
988368
Wed, May 27, 2026

Volume 21, Issue 1 (March 2023)
Iranian Rehabilitation Journal 2023, 21(1): 1-16 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mousavi Baigi S F, Sarbaz M, Sobhani-Rad D, Kimiafar K. A Comparative Study of Rehabilitation Information Systems in 8 Countries: A Literature Review. Iranian Rehabilitation Journal 2023; 21 (1) :1-16
URL: http://irj.uswr.ac.ir/article-1-1634-en.html
URL: http://irj.uswr.ac.ir/article-1-1634-en.html



1- Department of Health Information Technology, School of Paramedical Sciences, Mashhad University of Medical Sciences, Mashhad, Iran.; Student Research Committee, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Department of Health Information Technology, School of Paramedical Sciences, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Speech Pathology, School of Paramedical Sciences, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Department of Health Information Technology, School of Paramedical Sciences, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Speech Pathology, School of Paramedical Sciences, Mashhad University of Medical Sciences, Mashhad, Iran.
Full-Text [PDF 776 kb]
(1938 Downloads)
| Abstract (HTML) (4784 Views)
Full-Text: (4331 Views)
1. Introduction
Following the upward trend of aging and the number of chronic and persistent diseases during recent decades, the need for rehabilitation services has increased in all countries, especially underdeveloped and low-income countries [1, 2, 3]. According to the World Health Organization (WHO), 2.41 billion people needed rehabilitation services around the globe in 2019, implying that one out of three persons during a period of illness or injury requires such services [1]. Since 1990, this figure has increased, indicating the aging phenomenon in the concerned population. Moreover, evidence suggests that, because of the severity of the COVID-19 disease or the hospitalization period following its acute phase, many individuals affected by this virus experience long-term complications. Hence, demand for rehabilitation services worldwide has increased [1, 2, 4], while such a need has not been remarkably met. Above 50% of individuals in some low- and middle-income countries receive no rehabilitation services. Moreover, the provision of such services is disrupted in 60%-70% of countries because of the existing COVID-19 pandemic [5, 6].
From another perspective, since the needs for rehabilitation services significantly vary from one country to another, and the required information varies from one region to another, the outcome is inconsistent and insufficient information. This outcome comes especially true for low- and middle-income countries as they have provided no clear statistics on rehabilitation services [7]. Moreover, extensive planning is crucial due to the long-term complications of disabilities and their high treatment costs, following up on patient care processes, and reviewing existing evidence to detect the best care programs and control diseases. These needs are only met by using health information systems (HIS) [8, 9], which support making decisions in health policy, management, and clinical care by gathering, standardizing, coding, and managing information on health status indices, health determinants, and sanitary systems. Policymakers use such information to detect and address problems with evidence-based solutions and allocate resources effectively. Moreover, the information is also used by planners to develop more efficient services, by managers to monitor and assess services, and by physicians to provide evidence-based care with high quality [1]. Accordingly, HIS plays a critical role in health policy decisions in health policy, management, and clinical care [10]. However, as one of the basic obstacles to reinforcing rehabilitation services worldwide, national HIS often provides no sufficient information on rehabilitation. In this regard, WHO has called for some measures by 2030 to reinforce rehabilitation services worldwide [5].
Although much action is required for such measures, one of the main steps in this call is to upgrade HISs by importing rehabilitation information. Therefore, the present research aimed to conduct a comparative review of rehabilitation information systems available in 8 countries: Canada, the United States, the United Kingdom, Australia, Sweden, Malaysia, Russia, and Iran.
2. Materials and Methods
Overview
This literature review was performed using a systematic search. Methods of the review process and eligibility criteria were determined in advance, and a summary of findings was presented at the Information Technology and Health Promotion of Iran’s fourth annual conference in 2021. This study was approved after review and presentation in the Ethics Committee of Mashhad University of Medical Sciences (ِCode: IR.MUMS.REC.1400.296).
Literature search
A comprehensive overview of published studies with no time limit was conducted by searching for keywords of “information system”, “registries”, “registry”, “minimum data set”, “core data set”, “dataset”, “minimal”, “data set”, and “rehabilitation” in keywords, titles and abstracts of studies in the authoritative databases of Web of Science, Scopus, PubMed, and Embase on November 14, 2021. We also did a Google search engine to find rehabilitation information system websites in each country. Table 1 presents the search strategy separately in each database.
.jpg)
Inclusion criteria
The inclusion criteria for studies were as follows: All English and Persian articles without a time limit on May 2, 2021, articles related to the aim of the review and were developed and implemented in the field of rehabilitation information registration systems or minimum national and international data sets, and the availability of complete text of the studies.
Exclusion criteria
The exclusion criteria included studies that were letters to the editor, conference summaries, and studies that did not aim to design, develop, or implement rehabilitation information systems.
Study selection
A total of 13151 related main articles were extracted for review. In addition, the recovered records were examined in the first 10 pages of the Google search engine. After reviewing the studies and removing duplicate articles (5726 articles), 13151 documents remained and were screened based on their titles and abstracts. At the end of the review, 7105 studies that had nothing to do with the aim of this systematic review and 207 studies that were conference summaries were removed. Then, 113 articles were selected to review their complete text, of which 88 articles were removed, and eventually 25 main articles and 6 websites were selected. Figure 1 shows the steps for searching and including studies using the PRISMA (preferred reporting item for systematic reviews) flowchart.
.jpg)
Data extract
A similar standard checklist was used to extract and compare the findings. The data items in this checklist included reference, country, registry name, established year, founder, scope, standard classification systems (coding system), data elements, and subcategories of data elements of the registry.
3. Results
In this study, a comparative review was performed on rehabilitation information recording systems in different countries. The countries that emerged from the selection process were two EU countries (the UK and Sweden), two North American countries (the US and Canada), two Asian continents (Malaysia and Iran), and Australia and Russia. Finally, we compared rehabilitation information registration systems in each country, and the data are shown in Tables 2 and 3.
.jpg)
.jpg)
Rehabilitation information systems in the United States [11, 12], Australia [13, 14, 15, 16], Sweden [17, 18], Canada [19, 20], the United Kingdom [21, 22, 23], Malaysia [24], Russia [25, 26, 27, 28], and Iran [29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40] are as follows.
The Uniform Data System for Medical Rehabilitation (UDSMR) is a non-profit company affiliated with the University of Buffalo. The company provides a wide range of products and programs allowing rehabilitation service providers to record the severity of patients’ disabilities and medical rehabilitation outcomes consistently. UDSMR products cover the post-acute care needs of rehabilitation providers. This company is a leading company in terms of medical rehabilitation outcomes for more than 30 years. UDSMR possesses the largest independent reservoir of rehabilitation outcomes and Inpatient Rehabilitation Facility Patient Assessment Instrument (IRF-PAI) data obtained from more than 1400 rehabilitation centers worldwide, about 900 of which Inpatient Rehabilitation Facilities (IRFs) are located in the US using reports, accreditation, auditing, training, and consulting services. The company mainly aims to allow healthcare providers and related institutions to record and improve care outcomes, processes, and practices in a uniform manner. Internationally, this non-profit company is known to be leading in performance, appraisal, and research since it possesses the largest medical rehabilitation databases worldwide. Now, the UDSMR dataset, with more than 13 million patient appraisals, contains data from all over the world. UDSMR offers management products and services in accordance with the Centers for Medicare and Medicaid Services (CMS) and the Functional Independence Measure (FIM) principles to service providers during the post-acute care phase. The FIM instrument includes 18 data elements covering 6 areas included (self-management, sphincter control, transfer, movement, communication, and social cognition. It also provides medical rehabilitation outcomes for acute medical rehabilitation, acute care services, long-term skilled nursing facilities/homes (SNF) programs, pediatric hospitals, outpatient rehabilitation services, and community-oriented outpatient treatment services. The composition of such products enables healthcare organizations with authentic tools to assess and monitor patients during the post-acute care process. The products also allow subscribers to record the seriousness of a patient’s disability and the consequences of medical rehabilitation. A common language facilitates the link between disabilities in different disciplines and provides the grounds to compare rehabilitation outcomes. The data collected by FIM are used for different purposes, such as assessing rehabilitation outcomes, detecting the effectiveness and efficiency of care services, managing patients, and performing clinical research [11, 12].
The Australasian Rehabilitation Outcomes Centers (AROC) is a clinical registry providing a national standard system to promote clinical rehabilitation outcomes. Under the supervision of the Center for Health Services Development (CHSD) University of Wollongong (UoW), this institute is a joint Australian rehabilitation initiative among providers, investors, regulators, and consumers, which was founded on July 1, 2002, by the Australasian Faculty of Rehabilitation Medicine (AFRM) and the Royal Australasian College of Physicians (RACP). The objectives of the AROC are as follows: Improving clinical rehabilitation consequences in both public and private areas, documenting the effectiveness of interventions by gathering systematic outcome information on inpatient and outpatient programs, reporting clinical and managerial information on performance outcomes, high-risk groups, and other relevant variables meeting providers, payers, consumers, and other stakeholders’ needs in public and private rehabilitation areas, offering and making coordination for training FIM and issuing certificates and other performance measures, providing annual reports summarizing Australian data, and developing research to make modifications in adopted measures over time [13].
