
988368
Wed, May 27, 2026

Volume 22, Issue 1 (March 2024)
Iranian Rehabilitation Journal 2024, 22(1): 15-24 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nazir A, Tiksnadi B B, Ridzki M F F A. Exercise-based Rehabilitation to Improve Exercise Tolerance of Severe COVID-19 Survivors: A Review Paper. Iranian Rehabilitation Journal 2024; 22 (1) :15-24
URL: http://irj.uswr.ac.ir/article-1-1630-en.html
URL: http://irj.uswr.ac.ir/article-1-1630-en.html



1- Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Dr. Hasan Sadikin General Hospital, Padjadjaran University, Bandung, Indonesia.
2- Department of Cardiology and Vascular Medicine, Faculty of Medicine, Dr. Hasan Sadikin General Hospital, Padjadjaran University, Bandung, Indonesia.
3- Faculty of Medicine, Padjadjaran University, Bandung, Indonesia.
2- Department of Cardiology and Vascular Medicine, Faculty of Medicine, Dr. Hasan Sadikin General Hospital, Padjadjaran University, Bandung, Indonesia.
3- Faculty of Medicine, Padjadjaran University, Bandung, Indonesia.
Full-Text [PDF 496 kb]
(1053 Downloads)
| Abstract (HTML) (3301 Views)
Full-Text: (567 Views)
Introduction
Muscle weakness after acute phase recovery from COVID-19 is a real problem that could be experienced by survivors. As many as 10%-20% of COVID-19 patients experience persistent symptoms weeks to months after the acute phase of COVID-19 [1]. Research shows that survivors of severe COVID-19 can have various functional complications as a “follow-up”, such as persistent shortness of breath and post-intensive care syndrome which is characterized by muscle weakness, joint stiffness, deconditioning, cognitive dysfunction, psychiatric illness, and quadriparesis that persist after resolution of the acute illness [2–4].
COVID-19 survivors may experience a decrease in long-term exercise tolerance [5]. Research showed that COVID-19 survivors can experience a decrease in exercise capacity (VO2 max). VO2 max decreased by more than 10% compared to before infection [6]. Other studies showed that survivors of COVID-19 could have a VO2 max <80% of the predicted value after 3 months of being discharged from the hospital. The distance of the six-minute walk test (6-MWT) was decreased and a minimum SpO2 value in the 6-MWT was <96% 6 months after discharge from the hospital [7, 8]. The decrease in the functional capacity of COVID-19 survivors is not only caused