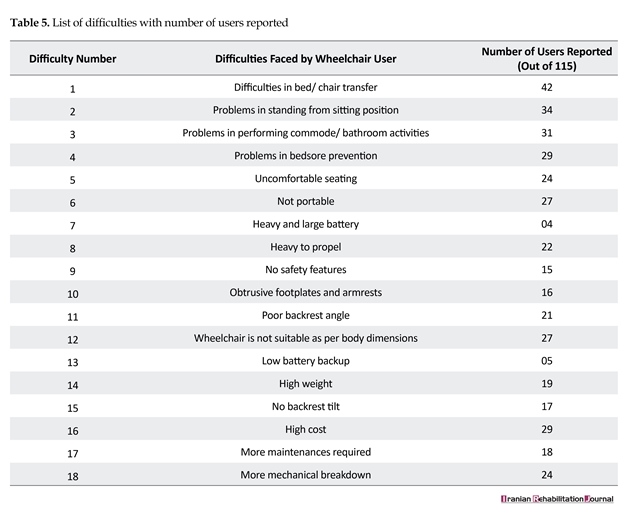
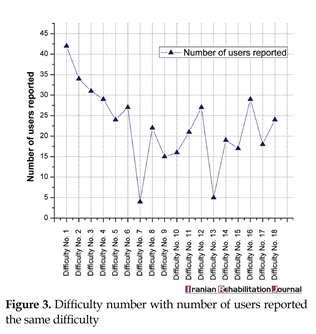
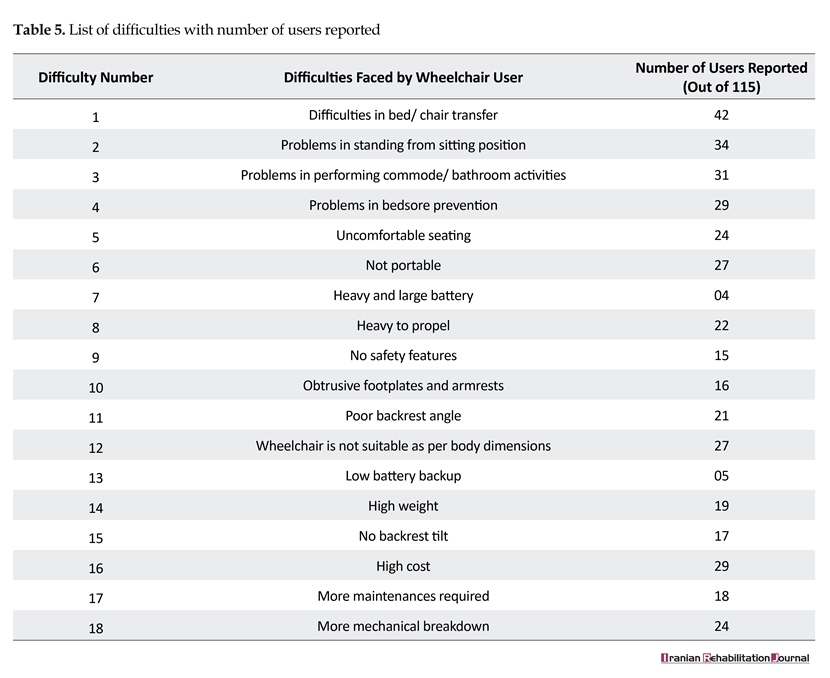
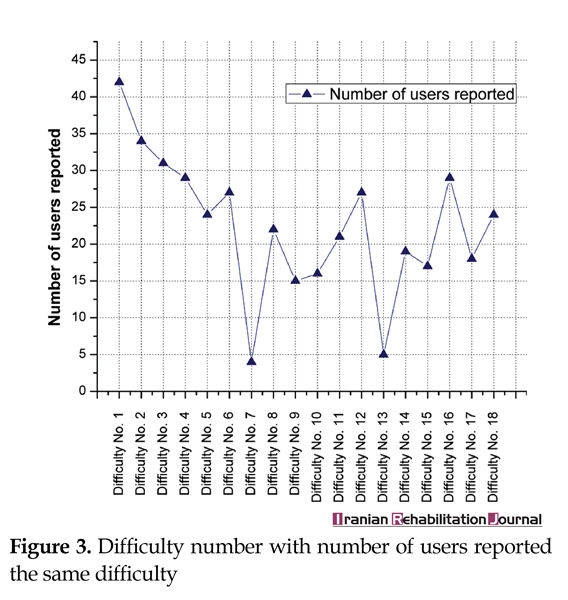
The four key themes that evolved from framework thematic analysis were the following: Difficulties in transfer from the wheelchair to and from the bed; Problems faced while standing from sitting position; Difficulties in using the commode/ bathroom; and Risk of bedsores due to extensive use of the wheelchair. List of difficulties with number of users reported is detailed in Table 5 and Figure 3.
Difficulties in transfer from the wheelchair to and from the bed
While using existing wheelchair, people with disability were facing the problem of transfer from the wheelchair to and from the bed. In most of the cases, transfer support is provided by the caregivers, which increases the problem of caregiver dependency. In response to the questions posed related to transfer, 42 (36.52%) users reported difficulties in bed/chair transfer. Thirty-three (28.69%) users provided 10/10 rating to assistance for wheelchair to bed transfer as desired wheelchair feature which received 9.15/10 overall rating.
A number of problems have been reported that are associated with bed/chair transfer. Seventy-five (65.21%) users reported an increase in the lower back injuries of their caregivers. Forty-six (40.00%) users reported injuries due to the failure of the caregiver to properly apply strength during transfer process. Forty-nine (42.60%) users reported inconvenience to get into/out of bed without the assistance of a caregiver. Thirty-nine (33.91%) users reported transfer is a tiring and tedious process for their caregivers.