The clinical AROC datasets have been developed over years by consulting rehabilitation service providers and the representatives of different organizations from Australia and New Zealand. Furthermore, in some possible cases, the dataset also uses the definitions provided by the national culture of health data [14]. After reviewing and updating different AROC versions, its last version was developed in July 2012. This version encompasses a bank of items addressing different rehabilitation care sections [15]. The collected and recorded information in this registry addresses patients’ ID information (i.e. patient code, first name, last name, date of birth, and gender), facilities, the first and the last date of care processes, AROC disability code, referral data, clinical information, and treatment information for inpatient, outpatient, and pediatric rehabilitation [16].
The Swedish Register for Rehabilitation Medicine (SRRM) was formerly known as WebRehab Sweden and was renamed in November 2021 regarding the information technology platform (available from https://svereh.registercentrum.se/om-registret/om-registret/). This registry aims at ensuring rehabilitation quality for individuals with acquired brain injuries, spinal cord injuries, or other complicated difficulties. It also encompasses both inpatient and outpatient rehabilitation operations. Inpatient rehabilitation also contains both acute and subacute rehabilitation. Some units also provide planned rehabilitation which may aim to evaluate or promote and maintain individuals’ abilities. Patients and their companions should reorient to reach rehabilitation achievements, and this often requires short- or long-term professional support. Rehabilitation content is developed for each person considering his diagnosis, function, lifestyle, and tendencies. The Swedish Association of Rehabilitation Medicine (SFRM) mainly aims to improve quality as such questionnaires contain some information, including patients’ social security code, diagnosis, waiting time, care time, rehabilitation effects, complications, if any, and responses. Such data are collected for general goals. The data in this register can be organized per the International Classification of Functioning, Disability, and health (ICF) domains. In Sweden, strong authentication is required when accessing personal information through open networks. This problem is addressed by an electronic-card (e-card) service that provides physical and electronic identification for each individual and is implemented in WebRehab [17, 18].
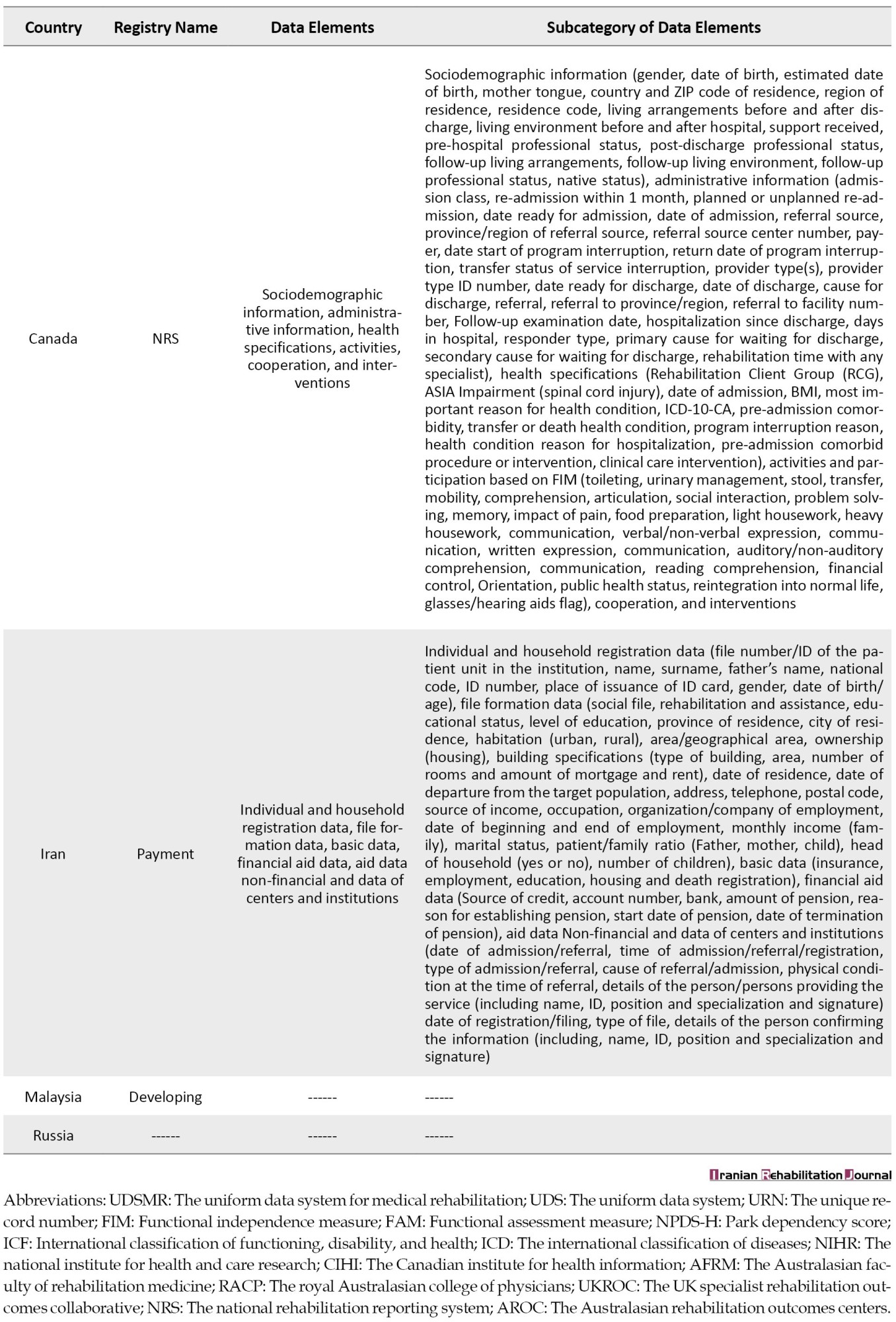
The National Rehabilitation Reporting System (NRS) is a part of about 40 roadmaps established in 1999 at the Canadian Institute for Health Information (CIHI), an independent non-profit organization providing information and basic analysis of necessary data and information on Canada’s health system and the health of Canadians. The National Rehabilitation Reporting System (NRS) was launched to develop national indices and report adult inpatient rehabilitation services, resulting in the implementation of the rehabilitation reporting system prototype. Further, an expert group was formed to guide CIHI in this regard. The group collects data from participants and adult patients undergoing rehabilitation programs in 9 provinces across Canada. NRS encompasses specialized facilities, hospital rehabilitation units, hospital rehabilitation services, and rehabilitation beds. The NRS rehabilitation minimum data set (MDS) manual assesses clinical data on functional status (based on the 18-item FIM) and additional data elements (i.e. cognitive function and Instrumental activities of daily living [IADL]). This registry contains a wide range of information, including socio-demographic information, administrative information, health specifications, activities, cooperation, and interventions) [19, 20].
The UK Specialist Rehabilitation Outcomes Collaborative (UKROC) is a national clinical database established in September 2008. It was funded by the Ministry of Health and Medical Education and typically gathers key information about each patient admitted to a specialized rehabilitation unit in the UK. During its first five years, UKROC focused on neurological rehabilitation, and it now contains information on all level 1 and 2 specialist neuro-rehabilitation services across the UK. The collected and recorded data elements in this database are as follows: NHS No. (a specific number for each patient), gender, age, ethnicity, date of birth, place of residence, references to service, waiting time for acceptance; some information on health status (e.g. primary diagnosis, time of onset, etc.), disease complications (e.g. paralysis, pain, and limitations in daily activities), care provided by nursing and medical staff, changes during the program (e.g. changes in mobility, self-care, communication with others, etc.), post-discharge place (e.g. transfer to another hospital, home, residential care centers, etc.) [21, 22, 23].
The rehabilitation information registration system in Malaysia is still in its infancy due to the lack of information sharing and concatenation. Cloud computing can be more compatible with establishing a virtual centralized rehabilitation registry. On-site rehabilitation registration systems may not apply well in Malaysia since this country is divided into two main areas (namely the Malay Peninsula and Borneo) as such Sabah is developing a virtual data warehouse to record rehabilitation in the latter region. Ahmedy et al. also implemented a virtual data warehouse to integrate the incongruity of data warehouses from multiple inpatient rehabilitation centers across the country. It was consequently expanded to assist big data analysis and interpretation visualization using a geographical mapping feature [24].
The rehabilitation information registration systems in Russia are implemented only in sub-disciplines such as the stroke registration system [25], heart rehabilitation [26], occupational diseases [27], and others. A review of previous studies revealed that Russia generally has no history of rehabilitation data for individuals with disabilities, and the only information is sent partially. Moreover, no organized flow of operational information exists between the executors of different sections of the rehabilitation process. Although there is some information on the main flows of different organizations and institutions’ operations as statistical reports in the form of articles, they are not cited to support the rehabilitation process. An organization, for example, helps individuals with severe disabilities across the city. However, there is no summarized information on disabled individuals’ functional impairment combined with real social conditions. Accordingly, many citizens who need immediate or consistent social assistance are disregarded [26, 28].