by pulmonary organ dysfunction and decreased gas exchange but also by extrapulmonary factors such as cardiac dysfunction and muscle weakness associated with long-term hospitalization and immobilization after recovery from the acute phase of COVID-19 [9, 10]. Survivors of severe COVID-19 could have a significantly greater decrease in exercise tolerance than survivors of mild COVID-19 [11-13]. Decreased exercise tolerance in COVID-19 survivors can result in increased morbidity and mortality, decreased quality of life, and a continuous increase in the burden on the health system [10, 14].
Rehabilitation is a multidisciplinary intervention that reduces morbidity, increases functional independence, and improves the ability to carry out daily activities. Based on the characteristics and complications caused by COVID-19, exercise-based multidisciplinary rehabilitation has the opportunity to increase functional capacity, provide a better prognosis, prevent long-term disability, and improve the quality of life of COVID-19 survivors [11, 15–17].
The magnitude of the negative physical impact on the survivors of COVID-19 and the absence of standardized guidelines in the implementation of rehabilitation were the reasons to conduct this review. In addition, the presence of potential barriers is important to know to determine the strategy to overcome the rehabilitation problems. This review aimed to determine the form, results, and barriers to exercise-based rehabilitation programs for severe COVID-19 survivors.
Materials and Methods
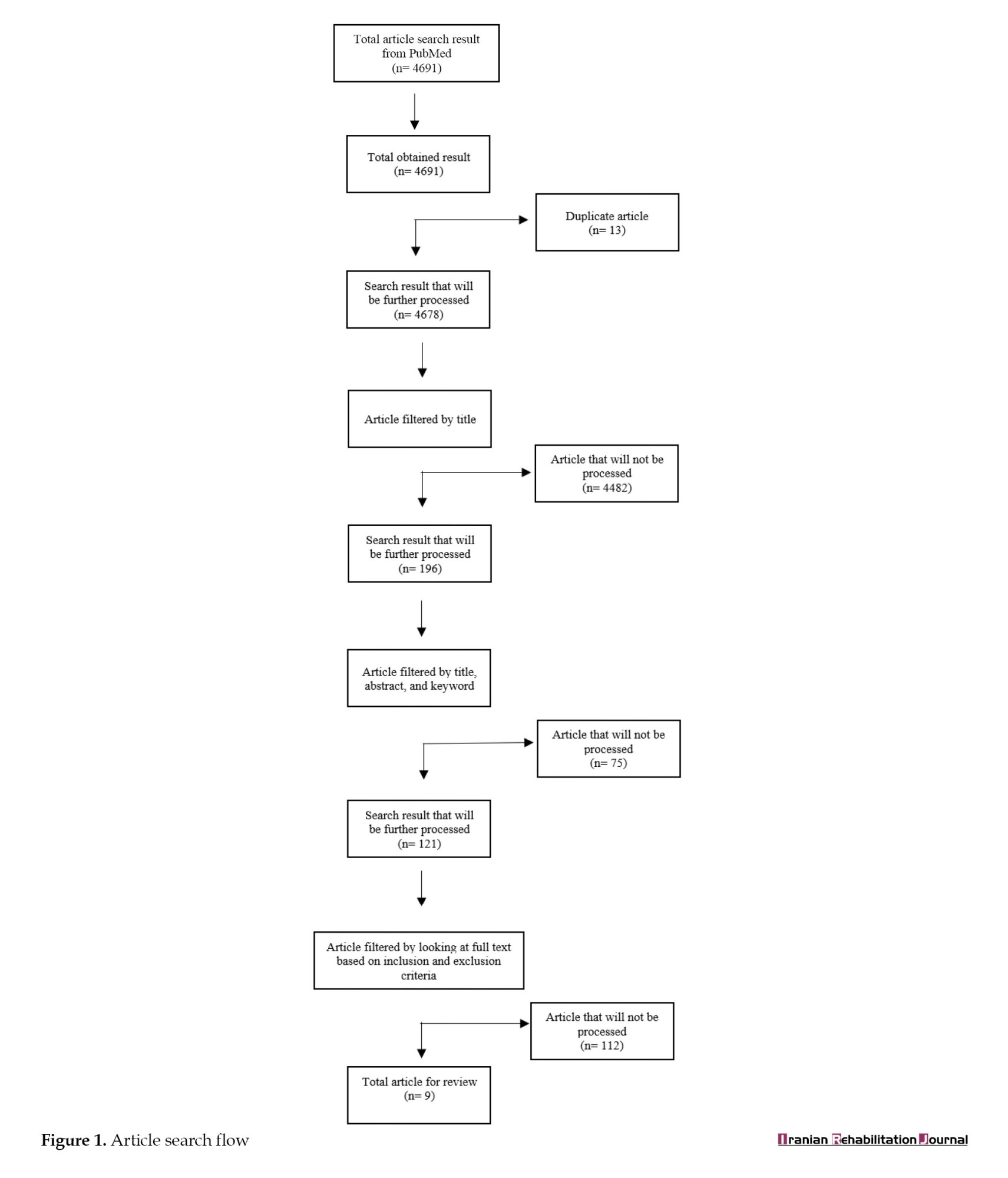
This study uses an article review method by collecting and synthesizing data from the article related to exercise-based rehabilitation in severe COVID-19 survivors. Searching for the article was carried out from August to October 2021. We used the PubMed database as a search media with the keywords ([‘COVID-19’ OR ‘COVID-19’ OR ‘SARS CoV-2’ OR ‘post COVID-19’]AND [‘rehabilitation’]). The type of articles used were original articles and case reports published in the last 2 years (2019-2021), available in English, and accessible in PDF or HTML format. Articles were excluded if they did not fit the research topic and were not available in full text. The article search flow is described in Figure 1.
Results
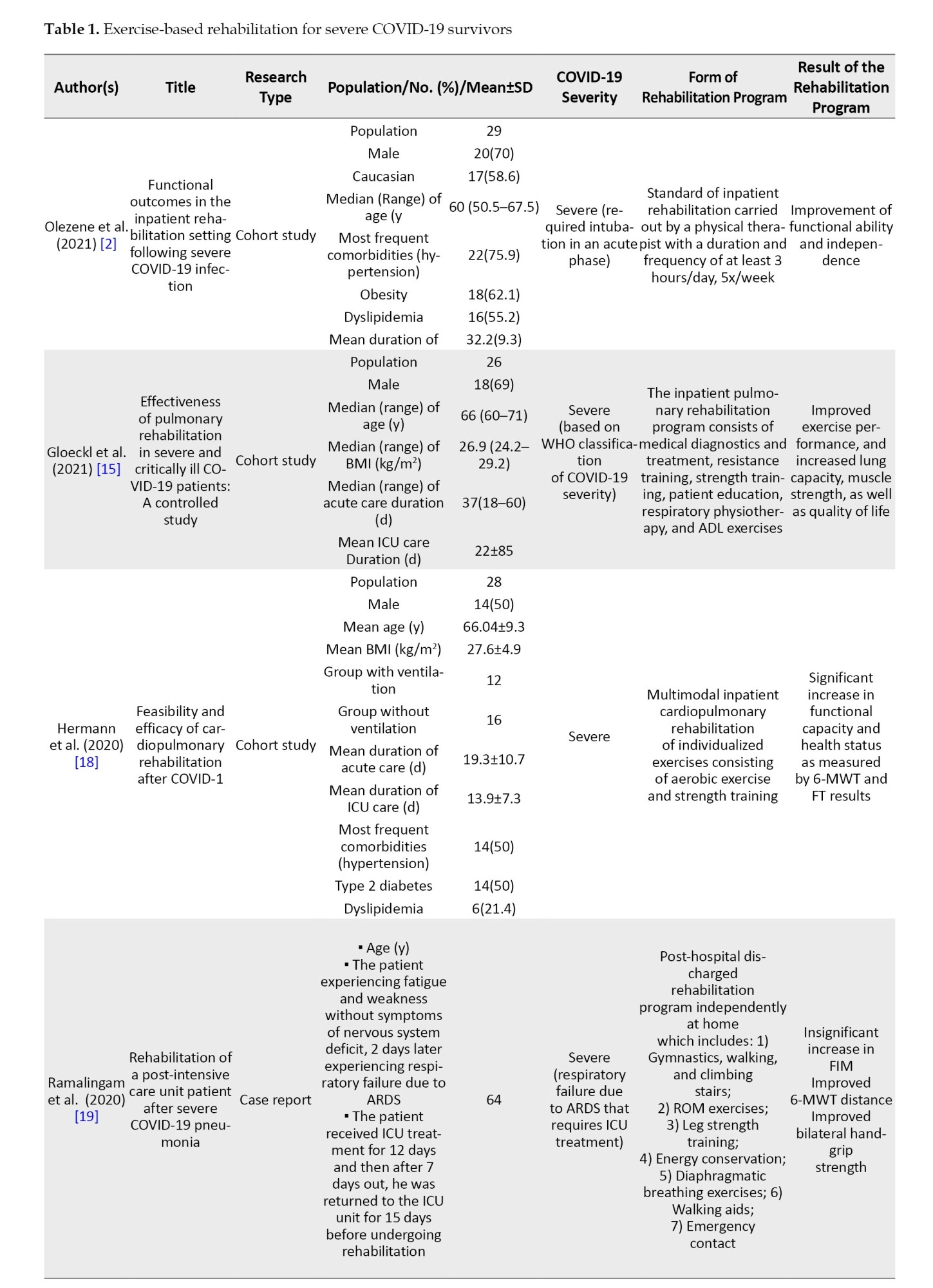
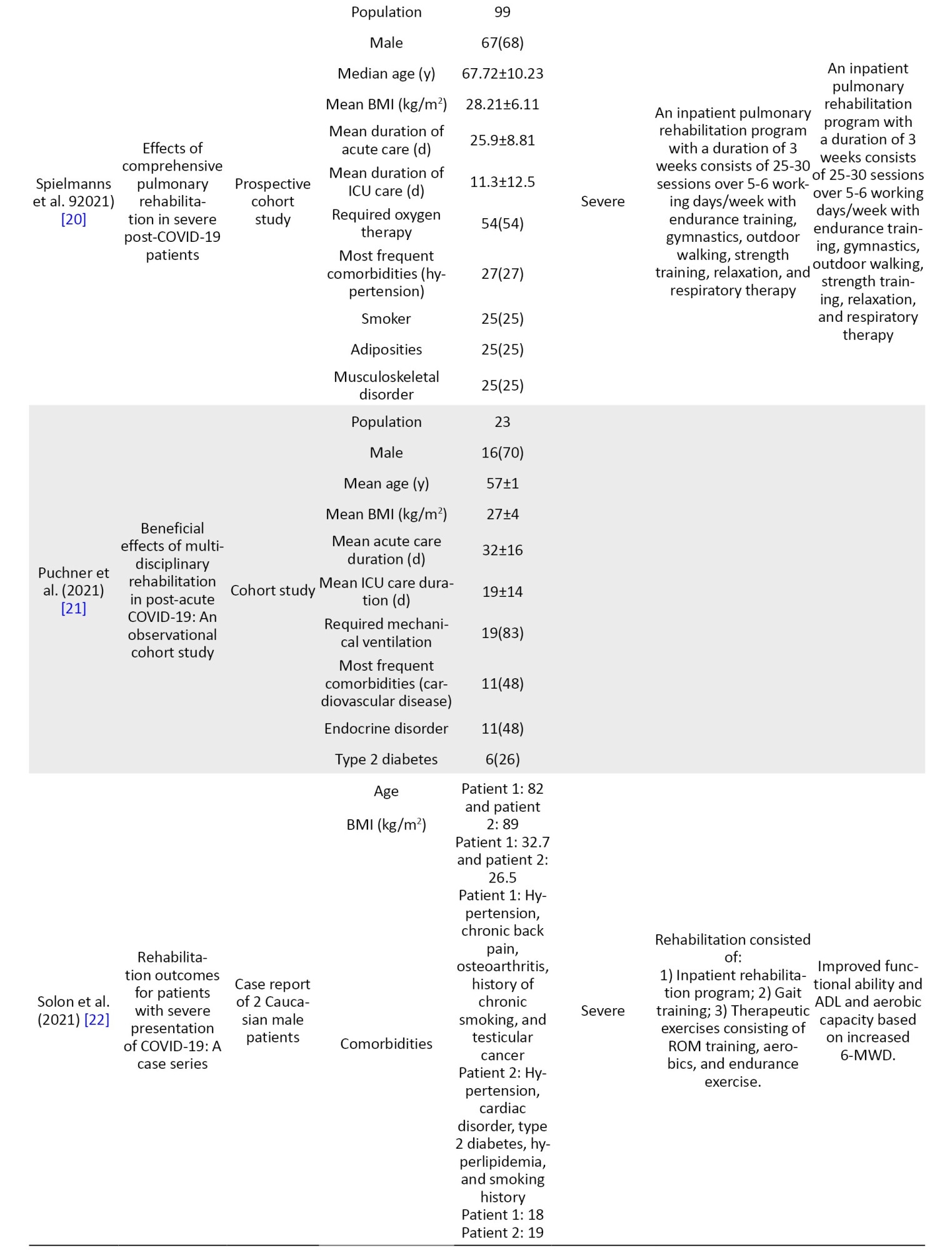