Problems faced while standing from sitting position
The capability to stand from sitting position is essential life quality. Many people with disability are confined to wheelchairs due to the absence of standing capability. Thirty-four (29.56%) users experienced difficulties in standing from the sitting position. Thirty-nine (33.91%) users provided 10.10 rating to assistance to sit to stand transfer as expected wheelchair feature which received 8.9/10 overall ratings. A number of difficulties have been reported by users related to the lack of ability to stand from a sitting position.
Increase in leg problems as unable to stand (59 (51.30%) users reported); Excretion system failure as unable to stand (51 (44.34%) users reported); Pain in hip joint as unable to stand (45 (39.13%) users reported); Low level of the eyesight creates psychological stress (29 (25.11%) users reported)
Difficulties in using the commode/ bathroom
Taking help from a caregiver for using toilet/ bathroom decreases their quality of life severely. In response to the questions posed, 31 (26.95%) users reported problems in performing commode/bathroom activities. Thirty (26.08%) users provided 10/10 rating to assistance for using commode as expected wheelchair feature which received 8.61/10 overall ratings.
Forty-five (39.13%) users reported problems with accessibility of existing toilets at public places and experienced lack of a good toilet environment. While using the toilet, postural control of a person with disability is necessary. Sixty-four (55.65%) people with disability reported inconvenience while using toilet because of lack of posture control.
Risk of bedsores due to extensive use of the wheelchair
Bedsores are regions of broken skin that can produce when individuals with long-term disabilities are confined to bed or wheelchair for long periods of time. Twenty-nine (25%) users reported risk of bedsores due to extensive use of existing wheelchair. Twenty-five (22%) users provided 10/10 rating to assistance for prevention of risk of bedsores as expected wheelchair feature which received 8.12/10 overall rating. A number of problems have been reported that are associated with the risk of bedsores due to extensive use of current wheelchair. Lack of frequent re-positioning arrangement (34 (29.56%) users reported); Caregiver dependency to keep skin and clothes dry and clean (45 (39.13%) users reported); Improper wheelchair fit (25 (21.17%) users reported).
QFD design
Users importance ratings
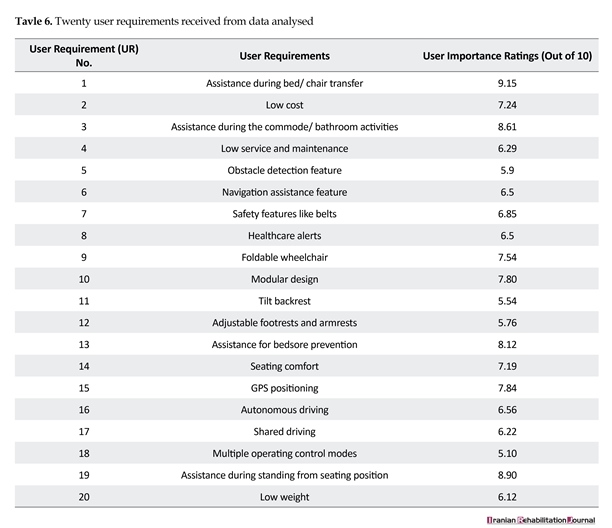
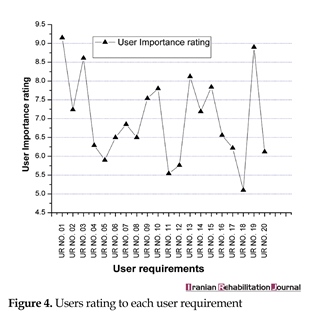
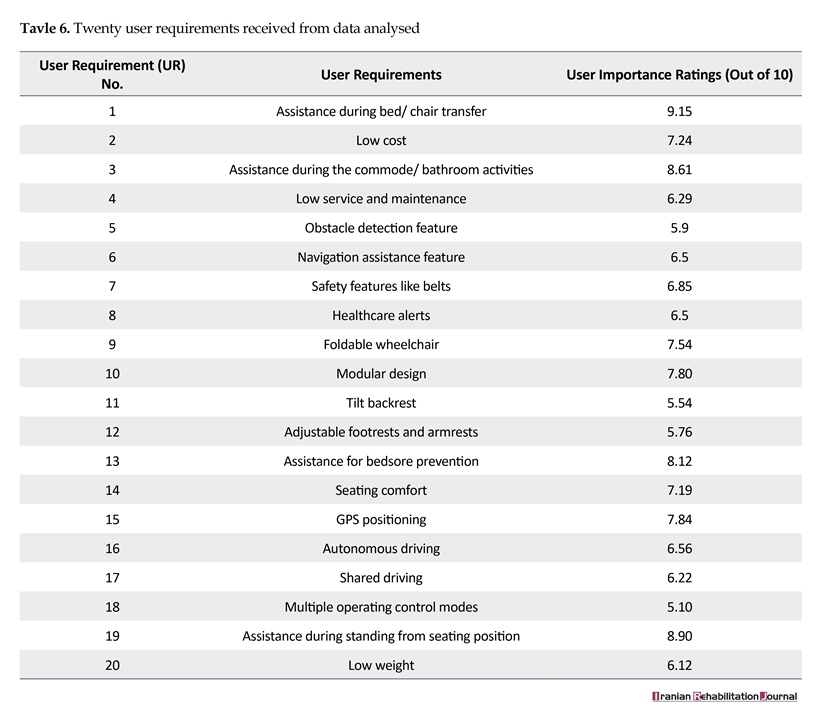
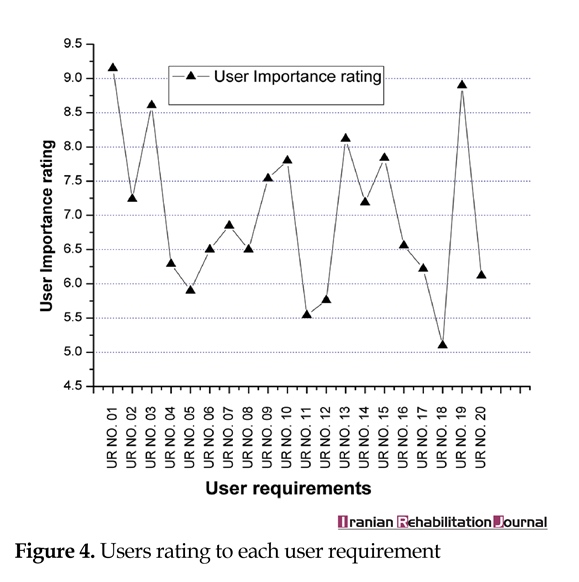
Identification of user requirements was performed during needs assessment step. The answers were weighted to get the measured value. This information was utilized directly in the QFD analysis to translate the user requirements into design parameters expressed in the technical terms. Table 6 reports the user requirements and user importance ratings.