In Iran, the identification and determination of disability is the responsibility of the Welfare Organization. Thus, the Welfare Organization forms a commission to diagnose and classify the types of disabilities based on international standards and determine the disability ID, which is responsible for diagnosing and determining the severity of disability in accordance with the ICF [29, 30]. The purpose of determining the severity of the disability is the result of the degree of damage in anatomy or physiology and limitations in the daily functioning of life. Medical documents on the diagnosis of disorders and diseases leading to disability before recording in the file of the disabled person should be reviewed by physicians in the commission and its physical and psychological consequences should be identified by a group of rehabilitation specialists [31]. After determining the type and seriousness of disability in the medical commission, if the disability was approved by the commission, a case would be filed for him or her in the Welfare Organization. Depending on the type and seriousness of the disability, the Organization provides a range of support services to the disabled. But in general, these services can be divided into two general groups: Rehabilitation services and financial aid. Rehabilitation services include physiotherapy, speech therapy, occupational therapy, psychotherapy, optometry, nursing care, and even funded disability coverage for surgery. The Welfare Organization provides these services through physiotherapy, speech therapy, occupational therapy, psychiatry, optometry, technical orthopedics and prosthesis manufacturing, rehabilitation, and daycare centers affiliated with the organization or the contracting party, providing services at home and transferring files to non-governmental centers. Currently, there are 25 rehabilitation and care centers for the mentally disabled, 7 rehabilitation and care centers for the elderly, 7 treatment and rehabilitation centers for the chronically mentally ill, and 2 rehabilitation and maintenance centers for the physically disabled under the supervision of the Welfare Organization. Since 2014, this organization has used an integrated system to register the information of the disabled throughout the country. This system is known as the “database of the Welfare Organization or payment system”. This system is subordinate and registers identity, socio-economic information, type and extent of disability, and support services received. In the payment system, client data are registered in six groups: Individual and household registration data, file formation data (social file, rehabilitation, and assistance), basic data (insurance, employment, education, housing, and death registration), financial aid data, aid data Non-financial and data of centers and institutions. It was also possible to report based on the registered data elements in this system [30]. For the authorized users of this system, it is available from the internet address https://payment.behzisti.net.
There are also some studies on rehabilitation MDS in sub-disciplines, including audiology [32], physiotherapy [33], orthopedics [34], occupational therapy [35], speech therapy [36], post-trauma rehabilitation [37], cerebral palsy rehabilitation, and schizophrenia patients’ rehabilitation [38], to be developed in Iran. Furthermore, in a study aimed at developing and implementing a national disability MDS in Iran. Ahmadi et al. concluded that MDS can be a start to standardize disability data. Providing consistent, complete, and uniform data elements, MDSs are potentially used to standardize data and conquer the problems posed by low-quality disability data in Iran. Accordingly, MDS can contribute to specifying disability levels and is more cost effective and efficient in making appropriate policies and plans for individuals with disabilities. National MDS for disability information management system encompasses 475 information elements, including a management category with 130 information elements and a clinical category with 345 information elements [39].
4. Discussion
According to the WHO in 2019, 2.41 billion people around the globe need rehabilitation services [1]. Thus, registration of rehabilitation information is crucial to achieving the best evidence and planning. The present research aimed to comparatively review the rehabilitation information systems available in 8 countries: Canada, the United States, the United Kingdom, Australia, Sweden, Malaysia, Russia, and Iran.
A review of the literature revealed that rehabilitation information systems in the United States [11, 12], Australia [16], and Sweden [17, 18] contain outpatient and inpatient rehabilitation. However, investigations in Canada have considered only adult inpatient rehabilitation information [19, 16], and specialized rehabilitation services are just recorded and reviewed in the UK [21, 22, 23]. In Iran, the Welfare Organization registers and collects (inpatient, outpatient, and home care) rehabilitation and financial data of the disabled with the “payment” system [30]. Regional rehabilitation information systems in Malaysia do not meet the national rehabilitation needs as such a virtual data warehouse that is being developed to record rehabilitation information [24]. In Russia, however, studies have just proposed establishing rehabilitation information registration systems, and no comprehensive national system has been proposed for the registration of rehabilitation services yet [26, 39].
No country has used rehabilitation information registration systems consistent with its national health information registration system (HIRS). A large number of studies on registries and MDSs have been conducted in Iran over recent years, most of which have also provided a native model for the MDS development for a disease, injury, or group of patients [33, 34, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49]. This is, while no study has addressed the development of rehabilitation MDS or registries. Some studies, however, have proposed that rehabilitation MDS in sub-disciplines such as audiology [32], physiotherapy [33], orthopedics [34], occupational therapy [35], speech therapy [36], post-trauma rehabilitation [37], cerebral palsy rehabilitation and schizophrenia patients’ rehabilitation [38], be developed in Iran. Such data sets and the Welfare Organization in Iran are not comprehensive enough because of the wide range of rehabilitation and different needs of supporting organizations involved in this issue, including the Ministry of Health and Medical Education and other centers. Furthermore, the disability data sets proposed and the Payment registry in Iran only aimed to manage information on disabled individuals and do not match other large populations requiring rehabilitation services [30, 39]. In Russia with one of the highest social budgets, however, no organization exists for the rehabilitation of disabled individuals because of financial constraints and the lack of information on rehabilitation opportunities [28].
Although Australia [16], the UK [21, 22, 23], and Sweden [17, 18] only have registries for clinical purposes, in the United States, the UDSMR, covers not only clinical purposes but also reporting, accreditation, auditing, training, and consulting services [11, 12]. In Iran, although the Welfare Organization is a national system, it provides both clinical and administrative registry purposes (financial and non-financial purposes) and according to the comprehensive protection law for the disabled, the Welfare Organization is the main custodian of identifying, reducing, and supporting the disabled [29, 30, 31]. In addition, the NRS collects detailed information on socio-demographic data, administrative data, health features, activities, partnerships, and interventions aimed at improving the health of Canada and Canadians [19, 20].
In this study, we found that the UKROC registry encodes diagnoses based on ICD 10 codes [21], the NRS registry based on ICD-10-CA codes [19], the WebRehab registry based on ICF [17], the AROC registry based on AROC impairment [13], the UDSMR registry based on UDS impairment [11], and the payment registry based on ICF [30]. From this perspective, the WebRehab and payment registries are the most compatible with WHO guidelines for coding functioning, disability, and health in people with disabilities. The finding of our literature review is similar to the study of Safdari et al. Their study examined standard classification systems on various rehabilitation-related topics, including the etiology of disability (international classification of diseases-10 [ICD-10]) and the international classification of diseases, the ninth revision, clinical modification (ICD-9-CM); disability diagnosis (ICF); measures (ICD-10 procedure coding system (ICD-10-PCS), International classification of procedures in medicine (ICPM)); refund (functional related group [FRG]); and functional status (FIM) [50].
In a similar vein, McPherson et al. aimed to illustrate the status of rehabilitation HISs in countries with different income levels and detect the main processes and measures to develop such systems in underdeveloped and low-income countries. In their study, they found out that no standard exists for rehabilitation in HISs. However, it is generally believed that valid data on the prevalence of disability, the economic situation, access to rehabilitation services, and practical outcomes of rehabilitation are required to plan for promoting health among individuals with disabilities. This finding implies that planning for disability and rehabilitation can be initiated by developing MDSs and then gradually leads to the system’s improvement and coordination [49].
In a comparative study entitled “Analytical comparison of rehabilitation programs for the disabled in Iran with other countries”, Irvani et al. documented that the integration of parallel organizations’ rehabilitation sectors in the Ministry of Health and Medical Education in Iran, not only enhances intersectoral coordination and the consistency of united management and policy-making but also decreases costs, enhances the proper allocation, and increase the financial resources of this sector. Further, it may decrease the overlap of more desirable service delivery; hence, undertaking responsibilities, preventing repetition, and training specialized personnel regarding the needs are of great importance. Policymakers and planners in this major should adopt a wider perspective to review and modify the structure, regulations, and activities in line with the movement toward formulating a system to equip rehabilitation programs for the disabled in Iran [50].
Commission on Accreditation of Rehabilitation Facilities (CARF) developed a framework to collect the required rehabilitation data by providing a standard model for establishing a management system and evaluating rehabilitation programs. The framework specifies the MDS according to the main rehabilitation components, including input (namely demographic information, health status history, primary diagnosis of disability, etiological injury, time of injury, the acute hospital care center’s functioning, and functional status), process (type of rehabilitation services, frequency of treatment sessions, test results, goals, interventions and measures, progress trend, complications and difficulties, and indicators such as length of stay in inpatient rehabilitation), and output (functional status, complications and difficulties, post-discharge services, and financial support for disabled individuals) [51].
In their study entitled “a review of information management standards of rehabilitation centers accreditation commission”, Safdari et al. aimed to develop a framework for standards required by information management processes in rehabilitation centers. They reported that information management processes ranging from data collection, registration, documentation, organization, and classification to information storage, retrieval, and dissemination in rehabilitation centers should follow the standards concerned by the evaluating organization. However, no consistent and comprehensive standards exist for this purpose at an international level as different institutions active in accrediting and evaluating rehabilitation services of different scopes and detail levels have set some standards in this regard [52].