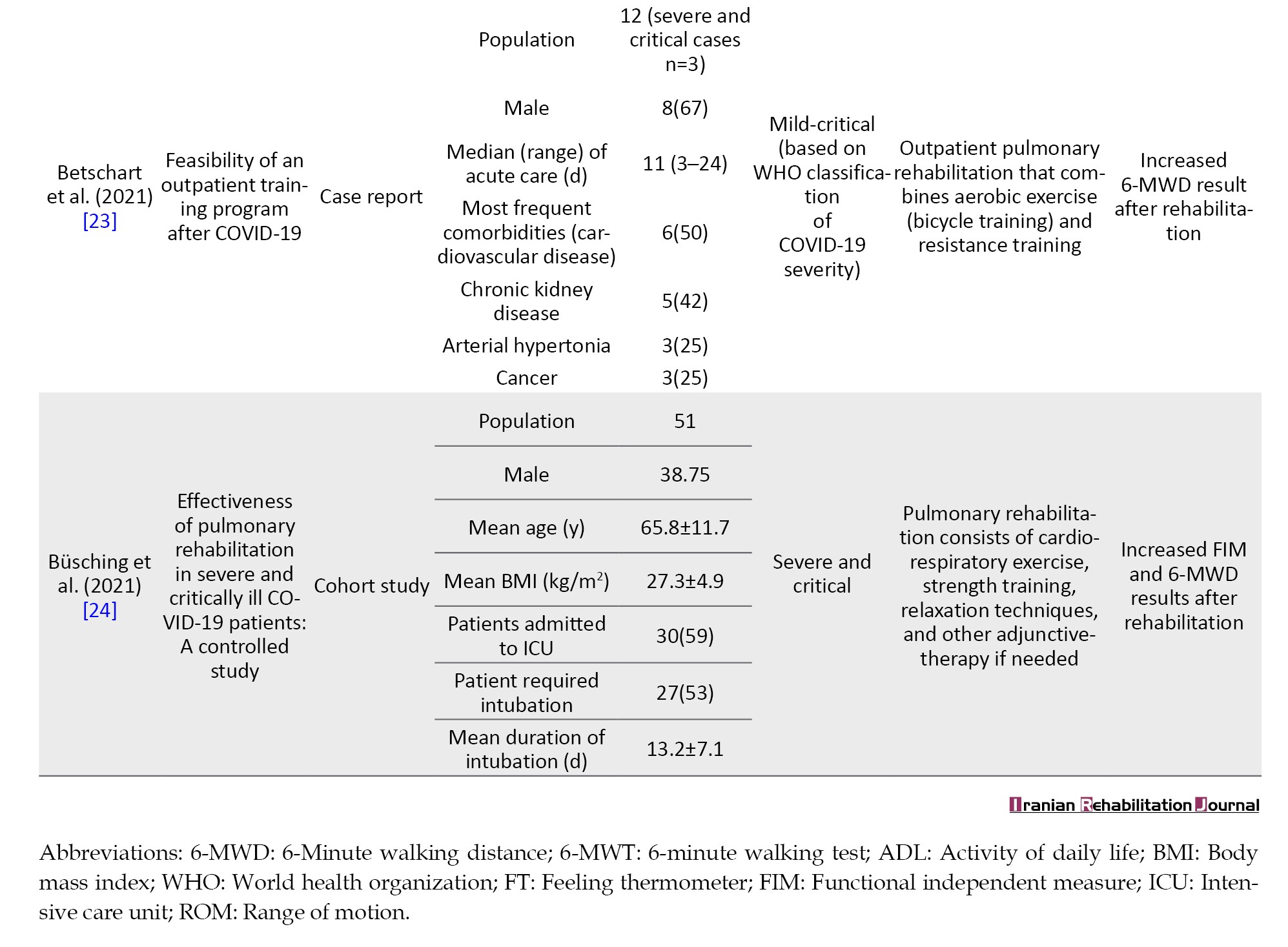
There were a total of 4691 articles found at the initial screening using keywords. In the next screening using the inclusion and exclusion criteria and after reading the whole articles, we found 9 articles that matched the topic. Of these, 7 articles were original articles and 2 case reports (Figure 1). Nine articles discussed the forms and outcomes of exercise-based rehabilitation and no article discussed the barriers to rehabilitation. Nine articles outlined cardiopulmonary rehabilitation as a rehabilitation effort for COVID-19 survivors which consisted of a combination of various exercises such as aerobic exercise, resistance training, strength training, activities of daily living (ADL) training, and breathing exercises. A total of 9 articles explained an increase in functional ability and quality of life of COVID-19 survivors in severe cases (Table 1) [2,15,18-24].
Discussion
Rehabilitation of COVID-19 survivors focuses on treating ongoing disorders including impaired mobility, respiratory function, nutrition, and communication to promote independence in performing ADL. The rehabilitation program provided is an ongoing treatment that is specific in nature according to the needs and abilities of the patient [12, 25].
Exercise-based rehabilitation for severe COVID-19 survivors
Based on the articles reviewed, it was found that the exercise to increase exercise tolerance in survivors of severe COVID-19 cases was generally given in the form of physical exercise which was included in the cardiopulmonary rehabilitation program [15, 18, 23, 24]. The physical exercise program consisted of aerobic exercise, muscle strength training (weight training), resistance training, breathing exercises, and ROM exercises. The exercise program was given since the patient was hospitalized until the outpatient phase [18–20]. These forms of exercise are also supported by several previous studies discussing rehabilitation in COVID-19 survivors.
Gentil et al. (2021) recommended resistance training for COVID-19 survivors. The form of resistance training was resistance exercise with a low-volume and multi-joint. In addition, low external load resistance training can also be carried out by the patient and can provide the same results as high external load resistance training which is carried out with greater effort. As an alternative, high-velocity resistance training can be given if the patient cannot perform low/high external load training. [26].