Selection of the design parameters for mapping user needs
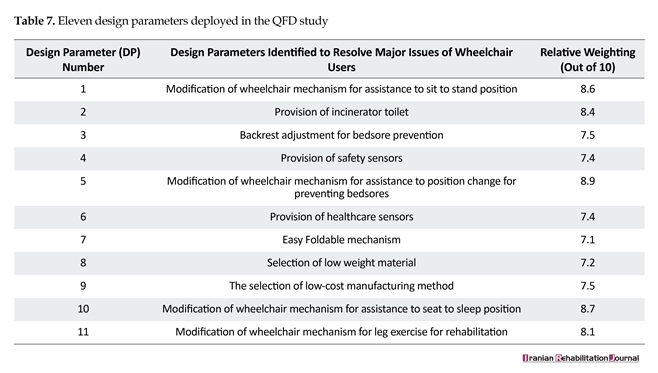
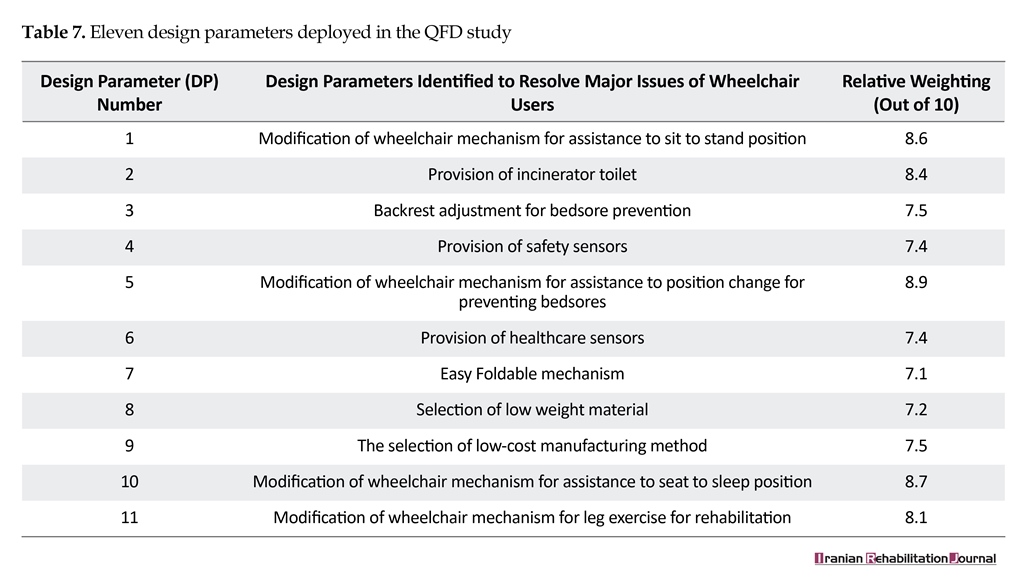
Design parameters were used to symbolize the voice of designers. The design parameters were determined by deliberation with specialists in the field of wheelchair design. However, the medical parameters related to the design were obtained through consultation with medical professionals. Table 7 presents the design parameters identified for study.
Correlations between user requirements and the design parameters
Selection of correlations among the user requirements and design parameters was performed through deliberations with the engineering experts and the medical professionals. The correlation values were assigned to each value based on the strength of relationship. The correlation values were represented by several categories such as strong (•=5), moderate (o=3), weak (Δ=1), and no relationship (no symbol).
Relationship among the design parameters
The relationship among the design parameters reflects design clash and corresponding characteristics [24-26]. It is also useful to see how a design parameter affects the other design parameter. There are five design parameter relationships used in present HoQ matrix. These relationships were
Key evolving themes
The four key themes that evolved from framework thematic analysis were the following: Difficulties in transfer from the wheelchair to and from the bed; Problems faced while standing from sitting position; Difficulties in using the commode/ bathroom; and Risk of bedsores due to extensive use of the wheelchair. List of difficulties with number of users reported is detailed in Table 5 and Figure 3.
Difficulties in transfer from the wheelchair to and from the bed
While using existing wheelchair, people with disability were facing the problem of transfer from the wheelchair to and from the bed. In most of the cases, transfer support is provided by the caregivers, which increases the problem of caregiver dependency. In response to the questions posed related to transfer, 42 (36.52%) users reported difficulties in bed/chair transfer. Thirty-three (28.69%) users provided 10/10 rating to assistance for wheelchair to bed transfer as desired wheelchair feature which received 9.15/10 overall rating.
A number of problems have been reported that are associated with bed/chair transfer. Seventy-five (65.21%) users reported an increase in the lower back injuries of their caregivers. Forty-six (40.00%) users reported injuries due to the failure of the caregiver to properly apply strength during transfer process. Forty-nine (42.60%) users reported inconvenience to get into/out of bed without the assistance of a caregiver. Thirty-nine (33.91%) users reported transfer is a tiring and tedious process for their caregivers.
Problems faced while standing from sitting position
The capability to stand from sitting position is essential life quality. Many people with disability are confined to wheelchairs due to the absence of standing capability. Thirty-four (29.56%) users experienced difficulties in standing from the sitting position. Thirty-nine (33.91%) users provided 10.10 rating to assistance to sit to stand transfer as expected wheelchair feature which received 8.9/10 overall ratings. A number of difficulties have been reported by users related to the lack of ability to stand from a sitting position.