Ghazi Saeedi et al. in their research entitled “MDS for Schizophrenia Electronic Health Card” concluded that an electronic health card for schizophrenia patients can help the treatment team in providing effective health care and better medical records for inpatient staff. It also reduces the problems of family members and relatives of the patient and simplifies the process of treating schizophrenia. The proposed MDS for schizophrenia includes 29 data elements. They included two general groups of demographic data (basic information, insurance information, and essential contact information) and clinical data (medical history, psychiatric history, and mental status) [38].
Ahmadi et al. in their research entitled “development of the MDS of the health information system of orthopedic injuries in Iran” concluded that some of the necessary data elements that exist in the MDS of other countries or are needed for organizations and health care providers of medical services are not covered in the current systems. Hence, a comprehensive content of MDS should be constructed. The existence of comprehensive and complete data about the causes and mechanisms of traumas informs public health policymakers about the incident of traumas and empowers them to take advisory measures to deal with these difficulties. The MDS of orthopedic injury included two management categories (6 categories and 142 data elements) and clinical categories (17 categories and 250 data elements) [34].
Arastoo et al. standardized the information elements in the audiometric file and provided a suitable model for Iran. This applied descriptive-comparative research was conducted using the Delphi method with the help of 17 faculty members and 110 audiologists. The information elements were introduced in this study in four categories: Demographic information, medical history, patient evaluation, and treatment plan [32].
Furthermore, Damanabi et al. in their research aimed to develop an MDS of speech therapy. They concluded that by designing and implementing appropriate speech therapy data gathering for data collection, and planning for check and debarment of speech disorders, it is necessary to provide high quality and better care to patients in speech therapy centers. The minimal data collection of speech therapy included clinical and administrative levels. The most principal elements of management information include name, last name, birth date, sex, address, phone number, date of admission and number of treatments, patient complaints, duration of impairment or disorder, cause and description of the disease, and the most principal elements of clinical information including health history, short-term goals and the long-term development of speech history [36].
In summary, in some countries, national and international rehabilitation information systems have been implemented and are being used. But still, the main goal of WHO in integrating health care systems with the rehabilitation system has not been achieved in any country. In this regard, WHO has expanded a framework and standards for national HIS and a global reference content of 100 key health values to assist countries to reinforce their HIS. There are opportunities to further expand this framework to accommodate rehabilitation information needs [5].
Undoubtedly, reaching this goal requires cooperation, targeted policies, and huge investment. Therefore, accurate evaluations in terms of cost-effectiveness and identification of challenges and facilitators for the development of rehabilitation information systems are critical [53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65].
5. Conclusion
This literature review demonstrates that the most comprehensive rehabilitation information systems belong to the United States and Australia, which included the sections of inpatient and outpatient rehabilitation for children and adults, then Canada and Sweden, which included the outpatient and inpatient sections. Afterward, the UK included specialist rehabilitation services. This is while a rehabilitation information system was being established in Malaysia. However, in Russia and Iran, only limited studies have been conducted to recommend the implementation of a comprehensive rehabilitation information system. Therefore, the future work of this study is to design and development a comprehensive rehabilitation information system in Iran.
One of the strengths of our study is that it was the first comprehensive review of rehabilitation information registration systems. The findings may contribute to clarifying the current situation in these 8 countries as a representative of the world’s countries. Moreover, in line with the call for planning, WHO should develop a broader view of the developed programs to direct policy-makers toward developing rehabilitation information registration systems.
Since the present study aimed to include comprehensive rehabilitation systems, one of the limitations of this study is disregarding rehabilitation registration systems in smaller disciplines, including pulmonary, heart, and stroke rehabilitation registration systems, and so on. On the other hand, the search keywords may not be adequate and perfect to pick more studies, and some significant and relevant research may have been missed in this review. According to the recommendations of WHO to integrate hospital information systems with the rehabilitation information system and given the current situation, there is no integrated system in accordance with the recommendations of WHO. Future studies are recommended to develop rehabilitation registration systems integrated with national HIRSs.
Ethical Considerations
Compliance with ethical guidelines
This study was approved after review and presentation in the Ethics Committee of Mashhad University of Medical Sciences (Code: IR.MUMS.REC.1400.296).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We hereby express our gratitude to the Student Research Committee of Mashhad University of Medical Sciences who helped us in conducting this research.
References
Following the upward trend of aging and the number of chronic and persistent diseases during recent decades, the need for rehabilitation services has increased in all countries, especially underdeveloped and low-income countries [1, 2, 3]. According to the World Health Organization (WHO), 2.41 billion people needed rehabilitation services around the globe in 2019, implying that one out of three persons during a period of illness or injury requires such services [1]. Since 1990, this figure has increased, indicating the aging phenomenon in the concerned population. Moreover, evidence suggests that, because of the severity of the COVID-19 disease or the hospitalization period following its acute phase, many individuals affected by this virus experience long-term complications. Hence, demand for rehabilitation services worldwide has increased [1, 2, 4], while such a need has not been remarkably met. Above 50% of individuals in some low- and middle-income countries receive no rehabilitation services. Moreover, the provision of such services is disrupted in 60%-70% of countries because of the existing COVID-19 pandemic [5, 6].
From another perspective, since the needs for rehabilitation services significantly vary from one country to another, and the required information varies from one region to another, the outcome is inconsistent and insufficient information. This outcome comes especially true for low- and middle-income countries as they have provided no clear statistics on rehabilitation services [7]. Moreover, extensive planning is crucial due to the long-term complications of disabilities and their high treatment costs, following up on patient care processes, and reviewing existing evidence to detect the best care programs and control diseases. These needs are only met by using health information systems (HIS) [8, 9], which support making decisions in health policy, management, and clinical care by gathering, standardizing, coding, and managing information on health status indices, health determinants, and sanitary systems. Policymakers use such information to detect and address problems with evidence-based solutions and allocate resources effectively. Moreover, the information is also used by planners to develop more efficient services, by managers to monitor and assess services, and by physicians to provide evidence-based care with high quality [1]. Accordingly, HIS plays a critical role in health policy decisions in health policy, management, and clinical care [10]. However, as one of the basic obstacles to reinforcing rehabilitation services worldwide, national HIS often provides no sufficient information on rehabilitation. In this regard, WHO has called for some measures by 2030 to reinforce rehabilitation services worldwide [5].
Although much action is required for such measures, one of the main steps in this call is to upgrade HISs by importing rehabilitation information. Therefore, the present research aimed to conduct a comparative review of rehabilitation information systems available in 8 countries: Canada, the United States, the United Kingdom, Australia, Sweden, Malaysia, Russia, and Iran.
2. Materials and Methods
Overview
This literature review was performed using a systematic search. Methods of the review process and eligibility criteria were determined in advance, and a summary of findings was presented at the Information Technology and Health Promotion of Iran’s fourth annual conference in 2021. This study was approved after review and presentation in the Ethics Committee of Mashhad University of Medical Sciences (ِCode: IR.MUMS.REC.1400.296).
Literature search
A comprehensive overview of published studies with no time limit was conducted by searching for keywords of “information system”, “registries”, “registry”, “minimum data set”, “core data set”, “dataset”, “minimal”, “data set”, and “rehabilitation” in keywords, titles and abstracts of studies in the authoritative databases of Web of Science, Scopus, PubMed, and Embase on November 14, 2021. We also did a Google search engine to find rehabilitation information system websites in each country. Table 1 presents the search strategy separately in each database.
Inclusion criteria
The inclusion criteria for studies were as follows: All English and Persian articles without a time limit on May 2, 2021, articles related to the aim of the review and were developed and implemented in the field of rehabilitation information registration systems or minimum national and international data sets, and the availability of complete text of the studies.
Exclusion criteria
The exclusion criteria included studies that were letters to the editor, conference summaries, and studies that did not aim to design, develop, or implement rehabilitation information systems.
Study selection
A total of 13151 related main articles were extracted for review. In addition, the recovered records were examined in the first 10 pages of the Google search engine. After reviewing the studies and removing duplicate articles (5726 articles), 13151 documents remained and were screened based on their titles and abstracts. At the end of the review, 7105 studies that had nothing to do with the aim of this systematic review and 207 studies that were conference summaries were removed. Then, 113 articles were selected to review their complete text, of which 88 articles were removed, and eventually 25 main articles and 6 websites were selected. Figure 1 shows the steps for searching and including studies using the PRISMA (preferred reporting item for systematic reviews) flowchart.
Data extract
A similar standard checklist was used to extract and compare the findings. The data items in this checklist included reference, country, registry name, established year, founder, scope, standard classification systems (coding system), data elements, and subcategories of data elements of the registry.
3. Results
In this study, a comparative review was performed on rehabilitation information recording systems in different countries. The countries that emerged from the selection process were two EU countries (the UK and Sweden), two North American countries (the US and Canada), two Asian continents (Malaysia and Iran), and Australia and Russia. Finally, we compared rehabilitation information registration systems in each country, and the data are shown in Tables 2 and 3.
Rehabilitation information systems in the United States [11, 12], Australia [13, 14, 15, 16], Sweden [17, 18], Canada [19, 20], the United Kingdom [21, 22, 23], Malaysia [24], Russia [25, 26, 27, 28], and Iran [29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40] are as follows.
