
988368
Fri, Jun 19, 2026

Volume 24, Issue 1 (March 2026)
Iranian Rehabilitation Journal 2026, 24(1): 11-26 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tomaszewski M, Pruc M, Fudalej P, Chirico F, Al-Jeabory M, Hicham K, et al . Biological Therapies in Treating Knee Osteoarthritis: A Narrative Review. Iranian Rehabilitation Journal 2026; 24 (1) :11-26
URL: http://irj.uswr.ac.ir/article-1-2444-en.html
URL: http://irj.uswr.ac.ir/article-1-2444-en.html
Marcin Tomaszewski1 

 , Michal Pruc2 , Piotr Fudalej3 , Francesco Chirico4 , Mahdi Al-Jeabory5 , Khabbache Hicham6 , Majid Ansari7 , Morteza Faghih Jouibari8 , Lukasz Szarpak *9
, Michal Pruc2 , Piotr Fudalej3 , Francesco Chirico4 , Mahdi Al-Jeabory5 , Khabbache Hicham6 , Majid Ansari7 , Morteza Faghih Jouibari8 , Lukasz Szarpak *9
, Michal Pruc2 , Piotr Fudalej3 , Francesco Chirico4 , Mahdi Al-Jeabory5 , Khabbache Hicham6 , Majid Ansari7 , Morteza Faghih Jouibari8 , Lukasz Szarpak *9
1- Department of Clinical Research and Development, LUXMED Group, Warsaw, Poland.
2- Institute of Medical Science, The John Paul II Catholic University of Lublin, Lublin, Poland.
3- ORTHOS Multi-Specialty Hospital Komorowice, LUXMED Group, Komorowice, Poland.
4- Department of Security and Bioethics, Section of Occupational Health, Università Cattolica del Sacro Cuore, Rome, Italy. & Health Service Department, Italian State Police, Ministry of the Interior, Milan, Italy.
5- Department of Clinical Orthopedic, Silesian Center for Rheumatology in Ustron, Ustron, Poland.
6- Department of Psychology, Faculty of Arts and Human Sciences Fès-Saïss, Sidi Mohamed Ben Abdellah University, Fez, Morocco. & Director of Lifelong Learning Observatory, UNESCO/USMBA, Fez, Morocco.
7- Department of Neurosurgery, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran.
8- Sports Medicine Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran.
9- Institute of Medical Science, The John Paul II Catholic University of Lublin, Lublin, Poland. & Department of Henry JN Taub Emergency Medicine, Baylor College of Medicine, Houston, United States.
2- Institute of Medical Science, The John Paul II Catholic University of Lublin, Lublin, Poland.
3- ORTHOS Multi-Specialty Hospital Komorowice, LUXMED Group, Komorowice, Poland.
4- Department of Security and Bioethics, Section of Occupational Health, Università Cattolica del Sacro Cuore, Rome, Italy. & Health Service Department, Italian State Police, Ministry of the Interior, Milan, Italy.
5- Department of Clinical Orthopedic, Silesian Center for Rheumatology in Ustron, Ustron, Poland.
6- Department of Psychology, Faculty of Arts and Human Sciences Fès-Saïss, Sidi Mohamed Ben Abdellah University, Fez, Morocco. & Director of Lifelong Learning Observatory, UNESCO/USMBA, Fez, Morocco.
7- Department of Neurosurgery, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran.
8- Sports Medicine Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran.
9- Institute of Medical Science, The John Paul II Catholic University of Lublin, Lublin, Poland. & Department of Henry JN Taub Emergency Medicine, Baylor College of Medicine, Houston, United States.
Keywords: Osteoarthritis, Knee, Platelet-rich plasma (PRP), Hyaluronic acid (HA), Mesenchymal stem cells (MSCs), Regenerative medicine
Full-Text [PDF 2909 kb]
(134 Downloads)
| Abstract (HTML) (2211 Views)
References:
Full-Text: (11 Views)
Introduction
Osteoarthritis (OA) of the knee is among the most commonly diagnosed conditions of the musculoskeletal system in adults and the elderly [1]. In 2020, 595 million individuals worldwide were afflicted with OA, representing 7.6% of the global population, and marking a 132.2% increase in total cases since 1990. In comparison to 2020, the incidence of OA is anticipated to rise by 74.9% for the knee, 48.6% for the hand, 78.6% for the hip, and 95.1% for other forms of OA by 2050. In 2020, the global age-standardised rate of years lived with disability (YLDs) for total OA was 255.0 YLDs per 100000, reflecting a 9.5% increase since 1990. In adults aged 70 years and above, OA ranked seventh among the causes of YLDs [2]. The chronic nature of the condition, characterized by pain, stiffness, and restricted mobility, markedly diminishes patients’ quality of life (QoL) [3]. The rise in life expectancy and the prevalent presence of risk factors, such as obesity and mechanical injuries, lead to a higher incidence of individuals afflicted by this disease [4, 5]. Obesity is a significant modifiable risk factor as it elevates pressure on the knee joints. Mechanical injuries, including ligament ruptures or intra-articular fractures, may accelerate joint degeneration, particularly in younger, active individuals. Aging results in diminished regenerative capacity of cartilage and alterations in synovial fluid composition, thereby facilitating the onset of OA symptoms. Moreover, genetic predispositions may affect the quality and functionality of articular cartilage, necessitating further research for more precise determination of the mechanisms by which non-coding single nucleotide polymorphisms regulate gene expression and affect cartilage homeostasis throughout the lifespan, including during joint development and aging [6]. The intricate pathogenesis of OA, stemming from cartilage degeneration and inflammatory processes in the synovium, renders the treatment of this condition challenging [7]. OA is a condition that causes extensive damage to joint structures, impairing their mechanical functions and disrupting patients’ daily activities. Characteristic alterations are degenerative processes in the articular cartilage, which softens, becomes fibrillated, and exhibits substantial defects [8]. This condition results in a decrease in cartilage thickness and a deterioration of its shock-absorbing capacity, leading to restricted mobility and discomfort [9]. Moreover, the development of osteophytes, or bone growths, as a response to alterations in joint biomechanics, exacerbates mobility restrictions and amplifies pain symptoms [10]. Articular cartilage undergoes progressive degeneration. The reduction in cartilage thickness markedly diminishes its load-bearing capacity, resulting in heightened pressure on the subchondral bone tissue. Sclerotization of subchondral bone tissue, caused by excessive stress on articular cartilage, is a significant factor in the pathogenesis of OA. It enhances the density of bone tissue, thereby diminishing its elasticity and resulting in pain [11]. These processes are intricate and gradual, necessitating a therapeutic strategy that considers both the prevention of progressive alterations and the potential regeneration of injured tissues. Due to the constraints of conventional treatment approaches, including pharmacotherapy and surgical procedures, biological therapies that can both mitigate symptoms and promote the regeneration of damaged joint structures are garnering heightened interest. Nonsteroidal anti-inflammatory drugs and glucocorticosteroids exhibit limited efficacy and may induce adverse effects, while surgical interventions like arthroplasty entail a risk of complications [12, 13]. The mechanisms of action are essential for effective intervention and treatment optimization in patients with this disease, facilitating improved adaptation of therapeutic methods to individual requirements.
Biological therapies, including the application of hyaluronic acid (HA) or platelet-rich plasma (PRP), seek to mitigate the degenerative process and facilitate the regeneration of compromised tissues. Furthermore, the advancement of stem cell therapies presents novel treatment alternatives; provide a more focused strategy for cartilage regeneration and the modulation of inflammatory processes, rendering them promising therapeutic alternatives for OA treatment, highlighting the necessity for additional investigation into their efficacy and safety.
This study aims to assess the efficacy and safety of specific biological therapies for knee OA treatment. The emphasis was on 3 therapeutic modalities: PRP, HA, and stem cells. Their efficacy is evaluated regarding pain alleviation, enhancement of joint function, and regenerative capacity. Addressing this issue is of considerable practical significance as it facilitates the selection of more effective and patient-specific therapeutic strategies.
Materials and Methods
The relevant articles published in the last 10 years were reviewed to obtain data about the efficacy of the biologic treatments utilized in knee OA, including PRP, Hyaluronate acid (HA) or stem cell therapies. Articles were collected at the beginning of December 2024 using PubMed, Cochrane Controlled Trials Register (CENTRAL), Web of Science, and Embase databases without limiting the type of article publication. The following search strategy was used to optimise both search specificity and sensitivity, with the following key words and phrases: “knee” AND “OA” OR “osteoarthritides” OR “osteoarthr*” OR “arthrosis” OR “degenerative arthr*” OR “knee OA” AND “Platelet Rich Plasma” OR “Plasma, Platelet-Rich” OR “PRP” OR “Hyaluronic Acid” OR “HA” OR “Hyaluronate, Sodium” OR “Sodium Hyalorunate“ OR “Mesenchymal stem cells” OR “MSCs” OR “Bone marrow aspirate concentrate” OR “BAMC.” Articles unavailable in full-text and English language were excluded.
Results
Sixty-seven articles pertained to the subject, comprising 20 review articles, 37 original research articles, and 10 meta-analyses [14-80]. Among these, 18 studies investigated the role of inflammatory mediators and cytokines in OA, 25 concentrated on regenerative therapies, including mesenchymal stem cells and PRP, and 24 assessed the efficacy and safety of viscosupplementation using HA and other advanced biological interventions. These research offer an in-depth comprehension of inflammatory mechanisms, regeneration capabilities, and the therapeutic utilization of biological therapies in the treatment of knee OA.
Discussion
Inflammatory and regenerative mechanisms
Inflammatory processes are pivotal in the onset and advancement of knee OA, facilitating the deterioration of articular cartilage and altering the intra-articular microenvironment. A critical factor in the pathogenesis of OA is an altered cytokine equilibrium favouring proinflammatory cytokines, which instigate a detrimental cycle resulting in damage to cartilage and other intra-articular structures through the activation of catabolic enzymes, specifically matrix metalloproteinases (MMPs) and a disintegrin and metalloproteinase with thrombospondin motif [14].
The most important inflammatory cytokines involve interleukin (IL)-1β, tumor necrosis factor alpha (TNFα), IL-6, IL-15, IL-17, and IL-18 and anti-inflammatory cytokines include IL-4, IL-10, and IL-13, interferon (IFN)-γ with regulatory cytokines IL-6 (negative regulator of chondrocyte proliferation), IL-8 (regulator of chondrocyte hypertrophy). Standard biomarkers of inflammation also include chemokines, adipokines, and collagen derivatives of nitrous oxide [15]. These cytokines facilitate the recruitment of inflammatory cells in the synovium, leading to additional damage to both cartilage and subchondral bone tissue. Under the influence of inflammatory cytokines, the immune system cells that traverse to the locus of inflammation produce inflammatory prostaglandin E2 (PGE2), cyclooxygenase-2, phospholipase A2, nitric oxide (NO), and free radicals [16]. A significant element of this process is the elevation in the production of reactive oxygen species, which induces oxidative stress and further exacerbates the deterioration of the extracellular matrix [17]. Research findings indicate that elevated levels of pro-inflammatory cytokines in synovial fluid correlate directly with the severity of symptoms, including pain and restricted joint mobility [18]. Anti-inflammatory cytokines suppress the production of inflammatory cytokines, particularly IL-1β and TNFα, while promoting proteoglycan synthesis, preventing chondrocyte apoptosis, reducing the synthesis and secretion of MMPs, and diminishing the degradation of PGE2 levels [19]. Anti-inflammatory cytokines primarily influence cells activated by inflammatory cytokines, exhibiting no substantial difference in the metabolism of unstimulated cells. Consequently, biological therapies that inhibit IL-1β and TNF-α signaling pathways may serve as a crucial instrument in mitigating cartilage tissue degradation in OA.