A review article conducted by Agostini et al. (2021) mentioned the recommendation of aerobic exercise starting with low to moderate-intensity exercise which was increased gradually according to individual abilities [27]. Another review article study was conducted by Calabrese et al. (2021) recommended interval aerobic training with moderate to high intensity performed 3-5 times a week, for COVID-19 survivors [17].
Individually prescribed exercises according to the ability of the patient could also be given [18, 28]. The rehabilitation program can be provided for a minimum of 3 weeks in the inpatient phase and for 3 weeks during the outpatient phase [2]. Home-based exercise with telerehabilitation can also be given as a substitution for face-to-face rehabilitation programs [17]. There is no standard protocol for physical exercise for COVID-19 survivors with severe cases yet, either in the inpatient or outpatient phase.
Result of exercise-based rehabilitation for COVID-19 survivors
The exercise-based cardiopulmonary rehabilitation program given to severe COVID-19 survivors could improve exercise tolerance, functional independence in ADL, as well as general health status which has a positive impact on the quality of life of survivors [2, 15, 18–20, 22–24]. A cohort study conducted by Olezene et al. (2021) showed that the multimodal rehabilitation program given to survivors of severe COVID-19 cases increased exercise tolerance as measured by an increase in the 6-MWT distance of 557.9 meters compared to before rehabilitation. This study also mentions an increase in 10-MWT speed of 0.61 meters/second and functional independence as measured by the ability for independence transfer and ambulation [2].
Another review reported similar results in an increase in 6-MWT distance and functional independence as measured by functional independence measure (FIM) after being given a combination of aerobic, endurance, strength, and breathing exercises [19, 20, 22, 24]. A rehabilitation program consisting of the series of these exercises which was increased gradually in intensity could also improve muscle strength and function as measured by an increase in bilateral hand muscle strength by 5 kg, peak quadriceps muscle strength by 21.2% of predicted value, and sit to stand speed by 3 seconds [15].