Increase in leg problems as unable to stand (59 (51.30%) users reported); Excretion system failure as unable to stand (51 (44.34%) users reported); Pain in hip joint as unable to stand (45 (39.13%) users reported); Low level of the eyesight creates psychological stress (29 (25.11%) users reported)
Difficulties in using the commode/ bathroom
Taking help from a caregiver for using toilet/ bathroom decreases their quality of life severely. In response to the questions posed, 31 (26.95%) users reported problems in performing commode/bathroom activities. Thirty (26.08%) users provided 10/10 rating to assistance for using commode as expected wheelchair feature which received 8.61/10 overall ratings.
Forty-five (39.13%) users reported problems with accessibility of existing toilets at public places and experienced lack of a good toilet environment. While using the toilet, postural control of a person with disability is necessary. Sixty-four (55.65%) people with disability reported inconvenience while using toilet because of lack of posture control.
Risk of bedsores due to extensive use of the wheelchair
Bedsores are regions of broken skin that can produce when individuals with long-term disabilities are confined to bed or wheelchair for long periods of time. Twenty-nine (25%) users reported risk of bedsores due to extensive use of existing wheelchair. Twenty-five (22%) users provided 10/10 rating to assistance for prevention of risk of bedsores as expected wheelchair feature which received 8.12/10 overall rating. A number of problems have been reported that are associated with the risk of bedsores due to extensive use of current wheelchair. Lack of frequent re-positioning arrangement (34 (29.56%) users reported); Caregiver dependency to keep skin and clothes dry and clean (45 (39.13%) users reported); Improper wheelchair fit (25 (21.17%) users reported).
QFD design
Users importance ratings
Identification of user requirements was performed during needs assessment step. The answers were weighted to get the measured value. This information was utilized directly in the QFD analysis to translate the user requirements into design parameters expressed in the technical terms. Table 6 reports the user requirements and user importance ratings.
Selection of the design parameters for mapping user needs
Design parameters were used to symbolize the voice of designers. The design parameters were determined by deliberation with specialists in the field of wheelchair design. However, the medical parameters related to the design were obtained through consultation with medical professionals. Table 7 presents the design parameters identified for study.
Correlations between user requirements and the design parameters
Selection of correlations among the user requirements and design parameters was performed through deliberations with the engineering experts and the medical professionals. The correlation values were assigned to each value based on the strength of relationship. The correlation values were represented by several categories such as strong (•=5), moderate (o=3), weak (Δ=1), and no relationship (no symbol).
Relationship among the design parameters
The relationship among the design parameters reflects design clash and corresponding characteristics [24-26]. It is also useful to see how a design parameter affects the other design parameter. There are five design parameter relationships used in present HoQ matrix. These relationships were
assigned by several categories such as a positive relationship (**), moderate positive relationship (+), no relationship (no symbol), moderate negative relationship (X), and strong negative relationship (XX).
Priority estimation of the design parameters
The values of absolute technical importance and relative technical importance were assigned to each design parameter. Technical importance of each design parameter was estimated by adding the results of multiplication of the user importance ratings with the corresponding correlation value [24]. For each design parameter, the absolute technical importance can be estimated using the below equation [23, 25].
Where AIj is the absolute technical importance of design parameter DPj, where j=1,…,n; Xi is the importance rating of user requirement URi, i=1,…, m; and Yij is the value of correlation that describes the relationship between DPj and URj [26].
The relative technical importance RIj can be estimated as the below equation [23, 25].
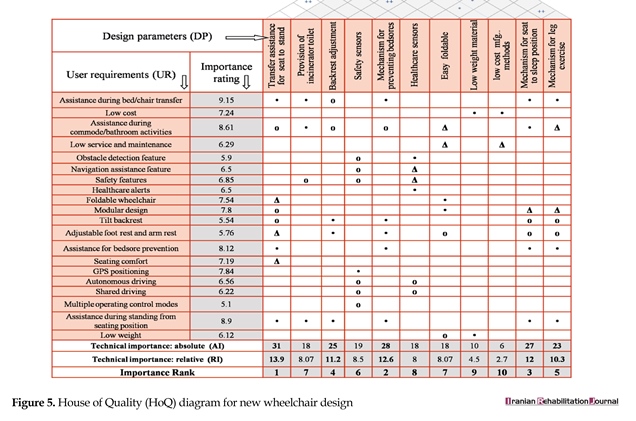
Figure 5 shows the HoQ matrix that comprises user requirements received from needs assessment, user importance ratings, correlations among the user requirements and the design parameters, relations among the design parameters, and the absolute and relative technical importance of each design parameter.
4. Discussion
Improvements in existing wheelchair design might play a decisive role in promoting quality of life and level of participation among people with disability. Most of the people with disability from India confront major problems such as caregiver dependency, risk of bedsores, risk of injury during transfer, and so on. By considering needs of the potential users at the beginning of design process, the design might get better and filter out the problems that are users confront. In the past, wheelchairs were designed by only aiming at maximizing the manufacturing efficiency and lowering
Priority estimation of the design parameters
The values of absolute technical importance and relative technical importance were assigned to each design parameter. Technical importance of each design parameter was estimated by adding the results of multiplication of the user importance ratings with the corresponding correlation value [24]. For each design parameter, the absolute technical importance can be estimated using the below equation [23, 25].
Where AIj is the absolute technical importance of design parameter DPj, where j=1,…,n; Xi is the importance rating of user requirement URi, i=1,…, m; and Yij is the value of correlation that describes the relationship between DPj and URj [26].
The relative technical importance RIj can be estimated as the below equation [23, 25].
Figure 5 shows the HoQ matrix that comprises user requirements received from needs assessment, user importance ratings, correlations among the user requirements and the design parameters, relations among the design parameters, and the absolute and relative technical importance of each design parameter.