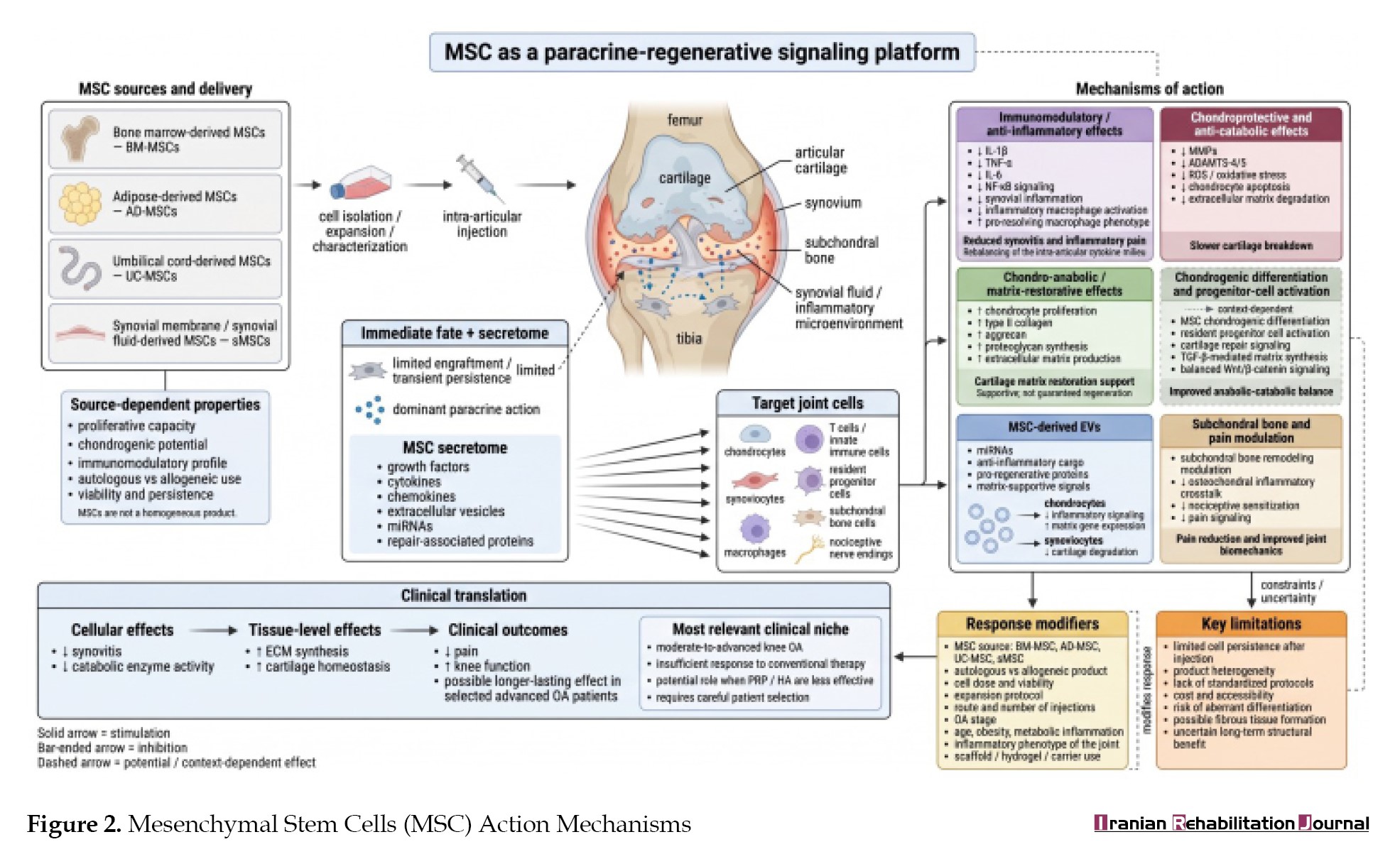
Regenerative processes are equally crucial in OA therapy, fostering anabolic activities and mitigating catabolic structural damage [20]. Mesenchymal stem cells (MSC) possess the capacity to differentiate into chondrocytes, thereby facilitating the regeneration of articular cartilage through enhanced synthesis of type II collagen and aggrecan. MSC secrete various bioactive molecules, including transforming growth factor (TGF)-β and vascular endothelial growth factor (VEGF), which promote anabolic processes while concurrently inhibiting the activity of catabolic MMPs. Furthermore, their secretome, which includes extracellular vesicles (EVs), influences the local inflammatory milieu in the joint, diminishing the levels of pro-inflammatory cytokines and preventing cartilage degradation [21, 22]. Clinical studies demonstrate that MSC administration alleviates pain and enhances joint function by repairing damaged cartilage and modulating inflammatory processes [23]. The Wnt-β catenin pathway is crucial in regulating regenerative processes in OA, and its modulation through biological therapies presents novel therapeutic opportunities [24]. This pathway modulates the equilibrium between anabolic and catabolic processes in articular cartilage. Hyperactivity of the pathway may result in unregulated cartilage degeneration, highlighting the necessity for its meticulous regulation. MSC can modulate the Wnt-β catenin pathway by enhancing the production of type II collagen and aggrecan, thereby facilitating cartilage regeneration [25]. Growth factors like TGF-β influence this pathway to enhance repair mechanisms in articular cartilage. The capacity of MSC to inhibit catabolic processes renders them especially efficacious in the initial phases of OA, indicating the necessity for additional research and the standardization of their application protocols.
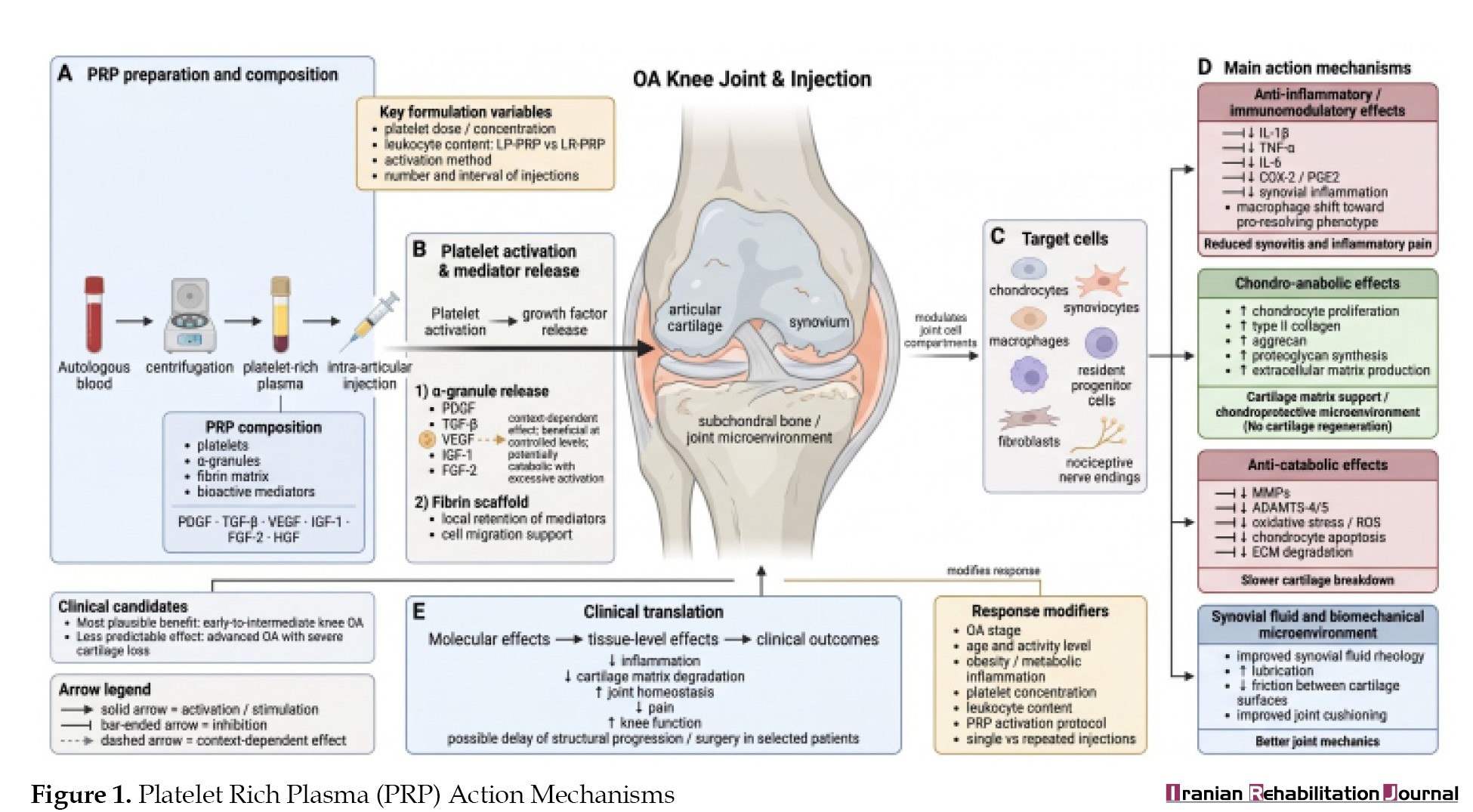
PRP facilitates the regeneration of joint tissues due to the presence of growth factors like TGF-β and platelet-derived growth factor (PDGF), which expedite cartilage reconstruction. PRP elevates the concentration of these growth factors at the administration site, thereby effectively promoting chondrocyte proliferation and proteoglycan synthesis. Growth factors in PRP, including TGF-β, regulate anabolic processes and diminish inflammation by inhibiting pro-inflammatory cytokine activity [26]. The mechanism of PRP also involves aiding fibroblasts and progenitor cells in the restoration of injured joint tissues, thereby enhancing the biomechanical characteristics of the joint [27]. Research indicates that leukocyte poor PRP reduces the likelihood of excessive inflammation and is more appropriate for the management of OA [28, 29]. Randomized controlled trials validate the efficacy of PRP in alleviating pain and enhancing joint function, particularly in the initial and intermediate phases of the disease [30].
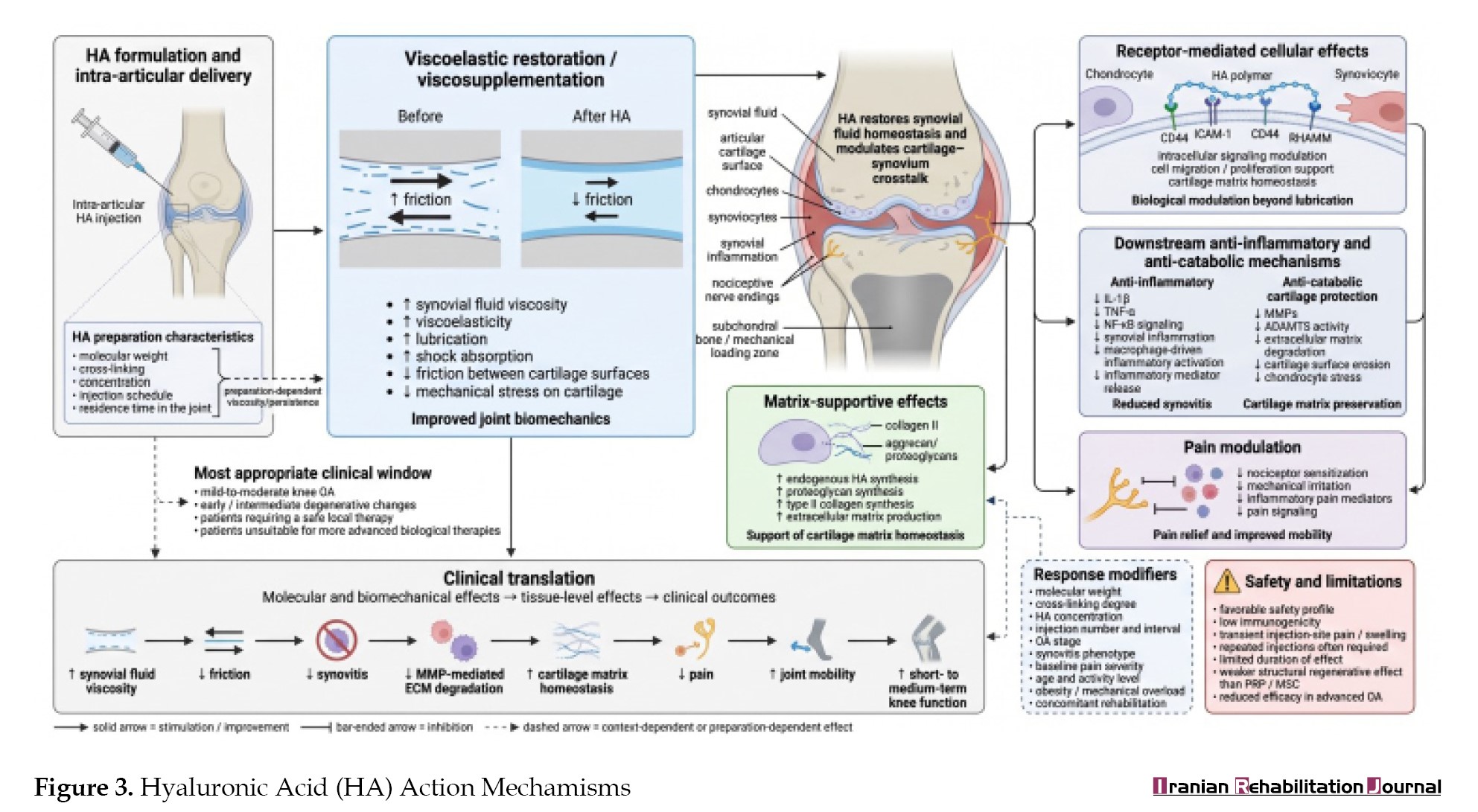
HA is a significant biological therapeutic approach that regulates inflammatory processes and enhances the synovial fluid milieu. HA enhances the viscosity of synovial fluid owing to its viscoelastic characteristics, thereby diminishing friction and augmenting joint cushioning [31]. The capacity of HA to diminish the activity of pro-inflammatory cytokines like IL-1β while concurrently promoting chondrocyte production of extracellular matrix underscores its significance in cartilage regeneration. HA viscosupplementation therapy diminishes synovial inflammation, leading to decreased pain and enhanced joint mobility [32].