Articles reviewed in this study also described similar results with several previous studies. Agostini, et al. (2021) found that comprehensive cardiopulmonary rehabilitation improved mobilization and ADL functions as well as neuropsychological status [15, 21, 27]. A previous article review conducted by Gentil et al. (2021) found that resistance exercise could also improve cardiovascular function, physical ability, and functional capacity in addition to increased muscle mass strength [26].
A cohort study conducted by Puchner et al. (2021) also found an increase in lung capacity in COVID-19 survivors after multidisciplinary rehabilitation with a duration of 3 weeks [21]. In addition, cardiovascular rehabilitation consisting of aerobic and interval training had a positive impact on improving cardiovascular function, decreasing blood pressure after exercise, and respiratory function [17].
The barrier of exercise-based rehabilitation for COVID-19 survivors
There was no article found that discussed barriers to the rehabilitation of COVID-19 survivors. The scoping review by Wasilewski et al. (2021) [25] described barriers to COVID-19 rehabilitation which were divided as follows: 1) COVID-19 infectivity (causing limitation of patients’ access to rehabilitation facilities, prohibition to mobilize to public areas, prohibition to the involvement of the families in patients’ care, and closure of healthcare facilities); 2) Patient health status (diversity in the severity of COVID-19, disability, and instability of the patient’s condition); 3) Lack of guidance in the rehabilitation management; 4) Problems related to the availability of personal protective equipment; 5) Problems related to healthcare staff (decreased health status of medical personnel, high workload, and fear of being infected with COVID -19); and 6) Problems in the health system (lack of communication between levels, lack of costs, and unpreparedness of health services to provide rehabilitation services) [25]. Barriers to the rehabilitation of COVID-19 survivors can occur in all phases of care [29].
To our knowledge, this study is the first to specifically discuss exercises to increase exercise tolerance in COVID patients and this study explores exercises to increase exercise tolerance from inpatient care to outpatient care. So, the results of this study can be used as a basis for efforts to prevent lowering exercise tolerance in COVID patients by providing exercise as early as possible after the patient is admitted. The weakness of this study is searching only 1 search engine so there is the possibility of other similar studies that are not explored.
Conclusion
Research on the rehabilitation of COVID-19 survivors is still limited in number, especially regarding the rehabilitation of severe cases survivors. Based on the reviewed articles, we found that the rehabilitation program was generally provided in both inpatient and outpatient cardiopulmonary rehabilitation programs. Exercises given were aerobic exercise, resistance, and strength training, as well as ADL, range of motion (ROM), breathing, and other exercises. The exercise program was given as needed and tailored to the patient’s needs. Exercise-based rehabilitation of severe COVID-19 survivors improved exercise tolerance, functional ability, and quality of life. Exercise could also improve organ function affected in the acute phase of COVID-19. There were several barriers encountered in the implementation of exercise-based rehabilitation such as the patient’s condition, COVID-19 infectivity, lack of guidelines, and issues related to the provision of health services.
Ethical Considerations
Compliance with ethical guidelines
This systematic review is regarded exclusively on published literature.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors
Authors' contributions
Conceptualization: Arnengsih Nazir; Supervision: Arnengsih Nazir and Badai Bhatara Tiksnadi; Methodology, investigation, writing, funding acquisition and resources: All authors.
Conflict of interest
The authors declared no conflict of interest
Acknowledgments
The author would like to thank Padjadjaran University and Dr. Hasan Sadikin General Hospital for the opportunity to conduct this work and for database facilitation.
References
Muscle weakness after acute phase recovery from COVID-19 is a real problem that could be experienced by survivors. As many as 10%-20% of COVID-19 patients experience persistent symptoms weeks to months after the acute phase of COVID-19 [1]. Research shows that survivors of severe COVID-19 can have various functional complications as a “follow-up”, such as persistent shortness of breath and post-intensive care syndrome which is characterized by muscle weakness, joint stiffness, deconditioning, cognitive dysfunction, psychiatric illness, and quadriparesis that persist after resolution of the acute illness [2–4].
COVID-19 survivors may experience a decrease in long-term exercise tolerance [5]. Research showed that COVID-19 survivors can experience a decrease in exercise capacity (VO2 max). VO2 max decreased by more than 10% compared to before infection [6]. Other studies showed that survivors of COVID-19 could have a VO2 max <80% of the predicted value after 3 months of being discharged from the hospital. The distance of the six-minute walk test (6-MWT) was decreased and a minimum SpO2 value in the 6-MWT was <96% 6 months after discharge from the hospital [7, 8]. The decrease in the functional capacity of COVID-19 survivors is not only caused by pulmonary organ dysfunction and decreased gas exchange but also by extrapulmonary factors such as cardiac dysfunction and muscle weakness associated with long-term hospitalization and immobilization after recovery from the acute phase of COVID-19 [9, 10]. Survivors of severe COVID-19 could have a significantly greater decrease in exercise tolerance than survivors of mild COVID-19 [11-13]. Decreased exercise tolerance in COVID-19 survivors can result in increased morbidity and mortality, decreased quality of life, and a continuous increase in the burden on the health system [10, 14].
Rehabilitation is a multidisciplinary intervention that reduces morbidity, increases functional independence, and improves the ability to carry out daily activities. Based on the characteristics and complications caused by COVID-19, exercise-based multidisciplinary rehabilitation has the opportunity to increase functional capacity, provide a better prognosis, prevent long-term disability, and improve the quality of life of COVID-19 survivors [11, 15–17].
The magnitude of the negative physical impact on the survivors of COVID-19 and the absence of standardized guidelines in the implementation of rehabilitation were the reasons to conduct this review. In addition, the presence of potential barriers is important to know to determine the strategy to overcome the rehabilitation problems. This review aimed to determine the form, results, and barriers to exercise-based rehabilitation programs for severe COVID-19 survivors.