4. Discussion
Improvements in existing wheelchair design might play a decisive role in promoting quality of life and level of participation among people with disability. Most of the people with disability from India confront major problems such as caregiver dependency, risk of bedsores, risk of injury during transfer, and so on. By considering needs of the potential users at the beginning of design process, the design might get better and filter out the problems that are users confront. In the past, wheelchairs were designed by only aiming at maximizing the manufacturing efficiency and lowering

cost, thereby effectively keeping potential users as passive part of the system. Thus, needs assessment of potential wheelchair users was required to provide design solution aiming at improvement in the quality of life.
The assessment of needs and expectations of Indian wheelchair users resulted in both quantitative and qualitative data. Framework approach was applied to the qualitative data which revealed that most of the users are uncomfortable with bed to and from chair transfer, standing from sitting position, using commode/bathroom, generation of bedsores due to extensive use of the wheelchair. Four key themes emerged: 1. Difficulties in transfer from wheelchair to and from bed; 2. Problems to stand from sitting position; 3. Problems in using commode; and 4. Risk of bedsores due to extensive use of wheelchair. Furthermore, QFD analysis revealed that out of 11 design parameters recommended by cross-functional team based on needs assessment study the following parameters received the highest technical importance: 1. Seat to stand transfer feature (13.90%); 2. The bedsore prevention feature (12.60%); 3. Seat to sleep transfer feature (12.00%); and 4. Adjustable backrest feature with multi-posture adjustment feature (11.20%).
Figure 5 depicts the association of 20 user requirements and 11design parameters with their importance in terms of absolute technical importance and relative technical importance. Every design parameter has minimum one correlation with the user requirements, whereas every user requirement has two or more correlations with the design parameters. No vacant user requirement rows or design parameter columns were found in the matrix; hence, no inappropriate or unnecessary parameters existed. Each user requirement was responded by at least two design parameters.
5. Conclusion
This study presented the perspective of Indian wheelchair users through comprehensive needs assessment study. Second part of this paper reported primary wheelchair design parameters to improve the quality of life of people with disability and technological importance of each design parameter in order to prioritize them by aiming at an evidence-based design solution. It can be concluded that the users’ requirements reported by the Indian wheelchair users can be resolved by considering the high ranked design parameters suggested in this study. The design parameters with higher absolute and relative technical importance might be chosen to design new wheelchairs which will reflect the satisfaction of the wheelchair users. The design of wheelchair for users’ of a developed country might be inadequate in comparison to a developing country because the users’ needs are different. Hence, wheelchairs for Indian people with disability should be designed based on the needs assessment study. Thus, the results of this study can contribute to enhancing the existing wheelchair designs aimed at improving quality of life of people with disability.
Acknowledgements
The authors acknowledge all people who helped during conducting the research. We express our thanks to the subjects who volunteered to take part in this study. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for profit sectors.
Conflict of Interest
The authors declared no conflicts of interest.
References
[1]Office of the Registrar General & Census Commissioner. C-20 SC; Disabled population by type of disability, age and sex for scheduled castes (Census of India 2001). New Delhi: Office of the Registrar General & Census Commissioner; 2001.
[2]Lakhan R, Mario A, Qureshi FN, Hall ML. Early intervention services to children with developmental delay in resource poor settings in India. Nepal Journal of Medical Sciences. 2013; 2(2):149-55. doi: 10.3126/njms.v2i2.8966
[3]World Health Organization. World Report on Disability. Geneva: World Health Organization; 2011.
[4]Kumar SG, Roy G, Kar SS. Disability and rehabilitation services in India: Issues and challenges. Journal of Family Medicine and Primary Care. 2012; 1(1):69. doi: 10.4103/2249-4863.94458
[5]Pearlman J. Review session: Review of literature on wheelchairs for developing countries & Review of wheelchair provision in developing countries. Paper presented at A Consensus Conference on Wheelchairs for Developing Countries. 6-11 November 2006, Bengaluru, India.
[6]Lindle RS, Metter EJ, Lynch NA, Fleg JL, Fozard JL, Tobin J, et al. Age and gender comparisons of muscle strength in 654 women and men aged 20–93 year. Journal of Applied Physiology. 1997; 83(5):1581-7. PMID: 9375323
[7]Reid DT, Hebert D, Rudman D. Occupational performance in older stroke wheelchair users living at home. Occupational Therapy International. 2001; 8(4):273-86. doi: 10.1002/oti.151
[8]Belcher MJ, Frank AO. Survey of the use of transport by recipients of a regional Electric Indoor/Outdoor Powered (EPIOC) wheelchair service. Disability and Rehabilitation. 2004; 26(10):563-75. doi: 10.1080/09638280410001684055
[9]Edwards K, Mccluskey A. A survey of adult power wheelchair and scooter users. Disability and Rehabilitation: Assistive Technology. 2010; 5(6):411-9. doi: 10.3109/17483101003793412
[10]Evans S, Frank AO, Neophytou C, De Souza L. Older adults' use of, and satisfaction with, electric powered indoor/outdoor wheelchairs. Age and Ageing. 2007; 36(4):431-5. doi: 10.1093/ageing/afm034
[11]Pettersson C, Iwarsson S, Brandt Å, Norin L, Månsson Lexell E. Men’s and women’s perspectives on using a powered mobility device: Benefits and societal challenges. Scandinavian Journal of Occupational Therapy. 2014; 21(6):438-46. doi: 10.3109/11038128.2014.905634
[12]Mortenson WB, Hammell KW, Luts A, Soles C, Miller WC. The power of power wheelchairs: Mobility choices of community-dwelling, older adults. Scandinavian Journal of Occupational Therapy. 2015; 22(5):394-401. doi: 10.3109/11038128.2015.1049289
[13]Frank AO, De Souza LH, Frank JL, Neophytou C. The pain experiences of powered wheelchair users. Disability and Rehabilitation. 2012; 34(9):770-8. doi: 10.3109/09638288.2011.619620
[14]Wilkinson P. The changing role of physical testing in vehicle development programmes. Journal of Terramechanics. 2007; 44(1):15-22. doi: 10.1016/j.jterra.2006.01.004
[15]Marsot J. QFD: A methodological tool for integration of ergonomics at the design stage. Applied Ergonomics. 2005; 36(2):185-92. doi: 10.1016/j.apergo.2004.10.005
[16]Giesbrecht E. Application of the Human Activity Assistive Technology model for occupational therapy research. Australian Occupational Therapy Journal. 2013; 60(4):230-40. doi: 10.1111/1440-1630.12054
[17]Chen LH, Weng MC. An evaluation approach to engineering design in QFD processes using fuzzy goal programming models. European Journal of Operational Research. 2006; 172(1):230-48. doi: 10.1016/j.ejor.2004.10.004
[18]Park T, Kim KJ. Determination of an optimal set of design requirements using house of quality. Journal of Operations Management. 1998; 16(5):569-81. doi: 10.1016/s0272-6963(97)00029-6
[19]Vairaktarakis GL. Optimization tools for design and marketing of new/ improved products using the house of quality. Journal of Operations Management. 1999; 17(6):645-63. doi: 10.1016/s0272-6963(99)00020-0
[20]Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi disciplinary health research. BMC Medical Research Methodology. 2013; 13(1):117. doi: 10.1186/1471-2288-13-117
[21]Baccarini D. The logical framework method for defining project success. Project Management Journal. 1999; 30(4):25-32.