Biological mechanisms in the repair of cartilage tissue
The regeneration of cartilage tissue in the knee represents a significant challenge in the management of knee OA. This condition results from the restricted regenerative ability of cartilage, attributable to its unique structure and diminished metabolic activity. The absence of blood vessels in cartilage tissue results in inadequate nutrient supply and waste removal, thereby complicating the repair process following injury or degenerative disease [33]. Furthermore, chondrocytes, the cells tasked with synthesizing the extracellular matrix, operate in an environment that restricts access to growth factors essential for regeneration, thereby diminishing their reparative capabilities [34]. Growth factors, including TGF-β and VEGF, are essential for cartilage regeneration. TGF-β facilitates the repair process by promoting chondrocyte proliferation, synthesizing type II collagen and aggrecan, and inhibiting extracellular matrix degradation. Nonetheless, VEGF exhibits a more ambiguous influence. It promotes angiogenesis in periarticular injury, yet its overexpression can trigger catabolic processes in chondrocytes, rendering its precise regulation a crucial aspect of therapy. Research utilizing VEGF inhibitors, including vandetanib, demonstrates that the inhibition of this factor can effectively impede degenerative processes in the knee joint, as corroborated by animal models [35]. In cartilage regeneration, therapies aimed at local progenitor cells within the superficial layer of cartilage may yield substantial effects. These cells, due to their capacity to proliferate and differentiate into chondrocytes, are crucial in the early phases of regeneration. Growth factors like TGF-β facilitate the recruitment and activation of these cells for tissue repair. The microstructural environment of the joint, including synovial fluid composition, may influence the regenerative capacity of these cells.
The use of PRP for the management of knee OA
PRP represents a novel method for addressing OA of the knee, utilizing the inherent properties of the growth factors present in the formulation.
PRP is a contemporary therapeutic approach for treating degenerative knee diseases, utilizing autologous platelets to promote tissue regeneration. PRP enhances the rheological properties of synovial fluid, augmenting its viscosity and lubricating capabilities, thereby diminishing friction between joint surfaces and mitigating further cartilage deterioration [36]. Growth factors present in PRP, including PDGF and TGF-β, are essential in the regeneration of joint cartilage [37]. Their mechanism of action involves the stimulation of chondrocyte proliferation, the production of extracellular matrix, and the regeneration of damaged joint structures (Figure 1).
Osteoarthritis (OA) of the knee is among the most commonly diagnosed conditions of the musculoskeletal system in adults and the elderly [1]. In 2020, 595 million individuals worldwide were afflicted with OA, representing 7.6% of the global population, and marking a 132.2% increase in total cases since 1990. In comparison to 2020, the incidence of OA is anticipated to rise by 74.9% for the knee, 48.6% for the hand, 78.6% for the hip, and 95.1% for other forms of OA by 2050. In 2020, the global age-standardised rate of years lived with disability (YLDs) for total OA was 255.0 YLDs per 100000, reflecting a 9.5% increase since 1990. In adults aged 70 years and above, OA ranked seventh among the causes of YLDs [2]. The chronic nature of the condition, characterized by pain, stiffness, and restricted mobility, markedly diminishes patients’ quality of life (QoL) [3]. The rise in life expectancy and the prevalent presence of risk factors, such as obesity and mechanical injuries, lead to a higher incidence of individuals afflicted by this disease [4, 5]. Obesity is a significant modifiable risk factor as it elevates pressure on the knee joints. Mechanical injuries, including ligament ruptures or intra-articular fractures, may accelerate joint degeneration, particularly in younger, active individuals. Aging results in diminished regenerative capacity of cartilage and alterations in synovial fluid composition, thereby facilitating the onset of OA symptoms. Moreover, genetic predispositions may affect the quality and functionality of articular cartilage, necessitating further research for more precise determination of the mechanisms by which non-coding single nucleotide polymorphisms regulate gene expression and affect cartilage homeostasis throughout the lifespan, including during joint development and aging [6]. The intricate pathogenesis of OA, stemming from cartilage degeneration and inflammatory processes in the synovium, renders the treatment of this condition challenging [7]. OA is a condition that causes extensive damage to joint structures, impairing their mechanical functions and disrupting patients’ daily activities. Characteristic alterations are degenerative processes in the articular cartilage, which softens, becomes fibrillated, and exhibits substantial defects [8]. This condition results in a decrease in cartilage thickness and a deterioration of its shock-absorbing capacity, leading to restricted mobility and discomfort [9]. Moreover, the development of osteophytes, or bone growths, as a response to alterations in joint biomechanics, exacerbates mobility restrictions and amplifies pain symptoms [10]. Articular cartilage undergoes progressive degeneration. The reduction in cartilage thickness markedly diminishes its load-bearing capacity, resulting in heightened pressure on the subchondral bone tissue. Sclerotization of subchondral bone tissue, caused by excessive stress on articular cartilage, is a significant factor in the pathogenesis of OA. It enhances the density of bone tissue, thereby diminishing its elasticity and resulting in pain [11]. These processes are intricate and gradual, necessitating a therapeutic strategy that considers both the prevention of progressive alterations and the potential regeneration of injured tissues. Due to the constraints of conventional treatment approaches, including pharmacotherapy and surgical procedures, biological therapies that can both mitigate symptoms and promote the regeneration of damaged joint structures are garnering heightened interest. Nonsteroidal anti-inflammatory drugs and glucocorticosteroids exhibit limited efficacy and may induce adverse effects, while surgical interventions like arthroplasty entail a risk of complications [12, 13]. The mechanisms of action are essential for effective intervention and treatment optimization in patients with this disease, facilitating improved adaptation of therapeutic methods to individual requirements.
Biological therapies, including the application of hyaluronic acid (HA) or platelet-rich plasma (PRP), seek to mitigate the degenerative process and facilitate the regeneration of compromised tissues. Furthermore, the advancement of stem cell therapies presents novel treatment alternatives; provide a more focused strategy for cartilage regeneration and the modulation of inflammatory processes, rendering them promising therapeutic alternatives for OA treatment, highlighting the necessity for additional investigation into their efficacy and safety.
This study aims to assess the efficacy and safety of specific biological therapies for knee OA treatment. The emphasis was on 3 therapeutic modalities: PRP, HA, and stem cells. Their efficacy is evaluated regarding pain alleviation, enhancement of joint function, and regenerative capacity. Addressing this issue is of considerable practical significance as it facilitates the selection of more effective and patient-specific therapeutic strategies.
Materials and Methods
The relevant articles published in the last 10 years were reviewed to obtain data about the efficacy of the biologic treatments utilized in knee OA, including PRP, Hyaluronate acid (HA) or stem cell therapies. Articles were collected at the beginning of December 2024 using PubMed, Cochrane Controlled Trials Register (CENTRAL), Web of Science, and Embase databases without limiting the type of article publication. The following search strategy was used to optimise both search specificity and sensitivity, with the following key words and phrases: “knee” AND “OA” OR “osteoarthritides” OR “osteoarthr*” OR “arthrosis” OR “degenerative arthr*” OR “knee OA” AND “Platelet Rich Plasma” OR “Plasma, Platelet-Rich” OR “PRP” OR “Hyaluronic Acid” OR “HA” OR “Hyaluronate, Sodium” OR “Sodium Hyalorunate“ OR “Mesenchymal stem cells” OR “MSCs” OR “Bone marrow aspirate concentrate” OR “BAMC.” Articles unavailable in full-text and English language were excluded.
Results
Sixty-seven articles pertained to the subject, comprising 20 review articles, 37 original research articles, and 10 meta-analyses [14-80]. Among these, 18 studies investigated the role of inflammatory mediators and cytokines in OA, 25 concentrated on regenerative therapies, including mesenchymal stem cells and PRP, and 24 assessed the efficacy and safety of viscosupplementation using HA and other advanced biological interventions. These research offer an in-depth comprehension of inflammatory mechanisms, regeneration capabilities, and the therapeutic utilization of biological therapies in the treatment of knee OA.
Discussion
Inflammatory and regenerative mechanisms
Inflammatory processes are pivotal in the onset and advancement of knee OA, facilitating the deterioration of articular cartilage and altering the intra-articular microenvironment. A critical factor in the pathogenesis of OA is an altered cytokine equilibrium favouring proinflammatory cytokines, which instigate a detrimental cycle resulting in damage to cartilage and other intra-articular structures through the activation of catabolic enzymes, specifically matrix metalloproteinases (MMPs) and a disintegrin and metalloproteinase with thrombospondin motif [14].
The most important inflammatory cytokines involve interleukin (IL)-1β, tumor necrosis factor alpha (TNFα), IL-6, IL-15, IL-17, and IL-18 and anti-inflammatory cytokines include IL-4, IL-10, and IL-13, interferon (IFN)-γ with regulatory cytokines IL-6 (negative regulator of chondrocyte proliferation), IL-8 (regulator of chondrocyte hypertrophy). Standard biomarkers of inflammation also include chemokines, adipokines, and collagen derivatives of nitrous oxide [15]. These cytokines facilitate the recruitment of inflammatory cells in the synovium, leading to additional damage to both cartilage and subchondral bone tissue. Under the influence of inflammatory cytokines, the immune system cells that traverse to the locus of inflammation produce inflammatory prostaglandin E2 (PGE2), cyclooxygenase-2, phospholipase A2, nitric oxide (NO), and free radicals [16]. A significant element of this process is the elevation in the production of reactive oxygen species, which induces oxidative stress and further exacerbates the deterioration of the extracellular matrix [17]. Research findings indicate that elevated levels of pro-inflammatory cytokines in synovial fluid correlate directly with the severity of symptoms, including pain and restricted joint mobility [18]. Anti-inflammatory cytokines suppress the production of inflammatory cytokines, particularly IL-1β and TNFα, while promoting proteoglycan synthesis, preventing chondrocyte apoptosis, reducing the synthesis and secretion of MMPs, and diminishing the degradation of PGE2 levels [19]. Anti-inflammatory cytokines primarily influence cells activated by inflammatory cytokines, exhibiting no substantial difference in the metabolism of unstimulated cells. Consequently, biological therapies that inhibit IL-1β and TNF-α signaling pathways may serve as a crucial instrument in mitigating cartilage tissue degradation in OA.
Regenerative processes are equally crucial in OA therapy, fostering anabolic activities and mitigating catabolic structural damage [20]. Mesenchymal stem cells (MSC) possess the capacity to differentiate into chondrocytes, thereby facilitating the regeneration of articular cartilage through enhanced synthesis of type II collagen and aggrecan. MSC secrete various bioactive molecules, including transforming growth factor (TGF)-β and vascular endothelial growth factor (VEGF), which promote anabolic processes while concurrently inhibiting the activity of catabolic MMPs. Furthermore, their secretome, which includes extracellular vesicles (EVs), influences the local inflammatory milieu in the joint, diminishing the levels of pro-inflammatory cytokines and preventing cartilage degradation [21, 22]. Clinical studies demonstrate that MSC administration alleviates pain and enhances joint function by repairing damaged cartilage and modulating inflammatory processes [23]. The Wnt-β catenin pathway is crucial in regulating regenerative processes in OA, and its modulation through biological therapies presents novel therapeutic opportunities [24]. This pathway modulates the equilibrium between anabolic and catabolic processes in articular cartilage. Hyperactivity of the pathway may result in unregulated cartilage degeneration, highlighting the necessity for its meticulous regulation. MSC can modulate the Wnt-β catenin pathway by enhancing the production of type II collagen and aggrecan, thereby facilitating cartilage regeneration [25]. Growth factors like TGF-β influence this pathway to enhance repair mechanisms in articular cartilage. The capacity of MSC to inhibit catabolic processes renders them especially efficacious in the initial phases of OA, indicating the necessity for additional research and the standardization of their application protocols.
PRP facilitates the regeneration of joint tissues due to the presence of growth factors like TGF-β and platelet-derived growth factor (PDGF), which expedite cartilage reconstruction. PRP elevates the concentration of these growth factors at the administration site, thereby effectively promoting chondrocyte proliferation and proteoglycan synthesis. Growth factors in PRP, including TGF-β, regulate anabolic processes and diminish inflammation by inhibiting pro-inflammatory cytokine activity [26]. The mechanism of PRP also involves aiding fibroblasts and progenitor cells in the restoration of injured joint tissues, thereby enhancing the biomechanical characteristics of the joint [27]. Research indicates that leukocyte poor PRP reduces the likelihood of excessive inflammation and is more appropriate for the management of OA [28, 29]. Randomized controlled trials validate the efficacy of PRP in alleviating pain and enhancing joint function, particularly in the initial and intermediate phases of the disease [30].
HA is a significant biological therapeutic approach that regulates inflammatory processes and enhances the synovial fluid milieu. HA enhances the viscosity of synovial fluid owing to its viscoelastic characteristics, thereby diminishing friction and augmenting joint cushioning [31]. The capacity of HA to diminish the activity of pro-inflammatory cytokines like IL-1β while concurrently promoting chondrocyte production of extracellular matrix underscores its significance in cartilage regeneration. HA viscosupplementation therapy diminishes synovial inflammation, leading to decreased pain and enhanced joint mobility [32].