Materials and Methods
This study uses an article review method by collecting and synthesizing data from the article related to exercise-based rehabilitation in severe COVID-19 survivors. Searching for the article was carried out from August to October 2021. We used the PubMed database as a search media with the keywords ([‘COVID-19’ OR ‘COVID-19’ OR ‘SARS CoV-2’ OR ‘post COVID-19’]AND [‘rehabilitation’]). The type of articles used were original articles and case reports published in the last 2 years (2019-2021), available in English, and accessible in PDF or HTML format. Articles were excluded if they did not fit the research topic and were not available in full text. The article search flow is described in Figure 1.
Results
There were a total of 4691 articles found at the initial screening using keywords. In the next screening using the inclusion and exclusion criteria and after reading the whole articles, we found 9 articles that matched the topic. Of these, 7 articles were original articles and 2 case reports (Figure 1). Nine articles discussed the forms and outcomes of exercise-based rehabilitation and no article discussed the barriers to rehabilitation. Nine articles outlined cardiopulmonary rehabilitation as a rehabilitation effort for COVID-19 survivors which consisted of a combination of various exercises such as aerobic exercise, resistance training, strength training, activities of daily living (ADL) training, and breathing exercises. A total of 9 articles explained an increase in functional ability and quality of life of COVID-19 survivors in severe cases (Table 1) [2,15,18-24].
Discussion
Rehabilitation of COVID-19 survivors focuses on treating ongoing disorders including impaired mobility, respiratory function, nutrition, and communication to promote independence in performing ADL. The rehabilitation program provided is an ongoing treatment that is specific in nature according to the needs and abilities of the patient [12, 25].
Exercise-based rehabilitation for severe COVID-19 survivors
Based on the articles reviewed, it was found that the exercise to increase exercise tolerance in survivors of severe COVID-19 cases was generally given in the form of physical exercise which was included in the cardiopulmonary rehabilitation program [15, 18, 23, 24]. The physical exercise program consisted of aerobic exercise, muscle strength training (weight training), resistance training, breathing exercises, and ROM exercises. The exercise program was given since the patient was hospitalized until the outpatient phase [18–20]. These forms of exercise are also supported by several previous studies discussing rehabilitation in COVID-19 survivors.
Gentil et al. (2021) recommended resistance training for COVID-19 survivors. The form of resistance training was resistance exercise with a low-volume and multi-joint. In addition, low external load resistance training can also be carried out by the patient and can provide the same results as high external load resistance training which is carried out with greater effort. As an alternative, high-velocity resistance training can be given if the patient cannot perform low/high external load training. [26].
A review article conducted by Agostini et al. (2021) mentioned the recommendation of aerobic exercise starting with low to moderate-intensity exercise which was increased gradually according to individual abilities [27]. Another review article study was conducted by Calabrese et al. (2021) recommended interval aerobic training with moderate to high intensity performed 3-5 times a week, for COVID-19 survivors [17].
Individually prescribed exercises according to the ability of the patient could also be given [18, 28]. The rehabilitation program can be provided for a minimum of 3 weeks in the inpatient phase and for 3 weeks during the outpatient phase [2]. Home-based exercise with telerehabilitation can also be given as a substitution for face-to-face rehabilitation programs [17]. There is no standard protocol for physical exercise for COVID-19 survivors with severe cases yet, either in the inpatient or outpatient phase.
Result of exercise-based rehabilitation for COVID-19 survivors
The exercise-based cardiopulmonary rehabilitation program given to severe COVID-19 survivors could improve exercise tolerance, functional independence in ADL, as well as general health status which has a positive impact on the quality of life of survivors [2, 15, 18–20, 22–24]. A cohort study conducted by Olezene et al. (2021) showed that the multimodal rehabilitation program given to survivors of severe COVID-19 cases increased exercise tolerance as measured by an increase in the 6-MWT distance of 557.9 meters compared to before rehabilitation. This study also mentions an increase in 10-MWT speed of 0.61 meters/second and functional independence as measured by the ability for independence transfer and ambulation [2].
Another review reported similar results in an increase in 6-MWT distance and functional independence as measured by functional independence measure (FIM) after being given a combination of aerobic, endurance, strength, and breathing exercises [19, 20, 22, 24]. A rehabilitation program consisting of the series of these exercises which was increased gradually in intensity could also improve muscle strength and function as measured by an increase in bilateral hand muscle strength by 5 kg, peak quadriceps muscle strength by 21.2% of predicted value, and sit to stand speed by 3 seconds [15].
Articles reviewed in this study also described similar results with several previous studies. Agostini, et al. (2021) found that comprehensive cardiopulmonary rehabilitation improved mobilization and ADL functions as well as neuropsychological status [15, 21, 27]. A previous article review conducted by Gentil et al. (2021) found that resistance exercise could also improve cardiovascular function, physical ability, and functional capacity in addition to increased muscle mass strength [26].
A cohort study conducted by Puchner et al. (2021) also found an increase in lung capacity in COVID-19 survivors after multidisciplinary rehabilitation with a duration of 3 weeks [21]. In addition, cardiovascular rehabilitation consisting of aerobic and interval training had a positive impact on improving cardiovascular function, decreasing blood pressure after exercise, and respiratory function [17].