The Uniform Data System for Medical Rehabilitation (UDSMR) is a non-profit company affiliated with the University of Buffalo. The company provides a wide range of products and programs allowing rehabilitation service providers to record the severity of patients’ disabilities and medical rehabilitation outcomes consistently. UDSMR products cover the post-acute care needs of rehabilitation providers. This company is a leading company in terms of medical rehabilitation outcomes for more than 30 years. UDSMR possesses the largest independent reservoir of rehabilitation outcomes and Inpatient Rehabilitation Facility Patient Assessment Instrument (IRF-PAI) data obtained from more than 1400 rehabilitation centers worldwide, about 900 of which Inpatient Rehabilitation Facilities (IRFs) are located in the US using reports, accreditation, auditing, training, and consulting services. The company mainly aims to allow healthcare providers and related institutions to record and improve care outcomes, processes, and practices in a uniform manner. Internationally, this non-profit company is known to be leading in performance, appraisal, and research since it possesses the largest medical rehabilitation databases worldwide. Now, the UDSMR dataset, with more than 13 million patient appraisals, contains data from all over the world. UDSMR offers management products and services in accordance with the Centers for Medicare and Medicaid Services (CMS) and the Functional Independence Measure (FIM) principles to service providers during the post-acute care phase. The FIM instrument includes 18 data elements covering 6 areas included (self-management, sphincter control, transfer, movement, communication, and social cognition. It also provides medical rehabilitation outcomes for acute medical rehabilitation, acute care services, long-term skilled nursing facilities/homes (SNF) programs, pediatric hospitals, outpatient rehabilitation services, and community-oriented outpatient treatment services. The composition of such products enables healthcare organizations with authentic tools to assess and monitor patients during the post-acute care process. The products also allow subscribers to record the seriousness of a patient’s disability and the consequences of medical rehabilitation. A common language facilitates the link between disabilities in different disciplines and provides the grounds to compare rehabilitation outcomes. The data collected by FIM are used for different purposes, such as assessing rehabilitation outcomes, detecting the effectiveness and efficiency of care services, managing patients, and performing clinical research [11, 12].
The Australasian Rehabilitation Outcomes Centers (AROC) is a clinical registry providing a national standard system to promote clinical rehabilitation outcomes. Under the supervision of the Center for Health Services Development (CHSD) University of Wollongong (UoW), this institute is a joint Australian rehabilitation initiative among providers, investors, regulators, and consumers, which was founded on July 1, 2002, by the Australasian Faculty of Rehabilitation Medicine (AFRM) and the Royal Australasian College of Physicians (RACP). The objectives of the AROC are as follows: Improving clinical rehabilitation consequences in both public and private areas, documenting the effectiveness of interventions by gathering systematic outcome information on inpatient and outpatient programs, reporting clinical and managerial information on performance outcomes, high-risk groups, and other relevant variables meeting providers, payers, consumers, and other stakeholders’ needs in public and private rehabilitation areas, offering and making coordination for training FIM and issuing certificates and other performance measures, providing annual reports summarizing Australian data, and developing research to make modifications in adopted measures over time [13].
The clinical AROC datasets have been developed over years by consulting rehabilitation service providers and the representatives of different organizations from Australia and New Zealand. Furthermore, in some possible cases, the dataset also uses the definitions provided by the national culture of health data [14]. After reviewing and updating different AROC versions, its last version was developed in July 2012. This version encompasses a bank of items addressing different rehabilitation care sections [15]. The collected and recorded information in this registry addresses patients’ ID information (i.e. patient code, first name, last name, date of birth, and gender), facilities, the first and the last date of care processes, AROC disability code, referral data, clinical information, and treatment information for inpatient, outpatient, and pediatric rehabilitation [16].
The Swedish Register for Rehabilitation Medicine (SRRM) was formerly known as WebRehab Sweden and was renamed in November 2021 regarding the information technology platform (available from https://svereh.registercentrum.se/om-registret/om-registret/). This registry aims at ensuring rehabilitation quality for individuals with acquired brain injuries, spinal cord injuries, or other complicated difficulties. It also encompasses both inpatient and outpatient rehabilitation operations. Inpatient rehabilitation also contains both acute and subacute rehabilitation. Some units also provide planned rehabilitation which may aim to evaluate or promote and maintain individuals’ abilities. Patients and their companions should reorient to reach rehabilitation achievements, and this often requires short- or long-term professional support. Rehabilitation content is developed for each person considering his diagnosis, function, lifestyle, and tendencies. The Swedish Association of Rehabilitation Medicine (SFRM) mainly aims to improve quality as such questionnaires contain some information, including patients’ social security code, diagnosis, waiting time, care time, rehabilitation effects, complications, if any, and responses. Such data are collected for general goals. The data in this register can be organized per the International Classification of Functioning, Disability, and health (ICF) domains. In Sweden, strong authentication is required when accessing personal information through open networks. This problem is addressed by an electronic-card (e-card) service that provides physical and electronic identification for each individual and is implemented in WebRehab [17, 18].
The National Rehabilitation Reporting System (NRS) is a part of about 40 roadmaps established in 1999 at the Canadian Institute for Health Information (CIHI), an independent non-profit organization providing information and basic analysis of necessary data and information on Canada’s health system and the health of Canadians. The National Rehabilitation Reporting System (NRS) was launched to develop national indices and report adult inpatient rehabilitation services, resulting in the implementation of the rehabilitation reporting system prototype. Further, an expert group was formed to guide CIHI in this regard. The group collects data from participants and adult patients undergoing rehabilitation programs in 9 provinces across Canada. NRS encompasses specialized facilities, hospital rehabilitation units, hospital rehabilitation services, and rehabilitation beds. The NRS rehabilitation minimum data set (MDS) manual assesses clinical data on functional status (based on the 18-item FIM) and additional data elements (i.e. cognitive function and Instrumental activities of daily living [IADL]). This registry contains a wide range of information, including socio-demographic information, administrative information, health specifications, activities, cooperation, and interventions) [19, 20].
The UK Specialist Rehabilitation Outcomes Collaborative (UKROC) is a national clinical database established in September 2008. It was funded by the Ministry of Health and Medical Education and typically gathers key information about each patient admitted to a specialized rehabilitation unit in the UK. During its first five years, UKROC focused on neurological rehabilitation, and it now contains information on all level 1 and 2 specialist neuro-rehabilitation services across the UK. The collected and recorded data elements in this database are as follows: NHS No. (a specific number for each patient), gender, age, ethnicity, date of birth, place of residence, references to service, waiting time for acceptance; some information on health status (e.g. primary diagnosis, time of onset, etc.), disease complications (e.g. paralysis, pain, and limitations in daily activities), care provided by nursing and medical staff, changes during the program (e.g. changes in mobility, self-care, communication with others, etc.), post-discharge place (e.g. transfer to another hospital, home, residential care centers, etc.) [21, 22, 23].
The rehabilitation information registration system in Malaysia is still in its infancy due to the lack of information sharing and concatenation. Cloud computing can be more compatible with establishing a virtual centralized rehabilitation registry. On-site rehabilitation registration systems may not apply well in Malaysia since this country is divided into two main areas (namely the Malay Peninsula and Borneo) as such Sabah is developing a virtual data warehouse to record rehabilitation in the latter region. Ahmedy et al. also implemented a virtual data warehouse to integrate the incongruity of data warehouses from multiple inpatient rehabilitation centers across the country. It was consequently expanded to assist big data analysis and interpretation visualization using a geographical mapping feature [24].
The rehabilitation information registration systems in Russia are implemented only in sub-disciplines such as the stroke registration system [25], heart rehabilitation [26], occupational diseases [27], and others. A review of previous studies revealed that Russia generally has no history of rehabilitation data for individuals with disabilities, and the only information is sent partially. Moreover, no organized flow of operational information exists between the executors of different sections of the rehabilitation process. Although there is some information on the main flows of different organizations and institutions’ operations as statistical reports in the form of articles, they are not cited to support the rehabilitation process. An organization, for example, helps individuals with severe disabilities across the city. However, there is no summarized information on disabled individuals’ functional impairment combined with real social conditions. Accordingly, many citizens who need immediate or consistent social assistance are disregarded [26, 28].