Biological mechanisms in the repair of cartilage tissue
The regeneration of cartilage tissue in the knee represents a significant challenge in the management of knee OA. This condition results from the restricted regenerative ability of cartilage, attributable to its unique structure and diminished metabolic activity. The absence of blood vessels in cartilage tissue results in inadequate nutrient supply and waste removal, thereby complicating the repair process following injury or degenerative disease [33]. Furthermore, chondrocytes, the cells tasked with synthesizing the extracellular matrix, operate in an environment that restricts access to growth factors essential for regeneration, thereby diminishing their reparative capabilities [34]. Growth factors, including TGF-β and VEGF, are essential for cartilage regeneration. TGF-β facilitates the repair process by promoting chondrocyte proliferation, synthesizing type II collagen and aggrecan, and inhibiting extracellular matrix degradation. Nonetheless, VEGF exhibits a more ambiguous influence. It promotes angiogenesis in periarticular injury, yet its overexpression can trigger catabolic processes in chondrocytes, rendering its precise regulation a crucial aspect of therapy. Research utilizing VEGF inhibitors, including vandetanib, demonstrates that the inhibition of this factor can effectively impede degenerative processes in the knee joint, as corroborated by animal models [35]. In cartilage regeneration, therapies aimed at local progenitor cells within the superficial layer of cartilage may yield substantial effects. These cells, due to their capacity to proliferate and differentiate into chondrocytes, are crucial in the early phases of regeneration. Growth factors like TGF-β facilitate the recruitment and activation of these cells for tissue repair. The microstructural environment of the joint, including synovial fluid composition, may influence the regenerative capacity of these cells.
The use of PRP for the management of knee OA
PRP represents a novel method for addressing OA of the knee, utilizing the inherent properties of the growth factors present in the formulation.
PRP is a contemporary therapeutic approach for treating degenerative knee diseases, utilizing autologous platelets to promote tissue regeneration. PRP enhances the rheological properties of synovial fluid, augmenting its viscosity and lubricating capabilities, thereby diminishing friction between joint surfaces and mitigating further cartilage deterioration [36]. Growth factors present in PRP, including PDGF and TGF-β, are essential in the regeneration of joint cartilage [37]. Their mechanism of action involves the stimulation of chondrocyte proliferation, the production of extracellular matrix, and the regeneration of damaged joint structures (Figure 1).
An essential aspect of PRP’s function is its influence on the equilibrium between anabolic and catabolic processes in the knee joint. Growth factors present in PRP, including TGF-β, activate macrophages to inhibit catabolic activities, thereby promoting the long-term stabilization of articular cartilage. Studies demonstrate that PRP is especially efficacious in the initial phases of knee OA, where cartilage deterioration is minimal, resulting in improved clinical outcomes [38].
The variability in PRP preparation protocols, encompassing centrifugation techniques, leukocyte composition, and activation methods, intrapersonal and interpersonal differences in PRP composition, significantly influences the therapeutic efficacy. PRP preparation protocols influence the concentration of growth factors and, therefore, the efficacy of treatment [39]. Procedures for PRP activation, such as thrombin or calcium ion application, enhance the release of growth factors, potentially expediting cartilage tissue regeneration [40]. Furthermore, leukocytes in PRP may induce transient inflammation, necessitating additional investigation into the ideal formulation of the preparation. Research findings also indicate that leukocyte-poor PRP exhibits superior efficacy relative to leukocyte-rich PRP, attributed to a diminished risk of leukocyte-induced inflammation [41]. Furthermore, the assessment of the efficacy of distinct PRP types reveals that the leukocyte-poor variant exhibits a diminished risk of adverse effects and enhanced effectiveness in mitigating inflammation relative to leukocytogenic PRP. The administration protocols for PRP, encompassing single or multiple injections, are a crucial component of the therapy. Multiple PRP injections may yield more enduring therapeutic advantages than a solitary administration, indicating the necessity for enhanced standardization of treatment protocols [42]. It is essential to note that the efficacy of PRP therapy is contingent upon the disease stage, necessitating the implementation of suitable patient selection criteria. The repeated application of PRP at designated intervals, such as weekly or monthly, yields superior outcomes in alleviating pain and enhancing joint functionality relative to a singular treatment. The customization of injection protocols based on the patient’s age, disease stage, and comorbidities may substantially influence therapeutic efficacy. Repeated PRP administration has been demonstrated to facilitate the reconstruction of the extracellular matrix, resulting in sustained enhancement of knee joint condition. The variety of protocols underscores the necessity for standardization to attain consistent therapeutic outcomes.
PRP is an innovative approach employed in the management of knee OA, with its efficacy substantiated by numerous scientific studies. Patients receiving intra-articular PRP injections demonstrate a marked decrease in pain and enhancement in joint function relative to alternative therapeutic approaches, including HA or placebo [43, 44]. Research indicates that PRP is most advantageous in the early and mid-stages of knee OA, rendering it more appropriate for younger patients with less severe injuries. The benefits of PRP are further enhanced by its excellent safety profile, attributable to its autologous source. PRP possesses a favourable safety profile owing to its autologous nature, thereby mitigating the risk of immune responses or disease transmission [45]. Clinical studies validate the negligible risk of complications, including transient swelling or pain at the injection site, thereby enhancing patient acceptance of this therapy. This condition reduces the likelihood of immune responses and disease transmission. This fact enhances the acceptance of the therapy among patients and physicians, establishing PRP as a significant alternative in the management of knee OA. The significant efficacy of PRP in alleviating pain and inflammation renders it a notably advantageous alternative for patients who are intolerant to conventional anti-inflammatory medications [46]. Although there is substantial evidence supporting the efficacy of PRP, certain studies challenge its effectiveness, suggesting the potential influence of a placebo effect or inadequate standardization in its preparation. In certain instances, no statistically significant differences were observed between PRP and placebo in alleviating pain and enhancing joint function, particularly in advanced disease stages where cartilage regeneration is constrained [47].
Numerous clinical studies have examined the long-term effects of PRP therapy on knee OA, concentrating on symptom alleviation, cartilage preservation, and the diminution of surgical intervention necessity. Studies demonstrate that PRP therapy can offer prolonged pain alleviation and functional enhancement for as long as 12 months following treatment. The studies indicate that PRP injections resulted in substantial decreases in pain and enhancements in physical function among patients with knee OA over a 12-month duration [48]. Research lacks consensus regarding the duration of effects from PRP injections for knee OA. Certain studies indicate that PRP therapy may confer advantages for up to 12 months post-injection, yet reveal no additional benefits beyond 24 months [38].
Imaging studies have indicated that PRP treatment may aid in the preservation of cartilage. The studies indicated that PRP exhibited a chondroprotective effect, implying its potential to safeguard cartilage from degeneration in knee OA [39]. PRP has been linked to a reduced necessity for total knee replacement in patients with moderate OA by mitigating symptoms and maintaining joint integrity. The studies indicated that PRP is a viable management option for alleviating symptoms in knee OA, potentially postponing the necessity for surgical intervention [49]. The findings indicate that PRP therapy may provide enduring advantages in the management of knee OA, encompassing prolonged symptom alleviation, cartilage preservation, and a diminished probability of necessitating surgical procedures.
Stem cell therapies
Amid escalating challenges associated with knee OA treatment, stem cell therapies are emerging as a promising alternative, providing distinctive regenerative and immunomodulatory mechanisms. It is essential to examine the origins of these cells and their mechanisms of action intended for cartilage reconstruction, as well as to evaluate the clinical efficacy of these approaches within the realm of biological therapies.
Stem cells are gaining prominence as a novel approach in the biological treatment of knee OA, primarily owing to their regenerative capabilities and capacity to modulate inflammatory responses. The origin of stem cells is a crucial factor that influences their therapeutic properties and the accessibility of this treatment. Stem cells can be extracted from multiple sources, including bone marrow, adipose tissue, umbilical cord blood, or synovial membrane [50]. Each source possesses distinct properties that may influence their therapeutic efficacy. In the realm of prospective regenerative therapies, stem cells are pivotal, particularly those derived from adipose tissue or bone marrow (BM-MSC). Umbilical cord blood cells (UC-MSC) serve as an alternative source due to their significant regenerative capabilities and low immunogenicity, enabling their application in allogeneic therapies with minimal risk of immune rejection [51]. Clinical trials have confirmed that the administration of UC-MSCs for knee OA treatment leads to substantial enhancements in joint function and alleviation of pain. Repeated administrations of UC-MSCs resulted in superior pain alleviation and enhanced knee joint functionality relative to HA therapy, thereby affirming their therapeutic efficacy [52, 53]. The mechanisms of action of UC-MSCs encompass their capacity for chondrogenic differentiation and the secretion of growth factors that facilitate the regeneration of articular cartilage by mitigating inflammatory processes and reconstructing the extracellular matrix (Figure 2).
The variability in PRP preparation protocols, encompassing centrifugation techniques, leukocyte composition, and activation methods, intrapersonal and interpersonal differences in PRP composition, significantly influences the therapeutic efficacy. PRP preparation protocols influence the concentration of growth factors and, therefore, the efficacy of treatment [39]. Procedures for PRP activation, such as thrombin or calcium ion application, enhance the release of growth factors, potentially expediting cartilage tissue regeneration [40]. Furthermore, leukocytes in PRP may induce transient inflammation, necessitating additional investigation into the ideal formulation of the preparation. Research findings also indicate that leukocyte-poor PRP exhibits superior efficacy relative to leukocyte-rich PRP, attributed to a diminished risk of leukocyte-induced inflammation [41]. Furthermore, the assessment of the efficacy of distinct PRP types reveals that the leukocyte-poor variant exhibits a diminished risk of adverse effects and enhanced effectiveness in mitigating inflammation relative to leukocytogenic PRP. The administration protocols for PRP, encompassing single or multiple injections, are a crucial component of the therapy. Multiple PRP injections may yield more enduring therapeutic advantages than a solitary administration, indicating the necessity for enhanced standardization of treatment protocols [42]. It is essential to note that the efficacy of PRP therapy is contingent upon the disease stage, necessitating the implementation of suitable patient selection criteria. The repeated application of PRP at designated intervals, such as weekly or monthly, yields superior outcomes in alleviating pain and enhancing joint functionality relative to a singular treatment. The customization of injection protocols based on the patient’s age, disease stage, and comorbidities may substantially influence therapeutic efficacy. Repeated PRP administration has been demonstrated to facilitate the reconstruction of the extracellular matrix, resulting in sustained enhancement of knee joint condition. The variety of protocols underscores the necessity for standardization to attain consistent therapeutic outcomes.
PRP is an innovative approach employed in the management of knee OA, with its efficacy substantiated by numerous scientific studies. Patients receiving intra-articular PRP injections demonstrate a marked decrease in pain and enhancement in joint function relative to alternative therapeutic approaches, including HA or placebo [43, 44]. Research indicates that PRP is most advantageous in the early and mid-stages of knee OA, rendering it more appropriate for younger patients with less severe injuries. The benefits of PRP are further enhanced by its excellent safety profile, attributable to its autologous source. PRP possesses a favourable safety profile owing to its autologous nature, thereby mitigating the risk of immune responses or disease transmission [45]. Clinical studies validate the negligible risk of complications, including transient swelling or pain at the injection site, thereby enhancing patient acceptance of this therapy. This condition reduces the likelihood of immune responses and disease transmission. This fact enhances the acceptance of the therapy among patients and physicians, establishing PRP as a significant alternative in the management of knee OA. The significant efficacy of PRP in alleviating pain and inflammation renders it a notably advantageous alternative for patients who are intolerant to conventional anti-inflammatory medications [46]. Although there is substantial evidence supporting the efficacy of PRP, certain studies challenge its effectiveness, suggesting the potential influence of a placebo effect or inadequate standardization in its preparation. In certain instances, no statistically significant differences were observed between PRP and placebo in alleviating pain and enhancing joint function, particularly in advanced disease stages where cartilage regeneration is constrained [47].
Numerous clinical studies have examined the long-term effects of PRP therapy on knee OA, concentrating on symptom alleviation, cartilage preservation, and the diminution of surgical intervention necessity. Studies demonstrate that PRP therapy can offer prolonged pain alleviation and functional enhancement for as long as 12 months following treatment. The studies indicate that PRP injections resulted in substantial decreases in pain and enhancements in physical function among patients with knee OA over a 12-month duration [48]. Research lacks consensus regarding the duration of effects from PRP injections for knee OA. Certain studies indicate that PRP therapy may confer advantages for up to 12 months post-injection, yet reveal no additional benefits beyond 24 months [38].
Imaging studies have indicated that PRP treatment may aid in the preservation of cartilage. The studies indicated that PRP exhibited a chondroprotective effect, implying its potential to safeguard cartilage from degeneration in knee OA [39]. PRP has been linked to a reduced necessity for total knee replacement in patients with moderate OA by mitigating symptoms and maintaining joint integrity. The studies indicated that PRP is a viable management option for alleviating symptoms in knee OA, potentially postponing the necessity for surgical intervention [49]. The findings indicate that PRP therapy may provide enduring advantages in the management of knee OA, encompassing prolonged symptom alleviation, cartilage preservation, and a diminished probability of necessitating surgical procedures.
Stem cell therapies
Amid escalating challenges associated with knee OA treatment, stem cell therapies are emerging as a promising alternative, providing distinctive regenerative and immunomodulatory mechanisms. It is essential to examine the origins of these cells and their mechanisms of action intended for cartilage reconstruction, as well as to evaluate the clinical efficacy of these approaches within the realm of biological therapies.