[22]Zadry HR, Rahmayanti D, Susanti L, Fatrias D. Identification of design requirements for ergonomic long spinal board using Quality Function Deployment (QFD). Procedia Manufacturing. 2015; 3:4673-80. doi: 10.1016/j.promfg.2015.07.559
[23]Tsai KH, Yeh CY, Lo HC, Li CT, Cheng CP, Chang GL. Application of quality function deployment in design of mobile assistive devices. Journal of Medical and Biological Engineering. 2008; 28(2):87-93.
[24]Tseng KC, Chu CH. A novel systematic approach for product variant design using one-step quality function deployment. Paper presented at the 11th IEEE International Conference on Computer-Aided Design and Computer Graphics. 19-21 Aug 2009, Huangshan, China.
[25]Chien CS. Design and development of solar power assisted manual/electric wheelchair. Journal of Rehabilitation research and Development. 2014; 51(9):1411-26. doi: 10.1682/jrrd.2013.11.0250
[26]Pasawang T, Chatchanayuenyong T, Sa-Ngiamvibool W. QFD based conceptual design of an autonomous underwater robot. Songklanakarin Journal of Science & Technology. 2015; 37(6):659-68.
The assessment of needs and expectations of Indian wheelchair users resulted in both quantitative and qualitative data. Framework approach was applied to the qualitative data which revealed that most of the users are uncomfortable with bed to and from chair transfer, standing from sitting position, using commode/bathroom, generation of bedsores due to extensive use of the wheelchair. Four key themes emerged: 1. Difficulties in transfer from wheelchair to and from bed; 2. Problems to stand from sitting position; 3. Problems in using commode; and 4. Risk of bedsores due to extensive use of wheelchair. Furthermore, QFD analysis revealed that out of 11 design parameters recommended by cross-functional team based on needs assessment study the following parameters received the highest technical importance: 1. Seat to stand transfer feature (13.90%); 2. The bedsore prevention feature (12.60%); 3. Seat to sleep transfer feature (12.00%); and 4. Adjustable backrest feature with multi-posture adjustment feature (11.20%).
Figure 5 depicts the association of 20 user requirements and 11design parameters with their importance in terms of absolute technical importance and relative technical importance. Every design parameter has minimum one correlation with the user requirements, whereas every user requirement has two or more correlations with the design parameters. No vacant user requirement rows or design parameter columns were found in the matrix; hence, no inappropriate or unnecessary parameters existed. Each user requirement was responded by at least two design parameters.
5. Conclusion
This study presented the perspective of Indian wheelchair users through comprehensive needs assessment study. Second part of this paper reported primary wheelchair design parameters to improve the quality of life of people with disability and technological importance of each design parameter in order to prioritize them by aiming at an evidence-based design solution. It can be concluded that the users’ requirements reported by the Indian wheelchair users can be resolved by considering the high ranked design parameters suggested in this study. The design parameters with higher absolute and relative technical importance might be chosen to design new wheelchairs which will reflect the satisfaction of the wheelchair users. The design of wheelchair for users’ of a developed country might be inadequate in comparison to a developing country because the users’ needs are different. Hence, wheelchairs for Indian people with disability should be designed based on the needs assessment study. Thus, the results of this study can contribute to enhancing the existing wheelchair designs aimed at improving quality of life of people with disability.
Acknowledgements
The authors acknowledge all people who helped during conducting the research. We express our thanks to the subjects who volunteered to take part in this study. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for profit sectors.
Conflict of Interest
The authors declared no conflicts of interest.
References
[1]Office of the Registrar General & Census Commissioner. C-20 SC; Disabled population by type of disability, age and sex for scheduled castes (Census of India 2001). New Delhi: Office of the Registrar General & Census Commissioner; 2001.
[2]Lakhan R, Mario A, Qureshi FN, Hall ML. Early intervention services to children with developmental delay in resource poor settings in India. Nepal Journal of Medical Sciences. 2013; 2(2):149-55. doi: 10.3126/njms.v2i2.8966
[3]World Health Organization. World Report on Disability. Geneva: World Health Organization; 2011.
[4]Kumar SG, Roy G, Kar SS. Disability and rehabilitation services in India: Issues and challenges. Journal of Family Medicine and Primary Care. 2012; 1(1):69. doi: 10.4103/2249-4863.94458
[5]Pearlman J. Review session: Review of literature on wheelchairs for developing countries & Review of wheelchair provision in developing countries. Paper presented at A Consensus Conference on Wheelchairs for Developing Countries. 6-11 November 2006, Bengaluru, India.