In Iran, the identification and determination of disability is the responsibility of the Welfare Organization. Thus, the Welfare Organization forms a commission to diagnose and classify the types of disabilities based on international standards and determine the disability ID, which is responsible for diagnosing and determining the severity of disability in accordance with the ICF [29, 30]. The purpose of determining the severity of the disability is the result of the degree of damage in anatomy or physiology and limitations in the daily functioning of life. Medical documents on the diagnosis of disorders and diseases leading to disability before recording in the file of the disabled person should be reviewed by physicians in the commission and its physical and psychological consequences should be identified by a group of rehabilitation specialists [31]. After determining the type and seriousness of disability in the medical commission, if the disability was approved by the commission, a case would be filed for him or her in the Welfare Organization. Depending on the type and seriousness of the disability, the Organization provides a range of support services to the disabled. But in general, these services can be divided into two general groups: Rehabilitation services and financial aid. Rehabilitation services include physiotherapy, speech therapy, occupational therapy, psychotherapy, optometry, nursing care, and even funded disability coverage for surgery. The Welfare Organization provides these services through physiotherapy, speech therapy, occupational therapy, psychiatry, optometry, technical orthopedics and prosthesis manufacturing, rehabilitation, and daycare centers affiliated with the organization or the contracting party, providing services at home and transferring files to non-governmental centers. Currently, there are 25 rehabilitation and care centers for the mentally disabled, 7 rehabilitation and care centers for the elderly, 7 treatment and rehabilitation centers for the chronically mentally ill, and 2 rehabilitation and maintenance centers for the physically disabled under the supervision of the Welfare Organization. Since 2014, this organization has used an integrated system to register the information of the disabled throughout the country. This system is known as the “database of the Welfare Organization or payment system”. This system is subordinate and registers identity, socio-economic information, type and extent of disability, and support services received. In the payment system, client data are registered in six groups: Individual and household registration data, file formation data (social file, rehabilitation, and assistance), basic data (insurance, employment, education, housing, and death registration), financial aid data, aid data Non-financial and data of centers and institutions. It was also possible to report based on the registered data elements in this system [30]. For the authorized users of this system, it is available from the internet address https://payment.behzisti.net.
There are also some studies on rehabilitation MDS in sub-disciplines, including audiology [32], physiotherapy [33], orthopedics [34], occupational therapy [35], speech therapy [36], post-trauma rehabilitation [37], cerebral palsy rehabilitation, and schizophrenia patients’ rehabilitation [38], to be developed in Iran. Furthermore, in a study aimed at developing and implementing a national disability MDS in Iran. Ahmadi et al. concluded that MDS can be a start to standardize disability data. Providing consistent, complete, and uniform data elements, MDSs are potentially used to standardize data and conquer the problems posed by low-quality disability data in Iran. Accordingly, MDS can contribute to specifying disability levels and is more cost effective and efficient in making appropriate policies and plans for individuals with disabilities. National MDS for disability information management system encompasses 475 information elements, including a management category with 130 information elements and a clinical category with 345 information elements [39].
4. Discussion
According to the WHO in 2019, 2.41 billion people around the globe need rehabilitation services [1]. Thus, registration of rehabilitation information is crucial to achieving the best evidence and planning. The present research aimed to comparatively review the rehabilitation information systems available in 8 countries: Canada, the United States, the United Kingdom, Australia, Sweden, Malaysia, Russia, and Iran.
A review of the literature revealed that rehabilitation information systems in the United States [11, 12], Australia [16], and Sweden [17, 18] contain outpatient and inpatient rehabilitation. However, investigations in Canada have considered only adult inpatient rehabilitation information [19, 16], and specialized rehabilitation services are just recorded and reviewed in the UK [21, 22, 23]. In Iran, the Welfare Organization registers and collects (inpatient, outpatient, and home care) rehabilitation and financial data of the disabled with the “payment” system [30]. Regional rehabilitation information systems in Malaysia do not meet the national rehabilitation needs as such a virtual data warehouse that is being developed to record rehabilitation information [24]. In Russia, however, studies have just proposed establishing rehabilitation information registration systems, and no comprehensive national system has been proposed for the registration of rehabilitation services yet [26, 39].
No country has used rehabilitation information registration systems consistent with its national health information registration system (HIRS). A large number of studies on registries and MDSs have been conducted in Iran over recent years, most of which have also provided a native model for the MDS development for a disease, injury, or group of patients [33, 34, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49]. This is, while no study has addressed the development of rehabilitation MDS or registries. Some studies, however, have proposed that rehabilitation MDS in sub-disciplines such as audiology [32], physiotherapy [33], orthopedics [34], occupational therapy [35], speech therapy [36], post-trauma rehabilitation [37], cerebral palsy rehabilitation and schizophrenia patients’ rehabilitation [38], be developed in Iran. Such data sets and the Welfare Organization in Iran are not comprehensive enough because of the wide range of rehabilitation and different needs of supporting organizations involved in this issue, including the Ministry of Health and Medical Education and other centers. Furthermore, the disability data sets proposed and the Payment registry in Iran only aimed to manage information on disabled individuals and do not match other large populations requiring rehabilitation services [30, 39]. In Russia with one of the highest social budgets, however, no organization exists for the rehabilitation of disabled individuals because of financial constraints and the lack of information on rehabilitation opportunities [28].
Although Australia [16], the UK [21, 22, 23], and Sweden [17, 18] only have registries for clinical purposes, in the United States, the UDSMR, covers not only clinical purposes but also reporting, accreditation, auditing, training, and consulting services [11, 12]. In Iran, although the Welfare Organization is a national system, it provides both clinical and administrative registry purposes (financial and non-financial purposes) and according to the comprehensive protection law for the disabled, the Welfare Organization is the main custodian of identifying, reducing, and supporting the disabled [29, 30, 31]. In addition, the NRS collects detailed information on socio-demographic data, administrative data, health features, activities, partnerships, and interventions aimed at improving the health of Canada and Canadians [19, 20].
In this study, we found that the UKROC registry encodes diagnoses based on ICD 10 codes [21], the NRS registry based on ICD-10-CA codes [19], the WebRehab registry based on ICF [17], the AROC registry based on AROC impairment [13], the UDSMR registry based on UDS impairment [11], and the payment registry based on ICF [30]. From this perspective, the WebRehab and payment registries are the most compatible with WHO guidelines for coding functioning, disability, and health in people with disabilities. The finding of our literature review is similar to the study of Safdari et al. Their study examined standard classification systems on various rehabilitation-related topics, including the etiology of disability (international classification of diseases-10 [ICD-10]) and the international classification of diseases, the ninth revision, clinical modification (ICD-9-CM); disability diagnosis (ICF); measures (ICD-10 procedure coding system (ICD-10-PCS), International classification of procedures in medicine (ICPM)); refund (functional related group [FRG]); and functional status (FIM) [50].
In a similar vein, McPherson et al. aimed to illustrate the status of rehabilitation HISs in countries with different income levels and detect the main processes and measures to develop such systems in underdeveloped and low-income countries. In their study, they found out that no standard exists for rehabilitation in HISs. However, it is generally believed that valid data on the prevalence of disability, the economic situation, access to rehabilitation services, and practical outcomes of rehabilitation are required to plan for promoting health among individuals with disabilities. This finding implies that planning for disability and rehabilitation can be initiated by developing MDSs and then gradually leads to the system’s improvement and coordination [49].
In a comparative study entitled “Analytical comparison of rehabilitation programs for the disabled in Iran with other countries”, Irvani et al. documented that the integration of parallel organizations’ rehabilitation sectors in the Ministry of Health and Medical Education in Iran, not only enhances intersectoral coordination and the consistency of united management and policy-making but also decreases costs, enhances the proper allocation, and increase the financial resources of this sector. Further, it may decrease the overlap of more desirable service delivery; hence, undertaking responsibilities, preventing repetition, and training specialized personnel regarding the needs are of great importance. Policymakers and planners in this major should adopt a wider perspective to review and modify the structure, regulations, and activities in line with the movement toward formulating a system to equip rehabilitation programs for the disabled in Iran [50].
Commission on Accreditation of Rehabilitation Facilities (CARF) developed a framework to collect the required rehabilitation data by providing a standard model for establishing a management system and evaluating rehabilitation programs. The framework specifies the MDS according to the main rehabilitation components, including input (namely demographic information, health status history, primary diagnosis of disability, etiological injury, time of injury, the acute hospital care center’s functioning, and functional status), process (type of rehabilitation services, frequency of treatment sessions, test results, goals, interventions and measures, progress trend, complications and difficulties, and indicators such as length of stay in inpatient rehabilitation), and output (functional status, complications and difficulties, post-discharge services, and financial support for disabled individuals) [51].
In their study entitled “a review of information management standards of rehabilitation centers accreditation commission”, Safdari et al. aimed to develop a framework for standards required by information management processes in rehabilitation centers. They reported that information management processes ranging from data collection, registration, documentation, organization, and classification to information storage, retrieval, and dissemination in rehabilitation centers should follow the standards concerned by the evaluating organization. However, no consistent and comprehensive standards exist for this purpose at an international level as different institutions active in accrediting and evaluating rehabilitation services of different scopes and detail levels have set some standards in this regard [52].
Ghazi Saeedi et al. in their research entitled “MDS for Schizophrenia Electronic Health Card” concluded that an electronic health card for schizophrenia patients can help the treatment team in providing effective health care and better medical records for inpatient staff. It also reduces the problems of family members and relatives of the patient and simplifies the process of treating schizophrenia. The proposed MDS for schizophrenia includes 29 data elements. They included two general groups of demographic data (basic information, insurance information, and essential contact information) and clinical data (medical history, psychiatric history, and mental status) [38].
Ahmadi et al. in their research entitled “development of the MDS of the health information system of orthopedic injuries in Iran” concluded that some of the necessary data elements that exist in the MDS of other countries or are needed for organizations and health care providers of medical services are not covered in the current systems. Hence, a comprehensive content of MDS should be constructed. The existence of comprehensive and complete data about the causes and mechanisms of traumas informs public health policymakers about the incident of traumas and empowers them to take advisory measures to deal with these difficulties. The MDS of orthopedic injury included two management categories (6 categories and 142 data elements) and clinical categories (17 categories and 250 data elements) [34].