Stem cells are gaining prominence as a novel approach in the biological treatment of knee OA, primarily owing to their regenerative capabilities and capacity to modulate inflammatory responses. The origin of stem cells is a crucial factor that influences their therapeutic properties and the accessibility of this treatment. Stem cells can be extracted from multiple sources, including bone marrow, adipose tissue, umbilical cord blood, or synovial membrane [50]. Each source possesses distinct properties that may influence their therapeutic efficacy. In the realm of prospective regenerative therapies, stem cells are pivotal, particularly those derived from adipose tissue or bone marrow (BM-MSC). Umbilical cord blood cells (UC-MSC) serve as an alternative source due to their significant regenerative capabilities and low immunogenicity, enabling their application in allogeneic therapies with minimal risk of immune rejection [51]. Clinical trials have confirmed that the administration of UC-MSCs for knee OA treatment leads to substantial enhancements in joint function and alleviation of pain. Repeated administrations of UC-MSCs resulted in superior pain alleviation and enhanced knee joint functionality relative to HA therapy, thereby affirming their therapeutic efficacy [52, 53]. The mechanisms of action of UC-MSCs encompass their capacity for chondrogenic differentiation and the secretion of growth factors that facilitate the regeneration of articular cartilage by mitigating inflammatory processes and reconstructing the extracellular matrix (Figure 2).
The synovial membrane and synovial fluid MSCs (sMSCs) confer significant chondrogenic potential to cells, as evidenced by research conducted on large animal models, which demonstrates their capacity for cartilage regeneration [54]. All sources of stem cells can differentiate into chondrocytes, facilitating the repair of damaged tissue by enhancing the production of type II collagen and aggrecan, essential components of the extracellular matrix [55]. The utilization of MSC is notably appealing owing to their facile acquisition and substantial proliferative capacity, rendering them a promising asset in regenerative therapy. BM-MSC, although exhibiting high regenerative efficacy, are constrained by more invasive harvesting techniques and a reduced quantity of accessible cells [56]. Additionally, stem cells demonstrate a paracrine effect by releasing bioactive factors, including cytokines and growth factors that regulate inflammatory processes and promote the proliferation of local chondrocytes, thereby enhancing tissue regeneration. Furthermore, the existence of bioactive elements like miRNAs and repair proteins in EVs facilitates cartilage tissue regeneration and mitigates its degradation, as evidenced by preclinical studies. The modulation of the local niche by MSCs includes the attenuation of pro-inflammatory cytokines like IL-1β and TNF-α, thereby mitigating symptoms of knee OA. These mechanisms facilitate chondrocyte proliferation and proteoglycan synthesis, resulting in enhanced integrity and function of articular cartilage. Clinical trial findings demonstrate that intra-articular injections of MSC result in diminished pain and enhanced biomechanical function of the knee joint, confirming their efficacy in OA treatment [57].
The application of MSCs via intra-articular injections demonstrates a distinct superiority over HA in alleviating pain and enhancing joint function, as corroborated by clinical trials [58]. Comparative analyses indicate that MSC provide a more enduring therapeutic effect than HA, particularly in advanced disease stages where conventional treatments are less efficacious. Repeated administration of MSCs results in prolonged enhancement of joint functionality, underscoring their potential in managing chronic degenerative diseases [59]. Clinical trial results concerning stem cells, specifically those derived from adipose tissue, BM-MSC, and UC-MSC, demonstrate their regenerative capacity and therapeutic efficacy in treating knee OA. Furthermore, the application of MSC has demonstrated enhancement in the histological outcomes of cartilage, suggesting reversible pathological alterations within the degenerative joint. The capacity of these cells to proliferate and differentiate into chondrocytes directly accounts for the therapeutic efficacy of aMSCs, as corroborated by numerous clinical observations [60, 61].
Viscosupplementation with HA
Viscosupplementation with HA is essential for treating knee OA, particularly for enhancing joint function and alleviating pain. HA is a crucial constituent of the extracellular matrix in synovial fluid, essential for the optimal functioning of the knee joint. Its presence guarantees enhanced viscoelastic characteristics of synovial fluid, resulting in diminished friction between cartilage surfaces and safeguarding the joint from mechanical stress. HA functions as a lubricant and shock-absorbing agent owing to its capacity to retain water and its distinctive molecular configuration that diminishes frictional forces [62]. Mechanical protection is especially crucial for patients with knee OA, as the gradual deterioration of cartilage results in pain and restricted mobility. HA facilitates natural regenerative mechanisms in the joint by prompting chondrocytes to synthesize proteoglycans and collagen, essential for reconstructing the extracellular matrix of cartilage (Figure 3).
The application of MSCs via intra-articular injections demonstrates a distinct superiority over HA in alleviating pain and enhancing joint function, as corroborated by clinical trials [58]. Comparative analyses indicate that MSC provide a more enduring therapeutic effect than HA, particularly in advanced disease stages where conventional treatments are less efficacious. Repeated administration of MSCs results in prolonged enhancement of joint functionality, underscoring their potential in managing chronic degenerative diseases [59]. Clinical trial results concerning stem cells, specifically those derived from adipose tissue, BM-MSC, and UC-MSC, demonstrate their regenerative capacity and therapeutic efficacy in treating knee OA. Furthermore, the application of MSC has demonstrated enhancement in the histological outcomes of cartilage, suggesting reversible pathological alterations within the degenerative joint. The capacity of these cells to proliferate and differentiate into chondrocytes directly accounts for the therapeutic efficacy of aMSCs, as corroborated by numerous clinical observations [60, 61].
Viscosupplementation with HA
Viscosupplementation with HA is essential for treating knee OA, particularly for enhancing joint function and alleviating pain. HA is a crucial constituent of the extracellular matrix in synovial fluid, essential for the optimal functioning of the knee joint. Its presence guarantees enhanced viscoelastic characteristics of synovial fluid, resulting in diminished friction between cartilage surfaces and safeguarding the joint from mechanical stress. HA functions as a lubricant and shock-absorbing agent owing to its capacity to retain water and its distinctive molecular configuration that diminishes frictional forces [62]. Mechanical protection is especially crucial for patients with knee OA, as the gradual deterioration of cartilage results in pain and restricted mobility. HA facilitates natural regenerative mechanisms in the joint by prompting chondrocytes to synthesize proteoglycans and collagen, essential for reconstructing the extracellular matrix of cartilage (Figure 3).
Research indicates that HA can regulate the activity of degradation enzymes, including MMPs, and pro-inflammatory cytokines, such as IL-1β and TNF-α, thereby mitigating the destructive processes in cartilage tissue. Simultaneously, diminishing the activity of these cytokines mitigates additional cartilage deterioration, facilitating enhanced equilibrium in the joint milieu [63]. Studies have confirmed the efficacy of HA in articular cartilage regeneration, demonstrating an increase in proteoglycan and type II collagen synthesis, which resulted in enhanced biomechanics of the knee joint. HA can attach to specific receptors present in various cells, including cluster determinant 44, intracellular adhesion molecule-1, and the receptor for hyaluronate-mediated motility. This binding initiates multiple intracellular signalling events, including cytokine release and activation of cell cycle proteins. The ramifications of these interactions are to enhance cellular functional activities, including migration and proliferation. In osteoarthritic joints, synovial fluid exhibits a diminished concentration of HA compared to healthy joints; thus, intra-articular administration of exogenous HA can reinstate its viscoelastic characteristics [64]. In vivo and in vitro studies have demonstrated diverse physiological effects of exogenous HA that may oppose the mechanisms implicated in OA pathogenesis [63]. Exogenous HA can augment chondrocyte production of endogenous HA and proteoglycans, inhibit cartilage degradation, and facilitate its regeneration. Furthermore, it can diminish the synthesis of proinflammatory mediators and MMPs, as well as alleviate nerve impulses and sensitivity related to OA pain.
The efficacy of intra-articular therapies utilizing HA, referred to as viscosupplementation, is contingent upon the specific preparation employed and its administration protocols. Clinical trials on viscosupplementation indicate that HA effectively alleviates pain and enhances knee joint function in the short to medium term; however, its efficacy is inferior to other biological methods, such as PRP [65]. The restricted efficacy of HA in advanced disease stages indicates that it should primarily be utilized in the early phases of joint degeneration, where its anti-inflammatory and lubricating attributes may be most effective. Tailoring HA therapy to the patient’s requirements, including age, disease stage, or physical activity level, may enhance the clinical efficacy of this approach. Although the therapeutic effects are not long-lasting and necessitate repeated injections at designated intervals, HA viscosupplementation demonstrates a positive safety profile [66]. Adverse effects, including localized swelling or discomfort at the injection site, are infrequent and typically temporary, rendering this therapy a secure alternative for patient’s ineligible for more invasive interventions. HA, as a natural constituent of synovial fluid, elicits no immune response, which constitutes its primary advantage over alternative methods. Research indicates that multiple HA injections typically yield greater pain alleviation and enhanced joint functionality than single doses [67]. The absence of standardized therapeutic protocols results in variations in clinical outcomes, underscoring the necessity to establish optimal dosages and administration frequency. Moreover, studies indicate that the integration of HA with other biological treatments, such as PRP, may enhance its efficacy, necessitating further examination within the framework of combined therapies [68]. HA administration protocols are typically based on treatment regimens of one to three injections at weekly intervals, which allows for maximizing therapeutic effects [69]. Differences between preparations, such as molecular weight or degree of cross-linking, affect the duration of action and effectiveness of therapy, which requires individualization of treatment depending on the patient’s needs.
Safety and future of biological therapies
The safety of biological therapies for knee OA treatment is a crucial factor in determining suitable therapeutic options.
The safety profile of specific biological therapies for knee OA is crucial as it influences the potential risk of adverse effects and patients’ tolerance to particular treatment modalities. A meta-analysis by Meng et al. (2022) reveals that biological therapies, while demonstrating considerable therapeutic advantages in alleviating pain and enhancing joint function, carry an increased risk of side effects relative to placebo [70]. The studies indicated that the relative risk (RR) of experiencing any side effects is 1.09, while the RR for treatment discontinuation due to these effects is 1.39. The elevated risks linked to biologic therapies highlight the necessity for meticulous patient selection and ongoing enhancement of protocols. Nerve growth factor (NGF) inhibitors, while effective in alleviating pain, exhibit a notably elevated risk of adverse effects, including nerve dysfunction, thereby constraining their broad application. In contrast to NGF inhibitors, IL-1 and TNF-α inhibitors exhibit a comparatively superior safety profile, potentially rendering them more appropriate for patients necessitating treatment with a diminished risk of adverse effects [71]. The safety of PRP therapy presents certain limitations. According to the research conducted by Nagao et al., the local administration of PRP may induce transient inflammation due to the activation of growth factors, including VEGF [72]. Elevated VEGF, linked to a transient rise in catabolic activities within chondrocytes, may result in detrimental consequences manifesting as cartilage tissue damage [73]. Excessively elevated levels of phosphorylated VEGFR2 in chondrocytes and synovial joint cells may result in degenerative alterations of cartilage, impeding regeneration. Consequently, it is essential to standardize PRP preparation protocols, including the regulation of growth factor concentrations such as VEGF, to mitigate the risk of catabolic reactions in the joint. Furthermore, leukocyte-poor PRP may be preferable for patients in the early stages of knee joint degeneration, as the diminished concentration of pro-inflammatory cytokines mitigates the risk of inflammatory responses. Stem cell therapies possess distinct safety constraints. In numerous cell therapies, the introduced cells swiftly experience apoptosis, constraining their efficacy to a transient therapeutic impact [74]. The elevated expenses of therapy due to sophisticated cell production and storage technologies pose a significant challenge. A notable risk is the potential for aberrant differentiation of cells into tissue types other than cartilage, which could result in the development of fibrous tissue instead of damaged cartilage. To mitigate these risks, innovative techniques are being devised to enhance cell viability, including the application of biological carriers or hydrogels that prolong the therapeutic efficacy of stem cells [75]. Utilizing allogeneic stem cells, notwithstanding elevated expenses, may diminish the likelihood of immune rejection and enhance therapeutic efficacy. HA is characterized by its advantageous safety profile relative to other biological therapies. Intra-articular injections of HA infrequently result in adverse effects, typically confined to transient swelling or discomfort at the injection site. Furthermore, HA, as a natural constituent of synovial fluid, does not elicit an immune response, rendering it a notably safe option for patients with contraindications to more advanced therapies. The sole limitation of this therapy is its brief duration, necessitating frequent injections, which may be uncomfortable for certain patients. HA therapy is especially efficacious in the early and intermediate phases of OA, thereby enhancing its utility for mild to moderate pain symptoms [76].
The choice of suitable biological therapy for knee OA treatment necessitates consideration of the disease’s progression stage. In the early phases of the disease, PRP demonstrates significant efficacy, as substantiated by clinical trials and MRI imaging [77]. PRP functions mainly by regulating inflammation, thereby reducing cartilage deterioration and facilitating its regeneration. Consequently, in later stages of the disease, therapies utilizing stem cells, such as MSC, may demonstrate greater efficacy. Their mechanisms of action encompass regenerative capabilities and immunomodulatory characteristics, facilitating the reconstruction of cartilage tissue structures and the alleviation of inflammation [78]. HA, as a constituent of synovial fluid, does not elicit immune responses, rendering it suitable for individuals with autoimmune disorders. PRP, while effective, poses a risk of short-term inflammation due to the activation of growth factors like VEGF. Stem cell therapies, while promising, may induce side effects such as aberrant cell differentiation, potentially leading to the development of fibrous tissue instead of damaged cartilage [79]. Consequently, when the risk of adverse effects linked to more advanced techniques is excessively elevated, HA is advised. While PRP and MSC therapies may provide more enduring therapeutic outcomes, the safety of HA renders this approach especially appealing for patients with contraindications to more invasive treatments. These findings underscore the necessity of tailoring therapy selection according to the extent of joint damage, thereby optimizing therapeutic outcomes. However, the ineffectiveness of PRP in advanced disease stages, characterized by significant cartilage damage, highlights the limitations of this treatment in more severe cases.