The barrier of exercise-based rehabilitation for COVID-19 survivors
There was no article found that discussed barriers to the rehabilitation of COVID-19 survivors. The scoping review by Wasilewski et al. (2021) [25] described barriers to COVID-19 rehabilitation which were divided as follows: 1) COVID-19 infectivity (causing limitation of patients’ access to rehabilitation facilities, prohibition to mobilize to public areas, prohibition to the involvement of the families in patients’ care, and closure of healthcare facilities); 2) Patient health status (diversity in the severity of COVID-19, disability, and instability of the patient’s condition); 3) Lack of guidance in the rehabilitation management; 4) Problems related to the availability of personal protective equipment; 5) Problems related to healthcare staff (decreased health status of medical personnel, high workload, and fear of being infected with COVID -19); and 6) Problems in the health system (lack of communication between levels, lack of costs, and unpreparedness of health services to provide rehabilitation services) [25]. Barriers to the rehabilitation of COVID-19 survivors can occur in all phases of care [29].
To our knowledge, this study is the first to specifically discuss exercises to increase exercise tolerance in COVID patients and this study explores exercises to increase exercise tolerance from inpatient care to outpatient care. So, the results of this study can be used as a basis for efforts to prevent lowering exercise tolerance in COVID patients by providing exercise as early as possible after the patient is admitted. The weakness of this study is searching only 1 search engine so there is the possibility of other similar studies that are not explored.
Conclusion
Research on the rehabilitation of COVID-19 survivors is still limited in number, especially regarding the rehabilitation of severe cases survivors. Based on the reviewed articles, we found that the rehabilitation program was generally provided in both inpatient and outpatient cardiopulmonary rehabilitation programs. Exercises given were aerobic exercise, resistance, and strength training, as well as ADL, range of motion (ROM), breathing, and other exercises. The exercise program was given as needed and tailored to the patient’s needs. Exercise-based rehabilitation of severe COVID-19 survivors improved exercise tolerance, functional ability, and quality of life. Exercise could also improve organ function affected in the acute phase of COVID-19. There were several barriers encountered in the implementation of exercise-based rehabilitation such as the patient’s condition, COVID-19 infectivity, lack of guidelines, and issues related to the provision of health services.
Ethical Considerations
Compliance with ethical guidelines
This systematic review is regarded exclusively on published literature.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors
Authors' contributions
Conceptualization: Arnengsih Nazir; Supervision: Arnengsih Nazir and Badai Bhatara Tiksnadi; Methodology, investigation, writing, funding acquisition and resources: All authors.
Conflict of interest
The authors declared no conflict of interest
Acknowledgments
The author would like to thank Padjadjaran University and Dr. Hasan Sadikin General Hospital for the opportunity to conduct this work and for database facilitation.
References
- World Health Organization (WHO). Expanding our understanding of post-COVID-19 condition web series: Rehabilitation care [Internet]. 2021 [Updated 2021 November 1]. Available from: [Link]
- Olezene CS, Hansen E, Steere HK, Giacino JT, Polich GR, Borg-Stein J, et al. Functional outcomes in the inpatient rehabilitation setting following severe COVID-19 infection. Plos One. 2021; 16(3):e0248824. [DOI:10.1371/journal.pone.0248824] [PMID] [PMCID]
- Demeco A, Marotta N, Barletta M, Pino I, Marinaro C, Petraroli A, et al. Rehabilitation of patients post-COVID-19 infection: A literature review. The Journal of International Medical Research. 2020; 48(8):300060520948382. [DOI:10.1177/0300060520948382] [PMID] [PMCID]
- Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, et al. Post-acute COVID-19 syndrome. Nature Medicine. 2021; 27(4):601-15. [DOI:10.1038/s41591-021-01283-z] [PMID] [PMCID]
- Paneroni M, Vitacca M, Bernocchi P, Bertacchini L, Scalvini S. Feasibility of tele-rehabilitation in survivors of COVID-19 pneumonia. Pulmonology. 2022; 28(2):152-4. [DOI:10.1016/j.pulmoe.2021.03.009] [PMID] [PMCID]
- Crameri GAG, Bielecki M, Züst R, Buehrer TW, Stanga Z, Deuel JW. Reduced maximal aerobic capacity after COVID-19 in young adult recruits, Switzerland, May 2020. Euro Surveillance. 2020; 25(36):2001542. [DOI:10.2807/1560-7917.ES.2020.25.36.2001542] [PMID] [PMCID]
- Skjørten I, Ankerstjerne OAW, Trebinjac D, Brønstad E, Rasch-Halvorsen Ø, Einvik G, et al. Cardiopulmonary exercise capacity and limitations 3 months after COVID-19 hospitalisation. The European Respiratory Journal. 2021; 58(2):2100996. [DOI:10.1183/13993003.00996-2021] [PMID] [PMCID]
- Saeki T, Ogawa F, Matsumiya M, Yamamura M, Oritsu H, Nonogaki M, et al. Long-term decreased exercise capacity of COVID-19 patients who received mechanical ventilation in Japan: A case series. American Journal of Physical Medicine & Rehabilitation. 2021; 100(8):737-41. [DOI:10.1097/PHM.0000000000001803] [PMID]
- Gao Y, Chen R, Geng Q, Mo X, Zhan C, Jian W, et al. Cardiopulmonary exercise testing might be helpful for interpretation of impaired pulmonary function in recovered COVID-19 patients. The European Respiratory Journal. 2021; 57(1):2004265. [DOI:10.1183/13993003.04265-2020] [PMID] [PMCID]