[6]Lindle RS, Metter EJ, Lynch NA, Fleg JL, Fozard JL, Tobin J, et al. Age and gender comparisons of muscle strength in 654 women and men aged 20–93 year. Journal of Applied Physiology. 1997; 83(5):1581-7. PMID: 9375323
[7]Reid DT, Hebert D, Rudman D. Occupational performance in older stroke wheelchair users living at home. Occupational Therapy International. 2001; 8(4):273-86. doi: 10.1002/oti.151
[8]Belcher MJ, Frank AO. Survey of the use of transport by recipients of a regional Electric Indoor/Outdoor Powered (EPIOC) wheelchair service. Disability and Rehabilitation. 2004; 26(10):563-75. doi: 10.1080/09638280410001684055
[9]Edwards K, Mccluskey A. A survey of adult power wheelchair and scooter users. Disability and Rehabilitation: Assistive Technology. 2010; 5(6):411-9. doi: 10.3109/17483101003793412
[10]Evans S, Frank AO, Neophytou C, De Souza L. Older adults' use of, and satisfaction with, electric powered indoor/outdoor wheelchairs. Age and Ageing. 2007; 36(4):431-5. doi: 10.1093/ageing/afm034
[11]Pettersson C, Iwarsson S, Brandt Å, Norin L, Månsson Lexell E. Men’s and women’s perspectives on using a powered mobility device: Benefits and societal challenges. Scandinavian Journal of Occupational Therapy. 2014; 21(6):438-46. doi: 10.3109/11038128.2014.905634
[12]Mortenson WB, Hammell KW, Luts A, Soles C, Miller WC. The power of power wheelchairs: Mobility choices of community-dwelling, older adults. Scandinavian Journal of Occupational Therapy. 2015; 22(5):394-401. doi: 10.3109/11038128.2015.1049289
[13]Frank AO, De Souza LH, Frank JL, Neophytou C. The pain experiences of powered wheelchair users. Disability and Rehabilitation. 2012; 34(9):770-8. doi: 10.3109/09638288.2011.619620
[14]Wilkinson P. The changing role of physical testing in vehicle development programmes. Journal of Terramechanics. 2007; 44(1):15-22. doi: 10.1016/j.jterra.2006.01.004
[15]Marsot J. QFD: A methodological tool for integration of ergonomics at the design stage. Applied Ergonomics. 2005; 36(2):185-92. doi: 10.1016/j.apergo.2004.10.005
[16]Giesbrecht E. Application of the Human Activity Assistive Technology model for occupational therapy research. Australian Occupational Therapy Journal. 2013; 60(4):230-40. doi: 10.1111/1440-1630.12054
[17]Chen LH, Weng MC. An evaluation approach to engineering design in QFD processes using fuzzy goal programming models. European Journal of Operational Research. 2006; 172(1):230-48. doi: 10.1016/j.ejor.2004.10.004
[18]Park T, Kim KJ. Determination of an optimal set of design requirements using house of quality. Journal of Operations Management. 1998; 16(5):569-81. doi: 10.1016/s0272-6963(97)00029-6
[19]Vairaktarakis GL. Optimization tools for design and marketing of new/ improved products using the house of quality. Journal of Operations Management. 1999; 17(6):645-63. doi: 10.1016/s0272-6963(99)00020-0
[20]Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi disciplinary health research. BMC Medical Research Methodology. 2013; 13(1):117. doi: 10.1186/1471-2288-13-117
[21]Baccarini D. The logical framework method for defining project success. Project Management Journal. 1999; 30(4):25-32.
[22]Zadry HR, Rahmayanti D, Susanti L, Fatrias D. Identification of design requirements for ergonomic long spinal board using Quality Function Deployment (QFD). Procedia Manufacturing. 2015; 3:4673-80. doi: 10.1016/j.promfg.2015.07.559
[23]Tsai KH, Yeh CY, Lo HC, Li CT, Cheng CP, Chang GL. Application of quality function deployment in design of mobile assistive devices. Journal of Medical and Biological Engineering. 2008; 28(2):87-93.
[24]Tseng KC, Chu CH. A novel systematic approach for product variant design using one-step quality function deployment. Paper presented at the 11th IEEE International Conference on Computer-Aided Design and Computer Graphics. 19-21 Aug 2009, Huangshan, China.
[25]Chien CS. Design and development of solar power assisted manual/electric wheelchair. Journal of Rehabilitation research and Development. 2014; 51(9):1411-26. doi: 10.1682/jrrd.2013.11.0250
[26]Pasawang T, Chatchanayuenyong T, Sa-Ngiamvibool W. QFD based conceptual design of an autonomous underwater robot. Songklanakarin Journal of Science & Technology. 2015; 37(6):659-68.
Article type: Original Research Articles |
Subject:
methodology in rehabilitation
Received: 2017/08/24 | Accepted: 2017/10/20 | Published: 2017/12/1
Received: 2017/08/24 | Accepted: 2017/10/20 | Published: 2017/12/1
References
1. Office of the Registrar General & Census Commissioner. C-20 SC; Disabled population by type of disability, age and sex for scheduled castes (Census of India 2001). New Delhi: Office of the Registrar General & Census Commissioner; 2001.
2. Lakhan R, Mario A, Qureshi FN, Hall ML. Early intervention services to children with developmental delay in resource poor settings in India. Nepal Journal of Medical Sciences. 2013; 2(2):149-55. doi: 10.3126/njms.v2i2.8966 [DOI:10.3126/njms.v2i2.8966]
3. World Health Organization. World Report on Disability. Geneva: World Health Organization; 2011.
4. Kumar SG, Roy G, Kar SS. Disability and rehabilitation services in India: Issues and challenges. Journal of Family Medicine and Primary Care. 2012; 1(1):69. doi: 10.4103/2249-4863.94458 [DOI:10.4103/2249-4863.94458]
5. Pearlman J. Review session: Review of literature on wheelchairs for developing countries & Review of wheelchair provision in developing countries. Paper presented at A Consensus Conference on Wheelchairs for Developing Countries. 6-11 November 2006, Bengaluru, India.