Economic factors significantly influence therapeutic decisions. HA is considerably less expensive than PRP and stem cell therapies, rendering it more accessible to patients with constrained finances or residing in countries with underfunded healthcare systems [80]. PRP, notwithstanding elevated expenses, may yield long-term profitability by potentially postponing the necessity for invasive procedures like arthroplasty. Nonetheless, stem cells, owing to the intricate procurement process and absence of standardization, continue to be the costliest alternative, thereby constraining their extensive application. Consequently, the choice to employ costlier therapies, such as MSC, must consider their prospective regenerative advantages and the longevity of therapeutic outcomes. Nonetheless, infrastructural limitations in underdeveloped healthcare systems may exacerbate disparities in access to advanced biological therapies.
Customizing treatment according to patient attributes, including age, physical activity level, and comorbidities, is a crucial component of effective therapy. Patients who are younger and more physically active exhibit superior responses to PRP, attributable to the enhanced regenerative capacity of growth factors in plasma. Women, although they report pain more frequently, demonstrate superior therapeutic outcomes following PRP treatment, potentially attributable to hormonal disparities and their influence on cartilage regeneration. MSC therapies may be more appropriate for patients with advanced degenerative changes, particularly when conventional treatments fail to yield anticipated outcomes. Comorbid conditions, such as obesity or rheumatoid arthritis, may further diminish the efficacy of biological therapies, necessitating a personalized patient evaluation prior to determining the most suitable treatment approach. Dynamic modification of treatment protocols according to the body’s response enhances therapeutic efficacy and reduces the likelihood of adverse effects.
Conclusion
This study underscores the significance of tailoring therapy to accommodate the unique needs of patients, their health status, and the progression of the disease. This approach enables the optimal utilization of available biological methods to enhance the QoL for patients with knee OA. The optimism conveyed in the work regarding the advancement of contemporary treatment methodologies signifies the promise of regenerative medicine, which could transform the management of degenerative diseases in the near future. The analysis of various biological therapies for knee OA provides a clear assessment of the efficacy and limitations of each approach, thereby addressing the research question concerning the extent of clinical and functional improvement in patients undergoing these treatments.
The study found that PRP treatment reduces pain and improves knee function, especially in early degenerative disease. PRP, rich in growth factors including TGF-β and PDGF, promotes cartilage repair and reduces joint inflammation. Clinical investigations have shown that PRP offers long-term benefits, especially for younger patients with mild cartilage degradation. The need to standardize techniques, including leukocyte composition and activity, limits the use of this treatment. PRP’s effectiveness in late illness stages is limited, underscoring the need for a personalized treatment strategy and more advanced regeneration procedures. Due to their immunomodulatory and chondrocyte-differentiating qualities, stem cell treatments are highly regenerative. Stem cells promote cartilage regeneration by increasing type II collagen and aggrecan synthesis while reducing pro-inflammatory cytokines like IL-1β and TNF-α. The continuous improvement of cartilage architecture and pain relief make this therapy a promising choice for severe joint degeneration when traditional therapies fail. Due to high prices, complicated cell separation, and aberrant cell differentiation, this treatment is difficult. Additionally, the lack of defined therapy regimens and limited access to long-term data require more study to improve therapeutic safety and predictability. HA is inferior to PRP and stem cells in cartilage repair; nevertheless, it is a useful treatment in early to moderate degenerative joint disease. HA increases synovial fluid viscosity and reduces cartilage surface friction, relieving joint discomfort and improving biomechanical performance. This approach has been shown to work in clinical studies, and its natural origin and safety make it a good choice for individuals who cannot tolerate more sophisticated biological medicines. The short duration of therapeutic benefits and repeated injections restrict this approach, especially in late degenerative alterations.
Upon analyzing all three methods, it is evident that none serves as a universal solution for all patients with knee OA. Therapies like PRP and stem cells possess greater regenerative potential; however, their application necessitates additional research due to technological and economic constraints, as well as a lack of standardization. Consequently, HA, although less effective in regeneration, continues to be a significant component of the treatment strategy, particularly for patients who are ineligible for more advanced therapies.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and funding acquisition: Marcin Tomaszewski and Lukasz Szarpak; Methodology and investigation: Marcin Tomaszewski, Michal Pruc, and Lukasz Szarpak; Writing the original draft: Marcin Tomaszewski, Piotr Fudalej, Michal Pruc, Lukasz Szarpak, and Mahdi Al-Jeabory; Resources: Marcin Tomaszewski, Michal Pruc, Piotr Fudalej, and Mahdi Al-Jeabory; Supervision: Mahdi Al-Jeabory, Lukasz Szarpak, and Piotr Fudalej; Review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
The efficacy of intra-articular therapies utilizing HA, referred to as viscosupplementation, is contingent upon the specific preparation employed and its administration protocols. Clinical trials on viscosupplementation indicate that HA effectively alleviates pain and enhances knee joint function in the short to medium term; however, its efficacy is inferior to other biological methods, such as PRP [65]. The restricted efficacy of HA in advanced disease stages indicates that it should primarily be utilized in the early phases of joint degeneration, where its anti-inflammatory and lubricating attributes may be most effective. Tailoring HA therapy to the patient’s requirements, including age, disease stage, or physical activity level, may enhance the clinical efficacy of this approach. Although the therapeutic effects are not long-lasting and necessitate repeated injections at designated intervals, HA viscosupplementation demonstrates a positive safety profile [66]. Adverse effects, including localized swelling or discomfort at the injection site, are infrequent and typically temporary, rendering this therapy a secure alternative for patient’s ineligible for more invasive interventions. HA, as a natural constituent of synovial fluid, elicits no immune response, which constitutes its primary advantage over alternative methods. Research indicates that multiple HA injections typically yield greater pain alleviation and enhanced joint functionality than single doses [67]. The absence of standardized therapeutic protocols results in variations in clinical outcomes, underscoring the necessity to establish optimal dosages and administration frequency. Moreover, studies indicate that the integration of HA with other biological treatments, such as PRP, may enhance its efficacy, necessitating further examination within the framework of combined therapies [68]. HA administration protocols are typically based on treatment regimens of one to three injections at weekly intervals, which allows for maximizing therapeutic effects [69]. Differences between preparations, such as molecular weight or degree of cross-linking, affect the duration of action and effectiveness of therapy, which requires individualization of treatment depending on the patient’s needs.
Safety and future of biological therapies
The safety of biological therapies for knee OA treatment is a crucial factor in determining suitable therapeutic options.
The safety profile of specific biological therapies for knee OA is crucial as it influences the potential risk of adverse effects and patients’ tolerance to particular treatment modalities. A meta-analysis by Meng et al. (2022) reveals that biological therapies, while demonstrating considerable therapeutic advantages in alleviating pain and enhancing joint function, carry an increased risk of side effects relative to placebo [70]. The studies indicated that the relative risk (RR) of experiencing any side effects is 1.09, while the RR for treatment discontinuation due to these effects is 1.39. The elevated risks linked to biologic therapies highlight the necessity for meticulous patient selection and ongoing enhancement of protocols. Nerve growth factor (NGF) inhibitors, while effective in alleviating pain, exhibit a notably elevated risk of adverse effects, including nerve dysfunction, thereby constraining their broad application. In contrast to NGF inhibitors, IL-1 and TNF-α inhibitors exhibit a comparatively superior safety profile, potentially rendering them more appropriate for patients necessitating treatment with a diminished risk of adverse effects [71]. The safety of PRP therapy presents certain limitations. According to the research conducted by Nagao et al., the local administration of PRP may induce transient inflammation due to the activation of growth factors, including VEGF [72]. Elevated VEGF, linked to a transient rise in catabolic activities within chondrocytes, may result in detrimental consequences manifesting as cartilage tissue damage [73]. Excessively elevated levels of phosphorylated VEGFR2 in chondrocytes and synovial joint cells may result in degenerative alterations of cartilage, impeding regeneration. Consequently, it is essential to standardize PRP preparation protocols, including the regulation of growth factor concentrations such as VEGF, to mitigate the risk of catabolic reactions in the joint. Furthermore, leukocyte-poor PRP may be preferable for patients in the early stages of knee joint degeneration, as the diminished concentration of pro-inflammatory cytokines mitigates the risk of inflammatory responses. Stem cell therapies possess distinct safety constraints. In numerous cell therapies, the introduced cells swiftly experience apoptosis, constraining their efficacy to a transient therapeutic impact [74]. The elevated expenses of therapy due to sophisticated cell production and storage technologies pose a significant challenge. A notable risk is the potential for aberrant differentiation of cells into tissue types other than cartilage, which could result in the development of fibrous tissue instead of damaged cartilage. To mitigate these risks, innovative techniques are being devised to enhance cell viability, including the application of biological carriers or hydrogels that prolong the therapeutic efficacy of stem cells [75]. Utilizing allogeneic stem cells, notwithstanding elevated expenses, may diminish the likelihood of immune rejection and enhance therapeutic efficacy. HA is characterized by its advantageous safety profile relative to other biological therapies. Intra-articular injections of HA infrequently result in adverse effects, typically confined to transient swelling or discomfort at the injection site. Furthermore, HA, as a natural constituent of synovial fluid, does not elicit an immune response, rendering it a notably safe option for patients with contraindications to more advanced therapies. The sole limitation of this therapy is its brief duration, necessitating frequent injections, which may be uncomfortable for certain patients. HA therapy is especially efficacious in the early and intermediate phases of OA, thereby enhancing its utility for mild to moderate pain symptoms [76].
The choice of suitable biological therapy for knee OA treatment necessitates consideration of the disease’s progression stage. In the early phases of the disease, PRP demonstrates significant efficacy, as substantiated by clinical trials and MRI imaging [77]. PRP functions mainly by regulating inflammation, thereby reducing cartilage deterioration and facilitating its regeneration. Consequently, in later stages of the disease, therapies utilizing stem cells, such as MSC, may demonstrate greater efficacy. Their mechanisms of action encompass regenerative capabilities and immunomodulatory characteristics, facilitating the reconstruction of cartilage tissue structures and the alleviation of inflammation [78]. HA, as a constituent of synovial fluid, does not elicit immune responses, rendering it suitable for individuals with autoimmune disorders. PRP, while effective, poses a risk of short-term inflammation due to the activation of growth factors like VEGF. Stem cell therapies, while promising, may induce side effects such as aberrant cell differentiation, potentially leading to the development of fibrous tissue instead of damaged cartilage [79]. Consequently, when the risk of adverse effects linked to more advanced techniques is excessively elevated, HA is advised. While PRP and MSC therapies may provide more enduring therapeutic outcomes, the safety of HA renders this approach especially appealing for patients with contraindications to more invasive treatments. These findings underscore the necessity of tailoring therapy selection according to the extent of joint damage, thereby optimizing therapeutic outcomes. However, the ineffectiveness of PRP in advanced disease stages, characterized by significant cartilage damage, highlights the limitations of this treatment in more severe cases.
Economic factors significantly influence therapeutic decisions. HA is considerably less expensive than PRP and stem cell therapies, rendering it more accessible to patients with constrained finances or residing in countries with underfunded healthcare systems [80]. PRP, notwithstanding elevated expenses, may yield long-term profitability by potentially postponing the necessity for invasive procedures like arthroplasty. Nonetheless, stem cells, owing to the intricate procurement process and absence of standardization, continue to be the costliest alternative, thereby constraining their extensive application. Consequently, the choice to employ costlier therapies, such as MSC, must consider their prospective regenerative advantages and the longevity of therapeutic outcomes. Nonetheless, infrastructural limitations in underdeveloped healthcare systems may exacerbate disparities in access to advanced biological therapies.
Customizing treatment according to patient attributes, including age, physical activity level, and comorbidities, is a crucial component of effective therapy. Patients who are younger and more physically active exhibit superior responses to PRP, attributable to the enhanced regenerative capacity of growth factors in plasma. Women, although they report pain more frequently, demonstrate superior therapeutic outcomes following PRP treatment, potentially attributable to hormonal disparities and their influence on cartilage regeneration. MSC therapies may be more appropriate for patients with advanced degenerative changes, particularly when conventional treatments fail to yield anticipated outcomes. Comorbid conditions, such as obesity or rheumatoid arthritis, may further diminish the efficacy of biological therapies, necessitating a personalized patient evaluation prior to determining the most suitable treatment approach. Dynamic modification of treatment protocols according to the body’s response enhances therapeutic efficacy and reduces the likelihood of adverse effects.
Conclusion
This study underscores the significance of tailoring therapy to accommodate the unique needs of patients, their health status, and the progression of the disease. This approach enables the optimal utilization of available biological methods to enhance the QoL for patients with knee OA. The optimism conveyed in the work regarding the advancement of contemporary treatment methodologies signifies the promise of regenerative medicine, which could transform the management of degenerative diseases in the near future. The analysis of various biological therapies for knee OA provides a clear assessment of the efficacy and limitations of each approach, thereby addressing the research question concerning the extent of clinical and functional improvement in patients undergoing these treatments.