- Motiejunaite J, Balagny P, Arnoult F, Mangin L, Bancal C, d'Ortho MP, et al. Hyperventilation: A possible explanation for long-lasting exercise intolerance in mild COVID-19 survivors? Frontiers in Physiology. 2021; 11:614590. [DOI:10.3389/fphys.2020.614590] [PMID] [PMCID]
- Frota AX, Vieira MC, Soares CCS, da Silva PS, da Silva GMS, Mendes F de SNS, et al. Functional capacity and rehabilitation strategies in COVID-19 patients: Current knowledge and challenges. Revista da Sociedade Brasileira de Medicina Tropical. 2021; 54:e07892020. [DOI:10.1590/0037-8682-0789-2020] [PMID] [PMCID]
- Sanchez-Ramirez DC, Normand K, Zhaoyun Y, Torres-Castro R. Long-term impact of COVID-19: A systematic review of the literature and meta-analysis. Biomedicines. 2021; 9(8):900. [DOI:10.3390/biomedicines9080900] [PMID] [PMCID]
- Rinaldo RF, Mondoni M, Parazzini EM, Pitari F, Brambilla E, Luraschi S, et al. Deconditioning as main mechanism of impaired exercise response in COVID-19 survivors. The European Respiratory Journal. 2021; 58(2):2100870. [DOI:10.1183/13993003.00870-2021] [PMID] [PMCID]
- McCoy J, Bates M, Eggett C, Siervo M, Cassidy S, Newman J, et al. Pathophysiology of exercise intolerance in chronic diseases: the role of diminished cardiac performance in mitochondrial and heart failure patients. Open Heart. 2017; 4(2):e000632. [DOI:10.1136/openhrt-2017-000632] [PMID] [PMCID]
- Gloeckl R, Leitl D, Jarosch I, Schneeberger T, Nell C, Stenzel N, et al. Benefits of pulmonary rehabilitation in COVID-19: A prospective observational cohort study. ERJ Open Research. 2021; 7(2):00108-2021. [DOI:10.1183/23120541.00108-2021] [PMID] [PMCID]
- Mohamed AA, Alawna M. Role of increasing the aerobic capacity on improving the function of immune and respiratory systems in patients with coronavirus (COVID-19): A review. Diabetes & Metabolic Syndrome. 2020; 14(4):489-96. [DOI:10.1016/j.dsx.2020.04.038] [PMID] [PMCID]
- Calabrese M, Garofano M, Palumbo R, Di Pietro P, Izzo C, Damato A, et al. Exercise training and cardiac rehabilitation in COVID-19 patients with cardiovascular complications: State of art. Life. 2021; 11(3):259. [DOI:10.3390/life11030259] [PMID] [PMCID]
- Hermann M, Pekacka-Egli AM, Witassek F, Baumgaertner R, Schoendorf S, Spielmanns M. Feasibility and efficacy of cardiopulmonary rehabilitation after COVID-19. American journal of Physical Medicine & Rehabilitation. 2020; 99(10):865-9. [DOI:10.1097/PHM.0000000000001549] [PMID] [PMCID]
- Ramalingam MB, Huang Y, Lim PAC. Rehabilitation of a post-intensive care unit patient after severe COVID-19 pneumonia. American Journal of Physical Medicine & Rehabilitation. 2020; 99(12):1092-5. [DOI:10.1097/PHM.0000000000001606] [PMID]
- Spielmanns M, Pekacka-Egli AM, Schoendorf S, Windisch W, Hermann M. Effects of a comprehensive pulmonary rehabilitation in severe post-COVID-19 patients. International Journal of Environmental Research and Public Health. 2021; 18(5):2695. [DOI:10.3390/ijerph18052695] [PMID] [PMCID]
- Puchner B, Sahanic S, Kirchmair R, Pizzini A, Sonnweber B, Wöll E, et al. Beneficial effects of multi-disciplinary rehabilitation in postacute COVID-19: An observational cohort study. European Journal of Physical and Rehabilitation Medicined. 2021; 57(2):189-98. [DOI:10.23736/S1973-9087.21.06549-7] [PMID]
- Solon K, Larson A, Ronnebaum J, Stevermer C. Rehabilitation outcomes for patients with severe presentation of COVID-19: A case series. Journal of Acute Care Physical Therapy. 2021; 12(3):115-21. [DOI:10.1097/JAT.0000000000000153] [PMID] [PMCID]
- Betschart M, Rezek S, Unger I, Beyer S, Gisi D, Shannon H, et al. Feasibility of an outpatient training program after COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(8):3978. [DOI:10.3390/ijerph18083978] [PMID] [PMCID]
- Büsching G, Zhang Z, Schmid JP, Sigrist T, Khatami R. Effectiveness of pulmonary rehabilitation in severe and critically Ill COVID-19 patients: A controlled study. International Journal of Environmental Research and Public Health. 2021; 18(17):8956. [DOI:10.3390/ijerph18178956] [PMID] [PMCID]
- Wasilewski MB, Cimino SR, Kokorelias KM, Simpson R, Hitzig SL, Robinson L. Providing rehabilitation to patients recovering from COVID-19: A scoping review. PM R. 2022; 14(2):239-58. [DOI:10.1002/pmrj.12669] [PMID] [PMCID]
- Gentil P, de Lira CAB, Coswig V, Barroso WKS, Vitorino PVO, Ramirez-Campillo R, et al. Practical recommendations relevant to the use of resistance training for COVID-19 survivors. Frontiers in Physiology. 2021; 12:637590. [DOI:10.3389/fphys.2021.637590] [PMID] [PMCID]
- Agostini F, Mangone M, Ruiu P, Paolucci T, Santilli V, Bernetti A. Rehabilitation setting during and after Covid-19: An overview on recommendations. Journal of Rehabilitation Medicine. 2021; 53(1):jrm00141. [DOI:10.2340/16501977-2776] [PMID] [PMCID]
- Santana AV, Fontana AD, Pitta F. [Pulmonary rehabilitation after COVID-19 (English, Portuguese)]. Jornal Brasileiro de pneumologia. 2021; 47(1):e20210034. [DOI:10.36416/1806-3756/e20210034] [PMID] [PMCID]
- Korupolu R, Francisco GE, Levin H, Needham DM. Rehabilitation of critically Ill COVID-19 survivors. The Journal of the International Society of Physical and Rehabilitation Medicine. 2020; 3(2):45. [DOI:10.4103/jisprm.jisprm_8_20]
Article type: Reviews |
Subject:
Physical Medicine and Rehabilitation
Received: 2022/03/14 | Accepted: 2023/10/11 | Published: 2024/03/1
Received: 2022/03/14 | Accepted: 2023/10/11 | Published: 2024/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