Arastoo et al. standardized the information elements in the audiometric file and provided a suitable model for Iran. This applied descriptive-comparative research was conducted using the Delphi method with the help of 17 faculty members and 110 audiologists. The information elements were introduced in this study in four categories: Demographic information, medical history, patient evaluation, and treatment plan [32].
Furthermore, Damanabi et al. in their research aimed to develop an MDS of speech therapy. They concluded that by designing and implementing appropriate speech therapy data gathering for data collection, and planning for check and debarment of speech disorders, it is necessary to provide high quality and better care to patients in speech therapy centers. The minimal data collection of speech therapy included clinical and administrative levels. The most principal elements of management information include name, last name, birth date, sex, address, phone number, date of admission and number of treatments, patient complaints, duration of impairment or disorder, cause and description of the disease, and the most principal elements of clinical information including health history, short-term goals and the long-term development of speech history [36].
In summary, in some countries, national and international rehabilitation information systems have been implemented and are being used. But still, the main goal of WHO in integrating health care systems with the rehabilitation system has not been achieved in any country. In this regard, WHO has expanded a framework and standards for national HIS and a global reference content of 100 key health values to assist countries to reinforce their HIS. There are opportunities to further expand this framework to accommodate rehabilitation information needs [5].
Undoubtedly, reaching this goal requires cooperation, targeted policies, and huge investment. Therefore, accurate evaluations in terms of cost-effectiveness and identification of challenges and facilitators for the development of rehabilitation information systems are critical [53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65].
5. Conclusion
This literature review demonstrates that the most comprehensive rehabilitation information systems belong to the United States and Australia, which included the sections of inpatient and outpatient rehabilitation for children and adults, then Canada and Sweden, which included the outpatient and inpatient sections. Afterward, the UK included specialist rehabilitation services. This is while a rehabilitation information system was being established in Malaysia. However, in Russia and Iran, only limited studies have been conducted to recommend the implementation of a comprehensive rehabilitation information system. Therefore, the future work of this study is to design and development a comprehensive rehabilitation information system in Iran.
One of the strengths of our study is that it was the first comprehensive review of rehabilitation information registration systems. The findings may contribute to clarifying the current situation in these 8 countries as a representative of the world’s countries. Moreover, in line with the call for planning, WHO should develop a broader view of the developed programs to direct policy-makers toward developing rehabilitation information registration systems.
Since the present study aimed to include comprehensive rehabilitation systems, one of the limitations of this study is disregarding rehabilitation registration systems in smaller disciplines, including pulmonary, heart, and stroke rehabilitation registration systems, and so on. On the other hand, the search keywords may not be adequate and perfect to pick more studies, and some significant and relevant research may have been missed in this review. According to the recommendations of WHO to integrate hospital information systems with the rehabilitation information system and given the current situation, there is no integrated system in accordance with the recommendations of WHO. Future studies are recommended to develop rehabilitation registration systems integrated with national HIRSs.
Ethical Considerations
Compliance with ethical guidelines
This study was approved after review and presentation in the Ethics Committee of Mashhad University of Medical Sciences (Code: IR.MUMS.REC.1400.296).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We hereby express our gratitude to the Student Research Committee of Mashhad University of Medical Sciences who helped us in conducting this research.
References
- Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the global burden of disease study 2019: A systematic analysis for the global burden of disease study 2019. The Lancet. 2021; 396(10267):2006-17. [DOI:10.1016/S0140-6736(20)32340-0] [PMID]
- World Health Organization. World report on disability 2011. Geneva: World Health Organization; 2011. [Link]
- World Health Organization. WHO global disability action plan 2014-2021: Better health for all people with disability. Geneva: World Health Organization; 2015. [Link]
- Halpin SJ, McIvor C, Whyatt G, Adams A, Harvey O, McLean L, et al. Postdischarge symptoms and rehabilitation needs in survivors of covid‐19 infection: A cross‐sectional evaluation. Journal of Medical Virology. 2021; 93(2):1013-22. [DOI:10.1002/jmv.26368] [PMID]
- World Health Organization. Rehabilitation in health systems: Guide for action. Geneva: World Health Organization; 2019. [Link]
- World Health Organization. Rehabilitation. Geneva: World Health Organization; 2021. [Link]
- Gupta N, Castillo-Laborde C, Landry MD. Health-related rehabilitation services: Assessing the global supply of and need for human resources. BMC Health Services Research. 2011; 11:276. [DOI:10.1186/1472-6963-11-276] [PMID] [PMCID]
- Ajami S, Maghsoudlorad AA. The role of information systems to manage cerebral palsy. Iranian Journal of Child Neurology. 2016; 10(2):1-9. [PMID] [PMCID]
- Gliklich RE, Dreyer NA, Leavy MB. Registries for evaluating patient outcomes: A user’s guide. Bethesda: Agency for Healthcare Research and Quality; 2014. [PMID]
- World Health Organization. Health information systems and rehabilitation. Rehabilitation. Geneva: World Health Organization; 2017. [Link]
- No author. Uniform data system for medical rehabilitation (UDSMR) [Internet]. 2022 [Updated December 28]. Available from: [Link]
- Graham JE, Granger CV, Karmarkar AM, Deutsch A, Niewczyk P, Divita MA, et al. The uniform data system for medical rehabilitation: Report of follow-up information on patients discharged from inpatient rehabilitation programs in 2002-2010. American Journal of Physical Medicine & Rehabilitation. 2014; 93(3):231-44. [DOI:10.1097/PHM.0b013e3182a92c58] [PMID] [PMCID]
- Simmonds F, Jones L, Berger M, Tazelaar-Molinia J, Zhang M. Australian clinical quality registries project for ACS & QHC: Final report. Wollongong: Australian Health Services Research Institute; 2009. [Link]
- Webster D. AROC data dictionaries. [Internet]. 2018 [Updated Jun 6 2018]. Available from: [Link]
- University of Wollongong. Australasian rehabilitation outcomes centre [Internet]. 2022 [Updated 2022 December 28]. Available from: [Link]
- Green L. Data collection forms [Internet]. 2022 [Updated 2022 January 13]. Available from: [Link]
- Rehabilitationgsedicine. The Swedish register for rehabilitation medicine has opened a new IT platform. Gothenburg: Rehabilitation Medicine website; 2021. [Link]
- Sunnerhagen KS, Flansbjer UB, Lannsjö M, Tölli A, Lundgren-Nilsson Å. WebRehab: A Swedish database for quality control in rehabilitation. Journal of Rehabilitation Medicine. 2014; 46(10):958-62. [DOI:10.2340/16501977-1886] [PMID]
- Canadian Institute for Health Information. National rehabilitation reporting system metadata [Internet]. 2022 [Updated 2022 December 28]. Available from: [Link]
- Canadian Institute for Health Information. Rehabilitation minimum data set manual, February 2016. Module 1: Technical specifications and data submission. Ottawa: Canadian Institute for Health Information; 2016. [Link]
- Turner-Stokes L, Sephton K, Williams H, Bill A, Kaminska M. UK Rehabilitation Outcomes Collaborative (UK ROC) Triennial report 2015–2018. Buckinghamshire: UK ROC; 2019.
- UK ROC. UK Rehabilitation outcomes collaborative. Buckinghamshire: UK ROC; 2019. [Link]
- UK ROC. UK rehabilitation outcomes collaborative. Buckinghamshire: UK ROC; 2015. [Link]
- Ahmedy F, Fan S, Tuah NM, Nasirin S, Shah SS. Developing virtual data warehouse for rehabilitation registry in Sabah, Borneo: Towards big data analytics and geomapping. UK Academy for Information Systems Conference Proceedings. 2019; 32. [Link]
- Wolfe C, McKevitt C, Rudd A. Stroke services. London: CRC Press; 2016. [DOI:10.1201/9781315385242]
- Pogosova NV, Sokolova OY, Yufereva YM, Osipova IV. [First results of analysis of the Russian part of the European register on cardiac rehabilitation EuroCaReD (European cardiac rehabilitation database) (Russian)]. Kardiologiia. 2015; 55(2):49-56. [PMID]
- Davoodi S, Sadeghniat Haghighi K, Rostam Niakan Kalhori S, Shams Hosseini N, Mohammadzadeh Z, Safdari R. Occupational disease registries-characteristics and experiences. Acta Informatica Medica. 2017; 25(2):136. [DOI:10.5455/aim.2017.25.136-140] [PMID] [PMCID]
- Shoshmin A, Martynova N, Riabokon A. Rehabilitation information system for people with disabilities. New Technology in the Human Services. 1999; 12(1-2):39-46. [Link]
- lamic Parliament Research Center of the Islamic Republic of Iran. [The comprehensive law protecting the rights of persons with disabilities (Persian)]. Tehran: Islamic Parliament Research Center of the Islamic Republic of Iran; 2003. [Link]
- State Welfare Organization of Iran. [Introduction of the State Welfare Organization of Iran Tehran (Persian)]. Tehran: State Welfare Organization of Iran; 2016. [Link]
- Davatgaran K. [The classification of functioning, disability and health (ICF), guide for medical commissions determine the type and severity of disability (Persian)]. Tehran: The State of Welfare Organization; 2016. [Link]
- Arastoo AA, Nickbakht M, Ghasemzadeh R, Azizi A, Zahednejad S, Latifi SM. [Standardization of data elements of audiology records: A suitable model for Iran (Persian)]. Auditory and Vestibular Research. 2012; 21(1):26-37. [Link]
- Arastoo AA, Nickbakht M, Ghasemzadeh R, Azizi A, Zahednejad S, Latifi SM. Developing a national minimum data set for physiotherapy in Iran: A delphi study. European Journal of Scientific Research . 2013; 107(4):573-9. [Link]
- Ahmadi M, Mohammadi A, Chraghbaigi R, Fathi T, Baghini MS. Developing a minimum data set of the information management system for orthopedic injuries in Iran. Iranian Red Crescent Medical Journal. 2014; 16(7):e17020. [PMID] [PMCID] [DOI:10.5812/ircmj.17020]
- Nelson DL, Glass LM. Occupational therapists’ involvement with the minimum data set in skilled nursing and intermediate care facilities. The American Journal of Occupational Therapy. 1999; 53(4):348-52. [DOI:10.5014/ajot.53.4.348]
- Damanabi S, Abdolnejad S, Karimi G. Suggested minimum data set for speech therapy centers affiliated to Tabriz University of Medical Sciences. Acta Informatica Medica. 2015; 23(4):243-7. [DOI:10.5455/aim.2015.23.243-247] [PMID] [PMCID]
- Hoffman KP, Playford DE, Grill E, Soberg HL, Brohi K. Minimum data set to measure rehabilitation needs and health outcome after major trauma: Application of an international framework. European Journal of Physical and Rehabilitation Medicine. 2016; 52(3):331-46. [PMID].