The study found that PRP treatment reduces pain and improves knee function, especially in early degenerative disease. PRP, rich in growth factors including TGF-β and PDGF, promotes cartilage repair and reduces joint inflammation. Clinical investigations have shown that PRP offers long-term benefits, especially for younger patients with mild cartilage degradation. The need to standardize techniques, including leukocyte composition and activity, limits the use of this treatment. PRP’s effectiveness in late illness stages is limited, underscoring the need for a personalized treatment strategy and more advanced regeneration procedures. Due to their immunomodulatory and chondrocyte-differentiating qualities, stem cell treatments are highly regenerative. Stem cells promote cartilage regeneration by increasing type II collagen and aggrecan synthesis while reducing pro-inflammatory cytokines like IL-1β and TNF-α. The continuous improvement of cartilage architecture and pain relief make this therapy a promising choice for severe joint degeneration when traditional therapies fail. Due to high prices, complicated cell separation, and aberrant cell differentiation, this treatment is difficult. Additionally, the lack of defined therapy regimens and limited access to long-term data require more study to improve therapeutic safety and predictability. HA is inferior to PRP and stem cells in cartilage repair; nevertheless, it is a useful treatment in early to moderate degenerative joint disease. HA increases synovial fluid viscosity and reduces cartilage surface friction, relieving joint discomfort and improving biomechanical performance. This approach has been shown to work in clinical studies, and its natural origin and safety make it a good choice for individuals who cannot tolerate more sophisticated biological medicines. The short duration of therapeutic benefits and repeated injections restrict this approach, especially in late degenerative alterations.
Upon analyzing all three methods, it is evident that none serves as a universal solution for all patients with knee OA. Therapies like PRP and stem cells possess greater regenerative potential; however, their application necessitates additional research due to technological and economic constraints, as well as a lack of standardization. Consequently, HA, although less effective in regeneration, continues to be a significant component of the treatment strategy, particularly for patients who are ineligible for more advanced therapies.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and funding acquisition: Marcin Tomaszewski and Lukasz Szarpak; Methodology and investigation: Marcin Tomaszewski, Michal Pruc, and Lukasz Szarpak; Writing the original draft: Marcin Tomaszewski, Piotr Fudalej, Michal Pruc, Lukasz Szarpak, and Mahdi Al-Jeabory; Resources: Marcin Tomaszewski, Michal Pruc, Piotr Fudalej, and Mahdi Al-Jeabory; Supervision: Mahdi Al-Jeabory, Lukasz Szarpak, and Piotr Fudalej; Review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
References:
- Vina ER, Kwoh CK. Epidemiology of osteoarthritis: Literature update. Current Opinion in Rheumatology. 2018; 30:160-7. [DOI:10.1097/BOR.0000000000000479] [PMID]
- GBD 2021 Osteoarthritis Collaborators. Global, regional, and national burden of osteoarthritis, 1990-2020 and projections to 2050: A systematic analysis for the global burden of disease study 2021. The Lancet Rheumatology Home Page. 2023; 5:e508-22. [Link]
- Wojcieszek A, Kurowska A, Majda A, Liszka H, Gądek A. The impact of chronic pain, stiffness and difficulties in performing daily activities on the quality of life of older patients with knee osteoarthritis. International Journal of Environmental Research and Public Health. 2022; 19:16815. [DOI:10.3390/ijerph192416815] [PMID]
- Shumnalieva R, Kotov G, Monov S. Obesity-related knee osteoarthritis-current concepts. Life. 2023; 13:1650. [DOI:10.3390/life13081650] [PMID]
- de Rezende MU, de Campos GC. Is osteoarthritis a mechanical or inflammatory disease? Revista Brasileira de Ortopedia. 2013; 48:471-4. [DOI:10.1016/j.rboe.2013.12.002] [PMID]
- Aubourg G, Rice SJ, Bruce-Wootton P, Loughlin J. Genetics of osteoarthritis. Osteoarthritis and Cartilage. 2022; 30:636-49. [DOI:10.1016/j.joca.2021.03.002] [PMID]
- Chow YY, Chin KY. The Role of Inflammation in the Pathogenesis of Osteoarthritis. Mediators of Inflammation. 2020; 2020:8293921. [DOI:10.1155/2020/8293921] [PMID]
- Goldring MB. Articular cartilage degradation in osteoarthritis. HSS Journal. 2012; 8:7-9. [DOI:10.1007/s11420-011-9250-z] [PMID]
- Bacon K, LaValley MP, Jafarzadeh SR, Felson D. Does cartilage loss cause pain in osteoarthritis and if so, how much? Annals of the Rheumatic Diseases. 2020; 79:1105-10. [DOI:10.1136/annrheumdis-2020-217363] [PMID]
- Junker S, Krumbholz G, Frommer KW, Rehart S, Steinmeyer J, Rickert M, et al. Differentiation of osteophyte types in osteoarthritis - proposal of a histological classification. Joint Bone Spine. 2016; 83: 63-7. [DOI:10.1016/j.jbspin.2015.04.008] [PMID]
- Ni R, Guo XE, Yan C, Wen C. Hemodynamic stress shapes subchondral bone in osteoarthritis: An emerging hypothesis. Journal of Orthopaedic Translation. 2021; 32:85-90. [DOI:10.1016/j.jot.2021.11.007] [PMID]
- Bindu S, Mazumder S, Bandyopadhyay U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochemical Pharmacology. 2020; 180:114147. [DOI:10.1016/j.bcp.2020.114147] [PMID]
- Stone S, Malanga GA, Capella T. Corticosteroids: Review of the History, the Effectiveness, and Adverse Effects in the Treatment of Joint Pain. Pain Physician. 2021; 24: S233-S246. [DOI:10.36076/ppj.2021.24.S233-S246]
- Kapoor M, Martel-Pelletier J, Lajeunesse D, Pelletier JP, Fahmi H. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nature Reviews Rheumatology. 2011; 7: 33-42. [DOI:10.1038/nrrheum.2010.196] [PMID]
- Mukherjee A, Das B. The role of inflammatory mediators and matrix metalloproteinases (MMPs) in the progression of osteoarthritis. Biomaterials and Biosystems. 2024; 13:100090. [DOI:10.1016/j.bbiosy.2024.100090] [PMID]
- Wojdasiewicz P, Poniatowski ŁA, Szukiewicz D. The role of inflammatory and anti-inflammatory cytokines in the pathogenesis of osteoarthritis. Mediators Inflamm. 2014; 2014: 561459. [DOI:10.1155/2014/561459] [PMID]
- Zahan OM, Serban O, Gherman C, Fodor D. The evaluation of oxidative stress in osteoarthritis. Medicine and Pharmacy Reports. 2020; 93:12-22. [DOI:10.15386/mpr-1422] [PMID]
- Nees TA, Rosshirt N, Zhang JA, Reiner T, Sorbi R, Tripel E, et al. Synovial cytokines significantly correlate with osteoarthritis-related knee pain and disability: Inflammatory mediators of potential clinical relevance.Journal of Clinical Medicine. 2019; 8:1343. [DOI:10.3390/jcm8091343] [PMID]
- Loffek S., Schilling O., Franzke C.-W. Biological role of matrix metalloproteinases: A critical balance. European Respiratory Journal. 2011; 38:191-208. [DOI:10.1183/09031936.00146510] [PMID]
- Sahin N, Yesil H. Regenerative methods in osteoarthritis. Best Practice & Research Clinical Rheumatology. 2023; 37:101824. [DOI:10.1016/j.berh.2023.101824] [PMID]
- Sulaiman SB, Chowdhury SR, Busra MFBM, Abdul Rani RB, Mohamad Yahaya NHB, Tabata Y, et al. Type II collagen-conjugated mesenchymal stem cells micromass for articular tissue targeting. Biomedicines. 2021; 9:880. [DOI:10.3390/biomedicines9080880] [PMID]
- Kristjánsson B, Honsawek S. Mesenchymal stem cells for cartilage regeneration in osteoarthritis. World Journal of Orthopedics. 2017; 8:674-80. [DOI:10.5312/wjo.v8.i9.674] [PMID]
- Lee WY, Wang B. Cartilage repair by mesenchymal stem cells: Clinical trial update and perspectives. Journal of Orthopaedic Translation. 2017; 9:76-88. [DOI:10.1016/j.jot.2017.03.005] [PMID]
- Zhou Y, Wang T, Hamilton JL, Chen D. Wnt/β-catenin signaling in osteoarthritis and in other forms of arthritis. Current Rheumatology Reports. 2017; 19:53. [DOI:10.1007/s11926-017-0679-z] [PMID]
- Wang X, Guan Y, Xiang S, Clark KL, Alexander PG, Simonian LE, et al. Role of canonical wnt/β-catenin pathway in regulating chondrocytic hypertrophy in mesenchymal stem cell-based cartilage tissue engineering. Frontiers in Cell and Developmental Biology. 2022; 10:812081. [DOI:10.3389/fcell.2022.812081] [PMID]
- Blaga FN, Nutiu AS, Lupsa AO, Ghiurau NA, Vlad SV, Ghitea TC. Exploring platelet-rich plasma therapy for knee osteoarthritis: an in-depth analysis. Journal of Functional Biomaterials. 2024; 15:221. [DOI:10.3390/jfb15080221] [PMID]
- Szwedowski D, Szczepanek J, Paczesny Ł, Zabrzyński J, Gagat M, Mobasheri A, et al. The effect of platelet-rich plasma on the intra-articular microenvironment in knee osteoarthritis. International Journal of Molecular Sciences. 2021; 22:5492. [DOI:10.3390/ijms22115492] [PMID]
- Gupta A, Jeyaraman M, Potty AG. Leukocyte-rich vs. leukocyte-poor platelet-rich plasma for the treatment of knee osteoarthritis. Biomedicines. 2023; 11:141. [DOI:10.3390/biomedicines11010141]
- Yoshioka T, Arai N, Sugaya H, Taniguchi Y, Kanamori A, Gosho M, et al. The effectiveness of leukocyte-poor platelet-rich plasma injections for symptomatic mild to moderate osteoarthritis of the knee with joint effusion or bone marrow lesions in a japanese population: A randomized, double-blind, placebo-controlled clinical trial. The American Journal of Sports Medicine. 2024; 52:2493-502. [DOI:10.1177/03635465241263073] [PMID]
- Nie LY, Zhao K, Ruan J, Xue J. Effectiveness of platelet-rich plasma in the treatment of knee osteoarthritis: A meta-analysis of randomized controlled clinical trials. Orthopaedic Journal of Sports Medicine. 2021; 9:2325967120973284. [DOI:10.1177/2325967120973284] [PMID]
- Altman RD, Manjoo A, Fierlinger A, Niazi F, Nicholls M. The mechanism of action for hyaluronic acid treatment in the osteoarthritic knee: A systematic review. BMC Musculoskeletal Disorders. 2015; 16: 321. [DOI:10.1186/s12891-015-0775-z] [PMID]
- Lee CH, Chiang CF, Kuo FC, Su SC, Huang CL, Liu JS, et al. High-molecular-weight hyaluronic acid inhibits il-1β-induced synovial inflammation and macrophage polarization through the GRP78-NF-κB signaling pathway. International Journal of Molecular Sciences. 2021; 22:11917. [DOI:10.3390/ijms222111917] [PMID]
- Roseti L, Desando G, Cavallo C, Petretta M, Grigolo B. Articular cartilage regeneration in osteoarthritis. Cells. 2019; 8:1305. [DOI:10.3390/cells8111305] [PMID]
- Sengprasert P, Kamenkit O, Tanavalee A, Reantragoon R. The immunological facets of chondrocytes in osteoarthritis: A narrative review. The Journal of Rheumatology. 2023; 816- 2023. [DOI:10.3899/jrheum.2023-0816] [PMID]
- Ma K, Singh G, Wang J, O-Sullivan I, Votta-Velis G, Bruce B, et al. Targeting vascular endothelial growth factor receptors as a therapeutic strategy for osteoarthritis and associated pain. International Journal of Biological Sciences. 2023; 19:675-90. [DOI:10.7150/ijbs.79125] [PMID]
- More S, Kotiya A, Kotia A, Ghosh SK, Spyrou LA, Sarris IE. Rheological properties of synovial fluid due to viscosupplements: A review for osteoarthritis remedy. Computer Methods and Programs in Biomedicine. 2020; 196:105644. [DOI:10.1016/j.cmpb.2020.105644] [PMID]
- Louis ML, Magalon J, Jouve E, Bornet CE, Mattei JC, Chagnaud C, et al. Growth factors levels determine efficacy of platelets rich plasma injection in knee osteoarthritis: A randomized double blind noninferiority trial compared with viscosupplementation. Arthroscopy. 2018; 34:1530-40.e2. [DOI:10.1016/j.arthro.2017.11.035] [PMID]