6. Lindle RS, Metter EJ, Lynch NA, Fleg JL, Fozard JL, Tobin J, et al. Age and gender comparisons of muscle strength in 654 women and men aged 20–93 year. Journal of Applied Physiology. 1997; 83(5):1581-7. PMID: 9375323 [DOI:10.1152/jappl.1997.83.5.1581] [PMID]
7. Reid DT, Hebert D, Rudman D. Occupational performance in older stroke wheelchair users living at home. Occupational Therapy International. 2001; 8(4):273-86. doi: 10.1002/oti.151 [DOI:10.1002/oti.151]
8. Belcher MJ, Frank AO. Survey of the use of transport by recipients of a regional Electric Indoor/Outdoor Powered (EPIOC) wheelchair service. Disability and Rehabilitation. 2004; 26(10):563-75. doi: 10.1080/09638280410001684055 [DOI:10.1080/09638280410001684055]
9. Edwards K, Mccluskey A. A survey of adult power wheelchair and scooter users. Disability and Rehabilitation: Assistive Technology. 2010; 5(6):411-9. doi: 10.3109/17483101003793412 [DOI:10.3109/17483101003793412]
10. Evans S, Frank AO, Neophytou C, De Souza L. Older adults' use of, and satisfaction with, electric powered indoor/outdoor wheelchairs. Age and Ageing. 2007; 36(4):431-5. doi: 10.1093/ageing/afm034 [DOI:10.1093/ageing/afm034]
11. Pettersson C, Iwarsson S, Brandt Å, Norin L, Månsson Lexell E. Men's and women's perspectives on using a powered mobility device: Benefits and societal challenges. Scandinavian Journal of Occupational Therapy. 2014; 21(6):438-46. doi: 10.3109/11038128.2014.905634 [DOI:10.3109/11038128.2014.905634]
12. Mortenson WB, Hammell KW, Luts A, Soles C, Miller WC. The power of power wheelchairs: Mobility choices of community-dwelling, older adults. Scandinavian Journal of Occupational Therapy. 2015; 22(5):394-401. doi: 10.3109/11038128.2015.1049289 [DOI:10.3109/11038128.2015.1049289]
13. Frank AO, De Souza LH, Frank JL, Neophytou C. The pain experiences of powered wheelchair users. Disability and Rehabilitation. 2012; 34(9):770-8. doi: 10.3109/09638288.2011.619620 [DOI:10.3109/09638288.2011.619620]
14. Wilkinson P. The changing role of physical testing in vehicle development programmes. Journal of Terramechanics. 2007; 44(1):15-22. doi: 10.1016/j.jterra.2006.01.004 [DOI:10.1016/j.jterra.2006.01.004]
15. Marsot J. QFD: A methodological tool for integration of ergonomics at the design stage. Applied Ergonomics. 2005; 36(2):185-92. doi: 10.1016/j.apergo.2004.10.005 [DOI:10.1016/j.apergo.2004.10.005]
16. Giesbrecht E. Application of the Human Activity Assistive Technology model for occupational therapy research. Australian Occupational Therapy Journal. 2013; 60(4):230-40. doi: 10.1111/1440-1630.12054 [DOI:10.1111/1440-1630.12054]
17. Chen LH, Weng MC. An evaluation approach to engineering design in QFD processes using fuzzy goal programming models. European Journal of Operational Research. 2006; 172(1):230-48. doi: 10.1016/j.ejor.2004.10.004 [DOI:10.1016/j.ejor.2004.10.004]
18. Park T, Kim KJ. Determination of an optimal set of design requirements using house of quality. Journal of Operations Management. 1998; 16(5):569-81. doi: 10.1016/s0272-6963(97)00029-6 [DOI:10.1016/S0272-6963(97)00029-6]
19. Vairaktarakis GL. Optimization tools for design and marketing of new/ improved products using the house of quality. Journal of Operations Management. 1999; 17(6):645-63. doi: 10.1016/s0272-6963(99)00020-0 [DOI:10.1016/S0272-6963(99)00020-0]
20. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi disciplinary health research. BMC Medical Research Methodology. 2013; 13(1):117. doi: 10.1186/1471-2288-13-117 [DOI:10.1186/1471-2288-13-117]
21. Baccarini D. The logical framework method for defining project success. Project Management Journal. 1999; 30(4):25-32.
22. Zadry HR, Rahmayanti D, Susanti L, Fatrias D. Identification of design requirements for ergonomic long spinal board using Quality Function Deployment (QFD). Procedia Manufacturing. 2015; 3:4673-80. doi: 10.1016/j.promfg.2015.07.559 [DOI:10.1016/j.promfg.2015.07.559]
23. Tsai KH, Yeh CY, Lo HC, Li CT, Cheng CP, Chang GL. Application of quality function deployment in design of mobile assistive devices. Journal of Medical and Biological Engineering. 2008; 28(2):87-93.
24. Tseng KC, Chu CH. A novel systematic approach for product variant design using one-step quality function deployment. Paper presented at the 11th IEEE International Conference on Computer-Aided Design and Computer Graphics. 19-21 Aug 2009, Huangshan, China. [DOI:10.1109/CADCG.2009.5246840]
25. Chien CS. Design and development of solar power assisted manual/electric wheelchair. Journal of Rehabilitation research and Development. 2014; 51(9):1411-26. doi: 10.1682/jrrd.2013.11.0250 [DOI:10.1682/JRRD.2013.11.0250]
26. Pasawang T, Chatchanayuenyong T, Sa-Ngiamvibool W. QFD based conceptual design of an autonomous underwater robot. Songklanakarin Journal of Science & Technology. 2015; 37(6):659-68.
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