- Nightingale F. UK rehabilitation outcomes collaborative. London: Cicely Saunders Institute; 2015. [Link]
- Ghazi Saeedi M, Safdari Safdari R, Khodaii MR, Hamidi M. Minimum data set for electronic health card of schizophrenia. Annals of Military and Health Sciences Research. 2015; 13(2):e62613. [Link]
- Ahmadi M, Madani T, Alipour J. Development a national minimum data set (MDS) of the information management system for disability in Iran. Disability and Health Journal. 2019; 12(4):641-8. [DOI:10.1016/j.dhjo.2019.05.008] [PMID]
- Mohammadi A, Zarei J, Kameli ME, Vahedi-barzoki A, Rampisheh Z, Meraji M, et al. Design a national minimum data set for hospital information system in Iran-2015. Kashan: Kashan University of Medical Sciences. 2015. [Link]
- Jangi M, Azizi A, Kamali Yousef Abad M, Tara SM. [Systematic design of the minimum data set storage: An essential need to create purposed for archiving (Persian)]. Journal of Health and Biomedical Informatics. 2015; 1(2):113-21. [Link]
- Ahmadi M, Alipour J, Mohammadi A, Khorami F. Development a minimum data set of the information management system for burns. Burns. 2015; 41(5):1092-9. [DOI:10.1016/j.burns.2014.12.009] [PMID]
- Kalankesh LR. Minimum data set for cystic fibrosis registry: A case study in northwest Iran. Acta HealthMedica. 2017; 2(2):180. [DOI:10.19082/ah180]
- Ajami S, Ahmadi G, Saghaeiannejad-Isfahani S, Etemadifar M. A comparative study on iMed© and European database for multiple sclerosis to propose a common language of multiple sclerosis data elements. Journal of Education and Health Promotion. 2014; 3:107. [DOI:10.4103/2277-9531.145894] [PMID] [PMCID]
- Mohammadi A, Ahmadi M, Gharagozlu A. Developing a minimum data set for an information management system to study traffic accidents in Iran. Iranian Red Crescent Medical Journal. 2016; 18(3):e23677. [DOI:10.5812/ircmj.23677] [PMID] [PMCID]
- Hosseini A, Moghaddasi H, Jahanbakhsh M. [Designing minimum data sets of diabetes mellitus: Basis of effectiveness indicators of diabetes management (Persian)]. Health Information Management. 2010; 7(3):330-40. [Link]
- Ahmadi M, Rafii F, Habibi Koolaee M, Mirkarimi A. A comparison of data elements of nursing minimum data set. Iranian Journal of Nursing Research. 2012; 7(24):45-52. [Link]
- Banaye Yazdipour A, Sarbaz M, Dadpour B, Moshiri M, Kimiafar K. [Development a national minimum data set for poisoning registry in Iran (Persian)]. International Journal of Health Planning and Management. 2020; 35(6):1453-67. [DOI:10.1002/hpm.3045] [PMID]
- McPherson A, Durham J, Richards N, Gouda H, Rampatige R, Whittaker M. Strengthening health information systems for disability-related rehabilitation in LMICs. Health Policy and Planning. 2017; 32(3):384-94. [DOI:10.1093/heapol/czw140] [PMID] [PMCID]
- Safdari R, Azadmanjir Z. [Review of information management standards of rehabilitation commission accreditation commission (Persian)]. Journal of Payavard Salamat. 2009; 3(2):18-29. [Link]
- CARF Intrnational. Medical rehabilitation standards manual. Arizona: CARF Intrnational; 2018. [Link]
- Iravani M, Riahi L, Abdi K, Tabibi SJ. A comparative study of the rehabilitation services systems for people with disabilities. Archives of Rehabilitation. 2020; 21(4):544-63. [DOI:10.32598/RJ.21.4.3225.1]
- Mousavi AS, Baigi SF. Assessing the status of tools and methods for evaluating physicians’ documentation in the emergency department: A review study. Frontiers in Health Informatics. 2022; 11(1):110. [DOI:10.30699/fhi.v11i1.348]
- Mousavi Baigi SF, Mousavi Baig SM. Challenges and opportunities of using telemedicine during covid-19 epidemic: A systematic review. Frontiers in Health Informatics. 2022; 11(1):109. [DOI:10.30699/fhi.v11i1.346]
- Mousavi Baigi SF, Moradi F, Vasseifard F, Mohammad Abadi F, Mazaheri Habibi MR. The effect of nutrition training on knowledge of students at university of medical sciences. Topics in Clinical Nutrition. 2022; 37(3):236-41. [DOI:10.1097/TIN.0000000000000290]
- Norouzi Aval R, Mousavi Baigi SF, Sarbaz M, Kimiafar K. Security, privacy, and confidentiality in electronic prescribing systems: A review study. Frontiers in Health Informatics. 2022; 11(1):115. [DOI:10.30699/fhi.v11i1.374]
- Sarbaz M, Baigi SF, Marouzi P, Hasani SM, Kimiafar K. Type and number of errors of the Iranian electronic health record (SEPAS) in hospitals affiliated with Mashhad University of Medical Sciences. Studies in Health Technology and Informatics. 2022; 295:354-7. [DOI:10.3233/SHTI220736] [PMID]
- Baigi SF, Mousavi AS, Kimiafar K, Sarbaz M. Evaluating the cost effectiveness of tele-rehabilitation: A systematic review of randomized clinical trials. Frontiers in Health Informatics. 2022; 11(1):118. [DOI:10.30699/fhi.v11i1.368]
- Sarbaz M, Manouchehri Monazaha F, Eslami S, Kimiafar K, Mousavi Baigi SF. Effect of mobile health interventions for side effects management in patients undergoing chemotherapy: A systematic review. Health Policy and Technology. 2022; 11(4):100680. [DOI:10.1016/j.hlpt.2022.100680]
- Baigi SF, Sarbaz M, Ghaddaripouri K, Noori N, Kimiafar K. The effect of tele-rehabilitation on improving physical activity in patients with chronic obstructive pulmonary disease: A systematic review of randomized controlled clinical trials. Frontiers in Health Informatics. 2022; 11(1):113. [DOI:10.30699/fhi.v11i1.359]
- Mousavi Baigi SF, Sarbaz M, Marouzi P, Kimiafar K. Evaluating the impact of digital game on learning medical terminology of paramedical students: Protocol for a randomized controlled trial. Studies in Health Technology and Informatics. 2022; 295:51-4. [PMID]
- Mousavi Baigi SF, Aval RN, Sarbaz M, Kimiafar K. Evaluation tools for digital educational games: A systematic review. Acta Medica Iranica. 2022; 60(8):508-12. [Link]
- Baigi SF, Sarbaz M, Sobhani-Rad D, Mousavi AS, Kimiafar K. Rehabilitation registration systems: Current recommendations and challenges. Frontiers in Health Informatics. 2022; 11(1):124.[Link]
- Baigi SF, Sarbaz M, Sobhani-Rad D, Dahmardeh F, Mehneh MR, Mousavi AS, Kimiafar K. Rehabilitation information systems: What we know and what we want. International Journal of Health Sciences. 2022; 6(S7):48241–55. [Link]
Article type: Reviews |
Subject:
Rehabilitation Management
Received: 2022/03/25 | Accepted: 2022/10/31 | Published: 2023/03/1
Received: 2022/03/25 | Accepted: 2022/10/31 | Published: 2023/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