- Rodríguez-Merchán EC. Intra-articular platelet-rich plasma injections in knee osteoarthritis: A review of their current molecular mechanisms of action and their degree of efficacy. International Journal of Molecular Sciences. 2022; 23:1301. [DOI:10.3390/ijms23031301]
- Bansal H, Leon J, Pont JL, Wilson DA, Bansal A, Agarwal D, et al. Platelet-rich plasma (PRP) in osteoarthritis (OA) knee: Correct dose critical for long term clinical efficacy. Scientific Reports. 2021; 11:3971. [DOI:10.1038/s41598-021-98365-2] [PMID]
- Rosenthal AK, Gohr CM, Uzuki M, Masuda I. Osteopontin promotes pathologic mineralization in articular cartilage. Matrix Biology. 2007; 26:96-105. [DOI:10.1016/j.matbio.2006.10.004] [PMID]
- Simental-Mendía M, Vílchez-Cavazos JF, Peña-Martínez VM, Said-Fernández S, Lara-Arias J, Martínez-Rodríguez HG. Leukocyte-poor platelet-rich plasma is more effective than the conventional therapy with acetaminophen for the treatment of early knee osteoarthritis. Archives of Orthopaedic and Trauma Surgery. 2016; 136:1723-32. [DOI:10.1007/s00402-016-2545-2] [PMID]
- Partan RU, Putra KM, Hafizzanovian H, Darma S, Reagan M, Muthia P, et al. Clinical outcome of multiple platelet-rich plasma injection and correlation with PDGF-BB in the treatment of knee osteoarthritis. Journal of Personalized Medicine. 2024; 14:183. [DOI:10.3390/jpm14020183] [PMID]
- Oeding JF, Varady NH, Fearington FW, Pareek A, Strickland SM, Nwachukwu BU, et al. Platelet-rich plasma versus alternative injections for osteoarthritis of the knee: A systematic review and statistical fragility index-based meta-analysis of randomized controlled trials. The American Journal of Sports Medicine. 2024; 52: 3147-3160. [DOI:10.1177/03635465231224463] [PMID]
- Dai WL, Zhou AG, Zhang H, Zhang J. Efficacy of platelet-rich plasma in the treatment of knee osteoarthritis: A meta-analysis of randomized controlled trials. Arthroscopy. 2017; 33: 659-670.e1. [DOI:10.1016/j.arthro.2016.09.024] [PMID]
- Reginster JY, Bruyère O, Conaghan PG, McAlindon T, Cooper C. Importance of safety in the management of osteoarthritis and the need for updated meta-analyses and recommendations for reporting of harms. Drugs Aging. 2019; 36:3-6. [DOI:10.1007/s40266-019-00659-8] [PMID]
- Kawano MM, Araújo IL, Castro MC, Matos MA. Assessment of quality of life in patients with knee osteoarthritis. Acta Ortopédica Brasileira. 2015; 23:307-10. [DOI:10.1590/1413-785220152306150596] [PMID]
- Vilchez-Cavazos F, Blázquez-Saldaña J, Gamboa-Alonso AA, Peña-Martínez VM, Acosta-Olivo CA, Sánchez-García A, et al. The use of platelet-rich plasma in studies with early knee osteoarthritis versus advanced stages of the disease: A systematic review and meta-analysis of 31 randomized clinical trials. Archives of Orthopaedic and Trauma Surgery. 2023; 143:1393-408. [DOI:10.1007/s00402-021-04304-1] [PMID]
- Zhuang W, Li T, Li Y, Zhang Y, Gao J, Wang X, et al. The varying clinical effectiveness of single, three and five intraarticular injections of platelet-rich plasma in knee osteoarthritis. Journal of Orthopaedic Surgery and Research. 2024; 19:284. [DOI:10.1186/s13018-024-04736-6] [PMID]
- Sánchez M, Jorquera C, Sánchez P, Beitia M, García-Cano B, Guadilla J, et al. Platelet-rich plasma injections delay the need for knee arthroplasty: A retrospective study and survival analysis. International Orthopaedics. 2021; 45:401-10. [DOI:10.1007/s00264-020-04669-9] [PMID]
- Huang R, Li W, Zhao Y, Yang F, Xu M. Clinical efficacy and safety of stem cell therapy for knee osteoarthritis: A meta-analysis. Medicine. 2020; 99:e19434. [DOI:10.1097/MD.0000000000019434] [PMID]
- Dhillon J, Kraeutler MJ, Belk JW, Scillia AJ. Umbilical cord-derived stem cells for the treatment of knee osteoarthritis: A systematic review. Orthopaedic Journal of Sports Medicine. 2022; 10:23259671221104409. [DOI:10.1177/23259671221104409] [PMID]
- Jung SH, Nam BJ, Choi CH, Kim S, Jung M, Chung K, et al. Allogeneic umbilical cord blood-derived mesenchymal stem cell implantation versus microdrilling combined with high tibial osteotomy for cartilage regeneration. Scientific Reports. 2024; 14:3333. [DOI:10.1038/s41598-024-53598-9]
- Zhang P, Dong B, Yuan P, Li X. Human umbilical cord mesenchymal stem cells promoting knee joint chondrogenesis for the treatment of knee osteoarthritis: A systematic review.Journal of Orthopaedic Surgery and Research. 2023; 18: 639. [DOI:10.1186/s13018-023-04131-7] [PMID]
- Kitajima H, Sakamoto T, Horie T, Kuwano A, Fuku A, Taki Y, et al. Synovial fluid derived from human knee osteoarthritis increases the viability of human adipose-derived stem cells through upregulation of FOSL1. Cells. 2023; 12: 330. [DOI:10.3390/cells12020330] [PMID]
- Carneiro DC, Araújo LT, Santos GC, Damasceno PKF, Vieira JL, Santos RRD, et al. Clinical trials with mesenchymal stem cell therapies for osteoarthritis: Challenges in the regeneration of articular cartilage.International Journal of Molecular Sciences. 2023; 24:9939. [DOI:10.3390/ijms24129939] [PMID]
- Gupta PK, Thej C. Mesenchymal stromal cells for the treatment of osteoarthritis of knee joint: Context and perspective. Annals of Translational Medicine. 2019; 7:S179. [DOI:10.21037/atm.2019.07.54] [PMID]
- Ho KK, Lee WY, Griffith JF, Ong MT, Li G. Randomized control trial of mesenchymal stem cells versus hyaluronic acid in patients with knee osteoarthritis -A Hong Kong pilot study. Journal of Orthopaedic Translation. 2022; 37:69-77. [DOI:10.1016/j.jot.2022.07.012] [PMID]
- Wei P, Bao R. Intra-articular mesenchymal stem cell injection for knee osteoarthritis: Mechanisms and clinical evidence. International Journal of Molecular Sciences. 2022; 24:59. [DOI:10.3390/ijms24010059] [PMID]
- Jin WS, Yin LX, Sun HQ, Zhao Z, Yan XF. Mesenchymal stem cells injection is more effective than hyaluronic acid injection in the treatment of knee osteoarthritis with similar safety: A systematic review and meta-analysis. Arthroscopy. 2024; S0749-8063(24)00555-3. [DOI:10.1016/j.arthro.2024.07.027] [PMID]
- Le H, Xu W, Zhuang X, Chang F, Wang Y, Ding J. Mesenchymal stem cells for cartilage regeneration.Journal of Tissue Engineering. 2020; 11:2041731420943839. [DOI:10.1177/2041731420943839] [PMID]
- Wu KC, Chang YH, Ding DC, Lin SZ. Mesenchymal Stromal Cells for Aging Cartilage Regeneration: A Review.International Journal of Molecular Sciences. 2024; 25:12911. [DOI:10.3390/ijms252312911] [PMID]
- Chavda S, Rabbani SA, Wadhwa T. Role and effectiveness of intra-articular injection of hyaluronic acid in the treatment of knee osteoarthritis: A systematic review. Cureus. 2022; 14:e24503. [DOI:10.7759/cureus.24503]
- Moreland LW. Intra-articular hyaluronan (hyaluronic acid) and hylans for the treatment of osteoarthritis: Mechanisms of action. Arthritis Research & Therapy. 2003; 5:54-67. [DOI:10.1186/ar623] [PMID]
- Migliore A, Procopio S. Effectiveness and utility of hyaluronic acid in osteoarthritis. Clinical Cases in Mineral and Bone Metabolism. 2015; 12:31-3. [DOI:10.11138/ccmbm/2015.12.1.031] [PMID]
- Qiao X, Yan L, Feng Y, Li X, Zhang K, Lv Z, et al. Efficacy and safety of corticosteroids, hyaluronic acid, and PRP and combination therapy for knee osteoarthritis: A systematic review and network meta-analysis. BMC Musculoskeletal Disorders. 2023; 24: 926. [DOI:10.1186/s12891-023-06925-6] [PMID]
- Navarro-Sarabia F, Coronel P, Collantes E, Navarro FJ, de la Serna AR, Naranjo A, et al. A 40-month multicentre, randomised placebo-controlled study to assess the efficacy and carry-over effect of repeated intra-articular injections of hyaluronic acid in knee osteoarthritis: The AMELIA project. Annals of the Rheumatic Diseases. 2011; 70:1957-62. [DOI:10.1136/ard.2011.152017] [PMID]
- Lippi L, Ferrillo M, Turco A, Folli A, Moalli S, Refati F, et al. Multidisciplinary rehabilitation after hyaluronic acid injections for elderly with knee, hip, shoulder, and temporomandibular joint osteoarthritis. Medicina. 2023; 59:2047. [DOI:10.3390/medicina59112047] [PMID]
- Ciapini G, Simonettii M, Giuntoli M, Varchetta G, De Franco S, Ipponi E, et al. Is the combination of platelet-rich plasma and hyaluronic acid the best injective treatment for grade II-III knee osteoarthritis? A prospective study. 2023; 2023: 1868943. [DOI:10.1155/2023/1868943] [PMID]
- De Lucia O, Jerosch J, Yoon S, Sayre T, Ngai W, Filippou G. One-year efficacy and safety of single or one to three weekly injections of hylan G-F 20 for knee osteoarthritis: A systematic literature review and meta-analysis. Clinical Rheumatology. 2021; 40:2133-42. [DOI:10.1007/s10067-020-05477-7] [PMID]
- Meng F, Li H, Feng H, Long H, Yang Z, Li J, et al. Efficacy and safety of biologic agents for the treatment of osteoarthritis: A meta-analysis of randomized placebo-controlled trials. Ther Adv Musculoskelet Dis. 2022; 14:1759720X221080377. [DOI:10.1177/1759720X221080377] [PMID]
- Schmelz M, Mantyh P, Malfait AM, Farrar J, Yaksh T, Tive L, et al. Nerve growth factor antibody for the treatment of osteoarthritis pain and chronic low-back pain: mechanism of action in the context of efficacy and safety. Pain. 2019; 160:2210-20. [DOI:10.1097/j.pain.0000000000001625] [PMID]
- Nagao M, Hamilton JL, Kc R, Berendsen AD, Duan X, Cheong CW, et al. Vascular endothelial growth factor in cartilage development and osteoarthritis. Scientific Reports. 2017; 7:13027. [DOI:10.1038/s41598-017-13417-w] [PMID]
- Fay J, Varoga D, Wruck CJ, Kurz B, Goldring MB, Pufe T. Reactive oxygen species induce expression of vascular endothelial growth factor in chondrocytes and human articular cartilage explants. Arthritis Research & Therapy. 2006; 8:R189. [DOI:10.1186/ar2102] [PMID]
- Uth K, Trifonov D. Stem cell application for osteoarthritis in the knee joint: A minireview. World Journal of Stem Cells. 2014; 6:629-36. [DOI:10.4252/wjsc.v6.i5.629] [PMID]
- Lu P, Ruan D, Huang M, Tian M, Zhu K, Gan Z, Xiao Z. Harnessing the potential of hydrogels for advanced therapeutic applications: current achievements and future directions. Signal Transduction and Targeted Therapy. 2024; 9:166. [DOI:10.1038/s41392-024-01852-x] [PMID]
- McArthur BA, Dy CJ, Fabricant PD, Valle AG. Long term safety, efficacy, and patient acceptability of hyaluronic acid injection in patients with painful osteoarthritis of the knee. Patient Prefer Adherence. 2012; 6:905-10. [DOI:10.2147/PPA.S27783] [PMID]
- Pretorius J, Habash M, Ghobrial B, Alnajjar R, Ellanti P. Current Status and Advancements in Platelet-Rich Plasma Therapy. Cureus. 2023; 15:e47176. [DOI:10.7759/cureus.47176] [PMID]
- Aly RM. Current state of stem cell-based therapies: An overview. Stem Cell Investing. 2020; 7:8. [DOI:10.21037/sci-2020-001] [PMID]
- Householder NA, Raghuram A, Agyare K, Thipaphay S, Zumwalt M. A Review of recent innovations in cartilage regeneration strategies for the treatment of primary osteoarthritis of the knee: Intra-articular Injections. Orthopaedic Journal of Sports Medicine. 2023; 11:23259671231155950. [DOI:10.1177/23259671231155950] [PMID]
- Samuelson EM, Ebel JA, Reynolds SB, Arnold RM, Brown DE. The cost-effectiveness of platelet-rich plasma compared with hyaluronic acid injections for the treatment of knee osteoarthritis. Arthroscopy. 2020; 36:3072-8. [DOI:10.1016/j.arthro.2020.07.027] [PMID]
Article type: Reviews |
Subject:
Rehabilitation Management
Received: 2025/01/6 | Accepted: 2025/07/29 | Published: 2026/03/1
Received: 2025/01/6 | Accepted: 2025/07/29 | Published: 2026/03/1
Send email to the article author

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
